Overcoming Pitfalls in the Diagnosis of Bipolar...
67
Em ging Challenges in Prim y C e: 2016 Overcoming Pitfalls in the Diagnosis of Bipolar Disorder
Transcript of Overcoming Pitfalls in the Diagnosis of Bipolar...

Emerging Challenges in Primary Care: 2016
Overcoming Pitfalls in the Diagnosis of Bipolar
Disorder

Faculty
• Richard H. Anderson, MD, PhD Principal Partner, St. Charles Psychiatric Associates, Midwest Research Group Clinical Faculty, Washington University School of Medicine, Department of Psychiatry St. Louis, MO
2

Disclosures • Richard H. Anderson, MD, PhD serves as a speaker for Takeda
Pharmaceuticals.
3

Learning Objectives After participating in the proposed educational activities, clinicians should be better able to:
1. Recognize the the high prevalence of bipolar disorder in patients who experience depression
2. Describe the high rate of misdiagnosis of patients with BD
3. Develop a knowledge of the key criteria that differentiate unipolar depression from BD
4. Provide information and tools for successful screening and recognition of patients with BD
4

Pre-Test Questions
5

Pre-test ARS Question 1On a scale of 1 to 5, please rate how confident you would be in the diagnosis and management of a patient with Bipolar Disorder: 1. Not at all confident 2. Slightly confident 3. Moderately confident 4. Pretty much confident 5. Very confident
6

Pre-test ARS Question 2Which of the following is true regarding the high prevalence of Bipolar Disorder in patients who experience depression? 1. Bipolar I patients are symptomatic almost half their lives
2. Depressive episodes are indistinct between Major Depressive Disorder and Bipolar Affective Disorder in a depressed episode
3. In Bipolar Disorder, patients are asymptomatic close to half of the time
4. The most common variant episode of Bipolar disorder is the depressed state
5. All of the above
7

Pre-test ARS Question 3Which of the following is false in describing the high rate of misdiagnosis of patients with Bipolar Disorder?
1. The prevalence of bipolar disorder may be higher than previously estimated
2. 50% of individuals with positive screens for bipolar I or II disorders reported they had previously received a diagnosis of bipolar disorder from a physician
3. Up to 80% of patients who screen positive for bipolar disorder have not been previously diagnosed with bipolar disorder
4. The Mood Disorder Questionnaire (MDQ) is a validated screening instrument for Bipolar I and II disorders 88

Pre-test ARS Question 4In developing knowledge of the key criteria that differentiate unipolar depression from Bipolar Disorder, is the following statement true or false?
“Depression is the initial symptom reported by the majority of patients with bipolar disorder”.
1. True
2. False
9

Pre-test ARS Question 5Which of the following statements regarding the recognition and initial management of Bipolar Disease is false?
1. Treatment of Bipolar Depression requires starting antidepressants first at illness onset to reduce suicidal risk and improve social adjustment, then adding a mood stabilizer once the depressive symptoms begin to improve
2. Bipolar disorder is most frequently misdiagnosed as unipolar depression
3. It takes up to 10 years before being accurately diagnosed in many BD patients
4. Antidepressants, in the absence of mood stabilizers, may induce mania or hypomania and worsen the course of bipolar disorder by accelerating cycling frequency
10

Primary Care Practitioners
§ They are the backbone of America’s mental health care system, providing a larger percentage of mental health care services than specialists in mental and addictive disorders
§ In many communities, they are the only professionals with mental health care training
Norquist GS, Regier DA (1996), Annu Rev Med 47:473-479 11

Stigma of Mental Health Diagnosis§ The public identifies mental illnesses with violence
and danger, which trigger the desire to maintain social distance from these patients1
§ The patient’s perception and concern about stigma are associated with greater impairment in social functioning with persons outside of the family circle, but not with family members2
§ Greater concern about stigma is associated with greater severity of mental disorder
§ Patient withdrawal from society in response to concerns with stigma
§ Absence of close or confiding relationships is associated with greater risk of relapse or nonremission among individuals with depression
121Link BG et al. (1999), Am J Public Health 89(9):1328-1333; 2Perlick DA et al. (2001), Psychiatr Serv 52(12):1627-1632

Patient Access to Mental Health CareSocioeconomic status plays a role in patient access to mental health treatment
§ The highest rates for bipolar disorder diagnosis are among the poorest respondents (annual income <$20,000)
§ Majority of the participants who screened positive for bipolar disorder are not previously diagnosed by a healthcare professional, although they sought professional help for these symptoms and had been previously diagnosed with another mental health condition
§ Poor patients are less likely to receive mental health care and, if they do, are comparatively less likely to receive treatment from a mental health specialist
13Das AK et al. (2005), JAMA 293(8):956-963

