Outpatient Breastfeeding Champion Course Lecture Notes
87
Outpatient Breastfeeding Champion Course Lecture Notes March 2021
Transcript of Outpatient Breastfeeding Champion Course Lecture Notes

Outpatient Breastfeeding Champion Course
Lecture Notes March 2021

3/7/2021
1
The OutpatientBreastfeeding
Champion Program
1
• The Instructor has no conflicts of interest to disclose
• Nursing credits, continuing education recognition points (CERPs) for IBCLE, or CPEUs for registered dietitians, are awarded commensurate with participation and complete/submission of the evaluation form.
What is the IABLE?
• Non-profit
• Establish Outpatient Breastfeeding-Knowledgeable Health Systems and Communities
• Provide free breastfeeding education for supporters
– Case discussion series 2nd Sunday of each month
– Clinical Question every 2 weeks
– Free videos on Youtube, Vimeo
– Breastfeeding education handouts
– Breastfeeding Medicine Podcast Series
3
Your Learning Materials
• Powerpoint Slides• All lectures in the course are
based on the slides
• Curriculum Book• Excellent reference guide as a
Breastfeeding Champion
• Has the same information as the slides, but structured organized differently
• All references for the course are in the curriculum book
Your Triage Tools and Breastfeeding Education Handouts
• All triage tools are printed in your curriculum book• In the back, after the green divider page
• Also available electronically in your IABLE dashboard• Can be copied and pasted into the electronic record
• There are many more triage tools than the ones we cover in class
• Triage tools can be shared with colleagues at your institution
Objectives for the Outpatient Breastfeeding Champion (OBC)• Breastfeeding
resource person at work– Colleagues, other
staff
• Education, counseling, and support for clients/patients
• Breastfeeding promotion
6

3/7/2021
2
Ideas for OBC Roles
• Phone triage
• Weight checks the first week
• Hospital visits
• Nurse visits
• Phone check-ins
• Congratulation program
• Office support groups
• Touch base at well child checks
• Educate coworkers 7
Scope of Practice
Your job description may not allow you to apply this knowledge or set of skills in practice
Knowledge that you cannot apply can be helpful in giving guidance to mothers about what they can expect from their care with a lactation consultant.
Every Participant Here Today:
• Understands that people in this course may never have breastfed and/or may have had trauma related to breastfeeding
• Brings valuable knowledge and experiences to share
• Is encouraged to respect each other’s identities and stories
• Is doing the best to listen with their heart
Session 1Breastfeeding
Basics
10
OBC Session 1 Topics
• Special Properties of Human Milk• The Entero-mammary Pathway• Risks of not breastfeeding• Contraindications to breastfeeding• Breastfeeding Demographics• Healthy People 2030 goals• Barriers to Breastfeeding• Prenatal Counseling• Counseling the Breastfeeding Mother
11
Objectives for Session 1
• Recite 3 components of breastmilk that provide immunologic protection from illness.
• Recite how antibodies directed against pathogens enter mother’s milk.
• Identify 6 infant risks of not breastfeeding and 2 maternal risks of not breastfeeding.
• Explain current recommendations on duration of breastfeeding.
• Recite 3 contraindications to breastfeeding.• Identify 4 ways that pregnant mothers can be supported to
breastfeed.• Describe how to demonstrate empathy, respect and
support for breastfeeding parents
12

3/7/2021
3
13
WaterProteinCarbsDHA/ARAFatVitaminsMinerals
WaterProteinCarbs
DHA/ARAFat
VitaminsMinerals
Comparing Breastmilk and Formula = Comparing Apples and Oranges
PLUS:Hormones AntibodiesActive white cellsEnzymesAnti-viral proteinsAntibacterial agents
Human MilkFormula
++OligosaccharidesAnti-allergy factorsCarotenoidsProtaglandinsCytokinesPeptidesEtc!!!
15
Formula is not evilThere are times that formula is essential
Infants are at Risk
16
Immature immune system at birth
High risk for infection
Breastmilk ✓ Protects from
infection✓ Promotes brain
and immune system maturity
✓ Reduces inflammation
✓ Optimal nutrition
Lets Look at Examples of How Human Milk Alters the Infants’
Immune System and Metabolism
Human Milk Oligosaccharides

3/7/2021
4
Breastmilk Factor Interleukin-7 keeps the thymus larger in breastfed infants, until weaning, improving infant immunity
Breastfed Children have less Risk of Obesity
Possible Reasons:✓Differences in metabolism✓Hormones in breastmilk✓Bfed infants drink smaller
volumes
Examples of Super-Heroes in Breastmilk
21
Antibodies in Breastmilk Attack
Viruses and Bacteria
FE
FE
FE
FE
Lactoferrin
Lysozyme
Lactadherin
Macrophages Haptocorrin
OligosaccharidesMucins
Casein

3/7/2021
5
Entero-Mammary Circulation of Antibodies
25
What do you know are benefits of breastfeeding for children (or risks of not breastfeeding)?
AllergiesAsthmaEczema
Anti-Inflammatory
Severe bacterialinfectionsEar infectionsGastroenteritis
Anti-Infective
Hormonal
Lower insulin levelsLess diabetesLess obesity
Immune-Modulating
Certain cancersArthritis
Higher IQRetinal maturity
Brain maturity
Neurological
Safety
Decreased SIDSImproved bonding
27
Special Properties of Breastmilk
What do you know are benefits of breastfeeding for mothers (or risks of not breastfeeding)?
Relaxation and
Bonding
Maternal Benefits
29
Not Breastfeeding?
• Risks of infant formula
– Bacterial contamination
• Cronobacter sakazakii
– Other contaminants
• Bug parts
• Metals
– Absence of nutrients
• Environmental risks
– Waste
• Packaging30

3/7/2021
6
Usbreastfeeding.org © IABLE 3232
• Exclusive bfeeding until 6 mo
• Add solids at 6 mo
• Nurse at least until 2 yrs
World Health Organization,
American Academy of Family Physicians
• Exclusive bfeeding until about 6 mo
• Add solids at around 6 mo
• Continue for at least 1 year or as long as desired
American Academy of Pediatrics
• Exclusive bfeeding for 6 mo
• Continue for 1 year or longer
American College of Obstetrics and
Gynecology
Infant Illnesses RequiringMore Evaluation Before
Breastfeeding
• Galactosemia type 1- cannot breastfeed
• Other metabolic illnesses infants can partially breastfeed, e.g.
– PKU
– Maple syrup urine disease
33
Maternal Relative Contraindications to
Breastfeeding
• HIV
• Herpes on nipple/breast
• Shingles on nipple/breast
• A few meds, mainly chemotherapy
• Most drugs of abuse
34
2018 Center for Disease Control National Breastfeeding Report Card
Healthy People 2030National Breastfeeding Goals
• Increase the proportion of infants who are breastfed exclusively through 6 months of age to 42.4%• Was 24.9 % in 2018
• Increase the proportion of infants who are breastfed at 1 year to 54.1%• Was 35.9% in 2018

3/7/2021
7
Which individuals are more likely to breastfeed? Least likely?
2016 Breastfeeding Rates at 6 Months by Race/Ethnicity
2016 Breastfeeding Rates at 6 Months by Poverty Level 2016 Breastfeeding Rates at 6 Months by Urban/Rural Living
2016 Breastfeeding Rates at 6 Months by Marital Status 2016 Breastfeeding Rates at 6 Months by Education Level

3/7/2021
8
2016 Breastfeeding Rates at 6 Months by Maternal Age
What do you think are barriers to initiating breastfeeding, that can be addressed
prenatally?
Educational Barriers to
Breastfeeding
Failure of Counseling by Medical Offices:
➢ risks of not breastfeeding
➢ lack of educational materials
➢ no encouragement to take a class
45© IABLE 46
Socio-Cultural Barriers to Breastfeeding
– Social conventions
• Not nursing in public
• Bottle as the norm
– Lack of family/social support
– Racial/ethnic barriers
• Few resources from one’s culture/race
Employment Barriers
• Lack of support in the work place
– Fair Labor Standards Act on Break time for Nursing Mothers
• Job stress47
Breastfeeding Challenges for the Lactating Parent
Who is Back to Work
• Childcare
• Changes in the infant’s feeding behavior
• Effect on lactation
48

3/7/2021
9
© IABLE 49
Medical Deterrents to Breastfeeding
• Painful breastfeeding
• Low milk production
• Excessive milk production
49
• Parental depression
• Breast reduction
• Parental illnesses and medication
© IABLE 50
Strategies for Prenatal Support
© IABLE 51
Verbalizing Support
• Verbalize support
• Start with an open-ended conversation
– How do you plan to feed your baby?ACOG- Optimizing Support for Breastfeeding As Part of Obstetric Practice
Opinion #658 2016
Address Barriers
– Identify mom’s perceived barriers
–Consider a prenatal counseling session• Getting off to a great start
• Breastfeeding plan52
© IABLE 53
PrenatalCounseling
• Inform all pregnant patients re the risks to formula feeding
• Avoid worry of instilling guilt
• No need to exert pressure or coercion
ACOG- Optimizing Support for Breastfeeding As Part of
Obstetric PracticeOpinion #658 2016 Photo by Mulyadi on Unsplash
Prenatal Lactation
Consultation• History of breastfeeding problems
– Recurrent mastitis– Low milk supply– Recurrent plugs– Sudden drop in supply– Pump problems
• Anticipated possible breastfeeding challenges– Medications– H/o breast cancer, breast surgery– Medical illnesses, ie rheumatoid– Upcoming medical procedures
postpartum
54

3/7/2021
10
Need for Prenatal Education
• Prenatal breastfeeding class
• Give educational resources
– IABLE resource handout
• Discuss employment concerns
55Source: US Breastfeeding Committee
Prenatal Toolkits- Free!
• ACOG
– https://www.acog.org/About-ACOG/ACOG-Departments/Toolkits-for-Health-Care-Providers/Breastfeeding-Toolkit
• Wisconsin Dept of Public Health/WIC- 15 Cards
– https://www.dhs.wisconsin.gov/nutrition/breastfeeding/education.htm
• Minnesota Bfeeding Coalition Prenatal Toolkit
– https://mnbreastfeedingcoalition.org/prenatal-toolkit-2/
• Read-Set- Baby Carolina Global Health Institute– https://sph.unc.edu/cgbi/resources-ready-set-baby/
56
IABLE
Socioeconomic Barriers
• Encourage partner/family members to join the pregnant parent for prenatal education, or for a prenatal visit
• Refer to WIC if financial concerns re breastfeeding
• Advocate for pts with employment barriers
Create a Breastfeeding-
Competent Environment Where
You Work
• NO gift packs of formula
• Provide tips for success during prenatal visits
• Close follow-up after hospital discharge
58
Creating a Breastfeeding
Competent Environment
• Comfortable place for individuals to nurse
• Visual messages that normalize breastfeeding
• Address breastfeeding concerns
• Provide community resources/support groups
• Support breastfeeding employees
59
Source: US Breastfeeding Committee
Counseling Lactating Parents and Families
60

