Oxidative Stress and its Role in Endometriosis ... · Therapeutic Implications Sajal Gupta, ... and...
11
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/259874036 Oxidative Stress and its Role in Endometriosis —Mechanistic and Therapeutic Implications Chapter · January 2014 CITATION 1 READS 108 5 authors, including: Some of the authors of this publication are also working on these related projects: Antioxidant therapy in idiopathic oligoasthenoteratozoospermia View project Sperm Diagnostics and Selecting Healthier Spermatozoa View project Sajal Gupta Cleveland Clinic 207 PUBLICATIONS 3,443 CITATIONS SEE PROFILE Joelle Safi Saint Joseph University, Lebanon 22 PUBLICATIONS 114 CITATIONS SEE PROFILE Ashok Agarwal Cleveland Clinic 1,844 PUBLICATIONS 31,897 CITATIONS SEE PROFILE All content following this page was uploaded by Ashok Agarwal on 27 January 2014. The user has requested enhancement of the downloaded file.
Transcript of Oxidative Stress and its Role in Endometriosis ... · Therapeutic Implications Sajal Gupta, ... and...
Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/259874036
OxidativeStressanditsRoleinEndometriosis—MechanisticandTherapeuticImplications
Chapter·January2014
CITATION
1
READS
108
5authors,including:
Someoftheauthorsofthispublicationarealsoworkingontheserelatedprojects:
AntioxidanttherapyinidiopathicoligoasthenoteratozoospermiaViewproject
SpermDiagnosticsandSelectingHealthierSpermatozoaViewproject
SajalGupta
ClevelandClinic
207PUBLICATIONS3,443CITATIONS
SEEPROFILE
JoelleSafi
SaintJosephUniversity,Lebanon
22PUBLICATIONS114CITATIONS
SEEPROFILE
AshokAgarwal
ClevelandClinic
1,844PUBLICATIONS31,897CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyAshokAgarwalon27January2014.
Theuserhasrequestedenhancementofthedownloadedfile.
316 Clinical Infertility and In Vitro FertilizationChapter 37
316
Oxidative Stress and its Role inEndometriosis—Mechanistic andTherapeutic ImplicationsSajal Gupta, Rathna S Shenoy, Joelle Safi, Aarti Gaglani, Ashok Agarwal
IntroductionEndometriosis is a common gynecological disorder thataffects about 2 to 22% of women in their reproductiveyears and between 35 to 50% of women diagnosed withinfertility.1 It is also diagnosed in 10 to 70% of womenwith pelvic pain.2
Endometriosis is finding of uterine and endometrialtissue as well as menstrual effluent outside of the uterus.The location of implantation of such tissue is typicallyin the peritoneal cavity, but has also been found withinthe pleural cavity, liver, kidney, gluteal muscles, andbladder.3 The disease itself is diagnosed throughlaparoscopy, the actual gold standard. Laparoscopic
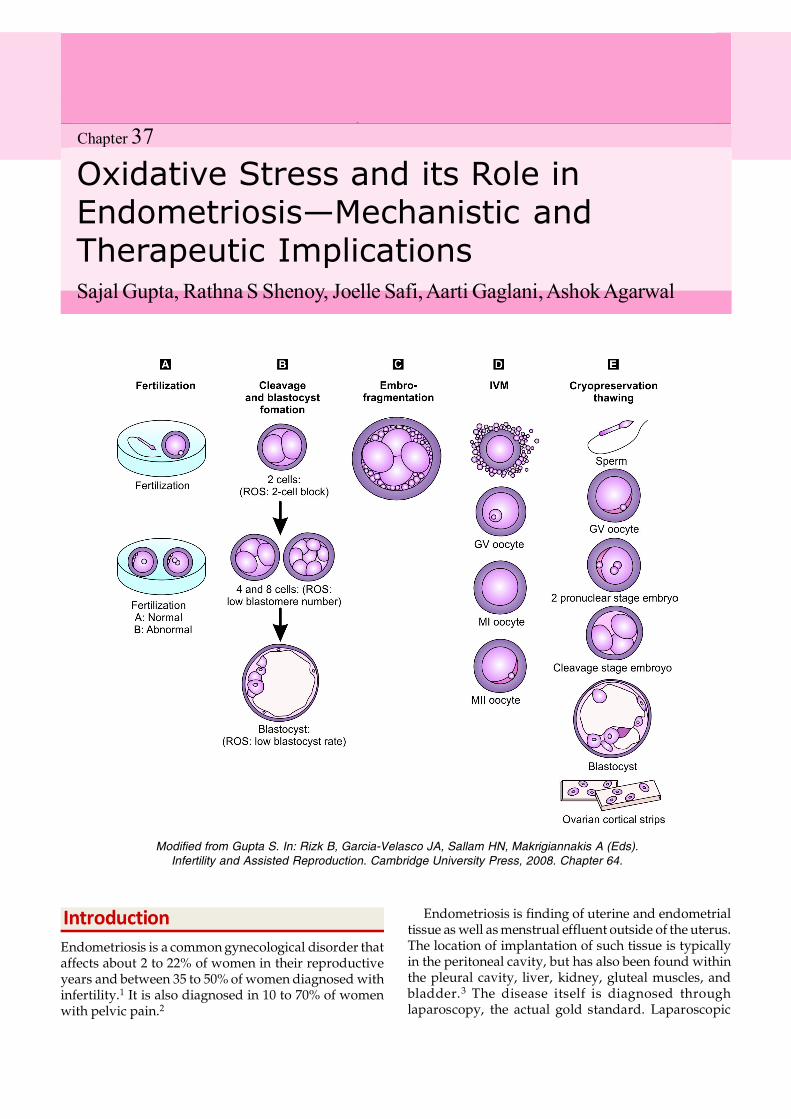
Modified from Gupta S. In: Rizk B, Garcia-Velasco JA, Sallam HN, Makrigiannakis A (Eds).Infertility and Assisted Reproduction. Cambridge University Press, 2008. Chapter 64.