Potential Consequences of Unfocused Treatment
§ Antidepressant monotherapy may worsen disease course § Creation of mania or mixed states § Accelerated mood cycling
§ More suicide attempts § More hospitalizations § More comorbidities § Greater psychosocial impairment § Greater healthcare costs
Goldberg JF, Ernst CL (2002), J Clin Psychiatry 63(11):985-991; Goldberg JF, Truman CJ (2003), Bipolar Disord 5(6):407-420
14

Bipolar Disorder: Untreated vs. Treated
Standardized Mortality RatiosZurich Cohort (N=406)
1959-1997
*p<0.001; †p<0.05; Angst F et al. (2002), J Affect Disord 68(2-3):167-181
0
5
10
15
20
25
Neoplasm Cardio- vascular
Cerebro- vascular
Accidents Suicide Other All Causes
Untreated
Treated
29.2*
6.4
1.4* 0.6 2.2* 1.7 1.6† 1.3 1.6 2.0 2.0* 1.3 2.2* 1.3 S
tand
ardiz
ed M
orta
lity
R
atio
15

Need for Improved Recognition
16

Positive Mood Disorder Questionnaire for Bipolar Disorder in the Community
Neither Bipolar Disorder Nor Depression Diagnosis
Diagnosed With Bipolar Disorder
Diagnosed With Depression, But Not Bipolar Disorder
49%
20%
31%
80% of Patients Who Screened Positive for Bipolar Disorder Had Not Been Diagnosed With Bipolar Disorder*
N=85,358 participants (3.7% screened positive for BD); *49% (neither BD nor depression diagnosis) + 31% (diagnosed with depression but not bipolar disorder); Hirschfeld RM et al. (2003), J Clin Psychiatry 64(1):53-59; Hirschfeld RM et al. (2003), J Clin Psychiatry 64(2):161-174 17

Underrecognition of Bipolar Disorder in Patients in a General Medicine Clinic
Patients Screened While Seeking Primary Care
10%
10% screened positive for lifetime history of BD
N=1,146; Das AK et al. (2005), JAMA 293(8):956-963
Depression, but Not BD Was
Most Common Diagnosis
79.5%
18
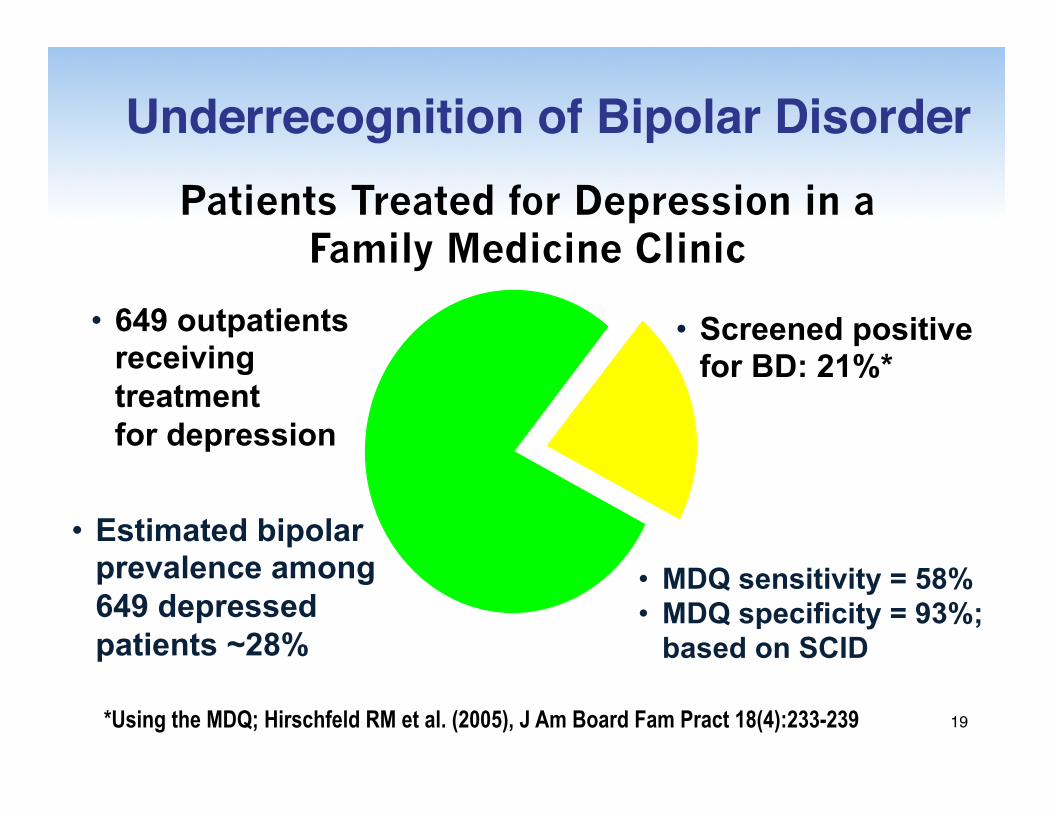
Underrecognition of Bipolar Disorder
• Screened positive for BD: 21%*
*Using the MDQ; Hirschfeld RM et al. (2005), J Am Board Fam Pract 18(4):233-239
• Estimated bipolar prevalence among 649 depressed patients ~28%
• MDQ sensitivity = 58% • MDQ specificity = 93%;
based on SCID
Patients Treated for Depression in a Family Medicine Clinic
• 649 outpatients receiving treatment for depression
19

