Oxygenation of nursing care.docx

of 56
-
Upload
lita-kamalia -
Category
Documents
-
view
224 -
download
0
Transcript of Oxygenation of nursing care.docx
-
7/27/2019 Oxygenation of nursing care.docx
1/56
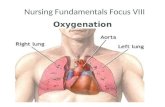
Oxygenation of nursing care
I. UNDERSTANDING oxygenation
Oxygenation is to provide the flow of oxygen gas (O2) is more than 21% at 1 atmosphere pressure so that oxygen concentrationincreases in the body.
II. GRANT PURPOSE oxygenation
1. To maintain adequate oxygen to the tissues
2. To lower the lungs work
3. To reduce cardiac work
III. BREATHING SYSTEM ANATOMY
A. Breath Top Channels
1. Nose
Consisting of external and internal parts
External section protruding from the face and propped up by the nasal bone and cartilage
The internal nose is a cavity-aisle which separated into right and left nasal cavity by a narrow vertical divider, called a septum nasal cavity is lined with mucous membranes which contain very many so-called vascular nasal mucosa
The surface of the nasal mucosa covered by the goblet cells that secrete mucus continuously and is moving back to the nasopharynxby cilia movement
The nose serves as a channel for air flow to and from the lungs
The nose also serves as a filter for dirt and moisten and warm air is inhaled into the lungs
Nose is also responsible for the olfactory (penghidu) because the olfactory receptors located in the nasal mucosa, and this function
is reduced in line with age
2. Pharyngeal
pharynx or throat is a structure such as tuba that connects the nose and mouth cavities into the larynx
pharynx is divided into three regions: nasal (nasopharynx), oral (oropharynx), and larynx (laringofaring)
pharyngeal function is to provide a channel on the respiratory and digestive tract
-
7/27/2019 Oxygenation of nursing care.docx
2/56
3. Larynx Larynx or voice organ is an epithelial structure of the cartilage that connects the pharynx and trachea
Larynx is often called the voice box and consists of:
- Epiglottis: leaf valve ostium cartilage that covers the larynx during swallowing direction
- Glottis: ostium between the vocal cords in the larynx- Thyroid cartilage: the largest cartilage of the trachea, a portion of this form the Adam's apple cartilage (Adam's apple)
- Cartilage krikoid: the only complete ring of cartilage in the larynx (located below the thyroid cartilage)
- Cartilage aritenoid: used in the movement of the vocal cords with the thyroid cartilage
- Vocal cords: the ligaments that are controlled by muscle movements that produce sounds sound (vocal cords attached to the lumen
of the larynx)
The primary function of the larynx is to allow the occurrence of vocalization
Larynx also serve to protect the lower airway from foreign object obstruction and facilitate stone
4. Trachea
Also called windpipe
The end of the trachea branches into two bronchi called Karina
B. Breath Channel Down1. Bronchus
Divided into right and left bronchus Called lobaris right bronchus (3 lobes) and the left bronchus lobaris (2 bronchial)
lobaris right bronchus is divided into 10 segmental bronchus and left bronchus is divided into 9 lobaris segmental bronchus
segmentalis bronchus is then divided again into subsegmental bronchi are surrounded by connective tissue that have: arterial,
lymphatic and nerve
2. Bronchioles
segmental bronchi branch into bronchioles
mengadung bronchial submucosal glands that produce mucus that forms an uninterrupted blanket to line the inside of the airway
3. Terminal bronchioles bronchioles form the branching into the terminal bronchioles (who had no mucous glands and cilia)
4. Respiratory bronchioles
-
7/27/2019 Oxygenation of nursing care.docx
3/56
terminal bronchioles and then into respiratory bronchioles respiratory bronchioles regarded as transitional between the airway channel conduction and airway gas exchange
5. Alveolar duct and alveolar Sakus
respiratory bronchioles and alveolar ducts leading into and sakus alveolar
And then into the alveoli6. Alveoli
Represents the exchange of O2 and CO2
There are approximately 300 million which, if united to form one sheet will be an area of70 m2
Consists of 3 types:
- The cells of alveolar type I: the epithelial cells that form the walls of the alveoli
- The cells of alveolar type II: is a metabolically active cells and secrete surfactant (a phospholipid that lines the inner surface and
prevents alveolar collapse for no)
- Alveolar cells Type III: is the macrophages which are cells fagotosis and worked as a defense mechanism
LUNG
A cone-shaped organ that elastic
Located in the chest or thoracic cavity The two lungs are separated by a central mediastinum contains the heart and some large blood vessels
Each has a lung apex and base Right lung is larger and divided into 3 lobes by fissures interlobaris
left lung is smaller and is divided into 2 lobes
Lobos-lobes are divided into several segments according to segment bronkusnya
Pleural
A thin layer that contains collagen and elastic tissue
Divided form the 2:
- Namely the parietal pleura that lines the chest cavity
- Namely the visceral pleura of each lung menyelubingi Among the pleural cavity there is a thin liquid-filled pleural effusion that serves to facilitate the two surfaces that move during
respiration, also to prevent separation of the thorax with the lung
-
7/27/2019 Oxygenation of nursing care.docx
4/56
Pressure in the pleural cavity is lower than atmospheric pressure, this is to prevent lung collapseIV. BREATHING SYSTEM PHYSIOLOGY
Breathing / respiratory merupkan air exchange process between the individual and the environment in which O2 is inhaled (inspired)
and CO2 are discarded (expired).
Breathing process consists of 3 parts, namely:1. Ventilation of entrance and exit of atmospheric air from the alveoli into the lungs or vice versa.
The process of exit and entry of air the lungs depends on the difference in pressure between atmospheric air to the alveoli. On
inspiration, the chest, expands, the diaphragm down and increased lung volume. While the expiration is a passive movement.
Factors that affect ventilation:
a. Atmospheric air pressure
b. Clear airway
c. Developing adequate lung
2. Diffusion is the exchange of gases (oxygen and carbon dioxide) between the alveoli and lung capillaries.
The process of exit and entry of air that is from blood-pressure / greater concentration to the blood pressure / concentration is lower.
Because the walls of the alveoli are very thin and is surrounded by a network of capillary blood vessels are very tight, the membrane
is sometimes called the membrane respiration.The difference in pressure on the gases contained in each side of the membrane greatly affects the process of diffusion respiration.
Normally the oxygen pressure gradient between alveoli and pulmonary capillary blood into about 40 mmHg.Factors that influence diffusion:
a. Lung surface area
b. Thick membrane respiration
c. Total blood
d. Circumstances / number of capillary blood
e. Affinity
f. When the air in the alveoli
3. Transport is the transport of oxygen through the blood to tissue cells and vice versa carbon dioxide from body tissues into thecapillaries.
Oxygen needs to be transported from the lungs to the tissues and carbon dioxide must be transported from the tissues back into the
-
7/27/2019 Oxygenation of nursing care.docx
5/56
lungs. Normally 97% oxygen will bind to hemoglobin in red blood cells and taken to the tissue as oxyhemoglobin. The remaining 3%are transported into the liquid plasma and cells.
Factors that affect the rate of transportation:
a. Cardiac output (cardiac output / CO)
b. The number of red blood cellsc. Blood hematocrit
d. Exercise (exercise)
V. FACTORS THAT INFLUENCE BREATHING
Factors affecting oxygenation are:
1. Development Stage
At birth there are major changes in respiration of the lungs that were previously filled with fluid to be filled with air. Babies have a
small chest and shortness of breath way. Shape rounded chest in infancy and childhood, the diameter from front to back is reduced by
the proportion of the transverse diameter. In adults thoracic assumed oval. At the advanced age was also a change in shape and
thoracic breathing pattern.