317Oxidative Stress and its Role in Endometriosis
procedures can also be used in conjunction withother surgical procedures for the treatment of endo-metriosis.4
There are many factors that can play a role in thegeneration of endometriosis including genetics. A studypublished in 2005 looked at familial endometriosis ingroups of sisters that had been surgically diagnosed withthe disease. From this study, it was concluded that a newgenetic linkage for the disease was found onchromosome 10q26.5 Another possible linkage wasfound on 20p13 along with other chromosomes thatrequires additional studies.5 Evolution of betterdiagnostic methods and treatments could evolve throughthe understanding of abnormalities at these loci.5
An additional method to diagnose endometriosis maybe to assess the level of oxidative stress, a coremechanism implicated in the pathophysiology of thedisease, within the serum and the peritoneal fluid.However, the effects of reactive oxygen species (ROS)and their implications in endometriosis are uncertainbased on experiments done by different groups. ROSsuch as super oxide radical, hydrogen peroxide, hydroxylradical, and peroxynitrate, can be measured. Throughreactions with cellular components, these ROS willproduce molecules such as lysophosphatidylcholine6
and malondialdehyde,7 which are products of lipidperoxidation. Elevated levels of these 2 molecules havebeen reported in women with endometriosis.
This chapter will focus on different markers that areelevated in oxidative stress and their contribution to theprogression of endometriosis. The role of various ROSalong with the roles of iron, nitric oxide, and cytokineswill be described. The newest clinical research, alongwith innovative treatments for this disease will also beevaluated.
Etiology of EndometriosisThe etiology of endometriosis is not currently addressedby only one theory. Rather four separate theories havebeen hypothesized to simulate the disease process. Theseinclude: (1) Sampson’s implantation theory (2) Coelomicmetaplasia and induction theories (3) The embryonic resttheory, and (4) Lymphatic and vascular metastasistheories.8 The coelomic metaplasia theory introduced byMeyer proposes that endometriosis originates due toreversible changes of the epithelial lining in theperitoneal cavity. The metaplasia may occur due toinfectious, hormonal, or other stimuli.8 The inductiontheory, a broadening of the coelomic metaplasia theoryproposes endogenous biochemical and immunologicalfactors as inducers of differentiation of previouslyundifferentiated cells into endometrial tissue.8 This
theory was proved experimentally in rabbits and in invitro human cells.8 The embryonic rest theory statesthat cell rests of mullerian origin differentiate intoendometrium due to a particular stimulus.8 Thelymphatic metastasis theory states that endometrial cellsspread through the blood and lymphatic pathways.8
Sampson’s theory, hypothesized in 1927, is the mainaccepted one within the scientific community. The theoryhas its basis in three major elements: retrogrademenstruation (the reflux of endometrial and uterinetissue along with menstrual effluent from the uterusthrough the fallopian tube and into the peritoneal cavitywhere implantation occurs),8 the presence of viable cellswithin this retrograde menstruation,8 and a third of theseviable cells must have the ability to then implant andform peritoneal lesions. For proper implantation to occurthere needs to be a blood supply to the lesion which isone of the findings that has been implicated in womenwith the disease.9
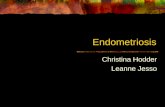
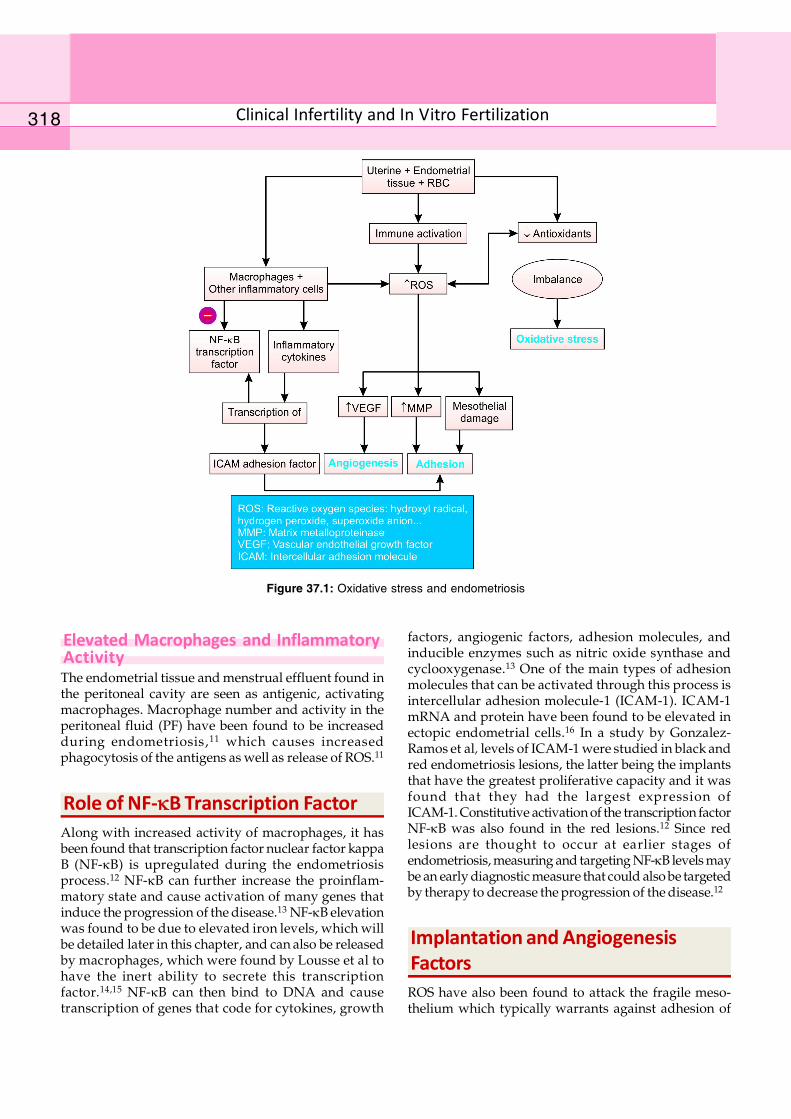
Role of Oxidative Stress inEndometriosis (Figure 37.1)
Imbalance Between ROS and AntioxidantsAlthough the different causes of endometriosis have notbeen proven yet, there does seem to be an implicationfor oxidative stress in the manifestation and progressionof the disease process. Oxidative stress occurs due to animbalance between reactive oxygen species andantioxidants. ROS are molecules that have an unpairedelectron and that stabilize themselves by extractingelectrons from different molecules in the body, like lipids,nucleic acids, and proteins. Antioxidants are a defensemechanism created by the body to neutralize the ROS.