Patients With BD-I Are Symptomatic Almost Half Their Lives
N=146 patients followed every 6 months over 2-20 years; Mean follow-up = 12.8 years; Judd LL et al. (2002), Arch Gen Psychiatry 59(6):530-537
Weeks Depressed
Weeks Asymptomatic
Weeks Cycling/Mixed Weeks
Manic/Hypomanic
NIMH Collaborative Depression Study
53% 32%
9% 6%
20

Percent of Time Patients With BD-II Have Depressive Symptoms
Judd LL et al. (2003), Arch Gen Psychiatry 60(3):261-269
• 86 patients followed every 6 months over 13.4 years
NIMH Collaborative Depression Study
Asymptomatic 46%
Depressed 51% Hypomanic 1%
Cycling/Mixed 2%
21

Hypomania
Mania
Depression
Euthymia
Depression
Subsyndromal Depression P
olar
ity
of S
ympto
ms
Longitudinal Assessment of Bipolar Disorder Is Critical
22

Bipolar Hypomanic Episode
HS = hora somni (bedtime); Manning JS et al. (1999), Psychiatr Clin North Am 22(3):689-703
Escalating Irritability
Euthymic Mood
Hypersomnic, Retarded
Depression
Hypersomnic, Retarded
Depression
1-3 Days Modal Duration
• Increased mental/physical activity
• Decreased need for sleep • Talkative and/or distinctly
more social • Mood irritable or elated • Tendency for impairment
of social judgment • No adequate cause for
symptoms • Labile • Recurrent
a.m. HS a.m. HS
23

Screening—From the General to the More Specific
24

Whom Do I Screen for Bipolar Disorder?
§ Patient types§ Every person with depressed mood§ Every person with generalized anxiety
disorder§ Persons with behavioral disruptions§ Persons with history of substance abuse
§ FDA health advisory§ Screen for bipolar disorder before initiating
antidepressant treatmentFDA Public Health Advisory (2004). Available at: www.fda.gov/cder. Accessed June 2, 2006
25

Helpful Mnemonics to Assist Clinicians in the Identification of Mental Health Problems
§ SOAP: problem-oriented medical record
§ BATHE: general psychosocial assessment
§ SIG E CAPS: diagnosis of depression§ DIGFAST: symptoms of hypomania/
mania26

SOAP: Problem-Oriented Medical Record§ Subjective—the patient’s stated reason
for the visit to the clinician§ Objective—the findings (e.g., physical,
laboratory, imaging) immediately prior to, at the time of or following a visit
§ Assessment—what is the clinician’s overall determination of the patient’s status based on the information obtained in the 2 previous steps?
§ Plan—what the clinician proposes to do regarding the patient’s situation
Weed LJ (1971), Ann Clin Res 3(3):131-134
27

Percentage of Physical Complaints With Identified vs. Unidentified Organic Causes
Over a 3-Year Period
0
2
4
6
8
10
Kroenke K, Mangelsdorff AD (1989), Am J Med 86(3):262-266
3-Y
ear
Inci
den
ce (
%)
No organic cause identified
Organic cause identified
28

The BATHE Technique§ Background: “What is going on in your
life?”
§ Affect/feeling: “How do you feel about that?”
§ Trouble: “What about that troubles you (most)?”
§ Handling: “How are you handling that?”
§ Empathy: “That must be very difficult” Stuart MR, Lieberman JA (2002), The Fifteen Minute Hour: Practical Therapeutic Interventions in Primary Care, 3rd ed. Philadelphia: Saunders Stuart MR, Lieberman JA (2002), The Fifteen Minute Hour: Practical Therapeutic Interventions in Primary Care,
3rd ed. Philadelphia: Saunders 29