3/7/2021
11
Parent-Centered Approach to Counseling
61
• Begin with introductions in the room
• Start with an upbeat comment
• Make sure language is understandable– Avoid technical terms
– Interpreter as needed
– Speak clearly, not fast
– Avoid over-explaining62
Identifying Concerns
• Make a list of breastfeeding concerns
• If long, ask the parent(s) to identify most important concerns
• Allow the parents to use their own words to explain concerns
63
Source: United States Breastfeeding Committee
Counseling Worksheet In Small Groups
Parent-Centered Approach to Counseling Worksheet
• What are her concerns?• What are her goals?• How can you demonstrate to her that you are
listening?– Verbal cues– Nonverbal cues
• What can you say to demonstrate empathy?– Show respect– Comment on her strengths– Express support
64
Shared Decision Making
• Outline options for managing the breastfeeding concern. Include risks and benefits to each:– She can continue to pump and bottle feed
– She can nurse, then give a bottle of formula and not pump at all
– Only pump after nursing when someone is with her
• Provide realistic encouragement– Will this improve?
– When will it improve?
65
Ending the Visit and Follow-up
➢ Recap➢ Ask the parent to recite what the plan is➢ Provide written instructions, or a video conversation
from her phone➢ Plan a follow-up➢ Phone, text, office, home visit? When? 66

3/7/2021
12
Conclusions Session 1
• There are many immune factors in breastmilk other than antibodies that provide optimal health for the baby.
• There are very few contraindications to breastfeeding.
• Individuals are encouraged to nurse for at least 1-2 years.
• Medical offices and other systems that work with breastfeeding dyads need to provide breastfeeding encouragement, education and support prenatally.
67
Conclusions Session 8 Cont’d
• Identifying mother’s concerns and goals will help with shared decision making.
• Demonstrating listening skills can be done in verbal and nonverbal ways.
• Empathy can be expressed as respect, support, and demonstrating understanding.
68
A new mom calls at 3 mo postpartum, stating that she will be going back to work next week, and she does not think she would be able to swing working and breastfeeding. She wonders if there are still advantages to nursing past 3 months. You advise:
69
A. Once you start solid food at 6 months, breastfeeding really does not matter anymore.
B. Your baby will benefit from breastfeeding for the first year and beyond.
C. Continuing to nurse, even if you need to supplement, is preferred over weaning.
D. It would be better to wean now, since working and breastfeeding will be too hard.
E. B & C
Mom calls with symptoms of the stomach flu and asks if she should stop nursing. You advise:
A. Keep nursing, but if the baby becomes sick with vomiting and diarrhea, stop nursing.
B. Keep nursing, and if the baby becomes ill, continue to breastfeed and call your doctor’s office to discuss further management.
C. Stop nursing to prevent spreading your illness, and give your baby either stored breastmilk or formula until you feel fine.
70
A pregnant individual calls and wonders if they should not nurse because they have diabetes, asthma and allergies. You
advise:
A. Since you might need various medications for your illnesses, it would be less complicated if you formula feed.
B. Your baby would have lower risks of these illnesses if you nurse your baby.
C. If you nurse for just 4 months, your baby will get all of the protection he needs from breastfeeding.
D. You should not nurse because your blood sugars will become too out-of-control.
71
Breastfeeding helps to prevent all of the following except:
A. Severe pneumonia in the infant.
B. Childhood obesity in the infant.
C. Ear infections in the infant.
D. Breast cancer in the mother.
E. Certain pediatric cancers.
F. Gastro-esophageal reflux in the infant.
72

3/7/2021
13
Breastfeeding is considered appropriate in which situation?
A. Maternal hepatitis B and C
B. Infant galactosemia type 1
C. Maternal chemotherapy for cancer treatment
D. Maternal use of heroin
73
Mom calls, concerned that her baby just turned 1 year old. The baby still likes to nurse, but she thought she had to wean at 1 year. She wonders what to do. You
advise:
74
A. Babies should really wean to cows milk because it is healthier. Breast milk is less nutritious after 1 year.
B. It is natural to keep nursing beyond 1 year, and your toddler will be healthier if you continue to nurse.
C. It is OK to keep nursing but you should never nurse your toddler at night.
D. It is best to wean because nursing toddlers tend to reject solids, so they don’t get all of their nutrients.

3/7/2021
1
© 2020 IABLE
The OutpatientBreastfeeding
Champion Program• The Instructor has no conflicts of interest to disclose
• Nursing credits, continuing education recognition points (CERPs) for IBCLE, or CPEUs for registered dietitians, are awarded commensurate with participation and complete/submission of the evaluation form.
© 2020 IABLE . 3
OBC Session 2
• Anatomy and Physiology
• Positioning for breastfeeding
• Infant Latch
• Defining a feeding
• Feeding Frequency and Duration
• Infant and Maternal signs of Adequate Milk Intake
© 2020 IABLE . 4
Session 2 Objectives
• Describe breast anatomy and hormones of milk production and release.
• Describe and demonstrate 4 typical positions used when breastfeeding.
• Identify 3 signs that indicate adequate breastmilk intake in the baby and effective feeding in the mother.
© 2020 IABLE 5
alveolus
lobule
Lactiferous duct
fat
© 2020 IABLE 6
Montgomery gland
Areola
NippleTypically 2-7 pores

3/7/2021
2
© 2020 IABLE 7 © 2020 IABLE 8
Alveoli in a lobule
Ducts
© 2020 IABLE 9 © 2020 IABLE 10
Estrogen
Progesterone
Human Placental Lactogen
Prolactin
Growth Hormone
Fibroblast Growth Factor
Insulin-like Growth Factor
Parathyroid hormone related protein
Hormones Affecting Breast Growth
Thyroid hormone
© 2020 IABLE 11
LactogenesisIn Pregnancy
Ache and
grow
Breast tissue growth and
development
Increase in protein,
lactose, Ig,Leaky,
Breasts may continue to
grow
© 2020 IABLE 12
Placenta is delivered
Placental hormones diminish
Pituitary & Breast tissue seize control

3/7/2021
3
© 2020 IABLE 13 © 2020 IABLE . 14
Prolactin
• Released from anterior pituitary
• Stimulates breasts to produce milk
• Requires nipple stimulation
• Prolactin level ≠ Amount of milk
© 2020 IABLE
What do you think raises the prolactin level higher- breastfeeding or pumping?
15© 2020 IABLE . 16
Oxytocin• Released by posterior
pituitary
• Stimulates milk ejection
• Several let-downs occur during a nursing session
• Tingly/tight sensation
© 2020 IABLE
What Causes the Milk Ejection (Letdown) to Occur?
17
The Multiple Triggers of Milk Letdown by Oxytocin
Seeing the baby
Hearing the baby
Holding/touching the baby
Smelling the baby
Thinking about the baby

3/7/2021
4
Red Flags for Breastfeeding Problems
No Breast Growth During
Pregnancy
History of Breast Surgery (Esp Reduction)
History of Breast Radiation
History of Low Production
Certain Meds Known to Impair Production © 2020 IABLE 20
©IABLE
Positioning at the Breast is
KEY for:
• Deep Latch• Maternal Comfort• Effective Milk Transfer
21
Source: United States Breastfeeding Committee© 2020 IABLE 22
Maternal Comfort
and Support
Proper Alignment
Mouth Wide Open
Firm, Secure Hold
Nose to Breast
Positioning Tips for Optimal LatchFirm Secure Hold
24

3/7/2021
5
Proper Alignment
Source: USBC
Maternal Comfort and Support
Mouth Open Wide Nose to Breast
© 2020 IABLE 29
Sitting in Lap Facing Mom;Mom is using aC-Hold
© IABLE 29 © 2020 IABLE 30
Semi-Reclined (laid back)Positioning
Global Health Media

3/7/2021
6
© 2020 IABLE . 31
Let’s Practice Positioning
• Cradle
• Cross Cradle
• Football
• Laid-back
• Side lying
• Sitting Upright
© 2020 IABLE . 32
What is a Feeding?• The baby latches on and nurses
– Transfer of milk
• Easy to fool everyone– Some infants sleep at the breast
• Proof is in the weight gain
© 2020 IABLE . 33
Teach Parents to Understand a FeedingNutritive vs Non-nutritive Feeding
• Nutritive feeding transfers milk– Swallows are seen/heard– Slower (~1 suck per
second), rhythmic– Wider jaw excursions
• Non-nutritive– Faster– Smaller jaw excursions– NO swallowing
Best Feedings Include Swallows!!
© IABLE 34
Sit with Parents to Teach Nutritive and Non-Nutritive Sucking
• Watch the infant feed on the first breast, and point out swallows
• As the infant relaxes, and there have been NO swallows for 3-4 minutes, switch infant to the other breast. No need to wait for the infant to unlatch on their own
• Point out swallows on the second side
• Once swallows are done for 3-4 minutes on the second side, OK to take infant off the breast
• If infant is still hungry, start the process over on the first, then the second breast
• Nursing on both sides twice is called Switch Nursing
© 2020 IABLE
What do you think determines the length of the feeding at the breast?
35
Duration of Feeding at the Breast, in the Early Weeks, is Determined by:
Infant wakefulness
Low Production
High Production
VS
Infant maturity/strength
Faster Feeding When:
✓ Awake✓ Alert✓ Strong✓ Fast flow, such as with
high production
Slower Feeding When:✓ Sleepy✓ Premature✓ Weak✓ Low/slow flow such as with
low production

