Overview of Issues: Barriers to Developing EHR in This Field Constance Weisner, DrPH, MSW Jennifer...
23
Overview of Issues: Barriers to Developing EHR in This Field Constance Weisner, DrPH, MSW Jennifer Mertens, PhD Stacy Sterling, MSW, MPH Narrowing the Research-Practice Divide in Evidence-Based Medicine with Adoption of Electronic Health Record Systems: Present and Future Directions National Institute of Drug Abuse Rockville, MD July 13-14, 2009
-
Upload
priscilla-welch -
Category
Documents
-
view
219 -
download
0
Transcript of Overview of Issues: Barriers to Developing EHR in This Field Constance Weisner, DrPH, MSW Jennifer...

Overview of Issues: Barriers to Developing EHR in This Field
Constance Weisner, DrPH, MSWJennifer Mertens, PhD
Stacy Sterling, MSW, MPH
Narrowing the Research-Practice Divide in Evidence-Based Medicine with Adoption of Electronic Health
Record Systems: Present and Future Directions
National Institute of Drug AbuseRockville, MD
July 13-14, 2009

Overview
HistoryBarriers
Infrastructure Workforce Multiple system interaction Most programs are free-standing-not part of a
health plan/using the same EMR Privacy
Potential

National Policy Approach to Behavioral Health Care
Crossing the Quality Chasm’s
aims, rules, and strategies for
redesign should be applied
throughout Mental Health/Substance Use health
care on a day-to-day operational basis
tailored to reflect the
characteristics that distinguish
Mental Health /Substance Use health care from general
health care.
Institute of Medicine. Improving the Quality of Health Care for Mental and Substance-Use Conditions: Quality Chasm Series. Washington, DC: National Academies Press; 2006.
Six Critical Pathways for Achieving Aims
Effective use of information technology (IT) News ways of delivering care Managing the clinical knowledge, skills, and
deployment of the workforce Effective teams and coordination of care
across patient conditions, services and settings
Improvements in how quality is measured Payment methods conducive to good quality

M/SU Health Care Compared to General Health Care
Increased stigma, discrimination, & coercion
Patient decision-making ability not as anticipated / supported
Diagnosis more subjective
A less developed quality measurement & improvement infrastructure
More separate care delivery arrangements
Less involvement in the NHII and use of IT
More diverse workforce and more solo practice
Differently structured marketplace

Health Plans / Purchasers Recommendations (cont):
Require all contracting organizations to appropriately share patient information;
Provide incentives for the use of electronic health records and other IT;
Use tools to reduce adverse risk selection of M/SU treatment consumers; and
Use measures of quality and coordination of care in purchasing / and oversight.
Associations of purchasers work to reduce variation in reporting / billing requirements.