2. Environmental
Altitude, heat, cold and pollution affect oxygenation. The higher the mainland, the lower the PaO2, so that fewer and fewerindividuals O2 that can be inhaled. As a result individuals at altitude areas have breathing and heart rate increases, also the depth of
breathing increases.In response to heat, peripheral blood vessels will be dilated, so blood will flow to the skin. Increasing the amount of heat lost from
the body surface will result in increased cardiac output so that the oxygen demand will also increase. In cold environments the
opposite happened kontriksi peripheral blood vessels, resulting in increased blood pressure which would reduce cardiac events,
thereby reducing the need for oxygen.
3. Lifestyle
Activity and physical exercise increases the rate and depth of breathing and heartbeat, as well as supply of oxygen in the body.
Smoking and certain occupations in dusty, can be a predisposing lung disease.
4. Health StatusIn people with healthy cardiovascular and respiratory systems can provide sufficient oxygen to meet the needs of the body. However,
diseases of the cardiovascular system often result in disruption of oxygen delivery to body cells. In addition, diseases of the
-
7/27/2019 Oxygenation of nursing care.docx
6/56
respiratory system may have the opposite effect on blood oxygen. One example of cardiovascular conditions that affect oxygen isanemia, because the hemoglobin carries oxygen and carbon dioxide, the anemia can affect the transport of gases to and from the cell.
5. Narcotics
Narcotics such as morphine and may decrease the rate and into the breathing when the respiratory center depression dimedula.
Therefore, when giving narcotic analgesic drugs, the nurse should monitor the rate and depth of breathing.6. Changes / disturbances in respiratory function
Respiratory function can be disrupted by conditions that can mempengarhi respiratory namely:
a. Air movement into or out of lungs
b. Diffusion of oxygen and carbon dioxide between the alveoli and pulmonary capillary
c. Oxygen transport and transport dioxide through the blood to and from the cell network.
Interference with the respiration of hypoxia, changes in breathing pattern and partial airway obstruction.
Hypoxia is a condition when insufficient oxygen in the body was inspired to network. This can be related to ventilation, gas diffusion
or gas transport by the blood that can be caused by conditions that can alter one or more parts of the process of respiration. Other
causes of alveolar hypoventilation hypoxia is inadequate in relation to the decrease in tidal volume, so that carbon dioxide
accumulates in the blood sometimes.
Cyanosis may be marked with a bluish color of the skin, nails and mucous membranes base caused by a deficiency of oxygen inhemoglobin levels. Adequate oxygenation is essential for cerebral function. Cerebral cortex can tolerate hypoxia for only 3-5 minutes
before permanent damage occurs. People face acute hypoxia usually looks anxious, tired and pale.7. Changes in breathing pattern
Normal breathing is effortless and breathing is the same distance and bit depth differences. Breathing is difficult called dyspnoe
(shortness). Sometimes there nostrils the breath of inspiration because of increased business, increased heart rate. Orthopneo namely
the inability to breathe except in a sitting position and standing as in patients with asthma.
8. Airway obstruction
Complete airway obstruction or in part can occur along the respiratory tract at the top or bottom. Upper airway obstruction include:
nasal, pharing, larynx or trachea, can occur because of foreign objects such as food, because the tongue falls backward (otrhopharing)
if the individual is not aware or if secretions accumulate disaluran breath.Airway obstruction in the lower part involves partial or complete occlusion of the airway to the bronchi and lungs. Maintain an open
airway is a nursing intervention that may sometimes require appropriate action. Onbstruksi part of the airway characterized by
-
7/27/2019 Oxygenation of nursing care.docx
7/56
snoring sound during inhalation (inspiration).VI. NURSING ASSESSMENT
In general, the assessment begins with collecting data about:
1. Biodata of patients (age, sex, occupation, education)
Age of patients could show patient's stage of development both physically and psychologically, gender and employment should bestudied to determine the relationship and its influence on the occurrence of problems / diseases, and education level can affect the
client's knowledge about the problem / illness.
2. Chief complaint and history of chief complaint (PQRST)
The main complaint is the complaint most disturbing perceived by the client at the time of nurses assess, and review of the history of
chief complaint should contain elements of PQRST (Palliative / Provocative, Quality, Region, Scale, and Time)
3. Historical developments
a. Neonates: 30 - 60 x / min
b. Infants: 44 x / min
c. Child: 20 - 25 x / min
d. Adults: 15 - 20 x / min
e. Older adults: increased residual volume, decreased vital capacity4. Family health history
In this case should be examined whether any family members who have problems / diseases are similar.5. Social History
Necessary to study the habits of clients and their families, for example: smoking, employment, recreation, environmental, etc. factors
allergens.
6. Psychological history
Here, nurses need to know about:
a. Behavior / client responses to the problem / illness
b. Effect of pain on the way of life
c. Client's feelings of pain and therapyd. Behavior / family response to the problem / disease and therapy
7. Spiritual History
-
7/27/2019 Oxygenation of nursing care.docx
8/56
8. Physical examinationa. Nose and sinuses
Inspection: nostrils, septum deviation, perforation, mucosal (color, swelling, exudate, blood), nasal symmetry.
Palpation: frontal sinus, maxillary sinus
b. PharyngealInspection: color, symmetrical, exudate ulceration, swelling
c. Tracheal
Palpation: by standing right beside the patient, place the middle finger on the bottom of the trachea and tracheal touch up, down and
sideways so that the position of trachea can be known.
d. Thorax
Inspection:
Posture, varies for example patients with chronic respiratory problems klavikulanya be elevation to the top.
The chest, in infants differ from adults. Baby's chest is round / circular with a diameter equal to Antero-posterior diameter tranversal
(1: 1). In adults Antero-posterior diameter ratio and tranversal is 1: 2
Some chest deformity including: Pigeon chest that forms the chest is marked with a narrow diameter tranversal, Antero-posterior
diameter of the sternum enlarged and very prominent in the future. Funnel chest is a congenital disorder characterized by contrastwith the pigeon chest, the sternum narrowed into Antero-posterior diameter and smaller. Barrel chest is marked with Antero-posterior
diameter and equal or comparison tranversal 1: 1.Spinal disorders including: Kiposis curved or bent where the back / convex to the rear. Lordosis ie breasts forward or back concave.
Scoliosis of the spine tergeliatnya to one side.
Patterns of breath, in this case should be examined speed / frequency of breathing if breathing is normal breathing eupnea clients
where speed of 16-24 x / mnt, clients calm, quiet and does not need power to do so, or rapid breathing tachipnea namely, the
frequency of more than 24 x / min, or slow breathing bradipnea ie, the frequency of less than 16 x / min, or whether the state of
cessation of respiratory apnea.
There should also be assessed whether hyperventilation respiratory volume is increasing the amount of air in the lungs that is
characterized by a deep and long breathing or hypoventilation is less air in the lungs that is characterized by a slow breathing.It should be also examined the nature of the respiratory whether clients use chest breathing is breathing that is characterized by the
development of the chest, or abdominal breathing is breathing that is characterized by the development of stomach.
-
7/27/2019 Oxygenation of nursing care.docx
9/56
There should also be studied rhythm / normal breathing rhythm is regular or irregular, or does the client have Cheyne Stokesrespiration is rapid breathing became slow and sometimes interspersed with apnea, or breathing kusmaul is breathing fast and deep,
or breathing Biot namely respiratory rhythm nor amplitodunya irregular and punctuated periods of apnea.
There should also be assessed difficulty breathing client, whether dyspnea is shortness of breath and persistent oxygen requirement is
not met, or orthopnea namely the ability to breathe only when in a sitting position or standing.There should also be assessed breath sounds, in this case should be examined a stertor / snoring that occurs because of upper airway
obstruction, or stidor that sounds dry and loud and be heard during inspiration, breath or wheezing that sounds like a whistle, or rales
are sound urgent or bubbly and heard during inspiration, or ronchi the breath sounds are harsh and dry and be heard during
expiration.