3/7/2021
7
© 2020 IABLE . 37
Infants Need to Feed Frequently the First Few Weeks
• Every 2-3 hours until at birth wt– Wake to feed
• OK to feed ad lib when:– Back to birth wt
– Gaining well
– Wakes up to eat on their own
© 2020 IABLE
What factors do you think determine how often an infant feeds (once feeding
is well established)?38
© 2020 IABLE . 39
What Determines How Often an Infant Feeds? (After the First Few Weeks, When Gaining Well)
Infant Hunger✓ A hungry infant may feed more often✓ Feeding frequency drives production
Parental Response to Cues
✓ Parent may or may not identify early cues✓ Sleep training reduces night time feeds
✓ Parents may not wake up infant for daytime feeds
Volumes Taken at Feeds ✓ High milk production allows larger feeds less often✓ Infants’ feeding volume preferences vary
Infant Behavior✓ Infant may nurse for comfort, when
upset/tired/ill
© 2020 IABLE . 40
Cluster Feeding Happens for Many Reasons
• Normal behavior in first 3-4 mo– Very often in evening– When babies are most
awake
• Infant illness– Seeking comfort– Taking less
volume/feeding
• Low production– Cluster feeding will
increase production
© 2020 IABLE 41
Typical Feeding Frequency and Duration
Age (mo) Frequency (~) Duration
1-3 mo 1.5-3 hours 20-30+ minutes
4-6 months 2-5 hours 5-15+ minutes
6-9 months 3-5 hours 5-15+ minutes
9-12 months 4+ times a day 5-10+ minutes
Toddlers Anyone’s guess Less than 10+ min
© 2020 IABLE . 42
Daytime Variation in Milk Production
• Highest production overnight
– prolactin rises overnight
• Lowest in the evening
– May lead to evening supplementation
Nightime
Daytime
Evening
Prolactin Levels over 24 hours

3/7/2021
8
© 2020 IABLE . 43
Growth Spurts
• Classic at 3,6,12 wks• Characterized by:
– Demanding for attention and food– Not sleeping as well– Very frequent feeding– Little to no stool for the preceding few days
© 2020 IABLE . 44
Signs That Feedings are Problematic
Infant won’t stop nursing
Sore Nipples
Infant StopsLatching
Fussy atthe Breast
© IABLE 45
Inverted nipple- no prep needed
Skin Tag- may need removalMilk coming from piercing
© IABLE 46
Flat Nipples Do Not Need Special PreparationClick for Video
© 2020 IABLE . 47
Conclusions- Session 2
• Understanding basic anatomy and physiology of breastfeeding helps with problem solving.
• There are several nursing positions, and all have in common an appropriate alignment for an ideal latch.
• Babies are individuals with different feeding patterns. Parents need help identifying feeding patterns that are successful.
© 2020 IABLE 48
An overweight pregnant woman reports that her breasts didn’t grow during pregnancy. You
advise:
A. She should be followed carefully postpartum to make sure that her milk supply becomes established.
B. She has a high likelihood of not making enough milk. She may want to consider not nursing.
C. Her breasts probably didn’t grow because she has not gained much weight in pregnancy. She should be fine.
D. B&C

3/7/2021
9
© 2020 IABLE 49
A pregnant person expresses concern about chestfeeding because 1 nipple is inverted. You
advise:
A. The individual should start rolling out her nipple on a regular basis.
B. Usually babies latch on fine despite an inverted nipple.
C. It might be hard for the baby to latch, so they should bring a nipple shield to the hospital.
D. A&C
© 2020 IABLE 50
You are counseling a first-time pregnant mom at 24 weeks, and ask about her breast changes thus far. She has not noticed much. You advise:
A. Let’s wait and see how things go. Please make sure that your baby is followed closely for weights during the first week.
B. There is a very likely chance that you won’t make enough milk. It is best to assume that you will need to give formula.
C. Maybe your breasts are not done growing yet.
D. A&C
© 2020 IABLE 51
A pregnant person is leaking colostrum during the 8th month of pregnancy. You
advise:A. Good for you, it means that you will have
plenty of milk.
B. I hope you don’t leak too much and lose all of your colostrum before the baby is born.
C. This is normal, use pads as needed.
D. A&C
© 2020 IABLE 52
Mom calls concerned about her 4 week old baby. He is popping on and off the breast and will only feed for
only a short time. You advise:
A. The baby might be uncomfortable. Try to switch positions. Call us back if this does not help.
B. Please bring the baby in for a weight check, and to be seen by a knowledgeable professional for a feeding assessment.
C. It sounds like your supply is low, give a bottle of formula after nursing.
© 2020 IABLE 53
Mom calls at 3 weeks to say that her 100% human milk-fed baby is ‘constipated’, no stool for 3 days. The baby has been
feeding often, a little fussy, no other illness symptoms. Possible reasons include:
A. Insufficient milk intake
B. Bowel obstruction
C. Growth spurt
D. It is common, the baby needs karosyrup.
E. A&C
© 2020 IABLE 54
A pregnant mom has a history of breast cancer and radiation to the R breast. She
can safely be told that she should not expect much milk from the R breast.
A. True
B. False

3/7/2021
10
© 2020 IABLE 55
You are seeing a 5 week old infant that is nursing well, and gaining weight well. Mom is concerned that the infant
constantly feeds in the evening, and she wonders if she should supplement because her breasts feel empty in the
evening. You advise:
A. Start with a cows- milk based formula, and supplement after the baby is done nursing.
B. It is common for the milk supply to be lower in the evening than am. Try pumping after the first 1 or 2 morning feeds, and refrigerate the milk for evening.
C. Your baby is just fussy, give the baby a pacifier or try other means to calm the baby.
© 2020 IABLE 56
Mom calls and is worried because their 10 day old baby won’t nurse for more than about 8
minutes on each side. She is worried that the baby is not getting enough calories. You advise:
A. Come in to be seen for a weight check, so that we can watch the baby nurse.
B. She should pump after feeding and supplement the baby with expressed breastmilk.
C. As long as the baby is happy with at least 5 stools a day and wet diapers, nothing to worry about.
D. The baby sounds weak, and should be seen ASAP.

3/7/2021
1
The OutpatientBreastfeeding
Champion Program
1
• The Instructor has no conflicts of interest to disclose
• Nursing credits, continuing education recognition points (CERPs) for IBCLE, or CPEUs for registered dietitians, are awarded commensurate with participation and complete/submission of the evaluation form.
OBC Session 3
• Breastfeeding in the Immediate Postpartum Period– Skin-to-Skin
– Self-Led Latch
– Delivery of the Placenta
– Colostrum
• Secretory Activation (Lactogenesis II)
• Engorgement
• Supporting Dyads during the First Week Postpartum
• Maternal Infant Separation
• Hospital Discharge & Follow Up
3
Objectives for Session 3
• Describe Infant Led Latch
• Identify the physiologic triggers that bring in mom’s milk supply
• Recite 4 crucial steps necessary to establish successful breastfeeding in the first few days after delivery
• Explain to mothers how to manage engorgement
4
Critical management procedures1a. Comply fully with the International Code of Marketing of Breast-milk Substitutes and relevant World Health Assembly resolutions.1b. Have a written infant feeding policy that is routinely communicated to staff and parents.1c. Establish ongoing monitoring and data-management systems.2. Ensure that staff have sufficient knowledge, competence and skills to support breastfeeding.Key clinical practices3. Discuss the importance and management of breastfeeding with pregnant women and their families.4. Facilitate immediate and uninterrupted skin-to-skin contact and support mothers to initiate breastfeeding as soon as possible after birth.5. Support mothers to initiate and maintain breastfeeding and manage common difficulties.6. Do not provide breastfed newborns any food or fluids other than breast milk, unless medically indicated.7. Enable mothers and their infants to remain together and to practice rooming-in 24 hours a day.8. Support mothers to recognize and respond to their infants’ cues for feeding.9. Counsel mothers on the use and risks of feeding bottles, teats and pacifiers.10. Coordinate discharge so that parents and their infants have timely access to ongoing support and care.
TEN STEPS TO SUCCESSFUL BREASTFEEDING
BABY-FRIENDLY HOSPITAL INITIATIVE (revised 2018)Breastfeeding Early
Postpartum
• Limit pain meds near the end of labor
• Skin-skin right after birth
• Encourage rooming-in of baby
• Breastfeeding education – Staff observes feeds each
shift
• No anti-lactation drugs for the parent
6

3/7/2021
2
Early Skin-to-Skin Contact
• Increased:– Breastfeeding duration
– Temperature regulation
– Blood sugar control
• Infant crying
• Maternal affection
7AAP Pediatrics 138(3) Sept 2016
Skin-to-Skin and Self-Led Latch
• Awakens infant feeding reflex
• Organizes route to feeding
– Search->feel->root
– Baby finds the nipple/areola and latches
8
First Feeding as Soon as
Possible After Birth
• Baby Friendly Hospital Initiative Step 4• Newborn awake & alert first 1-2 hours
➢Decreases risk of low blood sugars➢Low blood sugar leads to early bottle supplementation
➢Parental confidence9
Lactogenesis (Secretory Activation) After Birth
Placenta delivered, hormones fall
Colostrum
High in white cells, betacarotene, protein, antibodies
Gradual increase in fluid, blood flow, oxygen, glucose, breasts become fuller
10
11
ColostrumEarly colostrum feeds are small
12
First24 hrs 24-48 hrs
2-10ml/feed5-15ml/feed
Small, freq feeds are appropriate for newborn size
Every 1-3 hr feeds are expected8-12 times/24 hours

3/7/2021
3
13
Early Weight Loss Postpartum is NormalShould not exceed 10% from Birthweight
14
Feed on Cue- Early & Often!!
15
Latch Is More Manageable Before Infant is Crying!
Frequent Feeding +
Complete Emptying=
Rise in Milk Production
Infrequent Feeding +
Poor Milk Transfer =
Insufficient Milk Production
more milk
less milk
16
17
The Positive Trend in Milk Removal with Feeding
Infant Feeds Well
Milk Production Increases
Infant Gains Weight and
Strength
Milk Production
Regulates to Infant Needs
Infant Remains
Strong and Grows Well
18
Infant is sleepy/not
latched well
Infant Does Not Remove
Milk Well
Milk Production Slows or is Not Well
Established
Infant Does Not Gain
and Becomes
Weak
Milk Production
Declines Further
The Negative Trend when Insufficient Milk is Removed During Feeding

