How Companies are using StratApps Analytics to Outsmart Competition

OUTSMART HF: A Randomized Controlled
Trial of Routine Versus Selective Cardiac
Magnetic Resonance in Non-Ischemic
Heart Failure (IMAGE-HF project 1B)
Paterson I, Erthal F, Garrard L, Mielniczuk L, O'Meara E, White
J, Connelly K, Knuuti J, Radja M, Laine M, Chow B, Chen L,
Wells G, Ezekowitz J, Beanlands R, Chan K
Mazankowski Alberta Heart Institute, University of Alberta, Edmonton, AB, Canada; Ottawa Heart Institute, Ottawa, ON, Canada;
Université de Montréal, Montreal, QC, Canada; University of Calgary, Calgary, AB, Canada; University of Toronto, Toronto, ON,
Canada;. Turku University, Turku, Finland; Dalhousie University, Halifax, NS, Canada; Helsinki University, Helsinki, Finland.

Disclosures
Peer Review Funding
– Canadian Institutes for Health Research
– TEKES, the Finnish funding agency for Technology and Innovation
Industry Funding
– Speaker honoraria/consultant fees: none
– Unrestricted grant: General Electric (<$10K)
ACC.18, LBCT, March 12, 2018

Background
• Non-ischemic heart failure (HF) is highly prevalent and world-
wide has overtaken ischemic HF
• Management of non-ischemic HF is complex given multiple
potential etiologies, with many having specific therapies
• Bedside and echocardiographic assessments do not reliably
distinguish non-ischemic subtypes
ACC.18, LBCT, March 12, 2018

Background
• Cardiac Magnetic Resonance (CMR) is increasingly used to
characterize non-ischemic cardiomyopathies but at increased cost
and lower availability compared to echocardiography
• ACC/AHA and ESC guidelines provide a class I-IIa recommendation
for CMR in patients with HF however level of evidence is C
ACC.18, LBCT, March 12, 2018

Primary Aim
• In patients with non-ischemic HF, determine if a strategy using
routine CMR yields more specific diagnoses of the underlying
HF etiology compared to a strategy using CMR selectively
Design
• Randomized, controlled multi-centre trial
• Two arm, 1:1 allocation routine versus selective CMR in
patients with non-ischemic HF
• Analyzed as intention to treat
OUTSMART-HF: Routine versus
selective cardiac magnetic resonance
in non-ischemic heart failure
ACC.18, LBCT, March 12, 2018Paterson et al. Trials 2013.

Halifax
Quebec City
Montreal
Ottawa
Toronto (SBHC, SMHC)
London
Edmonton
Calgary
Vancouver
OUTSMART-HF Sites
March 12, 2018
CanadaFinland
Turku
Helsinki
Kuopio
ACC.18, LBCT, March 12, 2018

Eligibility
Inclusion
• newly diagnosed HF or patients with established HF and
deterioration/decompensation within the past 12 months
• working diagnosis of either non-ischemic cardiomyopathy (any LVEF) or
heart failure with preserved ejection fraction (HFPEF)
• NYHA class II-IV HF symptoms within the last 12 months
Exclusion
• prior CMR and no change in clinical condition
• previous well-documented specific HF etiology
• significant CAD; previous STEMI or non-STEMI in LAD territory
• advanced HF with ongoing need for supportive therapy
• life expectancy < 3 months
• contraindication to CMRACC.18, LBCT, March 12, 2018

OUTSMART-HF Design Overview
ACC.18, LBCT, March 12, 2018
R
Eligible
patient
with non-
ischemic HF
Echo +
Routine CMR
*suspicion of ARVC, infiltrative, congenital, or pericardial disease
3mo 12mo
Echo +
Selective CMR*
Phase 2:
IMAGING ASSESSMENT
Phase 1:
CLINICAL ASSESSMENT
Phase 3:
CLINICAL ASSESSMENT
Baseline HF Etiology Imaging-based HF etiology Clinical HF etiology

Potential HF Etiologies
• Inflammatory
• Infiltrative
• Hypertrophic
• Ischemic
• Valvular
• Mixed
• Other
• Dilated
• HFPEF
• Unknown
Paterson et al. Trials 2013.ACC.18, LBCT, March 12, 2018
Clinical and Imaging Assessments
Specific HF etiology
Non-specific HF etiology