It should also be reviewed coughing and secretions, whether the client has a cough productive cough followed by secretion, or non-
productive cough that is dry and harsh cough without secretion, or whether the cough hemoptue bleed
Status of the circulation, in this case should be examined heart rate / pulse takhikardi namely whether the pulse rate of more than
100 x / min, or bradikhardi ie the pulse is less than 60 x / min.
Blood pressure also should be studied whether hypertension is a high arterial blood pressure, or arterial hypotension is low blood
pressure.
Also need to be assessed on whether the patient oxygenation occurs anoxia is a condition with the amount of oxygen in tissue is less,or hipoxemia namely a state with less amount of oxygen in the blood, or hipoxia the reduced supply of oxygen in tissue due to
internal or external abnormalities, or cianosis the bluish color -tint on the mucosal membranes, nails or skin due to excessivedeoxygenation of Hb, namely enlargement of finger clubbing or fingers due to lack of oxygen in a long time.
Palpation:
To assess the state of the skin on the chest wall, tenderness, masses, inflammation, and tactile vremitus symmetry expansion.
Tactile vremitus is a vibration that can be delivered through the system bronkhopulmonal for someone to speak. Normally more
vibration felt in the apical right lung and the chest wall due to larger right bronchi. In men more easily felt because the big man's
voice
VII. Nursing Diagnosis
Nursing diagnoses commonly occurs in patients with impaired oxygenation needs include the following:1. Ineffective airway clearance
2. Ineffective breathing pattern
-
7/27/2019 Oxygenation of nursing care.docx
10/56
3. Impaired gas exchange4. Decrease in cardiac output
5. A sense of mourning
6. Ineffective coping
7. Changes in feeling comfortable8. Potential / risks of infection
9. Impaired social interaction
10. Activity intolerance, etc. according to client response
1. Ineffective airway clearance
Namely tertumpuknya secretion or obstruction of airway.
The signs:
an abnormal breath sound
productive or non productive cough
Cianosis
dyspnea
Change the speed and depth of breathingPossible causes:
a thick secretions or foreign objects causing obstruction Accident or trauma (trakheostomi)
Abdominal pain or chest pain that reduces the movement of the chest
Medications that suppress the cough reflex and the respiratory center
Loss of consciousness due anasthesi
inadequate hydration, forming a thick secretion and difficult to expektoran
Immobilization
chronic lung disease that facilitates accumulation of secretions
2. Ineffective breathing patternNamely the patient's response to the respiration by the amount of O2 supply is inadequate kejaringan
The signs:
-
7/27/2019 Oxygenation of nursing care.docx
11/56
dyspnea Increased respiratory rate
shallow breathing or slow
chest retraction
Enlargement of the finger (finger clubbing) Breathing through the mouth
Antero-posterior diameter Additions
Cianosis, flail chest, orthopnea
Vomitus
Expansion of the lungs are not symmetrical
Possible causes:
There is inadequate lung development due to immobilization, obesity, pain
neuromuscular disorders such as: tetraplegia, head trauma, drug toxicity anasthesi
musculoskeletal disorders such as: fracture of the chest, the trauma that causes lung collapse
CPPO such as emphysema, bronchial obstruction, distension of alveoli
hypoventilation due to high anxiety Airway obstruction such as acute infection or allergy that causes bronchial spasms or edema
Hoarding of CO2 due to lung disease3. Impaired gas exchange
Namely acid-base changes in the blood resulting in respiratory acidosis and respiratory alkalosis.
4. Decrease in cardiac output
The signs:
Cardiac arrhythmia
Blood pressure varies
Takikhardia or bradikhardia
Cianosis or pale Weakness, vatigue
jugular venous distension
-
7/27/2019 Oxygenation of nursing care.docx
12/56
decreased urine output edema
Problems breathing (orthopnea, dyspnea, shortness of breath, rales, and cough)
Possible causes:
output cardiac dysfunction due to coronary artery disease, heart disease Reduced blood volume due to hemorrhage, dehydration, allergic reactions and reactions of heart failure
Cardiak arrest due to electrolyte disturbance
Electrolyte imbalances such as excess blood potassiom
VIII. NURSING PLAN
1. Maintain open airway
A. Installation of artificial airway
Artificial airway (artificial airway) is a tool pipe (tube) is inserted into the mouth or nose to the level of the 2nd and 3rd from the
trachea to facilitate ventilation circle and secretion or disposal
Route installation:
Orotrakheal: mouth and trachea
Nasotrakheal: nasal and tracheal Trakheostomi: tube inserted into the trachea through an incision that is created in the circle of cartilage of the 2nd or 3rd
Intubation endotrakhealB. Practice deep breath and cough effectively
Usually performed on patients or postoperative bedrest
How it works:
Patients in a sitting or lying position
Place hands on chest
Inhale slowly through your nose until the chest expands
Hold your breath for a few seconds
Exhale slowly through your mouth to contract the chest dampai Repeat step 3 until the 5th as much as 2 -3 times
Breathe in through your nose and then hold for a few seconds then remove it quickly with a cough who voiced
-
7/27/2019 Oxygenation of nursing care.docx
13/56
Repeat according to the patient's ability In patients pot op. The nurse put the palms of hands or a pillow on the scar area and press it slowly when the patient coughs, to
avoid opening the incision wounds and reduce pain
C. Good position
semi-Fowler position or high Fowler allows maximum lung development because the abdominal contents are not pressing thediaphragm
Normally, adequate ventilation can be maintained through the change of position, ambulation and exercises
D. Mucus suctioning (suctioning)
Is a method to remove excessive secretions in the airway, suction can be performed on the oral, nasopharingeal, trakheal,
endotrakheal or trakheostomi tube.
E. Bronkhodilator drug delivery
Is a drug to dilate the airway bronchi mucosa against edema and muscle spasm and reduce obstruction and improve air exchange.
These drugs can be administered orally, sub-cutaneous, intravenous, rectal and nebulizer or suck or inject the drug into the airways.
2. Mobilization of pulmonary secretions
A. Hydration
Fluids given 2 orally by encouraging patients to consume a lot of fluids - 2.5 liters per day, but within the limits of ability / cardiacreserve.
B. Humidifikasi
Suction of steam to help thin or dissolve mucus.
C. Postural drainage
Is the position khuus used for gravitational forces to assist in the release of bronchial secretions from bronkhiolus who lodged in the
bronchi and trachea, with the intention in order to cough up secretions or inhaled.
Usually done 2-4 times before meals and before sleep / rest.
Technique: Before postural drainage, do:
- Nebulizer to drain secretions
- Percussion approximately 1-2 minutes
- Vibration 4-5 times in one period
-
7/27/2019 Oxygenation of nursing care.docx
14/56
Perform postural drainage, depending on the location of secretions in the lungs.3. Maintain and enhance the development of lung
A. Breathing exercises
Is a technique used to replace the deficit through increased efficiency of respiratory breathing aimed at saving energy through
breathing controlType of breathing exercises:
Respiratory diaphragm
Pursed lips breathing
Breathing rib side down
Breathing ribs and lower back
Respiratory segmental
B. Installation of mechanical ventilation
Is a tool that serves as a substitute for action flowing / blowing air into the thorax and diaphragm. This tool can maintain ventilation
automatically in a long period.
There are two types of negative pressure ventilation and positive pressure ventilation.
C. Installation of chest tubes and chest drainageChest tube drainage / intra-pleural drainage thorakik used after the procedure, one or more chest catheter made in the pleural cavity
through the chest wall surgery and connected to the drainage system.The indication of lung injury such as: hemothoraks, pneumothorax, open pneumothorax, flail chest.
The goal:
To remove the solution, solid, air from the pleural cavity or thoracic cavity and mediastinal cavity
To restore lung expansion and re-arrange normal cardiorespiratory function in patients post-surgery, trauma and medical conditions
by creating negative pressure in the pleural cavity.