3/7/2021
4
19
How could a pacifier affect breastfeeding success?
20
Early Pacifier Use
• Pacifier use on days 2-5 postpartum:
– 2.5 times risk of not breastfeeding exclusively if a pacifier is used
– Use of a pacifier might signal that dyad has breastfeeding problems
21
When Are Pacifiers OK?
• Baby is latching & nursing well
• Back to birth weight
• Good weight gain
• Painful procedures or separations when mom cannot be present
How could rooming-in affect breastfeeding success?
23
• Improved patient satisfaction
• Decreased risk of abductions/switches
• Decrease infant abandonment
• Empowerment to parents• Increased frequency of
breastfeeding• Decreased
hyperbilirubinemia• Increased likelihood of
nursing up to 6 months
Evidence for Rooming In
AAP Pediatrics 138(3) Sept 2016 24
Photo by Gabriel Tovar on Unsplash

3/7/2021
5
Risks of Early Bathing
• Bathing in the first 24 hours is associated with decreased exclusive bfeeding at time of hospital discharge
– Prevents skin to skin
– Increased risk of hypothermia, causing fatigue and poor feeding
• AAP advises infants born to COVID+ mothers be bathed right away
Bumps in the Road Early After Birth
26
Engorgement
Parent-Child
Separation
Delay in
Lactation
Parent-Infant Separation
Help parent establish and maintain lactation– Initiate milk expression within the first hour pp– Pumping + manual expression– Maintain and promote bonding– Skin-to-skin
27
Premature Infants• Initial milk expression within the first 1 hour• Frequent expression, at least every 3 hours with no more than a 5
hr break at night• Coach moms on optimal pump use + hand expression• Nuzzle, skin to skin when possible• Encourage full milk production by 4-6 wks
28
Dx of Delayed Lactation
• Milk is not ‘in’ by:
– Day 2-3 for those who’ve previously nursed
– Day 2-5 for first baby
29
• No breast fullness
• Excessive infant weight loss
Delayed Lactogenesis-(Milk Comes in Late)
What to do?
• Nurse the baby first– Pump + manual expression after nursing
– Supplement with expressed BM, + any other supplementation needed
• Supplement by ~10% weight loss if production is not sufficient yet
• Firm feeding plan, and follow dyad closely30

3/7/2021
6
What are Options for Supplementation?
• The parent’s expressed human milk
• Donor human milk
• Infant formula
31 32
Engorgement
• Days 3-5 pp
• Increased blood flow
• Edema (swelling)
• Not the same as ‘too much milk’
33
Swelling Occurs in the SurroundingTissues Outside of the Glands
34
Effects of Engorgement
• Harder to latch
• Sore nipples
• Breast discomfort
• Reduction in milk production
35 36
Engorgement
Trouble Latching
Sore nipplesDecreased
nursing freq
Lower supply
Infant fussiness Supplementation
Decreased nursing freq
Mom quits

3/7/2021
7
Treatment for Engorgement
• Heat before nursing to improve milk flow• Breast massage before nursing• Express some milk to soften areolae• Apply cool compresses after nursing to decrease edema• Reverse Pressure Softening• Best Treatment is prevention with frequent nursing!!
37
Breast Massage
• Knead the breasts with knuckles from both hands
• Gently tap the breasts
• Roll the breasts between open hands, one on top, the other on the bottom
http://bfmedneo.com/resources/videos/
Click for video
38
See Babies Within 24-72 Hours after Discharge
• 24 hours:
– If jaundice, poor nursing, sore nipples
– First breastfed infant, feeding OK, milk not in yet
• 48 hours:
– If nursing fine, milk increasing, no jaundice, no soreness
• 72 hours
– If cesarean birth, nursing fine, milk in at discharge, baby’s weight loss has stabilized 39
Early Postpartum Concerns
40
• Day-Night cycles reversed at birth
• Wake the baby to feed during the day
• Parents take daytime naps
• Keep baby up in the evening
• Keep lights low at night, put baby back to bed after feeding
41
Infant up during the Night, Sleepy in the DayInfant is feeding
every 30-60 minutes
Infant is not finishing feedings
More about this later!
Milk production is low
More about this later!
42

3/7/2021
8
Parents are exhausted, can they
give a bottle at night?
• Encourage all feeds at the breast
– Ideal for the lactating parent to not skip feedings
– Pump if she needs to take a break
• Nap while infant is napping
• Make sure the baby finishes feeding
– Typically nursing every 1.5-3 hours, occasional clusters
– Move feeding clusters to evening 43
Parents worry that they cannot tell how much the baby is taking
• Check infant weight with current eating pattern
– Encourage parents to trust the baby
• Weigh the baby often to instill confidence
• Explain risks and challenges of pumping/bottle feeding
44
Optimal Latch?
45
Optimal Latch?
46
Optimal Latch?
47 48
Optimal Latch?

3/7/2021
9
Optimal Latch?
49 50
Optimal Latch?
Optimal Positioning??
51
Conclusions Session 3
• Routines in the first several hours after birth play a huge role in breastfeeding success.
• Early skin-to-skin contact is essential for newborn health, and facilitates the first nursing.
• A delay in milk ‘coming-in’ (increasing) is common, and can lead to breastfeeding failure.
• Teaching families about engorgement before leaving the hospital is important.
• Follow-up in the office within 24-72 hours after hospital discharge is imperative.
52

3/7/2021
1
The OutpatientBreastfeeding
Champion Program
1
• The Instructor has no conflicts of interest to disclose
• Nursing credits, continuing education recognition points (CERPs) for IBCLE, or CPEUs for registered dietitians, are awarded commensurate with participation and complete/submission of the evaluation form.
Session 4 OBC
• Sore Nipples- The Most Common Causes
• Managing Nipple Sores
• Breast Swelling and Engorgement
• Infant Biting
• Infectious Causes of Breast/Nipple Pain
• Non-Infectious Causes of Breast/Nipple Pain
3
Objectives for Session 4
• Describe at least 4 common causes of nipple and breast pain during lactation.
• Identify 3 main pieces of advice to give individuals who call with cracked sore nipples.
• Manage initial recommendations for sore nipples over the phone.
4
Objectives for Session 4
• Describe
– 3 instructions typically given to moms with acute mastitis.
– How to advise moms who might have shingles or herpes on a breast.
– Typical advice given to moms with a plugged duct.
– How to identify and advise care of vasospasm.
– Initial advice in the care of nipple dermatitis.
5 6
Mom calls you on day 4 pp because her baby, who was nursing fine, now won’t latch. Her breasts feel
very heavy, and the infant is crying. Your initial recommendations are:
A. The baby might be sick and should be seen ASAP
B. Her breasts are probably engorged and the baby cannot grasp the breast. Express some milk so the breast is more compressible.
C. She should bottle feed the baby because the baby clearly does not want to nurse anymore.

3/7/2021
2
7
Phone call: A parent is worried that their term 10 day old baby is nursing too often, every 2 hours, and that his partner does not have enough milk. He reports 3 stools & 6 wet diapers/day. When seen on day 3, the baby up 1 oz from day 2. You advise:
A. Everything sounds fine, keep the 2 week exam appt. The feeding frequency sounds normal.
B. Ask family to come in for a visit and weight check.
C. Advise that mom should just pump and bottle feed to see how much milk she has.
8
This same baby comes in for a weight check. You advise:
A. Things are fine, your baby gained another 2 oz, and has another 4 days to get to birth weight.
B. The baby is gaining slowly, lets try to figure out why this is.
C. The parent’s milk production is low and formula should be given after breastfeeding.
D. B&C
Birth Weight 8 lb 0 oz
Day 2 7 lb 9 oz
Day 3 7 lb 10 oz
Day 10 7 lb 12 oz
9
Mom calls and states that her 3 week old baby is nursing too often. He wants to nurse every 45 minutes most of the day, and never seems satisfied. Her breasts feel larger and they leak. You advise:
A. Your milk production is probably low. Give a supplement of formula after nursing.
B. Your baby is falling asleep at the breast, try to keep the baby awake while feeding. No need to worry.
C. Please come in for a visit, to check the infant’s weight and observe feeding.
10
Dad mentions at the 2 week visit that his baby is nursing every hour overnight, and sleeps in the
day. He wonders what to do. You advise:
A. He should get up, give the baby a bottle, and let mom get some rest.
B. Don’t let the baby sleep away the day. Try to feed the baby often in the day, and try to keep the baby up in the evening.
C. It is normal, mom should nap in the day with the baby so that she has the energy to be up with the baby at night.
11
A lactating parent calls, reporting that her 3 week old is fussy and has not stooled for 2 days. She believes her milk production is low because the baby wants to constantly nurse. Her partner wants to give a bottle to the baby. You advise:
A. Although this might be a growth spurt, the baby should come in for a weight check.
B. Because the baby is 3 weeks old, she is in a growth spurt. It will get better in a few days.
C. The baby is probably having a reaction to something in her diet, she should just pump and give the baby formula for now.
12
Dad calls because he wants to give their 1 week old a pacifier. All the baby wants to do is suck at
the breast, and he is sick of it. You advise:
A. Let me talk to mom.
B. Let’s see the baby in the office. It would be great if both parents could come.
C. It is fine to give a pacifier as long as the baby is nursing at least every 3 hours.
D. A & B

3/7/2021
3
13
At her term baby’s 4 week visit, mom wonders if she still needs to wake the baby up every 3 hours at night to nurse. The baby’s weight is great. You
advise:
A. You may want to get up to nurse or pump after a 5 hour break at night to prevent mastitis and plugged ducts
B. It is OK to let the baby sleep as long as she wants, she will probably wake up after 4-5 hours.
C. You don’t need to worry about emptying your breasts at night, they will adjust.
D. You need to feed the baby every 3 hours at night for at least a few months.
E. A & B
Finding Additional Lactation Help in Your Community
• The Triage Tools default to referral to lactation consultants/physicians/providers
• Not all communities or individuals have access to these levels of care
• Please speak up if there are other resources you are aware of in this community, such as doulas, local breastfeeding support groups, or a breastfeeding coalition.
14
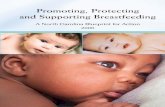
Breast Pain and Nipple Soreness
15
Myths re Sore Nipples
• Having to ‘toughen up’
• The baby having a strong suck
• Nursing the baby too much or too long
16
Nipple Pain Starts Early
–11-96% of lactating individuals have nipple pain at some point
• 43% with sore nipples at hospital D/C
• 73-76% with sore nipples at 3 days pp
• 19-26% having cracks
17 18
Cause of Nipple/Breast
Pain
Latch
Suck
Trauma
Pregnancy
Infection
Dermatitis
Vaso-spasm
High
production

