RDD Conf Day 2: Josh Lounsberry (Canadian Neuromuscular Disease Network)
description

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Paediatric Neuromuscular Disease
What is old in neuromuscular disease
(and should be remembered)
Recent Advances in Neuromuscular Disease
VS

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Insist on accurate terminology

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Changing DiagnosisPatient RT
1
2
3
4

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Muscle weaknessMuscle wastingHypotoniaHyporeflexiaSensory disturbance
Traditional symptoms and signs

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseaseMuscle weakness is not a complaint of childhood
My deltoids are about MRC 4/5

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Trouble walking and runningPoor at sportsCannot keep up with peersPoor coordinationTires easilyFalls frequently
Parental concerns20 ambulant children with weakness

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Behaviour disorder (dermatomyositis) Delayed intellectual or language development (DMD) Dysmorphic features : high palate, micrognathia,UDT, Arthrogryposis (foetal akinesia deformation syndrome) Feeding difficulty, pharyngeal incoordination Leucodystrophy (congenital musc dystrophy) Vocal cord palsy at birth (SMA) Constipation (myotonic dystrophy) Elevated aminotransaminases (dystrophies)
Some atypical presentations

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Read between the lines

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
22/12 5 year old male - prep grade
“Cannot run as fast as classmates”
“Always falling over”
“Teacher has recommended a check to see why he cannot run fast”
O/E: Gait - prominent lumbar lordosis - broad based
Imp: No serious abnormality - seems to be an awkward clumsy child
Patient JF - medical record notesVisit - 1

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseasePatient JF - medical record notesVisit - 2
2/2 “Noticed by teachers to be not running properly”
O/E: “Pleasant boy with rolling gait with pelvis tending to drop to right”
“Right quads slightly wasted”
“Tone, power, reflexes normal”
Plan: “X-ray hips. Refer to Orthopaedic clinic”
19/2 Orthopaedic and Neurology Clinics
Classical Duchenne
Can barely walk up steps or rise from floor

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Duchenne Muscular Dystrophy
Known family history
Delayed motor milestones
Gait disturbance
Delayed mental development
Delayed language development
Presentation

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Duchenne Muscular Dystrophy
Age at walking - 111 patients
months
num
ber
of p
atie
nts

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Duchenne Muscular Dystrophy
Known or suspected family history Unexplained delay in motor development
Especially male not walking by 18 months Unexplained gait disturbance - esp. toe walking Unexplained intellectual impairment Unexplained language delay
Indications for CK(In relation to muscular dystrophy)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Do not expect classic adult features
in
children

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular Atrophy
Commences in lower extremities Hands and forearms attacked early Disease is one of childhood Heredity is a marked feature Fibrillar or fascicular tremors are frequent Degenerative electrical changes often seen early Disease of peripheral nerves
Hallmarks of peroneal muscular atrophyTooth (1886)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular Atrophy
Harding / Thomas Brain 103:259 1980
Age at onset

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular Atrophy
0
5
10
15
20
25
30
number
0--3 3--6 6--9 9--11years
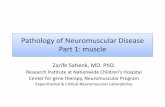
Age at onset of symptomsRCH - 42 children

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular AtrophyChampagne bottle legs

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular Atrophy
7
52
14
36
50
63
55
93
2
9
36
45
68
0 20 40 60 80 100
Hypotonia
Sensory
DTR's normal
DTR's absent
DTR's depressed
Foot deformity
Frequent falls
Abnormal walk/run
Weakness
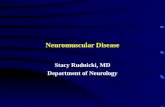
% patients
Signs Symptoms
Symptoms / signs at presentationRCH - 44 patients (types 1 & 2)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular AtrophyBrothers with PMA type 1

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Affected parents may be asymptomatic

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular Atrophy
34 years. Asymptomatic5 years age. Poor coordination, frequent falls, no foot deformity
Patient HR (1)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular Atrophy
34 years. Asymptomatic5 years age. Poor coordination, frequent falls, no foot deformity
Patient HR (2)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Peroneal Muscular AtrophyAsymptomatic parents
11 affected parents 4 definite symptoms 2 minimal deficit on examination 5 asymptomatic / normal examination
Vanasse et al 1981
RCH Series 7 out of 40 affected parents asymptomatic