Type:
a. The single-bottle water seal system
b. The two water bottlec. The three water bottle
4. Reduce / correcting hypoxia and hypoxia due to compensatory
-
7/27/2019 Oxygenation of nursing care.docx
15/56
By giving O2 to via: Nasal canule
Bronkhopharingeal khateter
Simple mask
Aerosol mask / trakheostomy collars ETT (endo trakheal tube)
5. Increasing gas transport and Cardiak Output
With cardiac pulmonary resuscitation (CPR), which includes the ABC action, namely:
A: The water way is to maintain the cleanliness or relieve the airway
B: Breathing is the provision of artificial breathing through the mouth to mouth or mouth to nose
C: Circulation is to begin cardiac compression or provide artificial circulation
So in general nursing interventions included in it:
a. Health promotion
Adequate ventilation
Avoid smoking
Protected / masks when working Avoid inhalers, nose drops, spray (which can suppress nerve 1)
Clothing that is comfortableb. Health restoration and maintenance
Maintain airway with efforts to thin the secretions
Mechanical cough and postural drainage
Suctioning
Eliminate fear with explanations, Fowler position semi-Fowler, significant other
Set the rest and activity by providing a useful HE, facilitating environment, increase a sense of comfort, appropriate therapy, ROM
Reduce business memeadai breathing with ventilation, light and warm clothing, avoid overeating and contains a lot of gas, set the
position Maintain nutrition and hydration as well with oral hygiene and food are easily chewed and digested
Maintain elimination by providing fiber and teach exercises
-
7/27/2019 Oxygenation of nursing care.docx
16/56
Prevent and control the potential infection by emphasizing the principles of medical asepsis O2 Therapy
Treatment of ventilation
Chest Drainage
IX. NURSING IMPLEMENTATION AND EVALUATIONImplementation of nursing in accordance with the intervention and evaluation were appropriate and objective criteria including
evaluation process.
Bibliography
http://iwansain.wordpress.com/2007/08/22/kebutuhan-oksigenasi/
________________________________________
Join with people who are looking, in your field in Answers
Posted by Arwin LIM at 02:29 2 comments
Respiratory tract ANFIS
Anatomy
Conductor channel air until it reaches the lungs is the nose, farinx, larinx trachea, bronchus, and bronchioles.
NoseThe anterior nares are the channels in the nasal cavity. Channels that empties into a section known as the vestibule. Nasal mucous
membrane is coated as a very rich in blood vessels, and continued with a layer farinx and sinus mucous membranes that have a hole
into the nasal cavity. Septum nasi separating the cavum nasi. This structure consists of thin bone and cartilage, often bent to one side
or the other side, and coated by both sides with mucous membranes. Cavum nasi lateral wall formed by the partial maxilla, palatine,
and os. Sphenoidale. Smooth and curved bones attached to the lateral wall and protruding into the cavum nasi are: (1) superior
conchae (2) Media, and (3) inferior. The bones are covered by mucous membrane.
Basic cavum nasi is formed by the palatine os os Frontale da roof while the cavum nasi is a narrow gap formed by the os and os
sphenoidale Frontale. Olfactory mucous membrane, on the roof and adjacent parts of cavum nasi, contains special nerve cells thatdetect odors. From these cells to nerve fibers through the lamina cribriformis Frontale os and into the olfactory bulb olfactory nerve I
cranial.
-
7/27/2019 Oxygenation of nursing care.docx
17/56
Paranasalis sinus is the space inside the skull associated through holes into cavum nasi, sinus mucous membrane is coated by acontinuous with cavum nasi. The hole that opens into the cavum nasi: (1) Nostrils (2) Sinus Sphenoidalis, above the superior concha
(3) Sinus ethmoidalis, by a hole between the superior concha and concha media and between media and inferior (4) the frontal sinus,
between the concha media and superior (5) ductus nasolacrimalis, below the inferior concha.
On the back, cavum nasi open into the nasopharynx through appertura nasalis posterior.
Farinx (pharynx)
is a muscular tube that runs from the base of the skull until persambungannya with oesopagus at an altitude of krikoid cartilage. Then
located behind the larinx (larinx-pharyngeal). Oropharynx is the part of the pharynx merrupakan combined respiratory and digestive
systems.
Laringx (throat)
Located on the front of the center line of the neck, next to the skin, glands tyroidea, and some muscle kecila, and front and upper
laringofaring esopagus.
Larynx is a complete structure consists of:
1. cartilago thyroidea cartilago ie, the epiglottis, cartilago cricoidea, and 2 cartilago arytenoidea2. Membarana namely cartilago connecting with each other and with the os. Hyoideum, mucous membranes, plika vocalist, and
muscles acting on the plica vocalistCartilago tyroidea V-shaped, with prominent V neck forward as the Adam's apple. Tip above the posterior border is the superior
horn, protrusion of the attachment of ligaments thyrohyoideum, and below is the horn a smaller place with the outside cartilago
beratikulasi cricoidea.
Membrane Tyroide mengubungkan upper limit and superior to the os hyoideum horn.
Cricothyroideum membrane connects the lower limit with cartilago cricoidea.
Epiglottis
Cartilago shaped leaves and protruding upward behind the tongue base. Epiglottis is attached to the back of the V cartilagothyroideum.
Plica aryepiglottica, walking backward from the side of the epiglottis toward cartilago arytenoidea, forming the entrance boundary
-
7/27/2019 Oxygenation of nursing care.docx
18/56
larynx
Cartilago cricoidea
Cartilago shaped signet ring with a large part behind. Located under cartilago tyroidea, associated with these cartilago by membrane
cricotyroidea. Cutaneous inferior cartilago thyroidea articulates with cartilago tyroidea on each side. Cricottracheale membraneconnects with the lower limit first tracheal ring
Cartilago arytenoidea
Two cartilago small pyramid-shaped base which is located on cartilago cricoidea. Plica vocalist on each side attached to section
posterio prominent corner forward pyramid
Mucous membrane
Larynx mostly covered by respiratory epithelium, composed of cylindrical cells are ciliated. Plica vocalists lined by squamous
epithelium.
Plica vocalistPlica vocalists are two sheets of thin mucous membrane that lies on top of ligamenturn vocale, two fibrous band stretched between
the inside cartilago thyroidea on the front and cartilago arytenoidea on the back.Plica false vocalists are two fold. mucous membrane just above the plica real vocalists. This section is not involved dalarn sound
production.
Muscle
Small muscles attached to the cartilago arytenoidea, cricoidea, and thyroidea, that with the contraction and relaxation can be closer
and separates plica vocalists. The muscles are innervated by cranial nerve X (vagus).
Respiration
During quiet respiration, plica vocalists held somewhat apart so that air can come and go. During the strong respiration, plica widthapart vocalists.
-
7/27/2019 Oxygenation of nursing care.docx
19/56
Fonasi
The sound vibrations produced olch plica vocalists during expiration. The sound produced is modified by motion palaturn Molle,
cheeks, tongue, and lips, and a particular resonance by the cranial air sinuses.
Clinical featuresLarynx can be blocked by:
(A) foreign objects, such as lumps of food, small toys
(B) swelling of mucous membranes, for example, after sucking the steam or the allergic reaction,
(C) infections, such as diphtheria,
(D) tumors, such as vocal cord cancer.
Trachea or windpipe
Is a flexible tube with a length of approximately 10 cm by 2.5 cm wide. trachea runs from cartilago cricoidea down on the front of the
neck and behind the manubrium sterni, ending sternal angle as high as (link manubrium with corpus sterni) or until approximately the
fifth thoracic vertebrate height and in this place two bronckus branched mcnjadi (bronchi). Trachea is composed of 16-20 non-circles
berupan complete cartilage rings are tied together by fibrous tissue and a complete circle on the back of the trachea, but it also makessome muscle tissue.