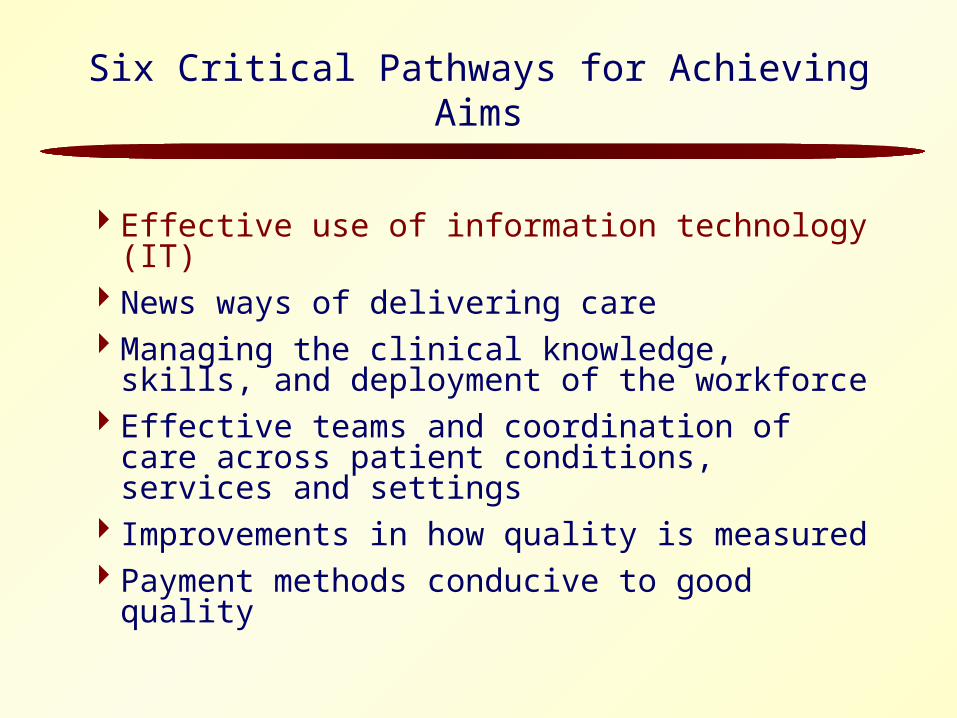
Characteristics of the Addiction Treatment System
13,200 specialty programs in US
• 31% treat less than 200 patients per year
• 65% private, not for profit
• 77% primarily government funded
Private insurance <12%
Sources – NSSATS, 2002; D’Aunno, 2004
11,600
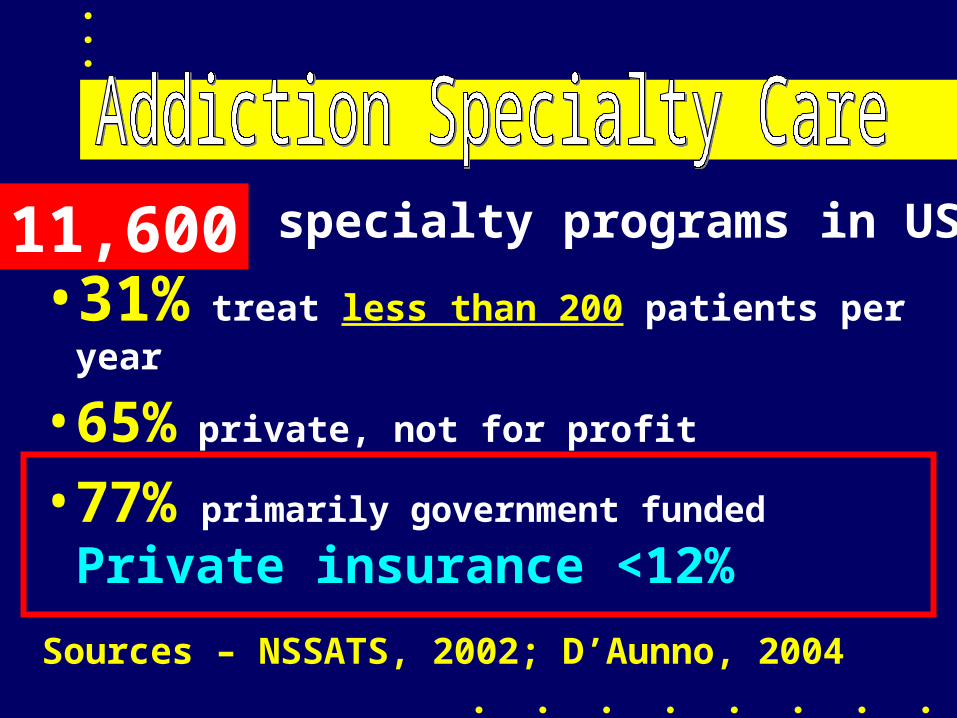
Source 1990 2008Criminal Justice 38% 61%
Employers/EAP 10% 6%
Welfare/CPS 8% 14%
Hosp/Phys 4% 3%
Referral Sources
Adolescent Treatment Referral Sources
Parents - 83%
Health care provider - 18%
Legal system - 33% (20% Court Mandated)
Friends - 19%
Mental health providers - 35%
Schools - 13%

Phone Interviews With National Sample of 175 Programs regarding personnel, management, information
McL, Carise & Kleber JSAT, 2003

• 12% had closed • 13% had changed service operation
• 31% of the rest had been taken over, usually by MH agencies
Program Changes In 16 Months:

• Counselor turnover 50% per year
• 50% of directors have been there Less Than 1 year
STAFF TURNOVER!
Other Staff
• 54% Had no physician 34% Had P/T physician39% Had a Nurse
• < 25% Had a SW or a Psychologist
• Major professional group - Counselors

• Modest Computer Availability– Mostly For Administrative Work– 80% Had a Computer – 50% had Web Access
• Still very little computer/software availability for CLINICAL STAFF
Information Systems:

Multiple System Interaction
Unique to behavioral health care: Most programs are free-standing collaborative care with:
Health systems Criminal Justice Welfare
Important issues for internal EMRs and cross-system communication
Should privacy regulations be the same for each system? Where the program is embedded?

Privacy
“Prevent disclosure of addiction treatment and diagnoses; also create barriers to accessing data and complicate coordination of care, especially with regard to EHRs and electronic networks.”(Institute of Medicine, 2006)
Privacy (cont’d)
Continuing CareStigmaVariation in clinical and patient concerns
Opportunities
Coordination with other systemsCommunication with patients Epidemiologic surveillanceOutcomes monitoring

Using Standardized Instruments at Intake and Follow-up


Conclusion
Barriers are large and involve characteristics of the treatment system, regulatory issues, workforce issues, and long-term work styles.
Opportunities are increasing and field is ready to grapple with these issues.

Thank you!