Measurement of Oxidative Stress MarkersThe ROS target polyunsaturated fatty acids of cellmembranes in the peritoneal cavity. This results in lipidperoxidation, of which breakdown products are themeasurable oxidative stress markers malondialdehyde(MDA)7 and lysophosphatidylcholine. Both products areseen as antigenic to the body causing activation of animmune response.6, 7 The autoantibodies along with theproducts of lipid peroxidation are indicators of oxidativestress.
Cellular markers such as heat shock protein 70B’(HSP70B’) are increased in the disease as well.10
Typically, HSP are present to maintain proper proteinsynthesis and protect it from cellular stress. CirculatingHSP70B’ has been found to be implicated in cellular stressalong with pathogenesis of endometriosis.10
318 Clinical Infertility and In Vitro Fertilization
Elevated Macrophages and InflammatoryActivityThe endometrial tissue and menstrual effluent found inthe peritoneal cavity are seen as antigenic, activatingmacrophages. Macrophage number and activity in theperitoneal fluid (PF) have been found to be increasedduring endometriosis,11 which causes increasedphagocytosis of the antigens as well as release of ROS.11
Role of NF-B Transcription FactorAlong with increased activity of macrophages, it hasbeen found that transcription factor nuclear factor kappaB (NF-B) is upregulated during the endometriosisprocess.12 NF-B can further increase the proinflam-matory state and cause activation of many genes thatinduce the progression of the disease.13 NF-B elevationwas found to be due to elevated iron levels, which willbe detailed later in this chapter, and can also be releasedby macrophages, which were found by Lousse et al tohave the inert ability to secrete this transcriptionfactor.14,15 NF-B can then bind to DNA and causetranscription of genes that code for cytokines, growth
factors, angiogenic factors, adhesion molecules, andinducible enzymes such as nitric oxide synthase andcyclooxygenase.13 One of the main types of adhesionmolecules that can be activated through this process isintercellular adhesion molecule-1 (ICAM-1). ICAM-1mRNA and protein have been found to be elevated inectopic endometrial cells.16 In a study by Gonzalez-Ramos et al, levels of ICAM-1 were studied in black andred endometriosis lesions, the latter being the implantsthat have the greatest proliferative capacity and it wasfound that they had the largest expression ofICAM-1. Constitutive activation of the transcription factorNF-B was also found in the red lesions.12 Since redlesions are thought to occur at earlier stages ofendometriosis, measuring and targeting NF-B levels maybe an early diagnostic measure that could also be targetedby therapy to decrease the progression of the disease.12
Implantation and AngiogenesisFactorsROS have also been found to attack the fragile meso-thelium which typically warrants against adhesion of
Figure 37.1: Oxidative stress and endometriosis
319Oxidative Stress and its Role in Endometriosis
the endometrial cells.17 In an additional study by Koks etal in 2000, mesothelial cells were placed in culture withmenstrual effluent or menstrual serum and morphologicchanges that included retraction, shrinking and gapformation of the mesothelial cells were observed.18 Thecreation of adhesion sites allows implantation of theendometrial cells, and progression of the disease.
Another group of enzymes that play a role in theprogression of endometrial disease are the matrixmetalloproteinases (MMPs). Different types of MMPs aretypically produced by endometrial stromal cells and playa role throughout the menstrual cycle.19 In order for theimplantation of ectopic cells to occur, the extracellularmatrix of the peritoneal mesothelium must be degraded,which is facilitated by MMPs. In vitro studies where theendometrium was displaced on chorioallantoicmembranes have shown that MMPs may be necessaryfor endometriotic lesions to form and could be atherapeutic target.19
Levels of angiogenic growth factor such as vascularendothelial growth factor (VEGF) have been shown tobe elevated in the PF of women with the disease.9
Furthermore, macrophages and other immune cellsactivated during the inflammatory process have theability to produce increased amounts of VEGF.9
Antioxidants and DifferentTreatment Options in EndometriosisAntioxidants are important in neutralizing the effects ofROS and they can be enzymatic or non-enzymatic.Enzymatic antioxidants include catalase and glutathioneperoxidase. The non-enzymatic antioxidants includeseveral vitamins along with glutathione.20 When thelevels of these antioxidants along with total antioxidantlevels were tested in the PF of women with endometriosisassociated infertility, it was found that all were dimi-nished significantly. The impairment of the antioxidantsystem decreases the ability to protect the PF from theeffects of ROS.21
One of the newer fields of treatment that is beingtested is the role of oral antioxidants for treatment ofendometriosis. In a study by Mier-Cabrera et al, dailyantioxidant intake was found to be significantlydecreased in women with endometriosis (WEN)compared to women without endometriosis (WWE).Four months after a high-antioxidant diet, plasmavitamin C levels had doubled with vitamins A and Eincreasing as well.22 Glutathione peroxidase andsuperoxide dismutase levels increased two months intothe study.22 Oxidative stress markers of lipid hydro-peroxides and malondialdehyde were decreased threemonths into the study. This new therapeutic measure has
shown that administration of a high antioxidant diet couldhave the ability to be successful in treating endometriosis.
An additional therapeutic measure to treat endomet-riosis associated infertility is the drug pentoxifylline.Several studies have shown contrasting results. In astudy published in 2008, pentoxifylline was administeredfollowing surgery for a total of six months.23 Thoughresults were not significant, it was found that there wasa 28% pregnancy rate in women receiving treatmentversus 14% in women who received the placebo.23
Another study by Kamencic et al, demonstrated theefficiency of pentoxifylline in the management of post-operative pain.24 It is essential that additional studiesare completed and evaluated as to the therapeutic aspectsof the drug.
Role of CytokinesCytokines play a major role in endometriosis, as they arereleased into the PF and contribute to the regulation ofleukocytes and act on ectopic endometrium, resulting intissue and cell damage.25 Sources of cytokines includeperitoneal macrophages, lymphocytes, ectopic endo-metrial implants, and mesothelial cells of the peri-toneum.26,27
These cytokines contribute to tissue remodeling andimplantation of cells or tissue within the endometrium.28
Thus, increased PF cytokine levels can be used as specificmarkers in the diagnosis of endometriosis.