Bronchus
Bronchus which is formed from two parts of the trachea at an altitude of approximately the fifth thoracic vertebrate, has a similar
structure to the trachea and coated oleh.jenis the same cell. Bronchus, bronchus was run down and laterally to the reins of the lung.
Right Bronckus shorter and wider, and more vertical than the left, slightly higher FROM pulmonary artery and pulled out a major
branch passes under the artery, called bronckus lower lobe. Left bronchus is longer and more slender than the right, and runs under
sebelurn pulmonary artery in the split into several branches that run kelobus top and bottom.
The main branch of the right bronchus and left bronchus branched out again into a lobe lobaris and kernudian segmentalis. This
branching bronchus which went on to become smaller in size, until eventually become bronkhiolus terminalis, ie the smallest airways
that do not contain alveoli (air bag). Bronkhiolus terminalis has a diameter of approximately I mm. Bronkhiolus not reinforced bycartilage rings. But surrounded by smooth muscle so that its size may change. All of the airways down to the level of the terminal is
-
7/27/2019 Oxygenation of nursing care.docx
20/56
called channel Conductor bronkbiolus air because its main function is as Conductor of air into the lungs for gas exchange.Alveolus where gas exchange is composed of bronkhiolus assinus and respiratory sometimes have a small air pocket or alveoli in the
walls. Alveolar ductus entirely limited by alveoilis and alveolar sakus terminalis was the end of the lungs, acini atau.kadang called
primary lobolus have hands approximately 0.5 to 1.0 cm. There are about 20 times the branching from the trachea to alveolar Sakus.
Alveoli are separated by a wall called Kohn pores.
Lungs
The lungs are contained within the thoracic cavity on the left and right. The lungs have:
1. Apex, apex of lung extends into the neck approximately 2.5 cm above calvicula
2. costo vertebral surface, attached to the inside of the chest wall
3. mediastinal surface, attached to the pericardium and heart.
4. and base. Located in the diaphragm
lungs also Coated by the parietal pleura and visceral pleural effusions. In the pleural cavity contained liquid surfactant that serves to
lubrication. Right lung lobes were divided into three lobes namely superior, medius and inferior, while the left lung divided into two
lobes namely the superior and inferior lobes. Each lobe is covered by elastic tissue containing lymph vessels, arterioles, venules,
bronchial venules, alveolar ductus, sakkus alveolar and alveoli. It is estimated that stiap lungs contain 150 million alveoli, which hasa surface large enough for the surface / gas exchange.
Blood Supply1. pulmonary artery
2. bronchial artery
Innervasi
1. Parasympathetic via the vagus nerve
2. Rehabilitated and reconstructed sympathetic truncus simpaticus
Pulmonary Circulation
The lungs have two sources of blood supply from bronchial arteries and pulmonary artery. Blood in the right atrium through the right
turn into water keventrikel other AV valve, called the valve semilunaris (trikuspidalis). Blood came out of the right ventricle and theflow through the fourth valve, pulmonary valve, into the artery pulmonais. Pulmonais artery branches into right and left pulmonary
-
7/27/2019 Oxygenation of nursing care.docx
21/56
artery which flowed keparu respective right and left. In the lungs the pulmonary artery branch many times into erteriol and thencapillaries. Each capillary perfusion to Saluan give breathing, through an alveolus, all capillaries reunite to become venules, and
venules into a vein. Veins fuse to form a large pulmonary vein.
Blood flow in the pulmonary venous return keatrium left to complete the cycle of blood flow. The heart, systemic circulation and
pulmonary circulation. Pulmonary blood pressure about 15 mmHg. The function of pulmonary circulation is carbon dioxide removedfrom the blood and oxygen is absorbed, through a continuous cycle of blood around the systemic circulation and the par, then the
supply of oxygen and spending the remaining substances can take place for all cells.
PHYSIOLOGICAL
The surface area of the lung area, which is only separated by a thin membrane of the circulatory system, theoretically resulting in a
person susceptible to the entry of foreign matter (dust) and bacteria that enter the air with inspiration. However, the lower respiratory
tract in normal circumstances is sterile. There are several defense mechanisms that maintain this sterility. We already know the reflex
swallowing or vomiting reflex that prevents the entry of food or liquids into the trachea, also working escalator mukosiliaris which
trap dust and bacteria then move into the esophagus. Next, a layer of mucus that contains factors that may be effective as a defense,
namely immunoglobulin (especially IIgA), PMNs, interferon, and specific antibodies. Cough reflex is an other, more powerful
mechanism to promote secretion into the top so that it can be swallowed or expelled. Alveolar macrophage is the last defense andmost importantly against the invasion of bacteria into the lungs. Alveolar macrophages are phagocytic cells with characteristics to
migrate and have enzymatic properties, These cells move freely on the surface of the alveoli and covers as well as swallowing objectsor bacteria. After covering the particles of microbial lytic enzyme found in macrophages will kill and digest microorganisms without
causing significant inflammatory reaction.
Physiological process of respiration in which oxygen is removed from the air into the tissues, and carbon dioxide released into the
expiratory air can be divided into three stages.
1. The first stage is the ventilation, namely the inclusion of a mixture of gases into and out of the lungs.
2. The second stage, transportation, which consists of several aspects:
(1) diffusion of gases between the alveoli and lung capillaries (external respiration) and between systemic blood and tissue cells;
(2) the distribution of blood in the pulmonary circulation and penyesuaiannVa with air distribution in the alveolar-alveolar; and
(3) chemical and physical reactions of oxygen and carbon dioxide with the blood.3. Or cell respiration internal respiration is the final stage of respiration. During this respiration metabolites oxidized for energy, and
-
7/27/2019 Oxygenation of nursing care.docx
22/56
carbon dioxide is formed as a waste of cell metabolism processes and issued by the lungs.
Ventilation
The air moves in and out of the lungs due to excess pressure contained between the atmosphere and alveolus by the mechanical work
muscles. As previously mentioned, the thoracic wall to function as a bellows. Seiama inspiration, thoracic volume increase in sizebecause of the diaphragm down and ribs lifted due to contraction of some muscles. M. sternokleidomastoideus lift the sternum up and
m. serratus, m. and m. scalenus External intercostalis role raised ribs. Thoracic enlarged in three directions: anteroposterior, lateral
and vertical. This volume increase causes a decrease in pressure intrapleura, from about -4 mm Hg (relative to atmospheric pressure)
to approximately -8 mm Hg when the lungs expand during inspiration. At the same time intrapulmonal pressure or airway pressure
decreased to about -2 mm Hg (relative to atmospheric pressure) of 0 mm Hg at the start of inspiration. The difference in pressure
between the airways and rnenyebabkan atmospheric air to flow into the lungs until the airway pressure at end inspiration longer the
same as atmospheric pressure.
During quiet breathing, expiration is a passive movement due to the elasticity of the chest wall and lungs. At the time m. External
intercostalis relaxation, decreased chest wall and diaphragm arch went up into the cavity toralks, causing decreased thoracic volume,
m. intercostal rib internus can press down firmly and into the expiratory time robust and active, cough, vomiting, or defecation. In
addition, the abdominal muscles may be contracted so that the enlarged intra-abdominal pressure and push the diaphragm upward.Reducing the volume of this thorax as well as the pressure increases pressure iintrapleura intrapulmonal. Intrapulmonal pressure now
increased to about I to 2 mmHg above atmospheric pressure. The difference in pressure between the airways and the atmosphere isnow reversed so that air flows out of the lungs to airway pressure and atmospheric pressure the same again at the end of expiration.
Note that the pressure intrapleura always under atmospheric pressure during respiration cycle. Changes in ventilation can be
predicted by lung function tests.