Primary Outcome
• Clinical Assessment of HF etiology at 3 months follow-up
Secondary Outcomes
• Imaging Assessment of HF etiology
– Routine CMR arm: CMR interpretation used
– Selective CMR arm: Echo interpretation used unless CMR performed
– Post-hoc analysis of HF etiology for CMR vs Echo in Routine arm
• Clinical events (death or cardiovascular hospitalization)
– Routine vs. Selective CMR
– Post-hoc Specific vs. Non-specific HF etiology
Paterson et al. Trials 2013.ACC.18, LBCT, March 12, 2018
Outcomes

Sample Size Estimation
Based on a study of patients with non-ischemic HF
which found that endomyocardial biopsy improved
specific diagnosis from 35% to 50%
Assumed
• specific HF etiology rate of 50% in routine and 35% in
selective CMR strategies
• two proportions will be compared based on the Chi-
square test (Z test) with a pooled variance estimate
• 90% power, two-sided alpha = 0.05
• 10% loss to follow-up or study withdrawal
• Total of 504 patients (252 patients per arm)ACC.18, LBCT, March 12, 2018
Felker et al. N Engl J Med 2000.

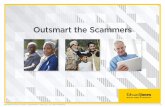
IMAGE-HF Project 1BPatients Randomized
13 sites, n = 518
ACC.18, LBCT, March 12, 2018
Echo + Routine CMR n=249 Echo + Selective CMR n=251
4 - Withdrew consent
1 - Admin withdrawal
4- site withdrawal*
3 - Withdrew consent
2 - Admin withdrawal
4 - site withdrawal*
3 month follow-up n=248 3 month follow-up n=250
2 -Lost to follow-up
8 - Death
1 - patient withdrawal
12 month follow-up n=236
4 - Lost to follow-up
7 - Death
1 - Incomplete follow up
12 month follow-up n=239
1 - Lost to follow-up1 - patient withdrawal
n=258 n=260
Recruitment from January 2011 – October 2016
*1 site withdrawn – unable to meet protocol requirements n = 8
CONSORT DIAGRAM

Baseline Patient Characteristics
Routine CMR Selective CMR
Age (years), mean±SD 59±13 58±14
Male 174 (70%) 170 (68%)
Hypertension 133 (53%) 132 (53%)
Diabetes mellitus 62 (25%) 70 (28%)
Myocardial Infarction 14 (6%) 10 (4%)
Atrial fibrillation 59 (24%) 66 (26%)
NYHA class: I
II
III
IV
9 (4%)
108 (44%)
100 (40%)
31 (13%)
10 (4%)
112 (45%)
110 (44%)
18 (7%)
SBP, mean±SD 122±20 123±22
HR, mean±SD 84±20 85±22
LVEF (%) , mean±SD 29±12 29±15
Creatinine (umol/L) , mean±SD 94±28 94±26
ACC.18, LBCT, March 12, 2018

Routine CMR Selective CMR
Beta blockers 217 (87%) 217 (87%)
ACE Inhibitors/ARB 212 (85%) 209 (83%)
MRAs (Spironolactone) 85 (34%) 96 (38%)
Diuretics 169 (68%) 175 (70%)
Nitrates 28 (11%) 21 (8%)
Digoxin 35 (14%) 39 (16%)
Anticoagulants 90 (36%) 111 (44%)
ASA/Other anti-platelet 118 (47%) 108 (43%)
Ca blockers 22 (9%) 34 (14%)
Antiarrhythmics 18 (7%) 18 (7%)
ACC.18, LBCT, March 12, 2018
Baseline Medications

Baseline Clinical Assessment
of HF Etiology
Routine CMR Selective CMR P value
HFPEF 18 (7%) 17 (7%)
Dilated 137 (55%) 136 (54%)
Inflammatory 12 (5%) 13 (5%)
Infiltrative 2 (1%) 3 (1 %)
Hypertrophic 2 (1%) 0
Ischemic 2 (1%) 3 (2%)
Valvular heart disease 1 (0.4%) 2 (1%)
Mixed 15 (6%) 9 (4%)
Other 58 (23%) 64 (26%)
Unknown 2 (1%) 3 (1 %)
Specific HF Etiology* 92 (36.9%) 95 (38.0%) 0.88
ACC.18, LBCT, March 12, 2018
*Specific = Inflammatory, Infiltrative, Hypertrophic,
Ischemic, Valvular, Mixed or Other