Chemoattractant cytokines, such as interleukin-8 (IL-8)and regulated on activation normal T cell expressed andsecreted (RANTES), assist macrophage recruitment intothe peritoneal cavity. Hsu et al29 found that there is a shiftof T cells toward Th2 (which produce cell-mediatedimmunity suppressant cytokines), suggesting that maybethis imbalance contributes to the defective immunologicaldefense in endometriosis.
IL-1 influences the activation of T cells and thedifferentiation of B cells and has also been found to beimplicated in the implantation of ectopic endometrium.30
IL-6 is an important cytokine that helps regulate theactivity of other cytokines, activates B-cell stimulationand is also important in reproduction, i.e. folliculo-genesis, steroid hormone synthesis, implantation and itmonitors growth of endometrial cells.31 Rier et aldemonstrated rising levels of IL-6 in the PF withincreasing severity of endometriosis.32 This suggests thepossibility of using IL-6 level as a marker for differentstages of endometriosis. Another study33 showed that PFIL-6 levels were higher in women with minimal-moderate(MM) endometriosis than in controls, but that these levelswere lower in women with moderate-severe (MS)endometriosis. Carbohydrate antigen-125 (CA 125) wasfound to be elevated in MS endometriosis, suggesting that

320 Clinical Infertility and In Vitro Fertilization
IL-6 is a reliable marker for MM endometriosis and CA125 is better for more severe cases. Several other studieshave also shown that the level of PF IL-6 is up-regulatedin women with endometriosis and can be used as aneffective, non-invasive marker for the diagnosis ofendometriosis.34-36 However the use of serum levels stillhave controversial value in diagnosis.37,38
IL-8 is a small polypeptide involved in the chemotaxisof neutrophils and in angiogenesis. Arici et al showedthat IL-8 levels were elevated in the PF of women withendometriosis, and that the levels increased with theseverity of the disease.39 It was also found to stimulateattachment of the endometrial cells to the extracellularmatrix protein, fibronectin, suggesting its important rolein the endometrial implant adhesion.40 It has beenstudied that the serum concentrations of IL-8 in ovarianendometriosis patients were higher than in patients withbenign ovarian cysts41 and that epithelial IL-8 levels werehigher in women with endometriosis when comparedto normal women during the proliferative phase.42 Thesefindings show that IL-8 plays an important role in thepathogenesis of endometriosis and can be detected andused as a reliable marker for diagnosis.
IL-12 is a cytokine important for the regulation ofnatural killer (NK) cell activity, proliferation of T cells,and increasing the cytotoxicity of NK cells.43 Levels ofIL-12 are low but detectable in the PF of women withand without endometriosis,44 suggesting that IL-12 levelsmay not be of predictive value for the diagnosis ofendometriosis. However, a study has shown that theaddition of IL-12 effectively interfered with the implan-tation of endometrium (surface and weight of lesions)in ectopic sites in a murine model of endometriosis.45
This shows the possible therapeutic value of cytokineadministration in the management of the developmentof endometriosis.
Tumor necrosis factor (TNF-) is a pleiotropiccytokine produced and stimulated by neutrophils,macrophages, lymphocytes, NK cells, among others. Itis a pro-inflammatory cytokine used to activate Th cellsand to promote endometrial proliferation andshedding.46 TNF- disrupts glutathione production,causing increased susceptibility to ROS productionwithin the female reproductive tract. A study found thatspermatozoa quality decreased when TNF- was addedin a dose- and time-dependent manner, and this decreasein sperm quality affected endometriosis-associatedinfertility.47 In addition to activation of Th cells, TNF- isalso involved in angiogenesis and cytotoxicity, tumorprogression, the up-regulation of metallomatrix proteinsin collaboration with IL-1, recruitment of neutrophils toendothelium, and the production of IL-1, oxidants, andPGE2.48 TNF- has also been found to increase theexpression of IL-6 in endometriotic stromal cells via the
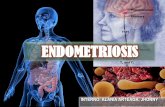
Figure 37.2: Protective mechanisms in women withoutendometriosis
NF-B pathway.49 PF TNF- levels are increased inpatients with endometriosis, and have been shown toincrease with increased severity of the disease50 but notwith its stage.37 Treatment of endometriosis couldinclude the inhibition of Th1 cytokines such as TNF-.Many substances are currently being tested to study thesuppression of endometriosis: hCG,51 as well as GnRHanalogs52 and danazol53 have been found to attenuatecytokine production and suppress endometrioticTNF- gene expression in vitro.
Role of IronIron is an essential element incorporated in a wide varietyof molecules throughout the body, including hemoglobin.However, overproduction and increased levels of iron inthe PF due to retrograde menstruation may be a cause ofoxidative stress.54
Endometrial cells have been quantitatively found inthe peritoneal cavity of 59 to 79% of menstruatingwomen, but only some develop endometriosis55 whichmay be attributed to the impairment or efficiency ofprotective mechanisms against elevated iron levels.These include macrophage maintenance of ironhomeostasis, haptoglobin sequestration of hemoglobin,and production of the hemopexin-heme complex(Figure 37.2).
Macrophages play a huge role in the homeostasis ofiron levels and have the ability to phagocytize theerythrocytes, releasing hemoglobin and heme.

321Oxidative Stress and its Role in Endometriosis
Subsequently, these molecules will be broken down intoiron, ferritin, carbon monoxide, and bilirubin throughan enzyme called heme oxygenase 1 (HO-1).56
Hemoglobin (Hb) released from erythrocytes can alsobe bound by haptoglobin (Hp), a scavenger protein.57
The Hb-Hp complex is then recognized by a scavengerreceptor CD163 on the surface of macrophages andphagocytized.57
Finally, any free floating heme released duringmetabolism of hemoglobin will be bound to hemopexinwhich has antioxidant capacity.58,59
In women with endometriosis, it has been found thatthere is an elevated level of iron within the PF comparedto controls.60-62 The increased levels of iron within thePF may occur in part due to increased amount oferythrocytes from retrograde menstruation or due toperitoneal lesion bleeding.63, 64 This, coupled with thedecreased protective mechanisms, may account for thedevelopment of endometriosis.