DIFFUSION
The second stage of the process of respiration includes the process of diffusion of gases across the alveolar-capillary membrane is
thin (thickness less than 0.5 um). Pernindahan driving force for this is the partial pressure difference between the blood and gas
phase. Partial pressure of oxygen in the atmosphere at sea level the amount of approximately 149 mm Hg (21 per cent of 760 mm
Hg). At the time of inspired oxygen and to the alveolar partial pressure was then decreased to about 103 mm Hg. Decrease in partialpressure is estimated on the basis of the fact that the inspiration of air mixed with indoor air airway anatomical loss, and with water
-
7/27/2019 Oxygenation of nursing care.docx
23/56
vapor. This anatomical loss of space in normal circumstances have a volume of 1 ml of air per pound body weight (150 ml/150 lbmale). Only clean air reaching the alveoli, which is effective ventilation. Partial pressure of oxygen in mixed venous blood (PV 02) in
the lung capillary size of about 40 mm Hg. Because the partial pressure of oxygen in the capillaries is lower than the pressure in the
alveolus (P A02 = 103 mm Hg), then the oxygen can easily diffuse into the blood stream. C02 pressure difference between the blood
and the alveoli are much lower (6 mmHg) causes the carbon dioxide diffuses into the alveoli. Carbon dioxide is then released into theatmosphere, where its concentration is essentially zero. The difference between blood and alveolar C02 was very small but adequate
as it can diffuse approximately 20 times faster than oxygen, across the alveolar-capillary membrane because of the solubility is
greater.
RELATED ventilation-perfusion
The transfer effectively between alveolar gas and pulmonary capillary require air distribution in the lungs and perfusion (blood flow)
in capillaries. In other words, ventilation and perfusion of the pulmonary unit should be appropriate. In a normal person in an upright
position and a resting state, the ventilation and perfusion nearly balanced except at the apex of lung. Pulmonary circulation pressure
and low resistance result in blood flow in the lung base is greater than at the apex of the lung, due to the influence of gravity. But
fairly evenly ventilated. The average value of the ratio of ventilation to perfusion (V / Q) was 0.13. This figure is obtained from the
ratio of the average normal alveolar ventilation rate (4 liters / min) divided by the normal cardiac output (5 liters / min). normalconditions of ventilation and perfusion lung of a balanced approached the value 0.8.
Most respiratory illnesses experienced an imbalance between ventilation-perfusion process. Consequently ventiIasi wasted (V / Q =infinity). Abnormal respiration unit which is a shunt into two units, where there was no ventilation, but normal perfusion, thus wasted
perfusion (V / Q = 0). The last unit is a stationary unit, in which there is no ventilation and perfusion. Of course there are variations
among the three extreme cases, depending on the overall balance between ventilation and perfusion lung. Lung disease and
respiratory functional disorders can be classified physiologically according to the type of illness they experience, whether caused a
large shunt (V / Q (0.8)
Transport OXYGEN IN BLOOD
Oxygen can be transported from the lungs to the network via two paths:
1. physically dissolves in plasma or2. chemically bound to hemoglobin as oxyhemoglobin (HbO2).
-
7/27/2019 Oxygenation of nursing care.docx
24/56
chemical bonding of oxygen and hemoglobin is reversible. The amount actually transported in this form has a nonlinear relationshipwith PaO2 (partial pressure of oxygen in arterial blood), which is determined by the amount of oxygen physically dissolved in blood
plasma. In contrast, the amount of oxygen physically dissolves in plasma have a direct relationship with the partial pressure of
oxygen in the alveolus (PaO2). Unless it also depends on the solubility of oxygen in plasma. The amount of oxygen dissolved in
normal circumstances is physically very small because the solubility of oxygen in plasma is low. only about one percent of total angamount of oxygen transported to tissues is transported in this way. Mode of transport like this do not survive even in a state of rest
though. Most of the oxygen transported by hemoglobin contained in red blood cells. In certain circumstances (for example: carbon
monoxide poisoning or massive hemolysis which occurs insufficiency of hemoglobin, the oxygen is sufficient to sustain life can be
transported in the form of a physical solution by providing oxygen to a pressure higher than atmospheric pressure (hyperbaric oxygen
chamber).
One gram of hemoglobin can bind with 1.34 ml of oxygen. Because the average concentration of hemoglobin in the blood of adult
males magnitude sekitair 15gr per 100 ml, then 100 ml of blood can carry (15 x 1.34 = 20.1), 20.1 ml of oxygen when the blood was
saturated (SaO2 = 100 percent) . But the blood that has been teroksigenisasi and leaving the lung capillaries to get a little additional
venous blood which is a mixture of blood, the bronchial circulation. This dilution process was the cause so that the blood leaving the
lungs is only 97 percent saturated, and 19.5 percent of the volume transported to the network. At the network level, dissociating
oxygen from hemoglobin and diffuses into the plasma.Of oxygen plasma into tissue cells of the body to meet the needs of the respective networks. Although about 75 percent of the
hemoglobin is bound with oxygen in the hemoglobin returned to the lungs in the form of mixed venous blood. So really only about25 psersen oxygen in arterial blood is used for networking purposes. Hemoglobin, which releases oxygen at the tissue level is called
reduced hemoglobin (Hb). Reduced hemoglobin causes the color purple and bluish in venous blood, as we see in the superficial
veins, misainya: on hand. Whereas oxyhemoglobin (hemoglobin that binds oxygen) in red light and causes the reddish color of
arterial blood.
Oxyhemoglobin dissociation curve
In order to understand clearly the process of respiration with oxygen must be known affinity of hemoglobin for oxygen supply to
tissues and taking oxygen by the lungs is dependent on those relationships. This knowledge is necessary to state the exact size of the
gas and to perform therapeutic measures in respiratory insufficiency. If the complete blood subjected to by the various partialpressure of oxygen and percentage saturation of hemoglobin was measured, then the S-shaped curve obtained when the two
-
7/27/2019 Oxygenation of nursing care.docx
25/56
measurements are combined. This curve is known as the oxyhemoglobin dissociation curve and expressed hemoglobin affinity tooxygen at various partial pressures. In normal circumstances the body temperature (98.60 F) and blood pH 7.4.
This curve has a physiological fact to note is, that part of the flat. At the top of the curve known as the artery (A) and the vein (V) at
the bottom of a steep, slightly shifted to the right. At the top of a flat curve, large changes in oxygen pressure is associated with little
change in oxyhemoglobin saturation. It states that a relatively constant amount of oxygen can be supplied to the networks even athigh altitudes where the P02 may be equal to 60 mmHg or less. It also stated that administration of high concentrations of oxygen
(normal air = 21 percent) in patients suffering from mild hypoxemia. (Pa02 60-75 mmHg) is futile, because oxyhemoglobin can only
be improved very little. Indeed, high concentrations of oxygen can be toxic jaringin lungs and cause adverse effects. release of
oxygen to the tissues can be enhanced by the relationship of the saturation of oxygenated P02 on a steep curve of the vein. In this
section, major changes in oxyhemoglobin saturation associated with little change in 02.
Oxygen affinity of hemoglobin is influenced by many other factors that accompany the metabolic network and can be changed by the
disease. Oxyhemoglobin curve is shifted to the right when the blood pH decreases or increases PC02. in this state, in particular P02
hemoglobin affinity for oxygen is reduced so that oxygen can be transported by the blood decreases. Pathological conditions that can
cause acidosis metabollk, such as shock (due to excessive formation of lactic acid-anaerobic metabolic) or the retention of carbon
dioxide will cause a shift in the curve right. Shift the curve slightly to right will help release oxygen kejaringan-network. This shift is
known as the Bohr effect. Slight increase in acidity due to the release of carbon dioxide from the tissues. Another factor that causes ashift to right curve is the increase in temperature and 2.3 diphosphoglyceric (2,3-DPG) which is an organic phosphate in red blood
cells that binds hemoglobin and reduces oxygen affinity of hemoglobin in anemia and chronic hypoxemia cell 2,3-DPG red bloodincreases. Keep in mind the fact that, despite the ability of oxygen transport by hemoglobin decreased when the curve shifts to the
right, the ability of hemoglobin to release oxygen to tissues made easier. Therefore, the anemia and chronic hypoxemia curve shift to
the right is a process of compensation.