Detection of Depression§ 2 questions § In the past 2 weeks, have you often
been bothered by feeling down, depressed or hopeless?
§ In the past 2 weeks, have you often been bothered by having little interest or pleasure in doing things?
§ A “yes” to either or both questions is a positive screen for depression
Pignone MP et al. (2002), Ann Intern Med 136(10):765-776 30

SIG E CAPS(“Prescribe Energy Capsules”)
Wise MG, Rundell JR (1994), Concise Guide to Consultation Psychiatry, 2nd ed. Washington, D.C.: American Psychiatric Press, pp55-56
31

Wise MG, Rundell JR (1994), Concise Guide to Consultation Psychiatry, 2nd ed. Washington, D.C.: American Psychiatric Press, pp55-56
SIG E CAPS • S—increased or decreased sleep and sexual desire • I—decreased interest or pleasure in almost all
activities • G—inappropriate guilt or feelings of worthlessness/
hopelessness • E—decreased energy or fatigue • C—decreased concentration • A—increased or decreased appetite, with weight
gain or loss • P—psychomotor agitation or retardation • S—suicidal ideation, plan or attempt
32

SIG E CAPS (Cont.)§ If a patient has ≥5 positive
responses, at least 1 of which is either depressed mood or anhedonia, for ≥2 weeks, and this represents a change from previous behavior, then he/she meets DSM-IV criteria for major depressive disorder
Wise MG, Rundell JR (1994), Concise Guide to Consultation Psychiatry, 2nd ed. Washington, D.C.: American Psychiatric Press, pp55-56
33

DIGFAST:Symptoms of Hypomania and Mania
• Distractibility: poorly focused, multitasking • Insomnia: decreased need for sleep • Grandiosity: inflated self-esteem • Flight of ideas: complaints of racing thoughts • Activities: increased goal-directed activities • Speech: pressured or more talkative • Thoughtlessness: “risk-taking” behaviors—
sexual, financial, travel, driving Ghaemi SN (2001), Primary Psychiatry 8:28-34 34

Criteria for Manic Episode• Elevated, expansive or irritable mood lasting ≥1 week (or any duration if hospitalization is required)
• Plus: ≥3* of the following symptoms: § Inflated self-esteem/grandiosity § Decreased need for sleep § Overly talkative (pressured speech) § Racing thoughts/flight of ideas § Distractibility § Increased activity/agitation § Excessive involvement in high-risk pleasurable
activities *For predominantly irritable mood, 4 or more symptoms needed for diagnosis; APA (2000), Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision. Washington, D.C.: American Psychiatric Publishing, Inc. 35
Diagnosis of Bipolar Disorder§ Is it just depression?
§ Is your depressed patient bipolar?
§ Not all depression is unipolar
§ 1/3 of bipolar disorder in the general population is misdiagnosed as unipolar depression
§ Unipolar depression is a diagnosis of exclusion
Hirschfeld RM et al. (2003), J Clin Psychiatry 64(2):161-174 36

Why Does It Matter if Bipolar Disorder Is Misdiagnosed?
APA (2002), Am J Psychiatry 159(4 Suppl):1-50; Frye MA et al. (2004), Depress Anxiety 19(4):199-208 37

When Are Symptoms of Depression Part of Bipolar Disorder Rather Than Unipolar
Disorder?
• In a survey of 600 patients with BD, more than 1/3 sought help within 1 year of symptom onset § 69% were not diagnosed with BD—most
frequent diagnosis was major depression § Mean number of physicians consulted before
correct diagnosis: 4 § 1/3 did not receive a BD diagnosis for 10
years Hirschfeld RM et al. (2003). J Clin Psychiatry 64(2):161-174
38

Differential Diagnosis: Unipolar or Bipolar?
1. Family history • Higher rates of psychiatric
illness • Positive for bipolar disorder 2. Course of illness
• Age of 1st mania/ depression
• Duration of episodes
• Frequency of episodes
• Seasonality
3. Treatment response • Multiple treatment
failures • Nonresponse or erratic
response to antidepressants
4. Mania symptoms • Distractibility • Insomnia • Grandiosity • Flight of ideas
• Activities • Pressured speech • Thoughtlessness
Key Elements
5. Associated features • Unevenness in
intimate relationships • Frequent career
changes • Substance use
disorders
39

Unipolar Bipolar
Sometimes Common Postpartum depression
Absent Common Mixed depression/hypomania/mania
Unusual Common Rapid on/off pattern
Less Common Common Antidepressant “misadventures”
Less Common More Common Highly recurrent depression
Occasional Common Seasonality
Sometimes Very common 1st episode <25 years
Sometimes Common Family history loaded for mood disorders
Moderate Very high Substance abuse
Kaye NS (2005), J Am Board Fam Pract 18(4):271-281
Unipolar vs. Bipolar Depression
40