Ferritin, an antioxidant, sequesters iron and allowsthere to be a decreased amount of the element availableto produce oxidative stress via the Fenton reaction.65
However, due to the elevated amount of erythrocytesfound in the peritoneal cavity of women with endomet-riosis, the ferritin sequestration system becomesoverwhelmed quickly, causing there to be release of ironinto the peritoneal cavity, which can then participate inthe Fenton reaction generating hydroxyl radical, andinducing oxidative stress.66
Another ROS-antioxidant imbalance cause is thedecreased amount of bilirubin, a potent antioxidant thatis produced by heme oxygenase (HO) breakdown ofheme.56 Although HO-1 levels were found to be elevatedin certain parts of the peritoneal cavity, the majority ofthe cells that constitute the peritoneal cavity inendometriosis, the macrophages, do not express theenzyme in endometriosis patients.67 Decreasedexpression of the enzyme does not allow the finalbyproduct of heme breakdown, bilirubin, to form, andits antioxidant capacity is missing in these women.67
Overall, iron overload does cause there to be elevatedproliferation of endometrial lesions and progression ofthe disease, which means that this mechanism shouldhave therapeutic targets. One such target is the ironchelator, desferrioxamine DFO, which has shown todecrease endometrial proliferation and progression ofthe disease. By decreasing levels of iron, the levels ofoxidative stress resulting from free iron in the peritonealcavity can also be controlled.54
Role of Nitric OxideNitric oxide (NO) is an important molecule formaintenance of pregnancy at physiological levels.68
However, in high concentrations, NO can havedamaging effects on the gametes, embryos, and oviductalfunction.69
It has been hypothesized that interleukin 10 (IL-10),increased during earlier stages of endometriosis, maystimulate the release of NO by macrophages.70
NO synthase, the enzyme that ultimately producesNO through conversion of L-arginine to L-citrulline, canbe found in three forms.71 These three forms include theneuronal form NOS1, the inducible form NOS2 (iNOS),and the endothelial form NOS3 (eNOS).71 Macrophagesisolated from women with endometriosis associatedinfertility had higher iNOS activity and subsequentlyreleased higher NO levels than endometriosis freecontrols.69 The peritoneal macrophages have the abilityto move from the peritoneal cavity to other parts of thefemale reproductive system including the fallopian tubeswhere fertilization takes place and where their increasedcapacity to produce nitric oxide can then cause greaterrisk of infertility.69
Some studies have shown the localization of thedifferent NOS in the endometrium of control womenand women with adenomyosis.72 Levels of eNOS werefound to be high in the luminal and glandular epitheliumof the endometrium of controls and in the eutopicendometrium of adenomyosis subjects, while levels ofiNOS were found to be elevated in stromal lesions ofendometrium, in control endometrium and in theeutopic endometrium of adenomyosis subjects. Thispattern of expression was found only to be in thesecretory stage of the menstrual cycle for both sets ofwomen. However, in the ectopic endometrium ofpatients with adenomyosis, both enzymes were foundto be high throughout the entire menstrual cycle(including the proliferative phase).72
NO released in high levels has the ability to react withsuperoxide radical forming a potent ROS called peroxy-nitrate that has a sustained half life.73 Nitrotyrosine, aproduct that forms when peroxynitrate reacts with theamino acid tyrosine was found to be elevated duringthe proliferative and secretory phases in the ectopicendometrium of women with adenomyosis.72 Peroxy-nitrate, like any ROS, can cause progression of the diseasethrough damage to other molecules. NO levels can alsobe increased by activation of NF-kB due to increasedexpression of the gene coding for NOS.13
The levels of NOS and NO are also correlated withthe levels of the reproductive hormones estrogen andprogesterone. When fasting blood samples were takenfrom women with endometriosis associated infertility, itwas found that there was a positive correlation betweenthe levels of estrogen and progesterone and eNOS proteinlevels.74 NO activates cyclooxygenase-2 (COX-2);subsequently, prostaglandins such as prostaglandin E2
322 Clinical Infertility and In Vitro Fertilization
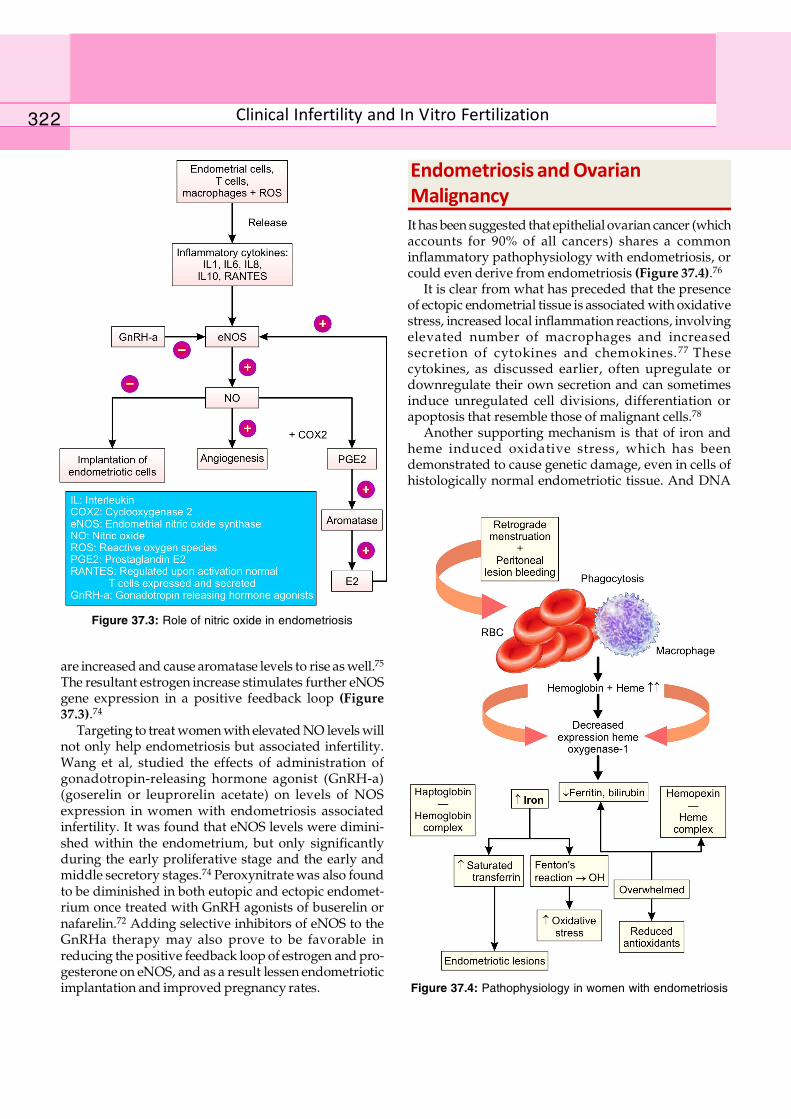
are increased and cause aromatase levels to rise as well.75
The resultant estrogen increase stimulates further eNOSgene expression in a positive feedback loop (Figure37.3).74
Targeting to treat women with elevated NO levels willnot only help endometriosis but associated infertility.Wang et al, studied the effects of administration ofgonadotropin-releasing hormone agonist (GnRH-a)(goserelin or leuprorelin acetate) on levels of NOSexpression in women with endometriosis associatedinfertility. It was found that eNOS levels were dimini-shed within the endometrium, but only significantlyduring the early proliferative stage and the early andmiddle secretory stages.74 Peroxynitrate was also foundto be diminished in both eutopic and ectopic endomet-rium once treated with GnRH agonists of buserelin ornafarelin.72 Adding selective inhibitors of eNOS to theGnRHa therapy may also prove to be favorable inreducing the positive feedback loop of estrogen and pro-gesterone on eNOS, and as a result lessen endometrioticimplantation and improved pregnancy rates.