Curve shift to the right accompanied by an increase in temperature, illustrates the increase of cell metabolism and increased need for
oxygen, also can fit in and to certain blood flow causes the increasing number of oxygen yaiag released into the tissues.
Conversely, an increase in blood pH (alkalosis) or a decrease in PCO2, temperature, and 2 3-DPG will cause a shift in
oxyhemoglobin dissociation curve to the left. The shift to the left causes an increase in hemoglobin affinity for oxygen. As a result of
oxygen uptake in the lungs increased if there was a shift to the left, but the release of oxygen to the tissues affected. Because it is
theoretically possible to happen hypoxia (insufficient oxygen to meet metabolic network in a state of severe alkalosis, especially ifaccompanied by hypoxemia. This condition can occur during the process overventilasi mechanism with respiratory or at high
-
7/27/2019 Oxygenation of nursing care.docx
26/56
altitudes due to hyperventilation. Because hyperventilation can also lowered due to decreased cerebral blood aiiran PaC02, it alsooften causes cerebral ischemia-geiala symptoms as if his head is light. The blood that is stored lose 2,3-DPG activity so that the
affinity of hemoglobin for oxygen increases. Therefore, patients given transfusions of blood stored in large quantities may be
impaired release of oxygen to the tissues due to shift of oxyhemoglobin dissociation curve to the left.
Affinity of hemoglobin is popularly defined by P02 was needed to produce 50 percent of saturation, and easily measured dalarnmodern laboratory. Under normal circumstances P50 about 27 mm Hg. Proved that if the dissociation curve shifts to the right
(reduction of hemoglobin affinity for oxygen) then the P50 will increase, while the shift of the curve to the left (increase in
hemoglobin for oxygen afinits P50 will go down.
Carbon monoxide has an affinity to hemoglobin approximately 250 times greater DARP on oxygen affinity of hemoglobin. If
carbonmonoksida inhaled it will be associated with the carboxy, the reaction is not reversible. So the amount of hemoglobin available
to transport oxygen is reduced.
TRANSPORT OF CARBON DIOXIDE IN BLOOD
Transport of CO2 from keparu-lung tissue in three ways as follows:
1. In Fisk soluble in plasma (10%)
2. Binds to amino groups in hemoglobin in red blood cells (20%)3. transported as plasma bicarbonate (70%)
Carbon dioxide binds with water to the reaction as below:CO2 + H2O = H2CO3 = H + + HCO3-
This reaction is reversible and is known by the name of equality Dapa bicarbonate acid-carbonic acid. Hyperventilation is alveolar
ventilation in a state of excessive metabolic requirement alkalosis as a result of excessive CO2 excretion keparu-lung. Ventilated
alveoli hypoventilation is not able to meet the needs of metabolism, as a result of the retention of CO2 by the lungs.
ARRANGEMENTS respiration
Respiration regulated / controlled in:
1. Medulla oblongata
2. PuncherBroadly speaking, that the lungs have the following functions:
-
7/27/2019 Oxygenation of nursing care.docx
27/56
1. There are surface gases namely oxygen from atmospheric air flow kedarah vein and remove carbon dioxide gas from the alveolikeudara atmosphere.
2. Filter out toxic substances from circulation
3. Blood Reservoir
4. Its main function is to exchange gasesHere is a picture of anatomy of the lungs:
http://iwansain.wordpress.com/2007/07/25/anfis-saluran-pernafasan/
Embolism (embolus)
Peers, you must be careful on the state of occurrence of embolism in blood vessels, because embolism can be claimed the lives of
patients in case of blockage in vital organs such as the pulmonary artery, the coroner artery, renal artery, and arterial cereberal. even
more patients died due to intravenous infusions of exactly what happened with the formation of air embolism. surely this should be a
concern that serius.Baiklah, to better understand the embolism, the following will I lay out as follows:
Is embolic it?
Is a foreign object stuck in a place in the blood circulation. The item carried by the blood stream, and coming from somewhere otherthan the composition of blood circulation.
Embolus (95%) originated from thrombus.This process is called embolism embolus formation
Type embolus
Represent solids derived from the thrombus, the tumor cells, groups of bacteria, tissue
are fluid embolus can form fatty substances, amniotic fluid
embolus is the gas can be air, nitrogen gas, carbon dioxide
Embolus often found in veins, arteries, lymph vessels and the heart
As a result - a result that caused by an embolus
Cause of sudden death
Death or myocardial tissue septic embolus nest - a nest of new infections and abscess-new abscess
-
7/27/2019 Oxygenation of nursing care.docx
28/56
Metastasis of malignant tumorsWhat is an embolus Vena
Derived from the veins, lower leg and then from the vein in the pelvis
Embolus -> follow the drainage vein -> larger veins -> vena cava -> right heart -> stuck in the pulmonary circulation -> obstruction /
occlusion a. TDP allows for the pulmonary circulation pulmonary blockade -> insufficiency a. coronaria and myocardial infarction,anoksemia, general anoksia -> sudden death
The existence of reflex vagal pulmo coronary -> cause spasms in the lungs and coronary arteries -> sudden death
Pulmonary embolus large krn rarely cause infarction patients had died first. Pulmonary embolus is often accompanied by infarction
mainly in the lower right lobe
What is Arterial embolus?
Coming from a mural thrombus in the heart, the thrombus is attached to the pond-dike heart and aorta
Artery embolus often about the brain, kidney, spleen, and lower limbs.
Embolus in a. mesenterica -> intestinal infarction
Embolus in a. coronaria -> sudden death
What is a fat embolus?This fat into the blood circulation and clog an artery or a capillary allows for an embolus -> cause of death
Fat embolus most often occur because of trauma to bone or fatty tissue that is broken long bones, especially femur and tibia alongwith bone marrow damage also occur during childbirth. It also occurs on: due to skin burns; in which inflammation of the bone or fat
tissue; in fatty liver caused by malnutrition or alcoholism
What is amniotic fluid embolus?
This situation is rarely found, the symptoms are:
shortness of breath
Shock
sudden death who unexpectedly in women who have given birth or during childbirth
Embolus in a. pulmonary-containing scrap pieces of baby skin epithelial tissue, verniks caseosa, mucus and lanugo
What is Gas embolus?Gas bubbles enter the circulation susuna so clogged and can cause death as the act of vaginal douche.
-
7/27/2019 Oxygenation of nursing care.docx
29/56
Can also be caused by thoracic surgery due to a large vein is cut off or torn.Can also be caused by blood transfusion or intravenous fluid infusion.
The authors expect, you are more professional in providing nursing care, especially in a situation that can cause embolic state in
patients.
----http://iwansain.wordpress.com/2007/09/20/embolus/
Thrombus
Hazards caused by thrombus is almost the same as emboli. both cause blockages in blood vessels, only difference is the occurrence of
the blockage. Thrombus is more directed at vascular endothelial cell injury that causes the aggregation of platelets to the recovery of
damaged tissue, but sometimes this process can block blood flow so it is said trombus.Untuk better understand the concepts
associated with thrombus, please read the following explanation:
Whether thrombus that?
Is an element which is composed of objects and of the elements of blood in blood vessels or the heart while still alive
Thrombosis -> The process of thrombus formationHow Thrombi Formation and Structure?
Normally -> blood flow remains liquid because of the particular balance that is very complex, but in certain circumstances thisbalance can be disturbed occur allows for thrombosis.
In these circumstances inherent pd platelet endothelial surface vessels or the heart. Blood streaming -> the number of platelets
attached to the place tersbt pd -> platelets stick to each other interchangeable -> form a mass protruding into the lumen.