Diagnosing Unipolar vs. Bipolar Disorder: The Critical Role of Past History
§ Presenting symptoms do not tell the whole story § Ask the patient about:
§ Past (hypo)manic symptoms, including overactivity as well as euphoric or irritable mood
§ Impulsive behaviors, divorce/separation, job changes § Medication-response history
§ Multiple antidepressant failures? § Apparent rapid recovery? § Insomnia on antidepressants?
§ Family history of mood disorders § Bipolar disorder may be progressive
APA (2002), Am J Psychiatry 159(4 Suppl):1-50; Akiskal HS et al. (2000), J Affect Disord 59 (suppl 1):S5-S30; Angst J et al. (2003), Eur Neuropsychopharmacol 13(suppl 2):S43-S50; Katzow JJ et al. (2003), Bipolar Disord 5(6):436-442; Stahl SM (2005), PsychEd Up 1(8):6-7; Frye MA et al. (2004), Depress Anxiety 19(4):199-208
41

Diagnosing Unipolar vs. Bipolar Disorder:The Critical Role of Outside Observers
N=600; Hirschfeld RM et al. (2003), J Clin Psychiatry 64(2):161-174
62
21
57
19
37
40
35
38 % Reporting
% Not reporting
0 10 20 30 40 50 60 70 80 90
100
Mania
Heightened Mood
Increased Activity
Depression
Prolonged Sadness
Loss of Energy
% E
xper
ienc
ing
Sym
pto
m
Patients Underreport Manic Symptoms
42
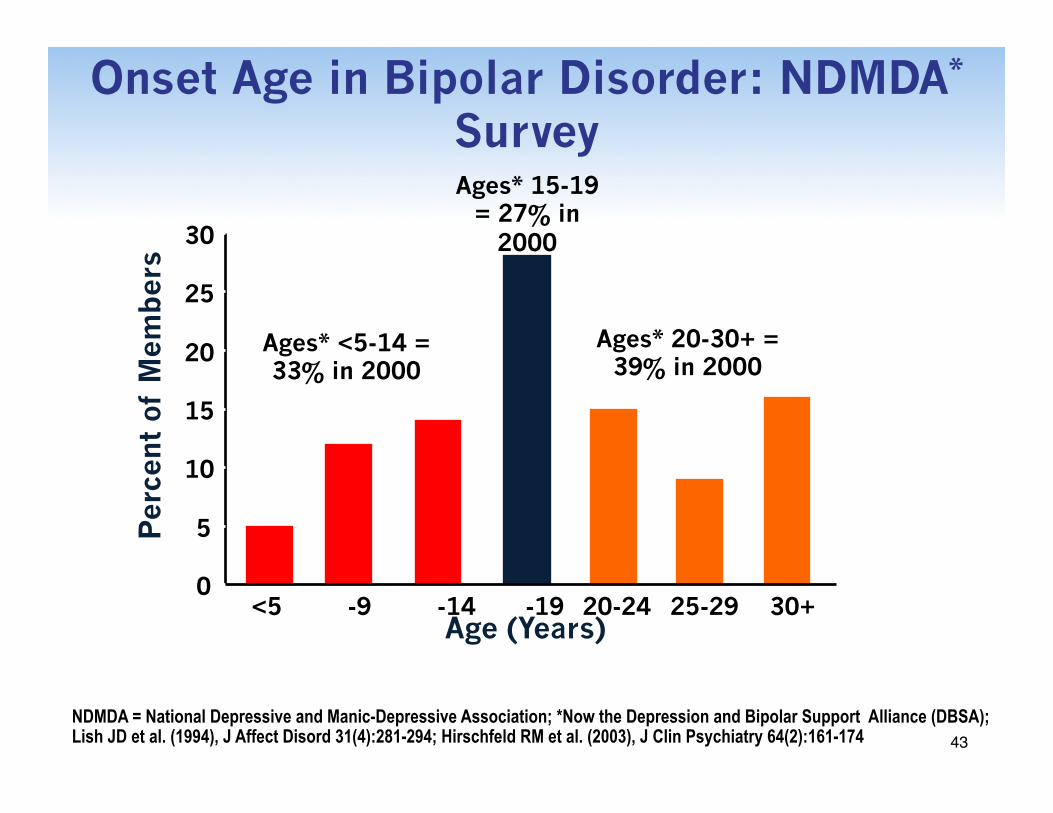
Onset Age in Bipolar Disorder: NDMDA* Survey
NDMDA = National Depressive and Manic-Depressive Association; *Now the Depression and Bipolar Support Alliance (DBSA); Lish JD et al. (1994), J Affect Disord 31(4):281-294; Hirschfeld RM et al. (2003), J Clin Psychiatry 64(2):161-174
Ages* 15-19 = 27% in
2000
Per
cent
of
Mem
ber
s
Age (Years) 10-14 15-19 20-24 25-29 30+ <5 5-9
0
5
10
15
20
25
30
Ages* <5-14 = 33% in 2000
Ages* 20-30+ = 39% in 2000
43