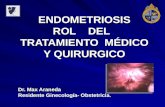
Endometriosis and OvarianMalignancyIt has been suggested that epithelial ovarian cancer (whichaccounts for 90% of all cancers) shares a commoninflammatory pathophysiology with endometriosis, orcould even derive from endometriosis (Figure 37.4).76
It is clear from what has preceded that the presenceof ectopic endometrial tissue is associated with oxidativestress, increased local inflammation reactions, involvingelevated number of macrophages and increasedsecretion of cytokines and chemokines. 77 Thesecytokines, as discussed earlier, often upregulate ordownregulate their own secretion and can sometimesinduce unregulated cell divisions, differentiation orapoptosis that resemble those of malignant cells.78
Another supporting mechanism is that of iron andheme induced oxidative stress, which has beendemonstrated to cause genetic damage, even in cells ofhistologically normal endometriotic tissue. And DNA
Figure 37.3: Role of nitric oxide in endometriosis
Figure 37.4: Pathophysiology in women with endometriosis

323Oxidative Stress and its Role in Endometriosis
damage or loss of heterozygosity as a result of oxidativestress are known to be part of carcinogenesis.79
Further more, endometrioma and ovarian cancer haveshown similar molecular genetic modifications, such asPTEN (phosphatase and tensin), p53 and bcl genesmutations, theorizing the existence of a geneticcontinuum between those pathologies.78 This theory issupported by epidemiology, pathology, anatomy, andclinical data.
Few epidemiologic controlled studies have assessedthe prevalence of ovarian cancer among endometriosispatients. However, the evidence available shows thatendometriosis could be a risk factor for ovarian cancer,with up to a 5 fold increased risk80 and at least 1.7 foldafter adjustment for other risk factors.81
On the other hand, it has been demonstrated thatendometriosis sometimes exhibits atypical architectural orcytological characteristics, like invasiveness or adherence,that resemble malignancy, and that 25% of the casespresenting with atypical ovarian endometriosis furtherdevelop ovarian cancer.82 Patients with epithelial ovariancancer have been confirmed to have a higher prevalenceof endometriosis than the general population.78 This isparticularly true of the clear cell carcinoma and theendometroid carcinoma subtypes of ovarian cancer, whichrepresent together up to 75% of endometriosis-associatedovarian carcinoma.83 These tumors were curiously foundto have a left-sided predominance (similar to endo-metriosis) and were also found to present at an earlier stageand to have better survival rates than the general populationof ovarian cancers.84
References1. Duckitt K. Infertility and subfertility. Clin Evid 2003;(9):
2044-73.2. Lapp T. ACOG issues recommendations for the
management of endometriosis. American College ofObstetricians and Gynecologists. Am Fam Physician 2000;62(6):1431-4.
3. Pritts EA, Taylor RN. An evidence-based evaluation ofendometriosis-associated infertility. Endocrinol MetabClin North Am 2003;32(3):653-67.
4. Eltabbakh GH, Charboneau AM, Eltabbakh NG.Laparoscopic surgery for large benign ovarian cysts.Gynecol Oncol 2008;108(1):72-6.
5. Treloar SA, et al. Genomewide linkage study in 1,176affected sister pair families identifies a significantsusceptibility locus for endometriosis on chromosome10q26. Am J Hum Genet 2005;77(3):365-76.
6. Murphy AA, et al. Lysophosphatidyl choline, a chemo-tactic factor for monocytes/T-lymphocytes is elevatedin endometriosis. J Clin Endocrinol Metab 1998;83(6):2110-3.
7. Shanti A, et al. Autoantibodies to markers of oxidativestress are elevated in women with endometriosis. FertilSteril 1999;71(6):1115-8.
8. Seli EM, Berkkanoglu, Arici A. Pathogenesis of endo-metriosis. Obstet Gynecol Clin North Am 2003;30(1):41-61.
Cleveland Clinic
324 Clinical Infertility and In Vitro Fertilization
9. Taylor RN, et al. Mechanistic and therapeutic implicationsof angiogenesis in endometriosis. Reprod Sci 2009;16(2):140-6.
10. Lambrinoudaki IV, et al. Measurable serum markers ofoxidative stress response in women with endometriosis.Fertil Steril 2009;91(1):46-50.
11. Zeller JM, et al. Enhancement of human monocyte andperitoneal macrophage chemiluminescence activities inwomen with endometriosis. Am J Reprod ImmunolMicrobiol 1987;13(3):78-82.
12. Gonzalez-Ramos R, et al. Nuclear factor-kappa B isconstitutively activated in peritoneal endometriosis. MolHum Reprod 2007;13(7):503-9.
13. Viatour P, et al. Phosphorylation of NF-kappaB andIkappaB proteins: implications in cancer and inflam-mation. Trends Biochem Sci 2005;30(1):43-52.
14. Lousse JC, et al. Increased activation of nuclear factor-kappa B (NF-kappaB) in isolated peritoneal macrophagesof patients with endometriosis. Fertil Steril 2008;90(1):217-20.