Pd certain moment when the blood flow quickly (like Dlm the arteries), which formed the mass of platelets will be separated from the
vessel walls but was then replaced with another platelet
If there is damage to the platelets -> released a thromboplastin substances, substances that stimulate the formation of blood clots.
Thromboplastin will change the prothrombin -> thrombin that reacts with the fibrinogen -> fibrin. In addition, thrombin causes the
rupture of platelets -> formation of thromboplastin
TDA has a shape typical thrombus platelet layer and covered by Leukocytes, erythrocytes and fibrin. From the outer surface of thethrombus appears as a rock with lines -> Line of Zahn. It's white and red thrombus grainy. When you cut the lines appear in layers of
-
7/27/2019 Oxygenation of nursing care.docx
30/56
gray and whiteWhat causes thrombus?
According to Virchow that the thrombus is formed due to three factors:
Changes to the endothelial surface of blood vessels
severity of such blood flow Changes to the constitution of blood
Ad 1. Changes in the surface of endothelial
Endothelial damage -> change in electrical potential -> platelet easily attached to the endothelium. Thrombosis can occur in
circumstances:
Atherosclerosis
Inflammation of blood vessels such as polyarteritis nodusa, thromboangitis obliterans, throbolplebitis
Thrombosis in the heart lining that coats endocard who suffered myocardial infarction and in endocarditis
Ruda force (trauma)
Ad 2. Changes in blood flow
Platelets flow in the peripheral zone and restricted zone of the vessel wall by the plasma. When blood flow slows down the platelets
into the plasma zone allows for increased contact with the endothelialWhen blood flow slows down -> platelets will step aside -> easily attached to the walls of blood vessels.
blood flow changes more frequently in veins than arteries. Thrombi also often occur in circumstances varices -> dilated veins.Varices are often found at the following places:
lower leg veins are superficial
plexus pampiniformis
plexus hemorrhoidalis
The end of the distal esophagus
Ad 3. Changes to the constitution of blood
Platelets in greater numbers make it easier for thrombus formation because they are more apt to occur adhesion (adhesive) state can
be found at:
puerperal period (2-3 times more than normal) pulmonary infarction
-
7/27/2019 Oxygenation of nursing care.docx
31/56
Malignant tumors Thromboplebitis
Thromboangitis obliterans
Dpt thrombosis is also found in blood diseases such as polycytemia, the diseases that accompanied 'sludged blood', blood cells lumpy
-> blood flow slows. malignant tumor cells to form thromboplastin
THE TYPES thrombus
occlusive thrombus is a thrombus that causes clogged vessel lumen.
propagating thrombus is formed along the vessel is unstoppable and is an extension of thrombus
Saddle / riding thrombus is a thrombus can be elongated and entered into the branch vessels
Mural / parietal thrombus with thrombus is attached to the walls of blood vessels and the part attached to the walls of blood vessels
and the part that escapes as if swimming in the blood without causing occlusion of vessels (large veins)
Pedinculated thrombus is mural thrombus in the heart of long-stemmed
Ball thrombus (embolus can be said) is pedinculated thrombus loose and washed away the blood flow, large krn can get caught and
can not be past the ostium
Thrombus according to color:
Red thrombus erythrocyte t.u TDA White thrombus leukocyte part besra TDA
Mixed thrombus most types of thrombus
It can also be distinguished according to the length of thrombus occurs, namely:
Fresh thrombus
-
7/27/2019 Oxygenation of nursing care.docx
32/56
-
7/27/2019 Oxygenation of nursing care.docx
33/56
REFERENCES
Preliminary
1.
2.
3.
4.
-
7/27/2019 Oxygenation of nursing care.docx
34/56
1. Metabolism
2.
1.
2. Radiation
3. Conduction
4.
1.
2.
1.
2.
-
7/27/2019 Oxygenation of nursing care.docx
35/56
1. Physical
2. Sweat
REFERENCES
DENGUE FEVER
-
7/27/2019 Oxygenation of nursing care.docx
36/56
Conclusion:
-
7/27/2019 Oxygenation of nursing care.docx
37/56
-
7/27/2019 Oxygenation of nursing care.docx
38/56
1.
2.
3.
IP Address
particular.
-
7/27/2019 Oxygenation of nursing care.docx
39/56
1. Hardware
2.
3.
-
7/27/2019 Oxygenation of nursing care.docx
40/56
I.
II.
III.
IV.
-
7/27/2019 Oxygenation of nursing care.docx
41/56
For example:
-
7/27/2019 Oxygenation of nursing care.docx
42/56
Name
Yahoo!
Lycos
-
7/27/2019 Oxygenation of nursing care.docx
43/56
Information
-
7/27/2019 Oxygenation of nursing care.docx
44/56
Browser
Cyberspace
FAQ
-
7/27/2019 Oxygenation of nursing care.docx
45/56
Home Page
HTML
HTTP
HyperLink
Hypertext
Internet
-
7/27/2019 Oxygenation of nursing care.docx
46/56
IP address
Java
Lycos
Net
Netscape
-
7/27/2019 Oxygenation of nursing care.docx
47/56
Newsgroups
Online
REFERENCES
0 comments:
Post Comments
Links to this post
Create a Link
Subscribe to: Post Comments (Atom)
Related Articles
-
7/27/2019 Oxygenation of nursing care.docx
48/56
Nursing
Blog Archive
-
7/27/2019 Oxygenation of nursing care.docx
49/56
-
7/27/2019 Oxygenation of nursing care.docx
50/56
-
7/27/2019 Oxygenation of nursing care.docx
51/56
-
7/27/2019 Oxygenation of nursing care.docx
52/56
-
7/27/2019 Oxygenation of nursing care.docx
53/56
-
7/27/2019 Oxygenation of nursing care.docx
54/56
Law.
-
7/27/2019 Oxygenation of nursing care.docx
55/56
Follower
-
7/27/2019 Oxygenation of nursing care.docx
56/56
Nursing
Baru! Klik kata di atas untuk melihat terjemahan alternatif.Singkirkan
Google Terjemahan untuk:PenelusuranVideoEmailTeleponObrolanBisnis
Tentang Google TerjemahanMatikan terjemahan instanPrivasiBantuan
http://translate.google.co.id/?client=firefox-a&rls=org.mozilla:en-GB:official&hl=id&tab=wThttp://translate.google.co.id/?client=firefox-a&rls=org.mozilla:en-GB:official&hl=id&tab=wThttp://translate.google.co.id/?client=firefox-a&rls=org.mozilla:en-GB:official&hl=id&tab=wThttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23searchhttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23searchhttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23communicatehttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23chathttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23chathttp://www.google.co.id/url?source=transpromo&rs=rssf&q=http://translate.google.co.id/about/intl/id_ALL/http://www.google.co.id/url?source=transpromo&rs=rssf&q=http://www.google.co.id/intl/id/privacy.htmlhttp://www.google.co.id/url?source=transpromo&rs=rssf&q=http://www.google.co.id/intl/id/privacy.htmlhttp://www.google.co.id/url?source=transpromo&rs=rssf&q=http://www.google.co.id/intl/id/privacy.htmlhttp://www.google.co.id/url?source=transpromo&rs=rssf&q=http://www.google.co.id/intl/id/privacy.htmlhttp://www.google.co.id/url?source=transpromo&rs=rssf&q=http://translate.google.co.id/about/intl/id_ALL/http://www.google.co.id/url?source=transpromo&rs=rssf&q=http://translate.google.co.id/about/intl/id_ALL/http://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23chathttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23chathttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23communicatehttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23communicatehttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23searchhttp://www.google.co.id/url?source=transpromo&rs=rsmf&q=http://translate.google.co.id/about/intl/id_ALL/tour.html%23searchhttp://translate.google.co.id/?client=firefox-a&rls=org.mozilla:en-GB:official&hl=id&tab=wT