3/7/2021
4
Engorgement• Days 3-5 postpartum
• Major reason for sore nipples– Leads to a shallow latch
19
Review of Engorgement TreatmentWhat are means of treating engorgement?What is the best way to prevent engorgement?
20
Cracked Nipple Treatment
• Moist Wound healing
– Don’t let nipple stick!!• Antibacterial ointment
• Coconut oil
• Lanolin
• Breastmilk
• Medicinal Honey
– Nonstick pad or parchment paper
• Decrease trauma- improve latch!!
• Treat underlying skin pathology
– ? Dermatitis/psoriasis
• Assess for breast infection– Mastitis
– Deep breast pain
21
Triage Tool Sore
NipplesGroup 2
22
23
• This is your second baby• Your baby is 3 weeks old• You had cracks of your nipples in the hospital,
then the pain seemed to improve, and now the nipples hurt again. The cracks are not healed yet.
• It hurts to latch the baby on.• You don’t know if you can keep nursing the baby
with this degree of pain.• You don’t have a fever, redness or swelling
Discussion Sore Nipple Case
• What are some pieces of advice that can help this mother right away, to decrease her pain?
• What are things that you can do as a breastfeeding champion to help this mom, if she comes in to see you in person?
24

3/7/2021
5
Underlying Problem Management StrategyInfant movement limitations due to torticollis, fractured clavicle, etc
Work on positioning
Prematurity/Low tone/sleepiness Limit time at breast, pump to maintain supply, supplement infant
Broad flat nipples Roll out or suction out nipples before latch, soften areola
Overactive letdown Change positioning, reduce milk volume
Infant disinterest due to low flow Supplement with a feeding tube at the breast
Oral defensiveness Bottle and finger feeding, speech eval
Tight lingual frenulum Clip the tongue tie
Oromotor dysfunction Speech eval 25 26
Before clipping After clipping
27
Before clipping After clipping
28
29
Hyperlactation
• Common symptoms
– Pain mainly when full
– Frequent breast fullness
– Recurrent mastitis
– Stringy milk
– Infant choking at the breast
– Infant feeds on one side only for short periods
– High supply when pumping
• People who are well matched typically express approx. 4-5 oz total every 3 hours
Acute Mastitis
Flu in the nursing individual is mastitis until proven otherwise! 30

3/7/2021
6
Acute Mastitis Symptoms
• Flu symptoms
• Breast pinkness-early stage– Harder to identify
on darker skin
• Breast swelling and redness later
• Possible nipple sores
• Often preceded by plugged ducts
31 32
What Do You Think Are Risk Factors for Mastitis?
© IABLE 33
Mastitis- Associated Risk FactorsSystematic Review
• 25% risk in first 26 weeks
• Nipple damage/pain
• Use of topical products
– Creams, nipple shield
• Staph aureus in milk
• Infant carrier of staph aureus
• History of mastitis in the past
• Multiparity
• Tight bra
Source: US Breastfeeding CommitteeWilson E, Wood SL JHL 2020 online
Complications of Mastitis
• 8-19% of women have recurrent episodes of mastitis
• 3-10% of women with mastitis develop abscesses
34
Mastitis Treatment
• Breastmilk culture– Check for resistant
bacteria
• Rest• Hot compresses• Frequent breast
drainage• Antibiotics• Anti-inflammatories-
ibuprofen
35
Abscesses during Lactation
• Require drainage, either I&D or repeated drainage with a needle
• Continue antibiotics, rely on culture results
• Keep breast well-drained
• Baby may nurse if milk is not purulent
36

3/7/2021
7
Infection
Dermatitis
Vasospasm
Latch and
Suck
Trauma
You are here
37 38
Cause of Nipple/Breast
Pain
Latch
Suck
Trauma
Pregnancy
Infection
Dermatitis
Vaso-spasm
High
production
Breast Pain- Yeast or Bacterial?
39
Typical Clinical Scenario
about Yeast
• A lactating parent calls, her 10 week old was recently diagnosed with thrush. She is noticing a burning/itchy sensation to her nipples, and would like to have something for the yeast infection of her nipples.
40
‘Yeast’ Overgrowth of the Nipple/Areolar Regions
• Typical sx– Burning, itching, ‘shards
of glass’, sharp shooting pain, redness of nipples
• Classic risks– Infant oral thrush
• Often treated by phone
• Symptoms are often not due to yeast
41
Nipple with dermatitis, not yeast
When to Treat for Yeast
• Nipples symptoms– Redness, shiny
– Pain, +/-itching
– AND infant has known oral thrush
• If nipples don’t look red, refer for evaluation before treatment
42

3/7/2021
8
43
How to treat YeastParent
• Only treat if– baby has thrush AND mom
has symptoms AND nipples appear to have thrush
• If nipples appear to have thrush, but baby does not, best to culture the nipples for thrush.
• Treatment options:– Topical nystatin ointment
– Topical clotrimazole cream
– Oral fluconazole x 10 days
Infant
• Treat if baby has thrush
– Nystatin drops
– Oral fluconazole
• No need to treat baby if parent has symptoms of thrush, if baby has no thrush
Symptoms of Subacute Mastitis or Mammary Dysbiosis
• Usually nipple pain
• Deep breast pain after feeding
• Breasts feel tender
• Recurrent plugged ducts
• Nipple scabs
44
45
Management of Mammary Dysbiosis
• This is a bacterial-overgrowth situation
• Breast exam and breastmilk culture
• Reduce any over-production of milk
• Antibiotics based on culture results
• Probiotics with Lactobacillus Salivarius and Lactobacillus Fermentum– Uncertain if it will help
• Refer to breastfeeding specialist for management if possible
46
Herpes Simplex onThe Breast
47
Herpes on the Breast
• Herpes Simplex– Can cause herpes in infant– The lactating parent is infected from nursing toddler
with cold sores
• Management– Avoid direct contact of lesions with baby– Express and discard milk on affected breast– OK to nurse on an unaffected side
• Often is on both breasts
– Cover lesions until scabbed over– Anti-viral medication
48
Shingles on the Breast
• Shingles- Reactivated Chickenpox– Blisters spread chickenpox
• Occur on 1 side of body• Can develop over 1 breast region• Management
– Avoid direct contact of lesions with baby– Express and discard milk on affected breast– OK to nurse on the other side– Cover lesions until scabbed over– Anti-viral medication

3/7/2021
9
Non-Infectious Causes of Pain
• Nipple Dermatitis
• Vasospasm
• Plugged Ducts
• Blebs
• Other nipple trauma
– Biting
49
Common Causes of Nipple Dermatitis
• Eczema
• Psoriasis
• Allergic reaction
50
Symptoms of Dermatitis
• Itchiness, pain
• Red and/or scaly
• May start during pregnancy or any time postpartum
51
Treatment of Dermatitis
• Identify underlying cause
• Avoid irritants
• Frequent repeated moisturization with an oil/non-petroleum jelly
• Topical steroids are typically needed– see her primary care provider or dermatologist for treatment
52
53
Classic Sx and Signs of Vasospasm
of the Nipples
• Nipple turns pale-blue-red
• Burning nipple pain
• Sharp breast pains
• Pain lasts variable duration of time– Color changes are assoc with pain
• Triggered by cold– Not just associated with feeding
54

3/7/2021
10
55
Treatment of Vasospasm
• Avoid infant biting
• Apply heat immediately after nursing
• Keep breasts warm
– Flannel or wool pads
– Foot warmers applied to backs of nursing pads- do not allow these to directly touch the breast/nipple!
– Medications56
Source: US Breastfeeding Committee
Plugged Ducts
• Symptoms– Tender localized area
of fullness and possible lump
– Pain radiates to/from the nipple during nursing
– No breast redness or fever
– Drop in milk production because the breast does not completely empty
57 58
What Do You Think Are Risk Factors for Plugged Ducts?
Risk Factors for Plugged Ducts
– High milk production
– Returning to work or maternal/infant separation
– Longer duration of sleeping
– Irregular feeding pattern
– Restrictive clothing/underwire bra
– Stress & fatigue
– Mammary Dysbiosis
59
Plugged Duct
• Treatment– Rest– Adequate nursing/pumping– Heat and massage – Electric toothbrush or
handheld massager– Ultrasound therapy– Vary nursing positions– If the lump does not
resolve in 48 hours, needs a visit
– Lecithin 1200mg 2-4 a day for prevention
60
Source: US Breastfeeding Committee

3/7/2021
11
Triage Tool Plugged DuctsGroup 2
61 62
• This is your first baby• Your baby is 3 months, and
you returned to work 3 weeks ago
• You notice a hard spot in your L breast, and that area feels full and won’t drain, for about a day
• No fever, swelling, redness
Discussion Plugged Duct Case
• What are reasons why this mother might have developed a plugged duct?
• What advice did you give mom to help her?
• When should she be seen for further evaluation?
63 64
• A milk-colored lesion on the nipple• May or may not be painful• Sometimes associated with blocked milk ducts
Nipple Blebs
65
• Treatment– IF no pain and no
underlying plugged duct, no need for treatment
– If painful, keep area well-moisturized• Olive oil on a
cotton ball in bra
• Lanolin
– Sterile unroofing by a provider when there is a plugged duct
– Steroid oint may helps
Photo- Kathy Leeper MD
Infant Biting
• Most often during teething
• Other causes:
– Bite reflex
– Mom’s milk flow
66

3/7/2021
12
Infant Biting During Teething
• Occurs with teething
• During non-nutritive sucking
• Treatment
– Keep the baby close
– Avoid non-nutritive sucking
– Alternative for infant teething
67
Photo by Deedee Geli on Unsplash
Conclusions for Session 4
▪ The most common causes of sore nipples are positioning and latch issues
▪ Breast engorgement during the first week increases the risk of nipple trauma
▪ Women with sore nipples who are not improved by changes in positioning and latch should be referred to a knowledgeable provider
68
69
You are seeing mom & her term healthy infant at 14 days postpartum. She complains that her nipples are sore when the baby latches on and the pain continues throughout feeding. When the baby comes off the breast, the nipple looks pinched and pale. You advise:
A. You have vasospasm of your nipples. Use heat on your breasts after nursing.
B. You likely have a yeast infection of your nipples. You will need to contact your provider for treatment.
C. You need to have the latch checked. Either I can do this, or lets have an LC see you.
70
A lactating individual who is 6 weeks postpartum reports stinging burning nipple pain for 1 week. Prior to this, they had no lactation problems. They would like to know what could possibly be wrong. You advise:
A. Your baby may not be latching properly.
B. You might have over-production, causing fullness and breast discomfort.
C. Your let-down is too fast, causing the baby to pinch the nipple.
D. You might have vasospasm.
E. You might have a nipple infection.
F. All of the above are possible.
71
A mother who is 20 days postpartum reports that her nipples are still cracked, sore, and the sores stick to her breast pad. She denies deep breast pain, fever or breast redness. Breastfeeding hurts with latch and improves during feeding. You advise:
A. You need to see a lactation specialist.
In the meantime, apply breastmilk, coconut oil, or lanolin and a nonstick pad over the wounds after each nursing.
B. Your nipples won’t heal until you stop nursing. Just pump and bottle feed for now.
C. Use a nipple shield to reduce pain and allow the sores to heal.
72
A lactating individual who is 3 months postpartum reports nipple redness with burning, stinging pain for 2 weeks. People on their Facebook support group suggested that they may have thrush. They wonder what you think. You advise:
A. You should be seen by a lactation consultant or breastfeeding medicine specialist to evaluate your pain.
B. Yes, it sounds like yeast. Call your physician for medication.
C. It sounds like vasospasm. Use heat on your nipples after nursing.
D. You should throw out your stored breastmilk in case it has yeast in it.

