
Overview of substance use, disorders and harms © 2009 University of Sydney.
51
Overview of substance use, disorders and harms © 2009 University of Sydney
-
date post
20-Dec-2015 -
Category
Documents
-
view
214 -
download
0
Transcript of Overview of substance use, disorders and harms © 2009 University of Sydney.

Overview of substance use,
disorders and harms
© 2009 University of Sydney

Learning objectives
To develop an understanding of:– Why people use drugs– Prevalence– Substance use diagnoses– Aetiology– The impacts of substance use on
public health – Overview of public health
approaches for preventing and reducing substance misuse

Case study
• Lisa, aged 18, presents to your practice for contraceptive advice
• Lisa uses ecstasy tablets about twice a year and is not at all concerned.
• Most of her friends do likewise, and Lisa says she has not experienced any harms

Questions about Lisa
• Why are so many young people using ecstasy?
• Would you say her ecstasy use is a problem?

Why do people use drugs?
• Two primary reasons:– Pleasurable sensation– Relief of discomfort (psychological
or physical)• Secondary reasons:
– Because it is accepted – Because it is not accepted!

Substance use in social context
• Substances are often taken as part of religious or social ritual. Examples are:
– Drinking at a bar to ‘wind down’ after a week’s work
– Wine in Christian and Jewish ceremonies
– Ecstasy taken at dance parties
– Coffee as a catalyst for meeting for conversation or to enhance work performance
• Moderate, controlled use is accepted with minimal harms

Historical context
Substances which are currently seen as being harmful have not always
been seen that way
Use of some became illegal after becoming problematic (cocaine, opiates,
cannabis)
• Substance use is a consistent feature of most cultures:• First opium use recorded on Sumerian tablet in 5000BC • First brewery dates from 3500BC• Patterns of drug use and social views change over time:

Some perspectives on addiction
• Moral: a sign of weakness or evil• Legal: an offence, which should be punished
to maintain law and order• Public Health model: widespread practices
that influence the health of a nation• Medical: dependence is a neurobiological
disease with psychosocial and medical complications
• Social: cultural influences determine individual behaviour
• Psychological: the influences of learning on individual behaviour

Major drugs of abuseAny drug that acts on the CNS to cause
pleasure can be abused:• Alcohol• Nicotine• Cannabis• Opiates (licit and illicit such as heroin)• Sedatives
– especially benzodiazepines, such as Valium• Stimulants
– amphetamines, cocaine, ecstasy• Hallucinogens• Others that may be abused: solvents,
antidepressants, antihistamines, anticholinergics

Prevalence of substance use in Australia
Australian Institute of Health and Welfare, 2008
National Drug Strategy Household Survey 2007
0 10 20 30 40 50 60 70 80 90 100
Alcohol
Tobacco
Any illicit
Cannabis
Ecstasy
Ampethamines
Hallucinogens
Alangesics
Cocaine
Tranquilisers
Inhalants
Heroin
GHB
Percent
Ever used Used in past 12 months

Assessing prevalence and patterns of drug use
• Household surveys of representative samples
• Industry sales figures for alcohol, tobacco and
prescribed drugs
• Illicit Drug Reporting Scheme: uses multiple
sources of users and their contacts
• Consequences: deaths, treatment seeking,
crime

When is drug and alcohol use a problem?
What do we mean by saying a person has a drug problem?
• A disorder of drug use is present– Drug dependence (addiction)– Harmful drug use
• Use of substance(s) without further harms– Not a diagnosis or medical disorder– May not be socially accepted, be
stigmatised, or illegal

The public’s understanding of drug and alcohol problems is shaped by what is visible, what is reported by the media and individual experience.
Doctors’ opinions tend to resemble those of the public but are also informed by their professional training and experiences.
What do we mean by saying a person has a drug problem?

What does a problem drinker look like?
• Only a very small proportion of heavy drinkers look like ‘park bench’ alcoholics

International Classification of Diseases (ICD)
• Intoxication
• Harmful use
• Dependence
Same criteria for alcohol, nicotine, other psychoactive drugs
WHO, 2007

International Classification of Diseases (ICD)
• Intoxication:• Transient condition after use of a
substance leading to altered consciousness, cognition or behaviour
• Harmful use:Continuing use of the substance despite
evident harms related to substance use
What is dependence? ICD-10
Dependence is a clinical syndrome
• Strong desire to use• Difficulties controlling use• Persistent use despite harm• Higher priority given to drug use than to
other activities/obligations (salience)• Increased tolerance• Physical withdrawal

Types of drinkers (adults)
5%
15%
65%
15%
dependent
hazardous or harmful
low risk
non-drinker
Teesson, 2000, ANZ J Psych, 34 (NSMHWB)

The prevention paradox
Hazardous and harmful drinkers contribute more to the burden of harm in the community than do dependent drinkers, even though the dependent drinkers have a more severe problem.
This is because there are many more people in the former category.