Tools for Diagnosing Unipolar vs. Bipolar Disorder Correctly
§ Can use patient health questionnaire (PHQ-9) as a screening tool for symptoms of depression
§ Cannot tell if depressive symptoms are part of a unipolar depression episode or bipolar disorder without also explicitly asking about current or past (hypo)manic symptoms
§ Can use MDQ as a screening tool for bipolar disorder
§ Additional tools § Bipolar Spectrum Diagnostic Scale (BSDS) § Hypomania Checklist (HCL-32)
Kroenke K et al. (2001), J Gen Intern Med 16(9):606-613; PHQ-9, Available at: www.pfizer.com/pfizer/download/do/phq-9.pdf. Accessed May 16, 2006; Akiskal HS et al. (2000), J Aff Disord 59(suppl 1):S5-S30; Angst J et al. (2003), Eur Neuropsychopharmacol 13(suppl 2):S43-S50; Hirschfeld RM et al. (2000), Am J Psychiatry 157(11):1873-1875; MDQ, Available at: www.psycheducation.org/PCP/launch/MDQlaunch.htm. Accessed May 16, 2006 44
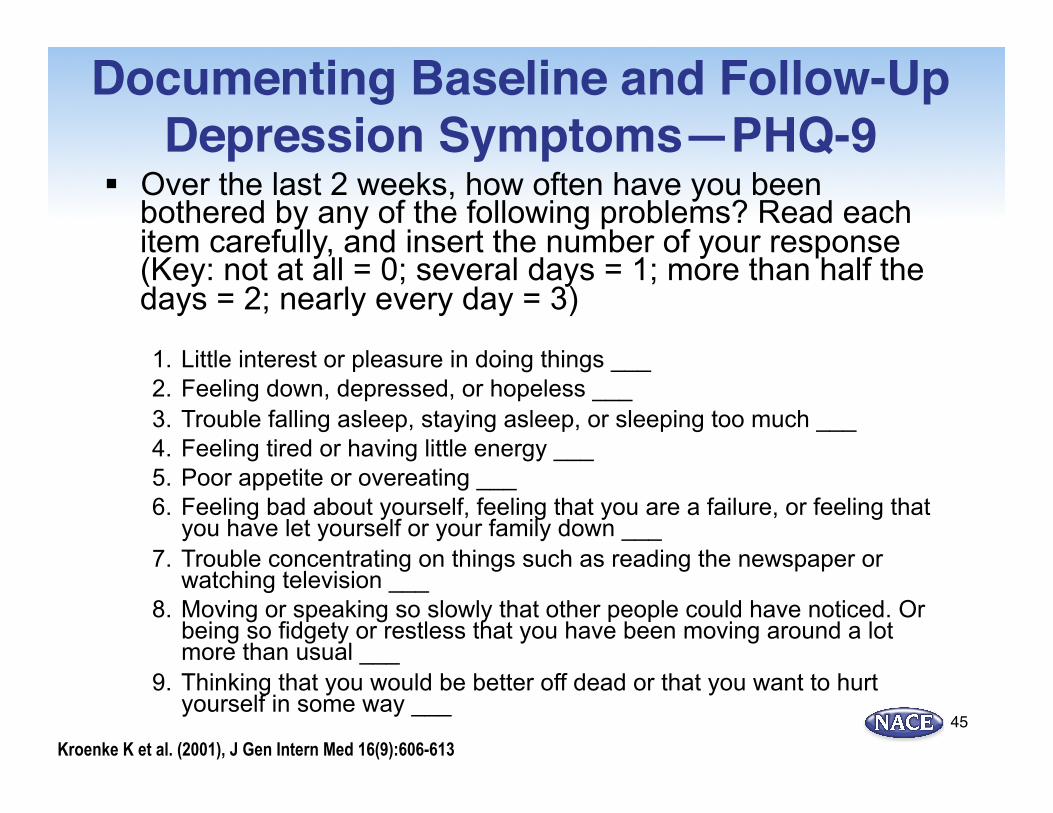
Documenting Baseline and Follow-Up Depression Symptoms—PHQ-9
§ Over the last 2 weeks, how often have you been bothered by any of the following problems? Read each item carefully, and insert the number of your response (Key: not at all = 0; several days = 1; more than half the days = 2; nearly every day = 3)
1. Little interest or pleasure in doing things ___ 2. Feeling down, depressed, or hopeless ___ 3. Trouble falling asleep, staying asleep, or sleeping too much ___ 4. Feeling tired or having little energy ___ 5. Poor appetite or overeating ___ 6. Feeling bad about yourself, feeling that you are a failure, or feeling that
you have let yourself or your family down ___ 7. Trouble concentrating on things such as reading the newspaper or
watching television ___ 8. Moving or speaking so slowly that other people could have noticed. Or
being so fidgety or restless that you have been moving around a lot more than usual ___
9. Thinking that you would be better off dead or that you want to hurt yourself in some way ___
Kroenke K et al. (2001), J Gen Intern Med 16(9):606-613 45