3/7/2021
13
73
Mom calls 4 months postpartum reporting recurrent plugged ducts. She usually can work them out in about 24 hours, but this one has been present for 4 days. She has no fever, chills or redness of the breast, but the area is tender. You advise:
A. Come in to be seen to have that area checked.
B. Try to nurse frequently, pump after nursing, use heat and massage as much as possible. IF it still is not gone in 3 days, call back. Watch for sx of infection.
C. You probably have too much milk, you should stop pumping so much extra milk.
74
A parent calls 7 mo postpartum with a recent diagnosis of shingles by their physician. They describe painful red skin lesions along the upper back and onto the R breast, involving the nipple. The physician advised weaning and the parent wants your opinion. You advise:
A. The baby is now old enough to be safely exposed to these shingles lesions, so no worries, keep nursing.
B. It is best to not nurse from that breast. Keep pumping and dump the milk until the lesions on the nipple and sores are dried up. Keep the area covered.
C. Don’t nurse from the R breast, but you can give the baby milk pumped from that breast.
75
A mother with her 4mo old reports that her infant is teething, and wonders how to prevent biting. She was told that babies need to wean when teeth come in. You advise:
A. Yes, sometimes babies bite. Good luck.
B. Pump and bottle feed when teething seems the worst.
C. Babies bite most often at the end of feeding. Keep the baby deeply latched to prevent biting, and take her off when she is biting and no longer seriously drinking.
D. Make sure to respond loudly and clearly, in order to scare the baby into never doing that again.

3/7/2021
1
The OutpatientBreastfeeding
Champion Program
OBC Session 5 Topics
• Reasons for Insufficient Infant Weight Gain• Triage Tool to Assess whether Baby is Transferring Enough
Milk• Weight Checks• The Sleepy Baby• Maternal Low Milk Production• Triaging the Mother Who is Worried About her Milk
Production• Pre/Post Feed Weights• Supplementing the Breastfed Baby• Night Time Feedings
Session 5 Objectives
• Identify 3 symptoms of a 3 day old infant who is not consuming in sufficient calories.
• Demonstrate competency at interpreting infant growth on an infant weight growth chart.
• Recite steps taken to perform a pre- and post-feed weight.
• Describe 4 typical pieces of advice given to parents with sleepy babies.
Session 5 Objectives
• Describe switch nursing.
• Identify 4 major reasons why milk production may be low.
• Describe 3 methods to supplement infants in the first few weeks postpartum.
• Identify 3 commonly used galactogogues.
• The Instructor has no conflicts of interest to disclose
• Nursing credits, continuing education recognition points (CERPs) for IBCLE, or CPEUs for registered dietitians, are awarded commensurate with participation and complete/submission of the evaluation form.
© 2019 IABLE. 6
Signs of Adequate Intake in theFirst 3 Days
• The baby nurses every few hours
• 2 stools a day
• 2-3 voids a day
• Content between feedings
• Minimal jaundice
• Breasts feel heavier

3/7/2021
2
© 2019 IABLE. 7
Reassuring Signs of Adequate Intake After the Milk Increases in Volume (after ~day 3)
• The baby nurses every few hours
• 3-4+ yellow seedy stools/day
• Always wet
• Infant content between feedings
• Breasts feel heavier before feeding, softer after
© 2019 IABLE. 8
Signs of Insufficient Intake
• Infant restlessness after feedings
• Dry small stools
• Dry diapers at times
• Constant nursing
• Breasts without fullness
• New breast/nipple pain
© 2019 IABLE. 9
Parental Concerns re Weight
Parents often express concerns that can lead to supplementation:
o Is our baby getting enough?
o Is our baby feeding too often?
o Is our baby not nursing long enough?
o Is our baby fussy because he is still hungry?
© 2019 IABLE. 10
Instilling Confidence
• Infant Weight=Proof of Adequate Feedings– Feedings cannot be assessed by phone
– Adequacy of calorie intake cannot be determined by observing feeds
• Non-gaining babies might:– Have nl # of stools/voids
– Be satisfied after nursing
– Spit- up after feedings
– Sleep all night
Does a report of adequate daily stools and voids indicate optimal intake?- NO
• Plenty of stools and voids indicate adequate hydration (fluid in the body).
• Hydration does not guarantee weight gain.
• People can lose weight without becoming dehydrated. Not everyone can see a provider, lactation consultant or WIC for a weight check.
What are other options in your community for a weight check?

3/7/2021
3
© 2019 IABLE. 13
Triage ToolIs My Baby
Getting Enough?Group 1
© 2019 IABLE. 14
• Your baby is 10 days old• The baby wants to nurse every hour when
awake• The baby falls asleep after nursing on one
side, and you cannot get her to wake up to feed from the other side
• The baby has lots of wet diapers, and 3 poops a day
• Your breasts feel somewhat full at times, mainly at night
• You think that your baby’s color is fine
© 2019 IABLE. 15
Discussion Case Is My Baby Getting Enough?
• What are the parent’s frustrations?
• What is the parent concerned about?
• How can you help this parent?
© IABLE 16
Common Reasons for Insufficient Infant Weight Gain
Infrequent feeding
Low milk production
Distraction at the breast
Infant illness
Sleepy at the breast
© 2019 IABLE. 17
‘Sleepy-Feeder’ Babies
▪ Too sleepy to transfer enough calories▪ All newborns are
sleepy▪ These babies are too
sleepy at the breast
▪ Increased risk▪ Small for Gestational
Age (SGA) babies▪ Premature infants
▪ Especially 35-38 week infants
Source: US Breastfeeding committee © 2019 IABLE 17 © 2019 IABLE. 18
Infant wakes to feed and nurses
Falls asleep before taking
enough
Infant awakens when taken off the breast and
acts hungry
Put back to the breast, falls
asleep quickly
Wakes up and still seems hungry when taken off the breast
Inadequate weight gain
The Infant Who Always Seems Hungry and Does Not Gain Enough

3/7/2021
4
© IABLE 19
An Infant Who is Sleepy but Wakes Up When Parent Attempts to Take Off the Breast
© 2019 IABLE. 20
Infant needs to be woken for feedings
Infant latches and nurses but
falls asleep
Infant is taken off, is content,
and sleeps
Infant is woken for next feed
Infant does not gain weight
The Content Sleepy BabyWho Does Not Gain well
© 2019 IABLE. 21
Why Doesn’t Milk Transfer Occur?
• Breastfeeding is an active process
• The baby has work to initiate milk flow
• Sleepy babies cannot generate this work
Source: US Breastfeeding committee
Keep Baby
Awake During
Feeding!!
Stimulate Infant
Switch nurse
Compress Breasts
Keep Infant Awake- Stimulate While at the Breast
What are other ways to stimulate the infant?
Global health media
Breast compressions while nursing can help transfer milk to a sleepy infant

3/7/2021
5
© IABLE 25
Switch Nursing- Nursing on Both Sides Twice
• Watch the infant feed on the first breast, and point out swallows
• As the infant relaxes, and there have been NO swallows for 3-4 minutes, switch infant to the other breast. No need to wait for the infant to unlatch on their own
• Point out swallows on the second side
• Once swallows are done for 3-4 minutes on the second side, OK to take infant off the breast
• If infant is still hungry, start the process over on the first, then the second breast
© IABLE 26
Watch for Sucks and SwallowsDetermine When Swallows End
© IABLE 27
Supplementing Sleepy BabiesBottles are often necessary when attempts to keep them awake, and
switch nursing does not help
Sleepy baby
swallows
Swallowing produces a
reflexive suck
Milk flows from the
bottle
Sleepy baby sucks
and swallows
Milk Flows from bottle
© IABLE 28
Why Paced Bottle Feeding?Click for video
▪ Slows feeding to mimic breastfeeding
▪ Prevents overfeeding
▪ Prevents propping▪ Encourages
socialization during feeding
© 2019 IABLE. 29
Triage Tool -Sleepy Baby; Group 2
© 2019 IABLE 29 © 2019 IABLE. 30
• This is your second baby• The baby is 3 weeks old, and has always been
sleepy since birth• The baby takes 40 minutes to finish each side• It is hard to wake the baby up after nursing on
one side• The baby nurses every 3 hours• He has 5 stools a day• Nothing has really changed in terms of # of stools
or voids• Mom does not have breast pain

3/7/2021
6
© 2019 IABLE. 31
Discussion of Case Sleep Baby
• What are mom’s concerns?
• What are helpful pieces of advice?
• How can the breastfeeding champion help her in-person?
© 2019 IABLE. 32
Growth ChartsA Measure of Expected Growth
Growth Curves
• The Centers for Disease Control uses the World Health Organization Growth Curves thru age 2
- http://www.cdc.gov/growthcharts/who_charts.htm
• Appropriate for breastfed and formula fed infants
• Plot naked weights for accuracy
© 2019 IABLE. 34
Expected Rates of Infant Weight GainAge of Infant Expected Rate of Weight Gain
The first 2-4 days • Mild decrease from birth weight• No more than ~10% weight loss• Lowest weight by day 3-4• Stop losing weight when breasts are
fuller• If more than 10% loss, see provider/LC
Day 5 thru approximately 3.5-4 months
• Gain at least 25-30 grams/day• Typically ~ 2 lb each month• If gaining less, plot weight on growth
curve to determine adequacy of growth
After 4 months • Weight gain/day depends on infant size• Plot the weight on growth chart to
determine adequacy of growth
© 2019 IABLE. 35
Normal Infant Growth

3/7/2021
7
Note: Drop across 2 growth curves is
concerning
© 2019 IABLE. 39
Abnormal Growth
© 2019 IABLE. 41
Premature Infant
© 2019 IABLE. 42
What Do You Think?