15. Dalton TP, Shertzer HG, Puga A. Regulation of geneexpression by reactive oxygen. Annu Rev PharmacolToxicol 1999;39:67-101.
16. Vigano P, et al. Expression of intercellular adhesionmolecule (ICAM)-1 mRNA and protein is enhanced inendometriosis versus endometrial stromal cells in culture.Mol Hum Reprod 1998;4(12):1150-6.
17. Koks CA, et al. Adhesion of shed menstrual tissue in anin-vitro model using amnion and peritoneum: a light andelectron microscopic study. Hum Reprod 1999;14(3):816-22.
18. Koks CA, et al. Menstruum induces changes in mesothelialcell morphology. Gynecol Obstet Invest 2000;50(1):13-8.
19. Pitsos M, Kanakas N. The role of matrix metalloproteinasesin the pathogenesis of endometriosis. Reprod Sci 2009;16(8):717-26.
20. Sikka SC. Role of oxidative stress and antioxidants inandrology and assisted reproductive technology. J Androl2004;25(1):5-18.
21. Szczepanska M, et al. Oxidative stress may be a piece inthe endometriosis puzzle. Fertil Steril 2003;79(6):1288-93.
22. Mier-Cabrera, J, et al. Women with endometriosisimproved their peripheral antioxidant markers after theapplication of a high antioxidant diet. Reprod BiolEndocrinol 2009;7:54.
23. Creus M, et al. Combined laparoscopic surgery andpentoxifylline therapy for treatment of endometriosis-associated infertility: a preliminary trial. Hum Reprod2008;23(8):1910-6.
24. Kamencic H, Thiel JA. Pentoxifylline after conservativesurgery for endometriosis: a randomized, controlled trial.J Minim Invasive Gynecol 2008;15(1):62-6.
25. Bedaiwy MA, Falcone T. Peritoneal fluid environment inendometriosis. Clinicopathological implications. MinervaGinecol 2003;55(4):333-45.
26. Tabibzadeh SS, et al. Cytokine-induced production of IFN-beta 2/IL-6 by freshly explanted human endometrialstromal cells. Modulation by estradiol-17 beta. J Immunol,1989;142(9):3134-9.
27. Betjes MG, et al. Interleukin-8 production by humanperitoneal mesothelial cells in response to tumor necrosis
factor-alpha, interleukin-1, and medium conditioned bymacrophages cocultured with Staphylococcus epider-midis. J Infect Dis 1993;168(5):1202-10.
28. Iwabe T, et al. Tumor necrosis factor-alpha promotesproliferation of endometriotic stromal cells by inducinginterleukin-8 gene and protein expression. J Clin Endo-crinol Metab 2000;85(2):824-9.
29. Hsu CC, et al. Enhanced interleukin-4 expression inpatients with endometriosis. Fertil Steril 1997;67(6):1059-64.
30. Simon C, et al. Embryonic implantation in mice is blockedby interleukin-1 receptor antagonist. Endocrinology1994;134(2):521-8.
31. Barcz EP Kaminski, Marianowski L. Role of cytokines inpathogenesis of endometriosis. Med Sci Monit 2000;6(5):1042-6.
32. Rier SE, Parsons AK, Becker JL. Altered interleukin-6production by peritoneal leukocytes from patients withendometriosis. Fertil Steril 1994;61(2):294-9.
33. Martinez S, et al. Serum interleukin-6 levels are elevatedin women with minimal-mild endometriosis. Hum Reprod2007;22(3):836-42.
34. Harada T, et al. Increased interleukin-6 levels in peritonealfluid of infertile patients with active endometriosis. Am JObstet Gynecol 1997;176(3):593-7.
35. Umezawa M, et al. Cytokine and chemokine expressionin a rat endometriosis is similar to that in humanendometriosis. Cytokine 2008;43(2):105-9.
36. Othman Eel D, et al. Serum cytokines as biomarkers fornonsurgical prediction of endometriosis. Eur J ObstetGynecol Reprod Biol 2008;137(2):240-6.
37. Bedaiwy MA, et al. Prediction of endometriosis with serumand peritoneal fluid markers: a prospective controlled trial.Hum Reprod 2002;17(2):426-31.
38. Seeber B, et al. Panel of markers can accurately predictendometriosis in a subset of patients. Fertil Steril 2008;89(5):1073-81.
39. Arici A, et al. Interleukin-8 induces proliferation ofendometrial stromal cells: a potential autocrine growthfactor. J Clin Endocrinol Metab 1998;83(4):1201-5.
40. Garcia-Velasco JA, Arici A. Interleukin-8 stimulates theadhesion of endometrial stromal cells to fibronectin. FertilSteril 1999;72(2):336-40.
41. Ohata Y, et al. Serum interleukin-8 levels are elevated inpatients with ovarian endometrioma. Fertil Steril 2008;90(4):994-9.
42. Ulukus M, et al. Expression of interleukin-8 and monocytechemotactic protein 1 in women with endometriosis. FertilSteril 2009;91(3):687-93.
43. Kobayashi M, et al. Identification and purification ofnatural killer cell stimulatory factor (NKSF), a cytokinewith multiple biologic effects on human lymphocytes.J Exp Med 1989;170(3):827-45.
44. Zeyneloglu HB, et al. The peritoneal fluid levels of inter-leukin-12 in women with endometriosis. Am J ReprodImmunol 1998;39(2):152-6.
45. Somigliana E, et al. Endometrial ability to implant inectopic sites can be prevented by interleukin-12 in a murinemodel of endometriosis. Hum Reprod 1999;14(12):2944-50.
325Oxidative Stress and its Role in Endometriosis
46. Siristatidis C, et al. Immunological factors and their role inthe genesis and development of endometriosis. J ObstetGynaecol Res 2006;32(2):162-70.
47. Said TM, et al. Infliximab may reverse the toxic effects indu-ced by tumor necrosis factor alpha in human spermatozoa:an in vitro model. Fertil Steril 2005;83(6):1665-73.
48. Gupta S, et al. Serum and peritoneal abnormalities inendometriosis: potential use as diagnostic markers.Minerva Ginecol 2006;58(6):527-51.