ACC.18, LBCT, March 12, 2018
R
Eligible
patient
with non-
ischemic HF
Echo +
Routine CMR
*suspicion of ARVC, infiltrative, congenital, or pericardial disease
Baseline HF etiology Echo +
Selective CMR*
Phase 2:
IMAGING ASSESSMENT
Phase 1:
CLINICAL ASSESSMENT
Imaging Tests Performed
Echo (N=249)
CMR (N=224)
Echo (N=249)
CMR (N=54)
However only 3/54 performed
per protocol (2 infiltrative and
1 ACHD)

Imaging Assessment
of HF Etiology
ACC.18, LBCT, March 12, 2018
Routine
CMR
Selective
CMRP value*
Selective CMR
Per ProtocolP value*
HFPEF 16 (6%) 17 (7%) 19 (8%)
Dilated 134 (54%) 135 (54%) 151 (60%)
Inflammatory 20 (8%) 12 (5%) 2 (1%)
Infiltrative 6 (2%) 3 (1%) 2 (1%)
Hypertrophic 4 (2%) 1 (0.4%) 1 (0.4%)
Ischemic 8 (3%) 20 (8%) 22 (9%)
Valvular heart disease 2 (1%) 8 (3%) 7 (3%)
Mixed 17 (7%) 14 (6%) 10 (4%)
Other 18 (7%) 12 (5%) 16 (6%)
Unknown 14 (6%) 24 (10%) 16 (6%)
No heart failure 10 (4%) 4 (2%) 4 (2%)
Specific HF Etiology 85 (34.1%) 73 (29.7%) 0.27 65 (25.7%) 0.04
* compared to Routine CMR

HF Etiology by Imaging Test
(Paired Analysis in Routine CMR)
CMR Echo P value
HFPEF 11 (5%) 21 (9%)
Dilated 122 (55%) 149 (67%)
Inflammatory 20 (9%) 2 (1%)
Infiltrative 6 (3%) 3 (1%)
Hypertrophic 4 (2%) 1 (0.5%)
Ischemic 5 (2%) 17 (8%)
Valvular heart disease 1 (0.5%) 1 (0.5%)
Mixed 17 (8%) 8 (4%)
Other 17 (8%) 11 (5%)
Unknown 11 (5%) 9 (4%)
No heart failure 10 (5%) 2 (1%)
Specific HF Etiology 80 (35.7%) 45 (20.1%) < 0.001
ACC.18, LBCT, March 12, 2018

0
10
20
30
40
50
60
70
80
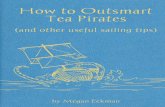
Baseline 3 month 12 month
Routine CMR Selective CMR
PRIMARY OUTCOME
Clinical Assessment of
Specific HF Etiologies
(%)
ACC.18, LBCT, March 12, 2018
P=0.14P=0.24
P=0.81
P<0.001
PRIMARY OUTCOME

Clinical Outcomes
(Death or CV hospitalization)
Routine vs. Selective CMR
ACC.18, LBCT, March 12, 2018
P =0.27

Clinical Outcomes
(Death or CV hospitalization)
CLINICALLY assigned (3 month)
Specific vs. Non-specific HF etiology
IMAGING assigned
Specific vs. Non-specific HF etiology
ACC.18, LBCT, March 12, 2018
P =0.65P =0.02

Limitations
• No standardized definitions for HF etiologies
• Abundance of non-protocol CMR in selective strategy
• Limited use of quantitative T1 and T2 mapping on CMR
ACC.18, LBCT, March 12, 2018

Conclusions
In patients with non-ischemic HF,
• No difference in the clinical diagnosis of specific HF etiology
between routine and selective CMR strategies
• However more specific HF etiologies were identified by routine
CMR at the time of image assessment
– CMR identified more specific HF etiologies compared to echo alone
• No difference in event-free survival between routine and
selective CMR arms
ACC.18, LBCT, March 12, 2018

Conclusions
• Patients with specific HF etiologies defined on imaging had
worse outcomes than those with non-specific diagnoses
• However there was no difference in event-free survival between
specific and non-specific diagnoses determined clinically
ACC.18, LBCT, March 12, 2018