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Congenital Myotonic Dystrophy
54 mothers of CMyoD children
asymptomatic at time of diagnosis 20
symptomatic - no medical attention 14
Harper 1975
Asymptomatic parents

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Ask for old photographs

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Congenital Myotonic DystrophyPatient JS (centre)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Review old biopsies and postmortems

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseaseReview old material / ask for photographs

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Review undiagnosed patients
changing signs
improved knowledge
new diagnostic tests

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Emery Dreifuss DystrophyPatient AB

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Do not always accept what parents tell you

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseasePatient CNFather of BN

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseasePatient BNDaughter of CN

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
If you think you are onto a good thing
stick to it

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Tomaculous Neuropathy (HNPP)
Acute onset brachial palsy while swimming
Patient SW 12y

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Tomaculous Neuropathy (HNPP)
32
4
1
Family of SW
1 Transient foot drop
2 Four focal neuropathies
3 Ulnar palsy
4 Brachial plexus palsy

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Tomaculous Neuropathy (HNPP)Pathology

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Tomaculous Neuropathy (HNPP)
Recurrent mononeuropathies or plexopathies NCS abnormalities in clinically unaffected nerves Characteristic pathology - myelin thickenings Autosomal dominant inheritance DNA deletion 17p 11.2 (PMP-22 gene)
Cardinal Features

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Tomaculous Neuropathy (HNPP)
Incidence: 16 / 100,000 population (?higher) Onset: 50% in second decade (birth - old age) Problem: Initial mononeuropathy (or plexopathy) Deficit: Motor > sensory. Painless Recover: Days to weeks
Note: Clinical heterogeneity. Many asymptomaticSome: tingling, cramps, myalgia, pes cavus
Clinical

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Tomaculous Neuropathy (HNPP)
Nerves subject to compression, stretch, friction
Usually associated with trivial trauma Commonest sites
• peroneal at fibula head• ulnar at elbow• radial at spiral groove of humerus• median at carpal tunnel• brachial plexus, sciatic, cranial
ClinicalSites involved

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Remember :
You may be dealing with an iceberg
The most dangerous bit is not obvious

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseaseFamily H (1)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseaseFamily H (2)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseaseFamily H (3)

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
Name Year AgeRH 1921 17SH 1926 24WB 1928 11AR 1935 39JB 1940 27MR 1940 16DB 1941 19GH 1948 24WR 1952 29DH 1952 12
Family H (4)
15 others positive for MH by CK or biopsy (2000)
Anaesthetic related deaths

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
5m Delayed development, hypotoniaDysmorphic features - ptosis, abnormal ears, small
- antimongoloid slant to eyes
4y Muscle biopsy (needle) - non specific / neurogenic
12y Scoliosis. CK 2243 (rr<240). Review of biopsy
16y Scoliosis surgery. Subtle MH reaction
In vitro testing for MH - positive
Patient MB (female)
Diagnosis: King-Denborough syndrome

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseasePatient MB

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
King-Denborough Syndrome
Small build Cryptorchidism Pectus carinatum Kyphosis / lordosis Hypoplastic mandible Crowded lower teeth Antimongoloid slant to eyes Ptosis Low attachment of ears Webbed neck
J Pediatrics 83:37 1973

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
King-Denborough Syndrome

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular DiseaseCentral core myopathy
MH susceptible
M.O.

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Central Core Myopathy

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Neuromuscular Disease
DNA might be the gold standard
but
it is not always infallible

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Myotonic Dystrophy
K.M.
S.M.M.M.
From 7 yrs: fatigue, poor concentration, poor writing, feet turning in
“Known to be affected” - DNA studies 1993 age 3 years
“A double check on the original studies will not go astray”
Patient MM - 9 yrs

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Myotonic Dystrophy
K.M.
S.M.M.M.
Allele 1 - 5 Allele 2 - 13 ie WNL. Repeated with same result
Patient MM - 9 yrs

Children’s Neuroscience CentreRoyal Children’s Hospital, Melbourne
Paediatric Neuromuscular Disease
Clinical Clues and Pitfalls
a series of anecdotes, experiences, facts and figures
Lloyd Shield