3/7/2021
8
Birth weight at 7 lb 7 oz
2 week weight = 6 lb 12 oz
1 month 2 month
What Do You Think of Growth from Birth to 2
Weeks?
© 2019 IABLE. 44
Birth wt- 8 lb 2.5 oz(3600g)
2 weeks- 7 lb 14.3 oz(3580g)
3 weeks- 9 lb 1.8 oz(4133g)
What do these weights tell us?How is the weight at 2 weeks? At 3 weeks?
Months
© 2019 IABLE. 45
You are seeing this infant at 2 months of age.
How is the growth frombirth to 2 months?
Months
© 2019 IABLE. 46
Now you are seeing this infant at 4 months of age.What do you think about the infant’s growth, from
2-4 months?
What questions would you ask parents about
feeding?
Months
© 2019 IABLE. 47
You are seeing the same infant at 7 months of age.
What do you think about the infant’s growth, from 4-7 months?
Months
© 2019 IABLE. 48
How is this growth?
IABLE 48

3/7/2021
9
© 2019 IABLE. 49
Is this growth OK?What may have
happened at 2-4 mo?
Months © 2019 IABLE. 50
Pre- and Post- Feed Weights
• A way to measure intake at one feeding
• One feeding does not represent all feedings for the whole day
• The proof of appropriate calorie intake is in the daily/weekly weight gain
© 2019 IABLE. 51
Pre/Post Feed WeightsCan Backfire
• Volumes vary per feed
• An office feeding ≠ home feeding
• What is the right amount?
– Is 2.5 oz, 3 oz, or 4 oz the right amount?
Optimal Situations for
Pre-Post FeedWeights
• The baby has not been gaining well, and mom appears to have plenty of milk
• Monitoring the baby known to have low milk transfer • Premature or sleepy babies
• The baby nurses for a long time, the parent is not sure about their milk production, baby’s growth is marginal
How to Do a Pre-PostFeed Weight
• Use a digital scale, measuring at least to 2 grams
• Weigh the baby naked, for documentation on growth chart
• Put on clean diaper and clothes that baby will wear while nursing, and weigh the baby in grams
• Feed the baby
• Reweigh the baby in the same clothes and diaper.
• Difference in grams= amount of milk transferred
• 5400g pre-feed, 5464g post feed =64g difference, which is 64ml transfer
The Breastfeeding Champion’s Role
• Weigh the baby and determine if growth is sufficient• If weight is excellent, provide reassurance.
• If not sufficient or unclear, needs a provider/LC visit
• Initial recommendation for supplementation
• Support the parent’s milk production

3/7/2021
10
© 2019 IABLE. 55
Cup feeding
Finger FeedingTube Feeding at the Breast
Options forSupplementation
© 2019 IABLE. 56
Bottle Feeding
Pros• Easy to use
• Available
• Easy to clean
• Culturally acceptable for most families
Cons• Parents may perceive this as
giving up
• Baby might prefer the bottle over the breast
Best Bottles?-elongated round nipples
© 2019 IABLE. 57
Cup Feeding
Pros• Does not fulfill infant’s suck
need
• Cups are easily available and cheap (shot glass)
• Easy to clean
Cons• Learning curve
– Spillage, slow
• Not typical in our culture
• Overwhelming task for some
Click for Video
© 2019 IABLE. 58
Finger Feeding
Pros• Avoids using a bottle
• Good for small volumes
• Active participation
Cons• Difficult with larger volumes
• Needs coordination
• Aspiration
• Cleaning
• Accessibility
Click for Video
© 2019 IABLE. 59
Supplementer at the Breast
Pros• Saves time
• Increase breast stimulation
• Avoids artificial nipples
• Can help drain the breast
Cons• Clumsy, hassle
• Need extra equipment
• Not easily transportable
• Some babies refuse it
• Not for sleepy babies
Click for Video
© 2019 IABLE. 60
Breastfeeding Champion’s Role in Cases of Low Milk Production
• Identify whether the parent may have low production
• Cannot diagnose etiology
• Support the milk production – Advise frequent nursing
– Pump after feeding• Unless infant empties the breast
thoroughly
– Help parent access a pump
– Advise on milk storage

3/7/2021
11
© 2019 IABLE. 61
Normal interval growth
Frequent nursing with a
marginal production
Fussy baby
Pain, GERD, Fear, Other
Growth Spurt
Sleepy, Snacker High Suck
Need
Normal postpartum
breast changes
Parental expectations
Perceived Low Milk Production
© 2019 IABLE. 62
If Interval Growth is Normal
• Reassure• Make sure that production is
not marginal• Advise on keeping baby
awake with feedings• Evaluate family’s
expectations• Identify growth spurts• Could consider a pacifier if
needed
© 2019 IABLE. 63
Low Milk Production
Insufficient breast development
Obesity, PCOS, DM, HBP, Infertility
Milk never came in
postpartum
PP bleed, medications,
retained placenta
Milk came in but milk production dropped
MOST COMMON CAUSE
Lack of nipple stimulation
Lack of breast emptying
Parental illness, medication
© 2019 IABLE. 64
Prenatal Reasons for Low Production
Source: US Breastfeeding committee
© 2019 IABLE. 65 © 2019 IABLE. 66
Little or No Breast Changesin Pregnancy
Little Breast Change
Insufficient Glandular Tissue
CongenitalAcquired (surgery,
radiation)
Polycystic Ovarian Syndrome, Obesity,
Gestational Diabetes

3/7/2021
12
© 2019 IABLE. 67
Congenital Insufficient Glandular Tissue
• May or may not report breast growth in pregnancy
• Not related to size of breast
• Shape of breasts can be a clue– Widely spaced– Nipples point down or
outward– Large areola on small
breasts
© IABLE 68
• High Androgens
–Obesity
–Polycystic Ovarian Syndrome
–Diabetes
–Pre-eclampsia
• Insulin resistance
• Meds (aripiprazole)
Hormonal Interference
© 2019 IABLE. 69
Postpartum ComplicationsLeading to Low Milk Production
© 2019 IABLE 69Source: US Breastfeeding committee© 2019 IABLE. 70
The Milk Does Not Increase Postpartum
Delay in lactation
Retained Placental
Fragments
Medication/hormones inhibiting lactation
Maternal illness, i.e. Sheehans
Insufficient glandular
tissue
If Minimal/No Milk by 7-8 Days, Refer to a Knowledgeable Physician/Provider
Labs and eval needed for::• Pituitary function• Uterus for retained placenta• Other hormone problems• Medication side effects
© 2019 IABLE. 72
Low Milk Production
Insufficient breast development
Obesity, PCOS, DM, HBP, Infertility
Milk never came in
postpartum
PP bleed, medications,
retained placenta
Milk came in but milk production dropped
MOST COMMON CAUSE
Lack of nipple stimulation
Lack of breast emptying
Parental illness, medication

3/7/2021
13
If the Milk Comes In, How Can a Parent Lose Milk Production in the First Week Postpartum?
(review of earlier sessions)© 2019 IABLE. 74
Substances that MayDecrease Milk Production
• Bromocriptine, cabergoline• Estrogen-containing birth control pills• Progesterone birth control, esp in the first
6 weeks• Decongestants- pseudoephedrine• Aripiprazole (Abilify)• Nicotine• Alcohol• High dose steroids• Epinephrine• Antihistamines, especially frequent use• Herbal teas/supplements• Placenta encapsulation
© 2019 IABLE. 75
First Steps toIncrease Milk Production
• Pumping and/or nursing at least every 3 hours with no more than a 5-6 hour break at night
• Avoid medications thatdecrease supply
• Sufficient self-care
– Eat, drink, sleep
© 2019 IABLE. 76
Galactogogues-Substances That
Increase Milk Production
© IABLE 76
© 2019 IABLE. 77
Commonly Used Galactogogues
• Fenugreek
• Moringa Leaf
• Shatavari Root
• Herbal combinations as tinctures/teas
• Metoclopramide- prescription
• Domperidone- non-FDA approved prescription
• Non-prescribers generally not licensed to endorse these products
© 2019 IABLE. 78
Fenugreek
• Considered possibly safe by the FDA in medicinal amounts
• Dose- 500mg-610mg caps of crushed seeds, 2-3 caps 3x/day
• Side effects- body odor, GI upset for mom, GI upset for baby
• Risks-Avoid if allergic to legumes/peanuts, can worsen asthma, low blood sugar
• Not found to be very effective in research studies

3/7/2021
14
© 2019 IABLE. 79
Shatavari- Asparagus Racemosus
• Root is the active, safe part of plant
• Side effects- headache, slight risk of a decrease in milk supply
• Interacts with Lithium
• Dose is 800mg-1000mg 3x/day
© 2016 IABLE 79 © 2019 IABLE. 80
Moringa=Malunggay
• Used grown and consumed in tropics
• Leaf portion shown in some studies to milk production
• Dose is 500mg-1000mg 3x/day
• Side effects- stomach upset for infant
• Possible interaction with thyroid medication
© 2019 IABLE. 81
Herbal Combinations
• Many brands
• Wide variety of herbs– Nettle
– Blessed thistle
– Milk thistle
– Goats Rue
– Fennel
– Fenugreek
– Saw Palmetto
Considerations in
Galactogogue Use
• Parents with high milk production will have a greater
response
• Studies on galactogogues do not typically include
women with low production
• No ‘one-size fits all’
– People respond differently to different herbs
• Research is generally low quality. Best evidence is
cultural experience
• No data on how long to take herbs for effectiveness
82
© 2019 IABLE. 83
Metoclopramide- Prescription Med
• Increases prolactin levels
• Side effects- fatigue, dizziness,depression, seizures, tremors, tics
• Contraindications- psychiatric disorders, seizures
• Dose = 5-10mg 3-4 times a day
• It can double milk volume at most
• Follow the lactating parent closely for depression, anxiety, seizures
© 2019 IABLE. 84
Domperidone- Prescription Med
• Increases prolactin levels• Rare neurologic side effects• Similar efficacy to metoclopramide• Dose at 10mg 4 times a day• Not FDA approved• Side effects- cardiac, abdominal cramps, rash, itching• Several medication interactions
– Fluconazole– Lithium– Erythromycin– + others