Documenting Baseline and Follow-Up Depression Symptoms—PHQ-9 (Cont.)§ Total score for questions 1-9: ____ § Scoring key: minimal <5; mild 5-9; moderate
10-14; moderately severe 15-19; severe >19 § Impairment: if you checked off any problem on
this questionnaire so far, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people? § Key: not difficult at all = 0; somewhat difficult
= 1; very difficult = 2; extremely difficult = 3
Kroenke K et al. (2001), J Gen Intern Med 16(9):606-613 46

Screening Tool:Mood Disorder Questionnaire
Hirschfeld RM et al. (2000), Am J Psychiatry 157(11):1873-1875 47

Mood Disorder Questionnaire§ Patients answer “yes” or “no” to a series of questions
§ Has there ever been a time in your life when you were not your usual self and (while not using drugs or alcohol?—13 questions
§ If you checked “yes” to more than one of the above, have several of these ever happened during the same period of time?
§ How much of a problem did any of these cause—like being unable to work; having family, money or legal troubles; getting into arguments or fights?
§ Family history of mood disorders and substances abuse
§ Has a health professional ever told you that you have manic-depressive illness or bipolar disorder?
Hirschfeld RM et al. (2000), Am J Psychiatry 157(11):1873-1875; MDQ, Available at: www.psycheducation.org/PCP/launch/MDQlaunch.htm. Accessed May 16, 2006
48

Criteria for a Positive MDQ Screen
§ A positive screen§ Requires 7 or more “yes” responses § Symptom co-occurrence and moderate-to-
severe functional impairment as rated by the patient
§ The level of functional impairment due to symptoms is queried on a 4-point scale, ranging from “no problem” to “serious problem”
Hirschfeld RM et al. (2000), Am J Psychiatry 157(11):1873-1875 49

Hypomania Checklist
01020304050607080901st Qtr2nd Qtr3rd Qtr4th QtrEastWestNorth
§ Self-administered inventory to help clinicians diagnose BD-II and minor bipolar disorders
§ 32 yes/no items used to identify hypomanic component in patients with depressive episodes
§ Designed to assess personal and social role consequences of hypomanic symptoms
§ Takes into account the subjects current overall affective status as a potentially interfering variable in answering the questions
§ Can reveal the extent to which the patient has insight into the condition 50

Bipolar Spectrum Diagnostic Scale
01020304050607080901st Qtr2nd Qtr3rd Qtr4th QtrEastWestNorth
§ Scale to identify BD-II and NOS conditions § Validated self-rating scale
§ For entire bipolar spectrum § Supplement to clinician’s semi-structured interview § 2 sections
§ Part I: a paragraph with 19 positively identified sentences (describing many of the symptoms of BD) followed by an underline space for participants to place a checkmark if it applies to them
§ Part II: 1 multiple choice question asking subjects to rate how well the paragraph describes them overall
51

When There’s Not a Lot of Time:3 Key Questions To Ask
01020304050607080901st Qtr2nd Qtr3rd Qtr4th QtrEastWestNorth
• How is your sleep? How much sleep do you require?
• How have you responded to antidepressants in the past?
• Do you have a family member with a mood disorder? Also Seek a Caregiver’s Perspective
• Remember the importance of seeking the comments of the patient’s relative or caregiver
52

Comorbidities: The Rule, Not the Exception
01020304050607080901st Qtr2nd Qtr3rd Qtr4th QtrEastWestNorth
The Multidimensionality of BD
McIntyre RS et al. (2004), Hum Psychopharmacol 19(6):369-386
Comorbidities: Medical Psychiatric
53