49. Yamauchi N, et al. Tumor necrosis factor-alpha inducedthe release of interleukin-6 from endometriotic stromalcells by the nuclear factor-kappaB and mitogen-activatedprotein kinase pathways. Fertil Steril 2004;82(Suppl 3):1023-8.
50. Eisermann J, et al. Tumor necrosis factor in peritoneal fluidof women undergoing laparoscopic surgery. Fertil Steril1988;50(4):573-9.
51. Huber AV, et al. Human chorionic gonadotrophinattenuates NF-kappaB activation and cytokine expressionof endometriotic stromal cells. Mol Hum Reprod 2007;13(8):595-604.
52. Sakamoto Y, et al. Tumor necrosis factor-alpha-inducedinterleukin-8 (IL-8) expression in endometriotic stromalcells, probably through nuclear factor-kappa B activation:gonadotropin-releasing hormone agonist treatmentreduced IL-8 expression. J Clin Endocrinol Metab 2003;88(2):730-5.
53. Mori H, et al. Danazol suppresses the production ofinterleukin-1 beta and tumor necrosis factor by humanmonocytes. Am J Reprod Immunol 1990;24(2):45-50.
54. Defrere S, et al. Iron overload enhances epithelial cellproliferation in endometriotic lesions induced in a murinemodel. Hum Reprod 2006;21(11):2810-6.
55. Kruitwagen RF, et al. Endometrial epithelial cells inperitoneal fluid during the early follicular phase. FertilSteril 1991;55(2):297-303.
56. Maines MD. The heme oxygenase system: a regulator ofsecond messenger gases. Annu Rev Pharmacol Toxicol1997;37:517-54.
57. Kristiansen M, et al. Identification of the haemoglobinscavenger receptor. Nature 2001;409(6817):198-201.
58. Muller-Eberhard U. Hemopexin. Methods Enzymol 1988;163:536-65.
59. Tolosano E, Altruda F. Hemopexin: structure, function,and regulation. DNA Cell Biol 2002;21(4):297-306.
60. Lousse JC, et al. Iron storage is significantly increased inperitoneal macrophages of endometriosis patients andcorrelates with iron overload in peritoneal fluid. FertilSteril 2009;91(5):1668-75.
61. Van Langendonckt AF. Casanas-Roux, Donnez J. Ironoverload in the peritoneal cavity of women with pelvicendometriosis. Fertil Steril 2002;78(4):712-8.
62. Arumugam K, Yip YC. De novo formation of adhesions inendometriosis: the role of iron and free radical reactions.Fertil Steril 1995;64(1):62-4.
63. D’Hooghe TM, Debrock S. Endometriosis, retrogrademenstruation and peritoneal inflammation in women andin baboons. Hum Reprod Update 2002;8(1):84-8.
64. Nisolle M, et al. Immunohistochemical analysis of estrogenand progesterone receptors in endometrium and
peritoneal endometriosis: a new quantitative method. FertilSteril 1994;62(4):751-9.
65. Balla G, et al. Ferritin: a cytoprotective antioxidant strategemof endothelium. J Biol Chem 1992;267(25):18148-53.
66. Van Langendonckt AF, Casanas-Roux, Donnez J.Oxidative stress and peritoneal endometriosis. Fertil Steril2002;77(5):861-70.
67. Van Langendonckt A, et al. Potential involvement ofhemoglobin and heme in the pathogenesis of peritonealendometriosis. Fertil Steril 2002;77(3):561-70.
68. Yallampalli C, et al. Role and regulation of nitric oxide inthe uterus during pregnancy and parturition. J Soc GynecolInvestig 1998;5(2):58-67.
69. Osborn BH, et al. Inducible nitric oxide synthaseexpression by peritoneal macrophages in endometriosis-associated infertility. Fertil Steril 2002;77(1):46-51.
70. Corradin SB, et al. Induction of macrophage nitric oxideproduction by interferon-gamma and tumor necrosisfactor-alpha is enhanced by interleukin-10. Eur J Immunol1993;23(8):2045-8.
71. Moncada SR, Palmer M, Higgs EA. Nitric oxide:physiology, pathophysiology, and pharmacology.Pharmacol Rev 1991;43(2):109-42.
72. Kamada Y, et al. GnRH agonist-suppressed expression ofnitric oxide synthases and generation of peroxynitrite inadenomyosis. Hum Reprod 2000;15(12):2512-9.
73. Beckman JS, Koppenol WH. Nitric oxide, superoxide, andperoxynitrite: the good, the bad, and ugly. Am J Physiol1996;271(5 Pt 1):C1424-37.
74. Wang J, et al. Prolonged gonadotropin-releasing hormoneagonist therapy reduced expression of nitric oxidesynthase in the endometrium of women with endo-metriosis and infertility. Fertil Steril 2006;85(4):1037-44.
75. Kitawaki J, et al. Detection of aromatase cytochrome P-450in endometrial biopsy specimens as a diagnostic test forendometriosis. Fertil Steril 1999;72(6):1100-6.
76. Ness RB, Cottreau C. Possible role of ovarian epithelialinflammation in ovarian cancer. J Natl Cancer Inst 1999;91(17):1459-67.
77. Gupta S, et al. Role of oxidative stress in endometriosis.Reprod Biomed Online 2006;13(1):126-34.
78. Nezhat F, et al. The relationship of endometriosis andovarian malignancy: a review. Fertil Steril 2008;90(5):1559-70.
79. Kobayashi H, et al. Molecular pathogenesis of endo-metriosis-associated clear cell carcinoma of the ovary(Review). Oncol Rep 2009;22(2):233-40.
80. Brinton LA, et al. Cancer risk after a hospital dischargediagnosis of endometriosis. Am J Obstet Gynecol1997;176(3):572-9.
81. Ness RB, et al. Factors related to inflammation of theovarian epithelium and risk of ovarian cancer. Epi-demiology 2000;11(2):111-7.
82. Fukunaga M, et al. Ovarian atypical endometriosis: itsclose association with malignant epithelial tumours.Histopathology 1997;30(3):249-55.
83. Ness RB. Endometriosis and ovarian cancer: thoughts onshared pathophysiology. Am J Obstet Gynecol 2003;189(1):280-94.
84. Kawaguchi R, et al. Clinicopathologic features of ovariancancer in patients with ovarian endometrioma. J ObstetGynaecol Res 2008;34(5):872-7.
View publication statsView publication stats