Interpretation
In patients with non-ischemic HF,
• CMR increases specific imaging diagnoses but does not change
specific clinical diagnoses
• Imaging based diagnoses enables stratification of risk whereas
clinically defined diagnoses do not
• Greater attention to use of CMR and HF diagnoses from
imaging in general should be considered
ACC.18, LBCT, March 12, 2018

OUTSMART HF Team• Edmonton, Canada
• I. Paterson, J. Ezekowitz
• Coordinators: M. Irwin
• Ottawa, Canada
• B.J.W. Chow, R.S. Beanlands, L. Mielniczuk, C. Dennie, A. Dick, L.
Duchesne
• Coordinators: E. Moga, M. Mohammed, V. MacKellar
• Montreal, Canada (Montreal Heart Institute)
• E O’Meara, J-C Tardif
• Coordinators: H. Brown, M. Dardes
• Toronto, Canada (Sunnybrook)
• G. Wright, K. Connelly
• Coordinator: M. Li
• Quebec City, Canada (Laval)
• E. Larose, P. Pibarot
• Coordinator: K. Bibeau
• Toronto, Canada (St. Michael’s)
• K. Connelly, M. Freeman, H. Leong-Poi
• Coordinator: J. Sloninko
• Halifax, Canada
• M. Rajda, H. Brown
• Coordinators: J. Kelly, S. Yarn
• Calgary, Canada
• J. White, A. Howarth
• Coordinators: S. Rivest
• Vancouver, Canada
• J. Leipsic, M. Kiess
• Coordinators: E. Grieve, L. Miklosova
• Turku, Finland
• J. Knuuti, H. Ukkonen, H. Leskinen
• Coordinators: T. Vasankari, K. Lahtonen
•
• Kuopio, Finland
• J. Hartikainen, M. Hedman
• Coordinator: L. Kujanen
• Helsinki, Finland
• M. Laine, H. Hanninen
• Coordinator: C. Salmen
• IMAGE-HF Data & Coordinating Centre
• L. Garrard, RN, BScN
• A Guo, MSc
• G. A. Wells, PhD (Research and Methods)
• L. Chen, PhD
• ML. Tran, MSc
•
• Quality Assurance
• Rob deKemp, PhD
• O. Clarkin, PhD
• I. Paterson, MD, F. Erthal (CMR)
• K. Chan, MD (IEcho)
March 12, 2018
ACC.18, LBCT, March 12, 2018

3 month HF Etiology
Routine CMR Selective CMR
HFPEF 16 (7%) 12 (5%)
Dilated 118 (49%) 111 (45%)
Inflammatory 14 (6%) 15 (6%)
Infiltrative 2 (1%) 4 (2%)
Hypertrophic 2 (1%) 2 (1%)
Ischemic 7 (3%) 8 (3%)
Valvular heart disease 4 (2%) 4 (2%)
Mixed 17 (7%) 8 (3%)
Other 61 (25%) 79 (32%)
Unknown 1 (0.4%) 1 (0.4%)
No heart failure 1 (0.4%) 3 (1.2%)
Specific HF etiology* 108 (44.4%) 123 (49.8%)
ACC.18, LBCT, March 12, 2018
P=0.24
*Specific = Inflammatory, Infiltrative, Hypertrophic,
Ischemic, Valvular, Mixed or Other

Routine CMR Selective CMR
HFPEF 13 (6%) 9 (4%)
Dilated 112 (48%) 98 (42%)
Inflammatory 14 (6%) 15 (6%)
Infiltrative 1 (0.4%) 2 (1%)
Hypertrophic 1 (0.4%) 2 (1%)
Ischemic 8 (3%) 9 (4%)
Valvular heart disease 4 (2%) 4 (2%)
Mixed 19 (8%) 7 (3%)
Other 62 (26%) 81 (34%)
Unknown 1 (0.4%) 3 (1%)
No heart failure 1 (0.4%) 6 (3%)
Specific HF etiology* 110 (46.6%) 126 (53.4%)
ACC.18, LBCT, March 12, 2018
12 month HF Etiology
P=0.14
*Specific = Inflammatory, Infiltrative, Hypertrophic,
Ischemic, Valvular, Mixed or Other