Lifetime Substance Use Comorbidity in BD
*Stimulants, sedatives, hallucinogens, opiates; THC = δ-9-tetrahydrocannabinol; McElroy SL et al. (2001), Am J Psychiatry 158(3):420-426
01020304050607080901st Qtr2nd Qtr3rd Qtr4th QtrEastWestNorth
0
10
20
30
40
50
Any SUD EtOH THC Cocaine Others* Pat
ient
s W
ith
BD
Aff
ecte
d
(%)
54

Suicide Risk Factors in BD§ Early age at disease onset§ High number of depressive episodes
§ Comorbid alcohol abuse§ History of antidepressant-induced mania
§ Family history of suicidal behavior§ Traits of hostility and impulsivity
Slama F et al. (2004), J Clin Psychiatry 65(8):1035-1039; Michaelis BH et al. (2004), Suicide Life Threat Behav 34(2):172-176 55

Suicide Lethality Risk: Unipolar vs. Bipolar Patients
N=2,395; Raja M, Azzoni A (2004), J Affect Disord 82(3):437-442
� Patients with BD are 6x more likely to make a highly lethal suicide attempt than unipolar patients
Unipolar Bipolar
60
40
20
0
56

Candidates for Consultation or Referral
§ Diagnostic uncertainty or dilemma
§ Treatment refractory
§ Acuity/severity § Danger to self/others mandating inpatient
status § Need for intensive outpatient therapy
§ Patient-provider mismatch § Clinician or patient preference
Jackson WC (2005), Drug Benefit Trends 17(Suppl A):17-22 57

Obstacles to Consultation and Referral
§ Availability§ Provider scarcity§ Long waiting times
§ Negative stigmatization§ Patient perceptions§ Provider perceptions
§ Co-management§ Legal issues§ Care coordination
§ Financial§ Reimbursement
rates§ Carveouts§ Others
58

Potential Benefits of Shared Care� Patient
§ Intensity of focus on a complex illness § Open communication between primary care
and mental health care providers
� Referring provider § Learning through focused questions to experts § Building relationships
� Consultant § Interaction of mental and general medical
care providers 59

Summary§ Symptoms of depression can be due to
major depressive disorder or to bipolar disorder
§ An accurate diagnosis can be made by taking a history not only of current symptoms, but also of past symptoms, and by getting additional information from family members
§ Diagnostic screening tools can help make a diagnosis 60

Summary (Cont.)
§ 1/3 of bipolar disorder in the general population is misdiagnosed as unipolar depression
§ Unipolar depression is a diagnosis of exclusion
§ An awareness of cultural variability with affective disorders is critical in the clinical setting
Hirschfeld RM et al. (2003), J Clin Psychiatry 64(1):53-59; Das AK et al. (2005), JAMA 293(8):956-963 61

Post-Test Questions
62
Post-test ARS Question 1Which of the following is true regarding the high prevalence of Bipolar Disorder in patients who experience depression? 1. Bipolar I patients are symptomatic almost half their lives
2. Depressive episodes are indistinct between Major Depressive Disorder and Bipolar Affective Disorder in a depressed episode
3. In Bipolar Disorder, patients are asymptomatic close to half of the time
4. The most common variant episode of Bipolar disorder is the depressed state
5. All of the above
63

Post-test ARS Question 2Which of the following is false in describing the high rate of misdiagnosis of patients with Bipolar Disorder?
1. The prevalence of bipolar disorder may be higher than previously estimated
2. 50% of individuals with positive screens for bipolar I or II disorders reported they had previously received a diagnosis of bipolar disorder from a physician
3. Up to 80% of patients who screen positive for bipolar disorder have not been previously diagnosed with bipolar disorder
4. The Mood Disorder Questionnaire (MDQ) is a validated screening instrument for Bipolar I and II disorders 64

Post-test ARS Question 3In developing knowledge of the key criteria that differentiate unipolar depression from Bipolar Disorder, is the following statement true or false?
“Depression is the initial symptom reported by the majority of patients with bipolar disorder”.
1. True
2. False
65

Post-test ARS Question 4Which of the following statements regarding the recognition and initial management of Bipolar Disease is false?
1. Treatment of Bipolar Depression requires starting antidepressants first at illness onset to reduce suicidal risk and improve social adjustment, then adding a mood stabilizer once the depressive symptoms begin to improve
2. Bipolar disorder is most frequently misdiagnosed as unipolar depression
3. It takes up to 10 years before being accurately diagnosed in many BD patients
4. Antidepressants, in the absence of mood stabilizers, may induce mania or hypomania and worsen the course of bipolar disorder by accelerating cycling frequency
66

Post-test ARS Question 5On a scale of 1 to 5, please rate how confident you would be in the diagnosis and management of a patient with Bipolar Disorder: 1. Not at all confident 2. Slightly confident 3. Moderately confident 4. Pretty much confident 5. Very confident
67