Natural history of dependence
• Usually a lifelong disorder, with remissions and relapses
• Some spontaneous remission– 5% return to controlled drinking– Most need to be abstinent to avoid
out-of-control drinking

Who develops drug-related problems?
• A complication from an individual episode of drug use
• Those who experiment too often and get “caught”
• Those who try to “drown” their sorrows: – childhood abuse, psychiatric disorders– social disadvantage
• Prisoners – (imprisonment may be the result or cause of
addiction)• High risk occupations:
– military personnel, doctors, sales people, hoteliers
• Ready availability of substance

Also non-environmental risk factors for dependence
• Genetic (e.g. for alcohol) – 4 x risk if father affected even if
reared apart– Polygenic
• Psychiatric disorders

How does dependence occur?
• Dependence-producing substance– Psychoactive/rewarding
– Faster onset, more immediate reward
• e.g. parenteral administration
– Short duration of action: effect wears off quickly
– Tolerance leading to increased use
• Individual vulnerability• Availability

Neuroadaptation
Neuroadaptation is a core
neurobiological feature of addiction

Neuroadaptation
• The brain cells adapt to the chronic presence of a psychoactive drug, so that the person can function relatively normally when intoxicated (tolerance)– Involves a variety of cellular mechanisms– Need higher doses of the drug to get the
desired effect
• When substance use ceases, the person is then left in a state of imbalance (withdrawal).

Extent and nature of drug and alcohol problems

Global burden of disease
World Health Report 2002, WHO

Impact of substance misuse on health in Australia
Collins & Lapsley, NDS monograph 66, 2008
Impact of substance misuse in Australia, 2003• Alcohol
– Harmful levels of drinking accounts for 3.2% of Australia’s burden of disease
– Safe levels of drinking averts 0.9% of the total burden
• Deaths from alcohol and illicits often occur in younger people
• Tobacco accounts for 7.8% of the burden of disease (the greatest disease burden)
• Tobacco causes more deaths, but later in life
Begg et al, 2007, Australian Institute of Health and Welfare

Harm related to substance use
Psychosocial
Physical complications may be related to:
• the substance itself
• route of use e.g. IV injection
• dependence– Higher priority given to substance use
than health or diet– Malnutrition

Harm related to substance use
Social responsibilitiesRelationshipsFamilyOccupational
PersonalPhysical healthMental health
Legal

Social consequences
• Illicit nature– (high cost, crime, impurity, injecting in
unsafe places/manners)– Imprisonment in this population is as high
as 50%. (60% of prisoners are incarcerated for drug-related crime)

Social consequences
• Illicit
• Stigmatised– Alienation from parents, spouses and
children – Discrimination in workplace, health care– Stigma extends to those involved in D&A
services
Social consequences• Illicit• Stigmatised• Finance : $50-200 per day
– Involvement in crime (theft, dealing, importation)
– Prostitution– Homelessness and debt to unscrupulous
drug dealers predispose this group to becoming victims of violent crime.
– The combination of dependence and high cost may lead to anti-social behaviour (which is potentially reversible)
– Drained finances may lead to the loss of necessities of life in favour of drug procurement (which is an overpowering physical and psychological need)

Social consequences• Illicit
• Stigmatised
• Finance
• Intoxication – Inability to complete education or maintain
paid employment– user/parent unable to care for their children,
and family breakdown may result

Social consequences• Illicit
• Stigmatised
• Finance
• Intoxication
• Vulnerability– IDUs commonly also victims of crime:
homeless, intoxicated, disenfranchised

Medical complications
• Specific to drugs
• Related to injecting
• Contaminants

Physical harm from the substance itself
– Acute • intoxication (eg falls, motor
accidents, overdose, violence)• specific side effects (eg myocardial
infarction related to cocaine)
– Chronic• dependence• specific chronic effects (eg alcohol
related liver disease)
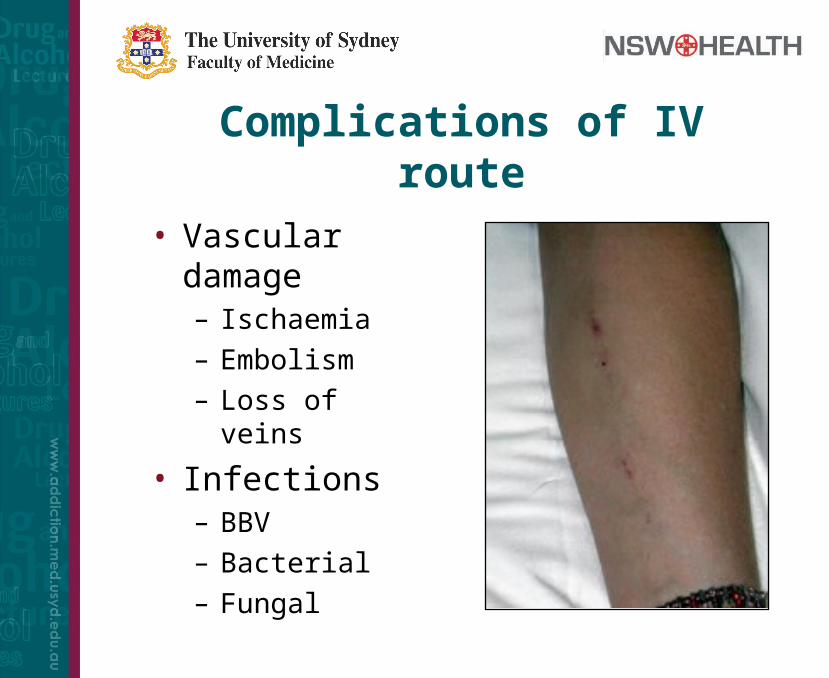
Complications of IV route
• Vascular damage– Ischaemia– Embolism– Loss of veins
• Infections– BBV– Bacterial– Fungal

Contaminants
A surprisingly uncommon cause of
illness
Recognised examples:• Lead poisoning (found in some
amphetamine preparations)
• Talc (used to “cut” drugs down; toxic to lung)

Why public health?• Public health refers to the health of
the community
• Prevention efforts must be directed to people who do NOT yet have the drug problem.– Interventions are directed to the
community, not just to affected people
• Drug-related harm is experienced by non-users and first-time users as well as habitual users

Two complementary approaches
• Reducing or stopping drug usePriority on cessation of drug use which will prevent all adverse effects
• ‘Harm reduction’Definition: refers to policies, programs, and practices that aim primarily to reduce the adverse health, social and economic consequences of the use of legal and illegal psychoactive drugs without necessarily reducing drug consumption. Harm reduction benefits people who use drugs, their families, and the community. (International Harm Reduction Association, 2009 www.ihra.net)

Reducing drug use: supply vs demand reduction
• Reducing drug use via reduced supply
• Border controls• Reducing production of drugs• Punishment of dealers
• Reducing drug use via reduced demand
• Education• Treatment of dependent users• Deterrence: e.g. imprisonment

The heroin drought 2000-2
What caused it?• Local police heroin hauls?• International factors: reduced exportation
from primary producers (Afghanistan war)
Effects• Increase in users presenting for treatment• Increase in alternative drug use (eg injected
temazepam, stimulants)– Ischaemic limbs– Stimulant induced psychosis
Harm reduction for IDUs
HIV prevalence in IDU – New York City up to 50%
– Sydney 1%
Estimates
• Lifetime cost of HIV care = $100,000
• Drug users in Australia = 100,000
• Potential total life-time cost in Australia = $10B!!
Harm reduction for IDUs• Needle Syringe Programs (NSPs)
• Non-injecting route of administration (NIROA)
• Peer-education regarding safe injecting
• Medically Supervised Injecting Centre (MSIC)
• Decriminalisation?
• May lead to safer routes of use and hence decrease the burden of disease and also decrease health costs in a ‘market’ economy
Needle Syringe Programs (NSP)
• Rapid outbreaks of HIV occur in cities with and without NSP
• In regions lacking NSP, IDU is a major mode of HIV transmission
• NSPs aim to provide enough sterile equipment for each occasion of IDU
• Cost of NSP is 1% of the cost of no NSP
Summary• Humans are fascinated by mind altering
experiences, and also use drugs to relieve suffering or anxiety
• Disorders of substance use may develop
• Personal, social and legal barriers limit drug use
• It is a challenge to develop rational and evidence based policies because of emotional and moral associations

Case study: returning to Lisa
• Upon further enquiry:– Lisa uses ecstasy at parties 2x a month– Alcohol typically 10 wines on Fridays
• Drug related harms:– Threatened with assault at a bar– Unwanted sex while intoxicated without
injury or pregnancy
• You advise Lisa– MDMA is illicit and pills are variable– Encourage to reduce alcohol intake

Contributors
Associate Professor Kate Conigrave
Royal Prince Alfred Hospital & University of
Sydney
Professor Paul Haber
Royal Prince Alfred Hospital & University of
Sydney
All images used with permission, where applicable
![Lesson 91 Muslims Suffering Harms. [21] Quraysh harms the Prophet, peace be upon him.](https://static.fdocuments.in/doc/165x107/56649cd05503460f9499c232/lesson-91-muslims-suffering-harms-21-quraysh-harms-the-prophet-peace-be.jpg)




![Canadian Substance Use Costs and Harms (2015-2017) [report] · Dr. Pamela Kent . Executive Summary 1 Overall Costs of Substance Use 1 Healthcare Costs 2 Lost Productivity Costs 3](https://static.fdocuments.in/doc/165x107/5fe3ff9e64829a61ad37d217/canadian-substance-use-costs-and-harms-2015-2017-report-dr-pamela-kent-executive.jpg)
![Canadian Substance Use Costs and Harms (2015-2017) [report]](https://static.fdocuments.in/doc/165x107/61ae54b60ca4aa7c2c6ad2d3/canadian-substance-use-costs-and-harms-2015-2017-report.jpg)