3/7/2021
15
Common Foods Believedto Increase Milk Production
Based on Culture, Little Research
• Herbs and Spices
– Garlic, ginger, basil, onions, caraway, anise, coriander, dill, cumin
• Hops
• Chamomile, marshmallow
• Green Leafy Vegetables and sprouts
• Grains- oats, quinoa, barley, rice
• Nuts and nut butters
• Brewers yeast
Mother-food.com© 2019 IABLE. 86
When to use Galactogogues
• Galactogogues are not asubstitute for optimal nursing/pumping
• Milk production will not increasewith supplements alone
© 2019 IABLE. 87
Conclusions Session 5
• Many babies appear to nurse well, but they need weight checks to confirm proper growth.
• It is important to instill confidence in lactating parents by weighing babies whenever they are concerned about the baby taking enough milk.
• Parents need support in protecting their milk production when babies are not nursing well.
© 2019 IABLE. 88
Conclusions Session 5
• There are many reasons why a parent may have low milk production, and sorting out the underlying reason(s) can be tricky.
• Most parents can increase their production with effective and consistent nursing/milk expression routines.
• Galactogogues do not take the place of regular nursing and breast expression to increase the milk production.

3/7/2021
1
The OutpatientBreastfeeding
Champion Program• The Instructor has no conflicts of interest to disclose
• Nursing credits, continuing education recognition points (CERPs) for IBCLE, or CPEUs for registered dietitians, are awarded commensurate with participation and complete/submission of the evaluation form.
© IABLE 3
Review of Session 5
© IABLE 4
A lactating parent’s partner calls concerned that their 7 day old baby is not getting enough. He only feeds for 10 minutes on 1 side, then falls asleep. He is not fussy and feeds every 2.5 hours. Diapers are always wet, & he has 5-6 stools/day. You advise:
A. It sounds like your baby is fine, keep your 2 week appointment.
B. It sounds like your baby is doing fine, please come in to see me for a weight check.
C. Your baby should be nursing for 15 min each side. I will refer you to a lactation consultant.
D. Pump the other side and offer that in a bottle.
© IABLE 5
What is the most reliable indication that a newborn infant (<30 days) is gaining well?
A. Frequent stools and urine
B. Contentment and relaxation between feedings
C. Infant weight
D. Feeding every 2-2.5 hours
E. Sleeping thru the night
© IABLE 6
Mom brings her 3 month old baby in for a weight check. She is
worried that the baby is fussy, and she seems to spit up frequently.
You advise:
A. Your baby’s weight % decreased, but not that much. Please come back in a week for another weight check.
B. Your baby’s weight% decreased, the baby needs to see her provider.
C. Your baby seems to be doing fine, keep your 4 month appt.

3/7/2021
2
© IABLE 7
You weigh a 2 mo old- her weight % dropped from the 78% to the 54%. The baby has been happy, feeds every 2-3 hours, and seems satisfied. The parent can pump 8 ounces at one time at work. The parent has not been concerned.
© IABLE 8
You advise:A. Your baby looks healthy. I notice that
your baby dropped in her weight %. Lets recheck her weight in 2 weeks.
B. Your baby dropped in her weight %. I am somewhat concerned. Please supplement with a bottle of expressed breastmilk twice a day.
C. Your baby dropped in weight %, she needs to see her provider or a lactation consultant.
© IABLE 9
You are seeing a 17 day old baby for a pre/post feed weight because the family is worried how much the baby is drinking. The infant is fussy in the evenings and feeds often. You do a pre-post feed weight, and the baby transfers 110ml. Mom’s partner wonders if this is enough. You advise:
A. The baby transferred about 3.5 ounces, so the baby is doing fine.
B. The baby transferred a good amount. Lets check her growth curve.
C. Your baby should be drinking 120ml, or 4oz each feeding. You need to take fenugreek and give some formula in the evening.
© IABLE 10
Session 6 Topics
• The non-latching baby
• Infant led latch
• The baby who prefers one side
• Risks of nipple shields
• Pacifiers
• Infant fussiness at the breast
• Weaning
• Induced Lactation and Re-lactation
• Complementary Feeding
© IABLE 11
Session 6 Objectives
• Identify 3 reasons why a newborn baby may refuse to latch onto the breast
• Describe 3 reasons why a breastfeeding baby may gradually or suddenly refuse to nurse
• Understand how to counsel a parent to practice infant-led latch
• Give 2 reasons to avoid nipple shields
• Identify how to counsel a family on use of pacifiers
© IABLE 12
Session 6 Objectives cont’d
• Demonstrate proficiency triaging the baby who is fussy at the breast.
• Describe how to counsel a parent on weaning.
• Define induced lactation and re-lactation.

3/7/2021
3
© IABLE 13
The Baby Who Won’t Latch
No Latch in the First Several Days of Life
• Variable nursing on day 1 is common
• Nursing skills usually improve by day 2
• If no latch in first hour
– Manually express and supplement with spoon/syringe every 2-3 hours
– Keep skin to skin14Spoon Feeding Video
© IABLE 15
Non-latching
Baby
Bottle preference
Anatomic or motor
issues
Sleepy and/or
premature
© IABLE 16
Sleepy and Premature Infant
• Falls asleep at the breast
• Sluggish suck/swallow reflex
• Often needs supplementation until nursing improves
© IABLE 17
Bottle Preference
• Babies who receive a bottle early may become imprinted on a bottle
– Look for firm stimulus on palate
– Look for immediate and low resistance milk flow
© IABLE 18
Anatomic and Motor Problems
• Tongue Tie- prevents a deep latch
• Torticollis
– Won’t latch on one breast
• Nasal obstruction
• Pain
• Flat or inverted nipples
• ENGORGEMENT

3/7/2021
4
© IABLE 19
Triage Tool- Refusal of One Breast-Group 1
© IABLE 20
• This is mom’s 3rd baby• The baby is 9 days old, and
won’t take the R breast. This started on day 4.
• Mom is not sure if the baby has a preference of keeping the head to one side or not
• Mom is not aware of any sort of birth injury
© IABLE 21
Discussion of Case Refusal ofOne Breast
• What can we tell mom re some reasons why the baby might not latch on one side?
• What initial steps can the breastfeeding champion advise for mom?
© IABLE 22
Breastfeeding Champion’s Role with a Non-Latching Baby
• Help to maintain milk production
• Choosing supplementation method
• Demonstrate use of a supplementer if needed
• Help to establish care with a lactation consultant
© IABLE 23
Skin to Skin for theNon-Latching Baby
Chest toChest
Bobs andPecks
Moves DownTo Breast
Roots andLatches
© IABLE 24
Infant Led Latch VideoClick to Start

3/7/2021
5
© IABLE 25
Why Not a Nipple Shield?
➢An easy fix
➢Nipple shields might decrease prolactin
o Risk of decrease in milk supply
➢Risk of insufficient milk transfer
➢Need to pump after nursing
➢Does not teach nursing
o ? Increase nursing challenges
Click to Play Video
© IABLE 26
The Baby Who Stops Latching or is Fussy at the Breast
© IABLE 27
Baby Stops
Latching
Frequent Bottles
Change in milk flow; lower or higher
Infant illness
Infant Distraction
Infant Preference
for Position
Mom yells/Fear
Disinterest
© IABLE 28
Change in Milk Flow
• Decrease in milk production
– Slower flow
• High production
– Heavier letdown, baby chokes
© IABLE 29
Low Milk Production
• Baby stops latching due to frustration and hunger
• Often has been given bottles or a finger feeder
• Supplementer at the breast helps
© IABLE 30
Solution to Milk Flow Problems
• Low production - use the low supply triage tool
• If production is high and let-down is heavy:– Decrease excessive pumping
– Stop galactogogues
– Express the first let-down, then nurse
– Lay back to nurse
– Refer to a lactation specialist

3/7/2021
6
© IABLE 31
Frequent Bottles
• Firmer stimulus
• The bottle is either a faster or slower flow, and is preferred by the baby
Can you think of strategies to help resolve bottle preference for a baby?
© IABLE 33
Solution for Bottle Preference
• Pace the bottle feeding
• Only bottle feed with baby facing parent/caregiver
• Reduce distractions when nursing
• Consider a supplementer at the breast
• Infant-led latch
© IABLE 34
Infant Illness
• Nasal congestion
• Thrush or mouth sores
• Ear pain with sucking
• Nausea or abdominal pain
• Pain from recent surgery
© IABLE 35
Infant Distraction
Often by 4 monthsMore likely to nurse at nightSolution is to decrease distractionsConsider referring to mother support groups © IABLE 36
Disinterest
• Commonly occurs at 6-10 months
• Often infant is self-weaning
• Very hard to get these babies to nurse
• May nurse best at night

3/7/2021
7
© IABLE 37
Triage Tool Fussy at the Breast
Group 2
Source: US Breastfeeding committee © IABLE 38
• This is mom’s 4th baby• The baby is now 7 weeks old• The baby is very fussy at the breast. He
squirms, pops on and off, and cries after feeding, but not for every feeding
• She feels that her milk supply is normal, not too high, not too low
• The baby is somewhat spitty between feedings
• The baby does not have mucous or blood in the stool
• The baby is fussy all the time, but more at night
© IABLE 39
Discussion of Case- Fussy At the Breast
• What are possible reasons that the baby is fussy at the breast?
• What are some initial ways that the breastfeeding champion that can help this mother?
© IABLE 40
Weaning
Source: US Breastfeeding Committee
© IABLE 41
Weaning Has Several Meanings
• Addition of complementary foods
• Substituting formula for breastmilk or breastfeeding
• Decrease frequency of nursing, but not pumping at other times of infant feeding
• Actively and continually decreasing the number of breastfeeds or pumpings per day, until done
© IABLE 42
The Decision to Wean
• Sometimes weaning is a health recommendation
• Most of the time, the lactating parent makes the decision to wean– Parents should not be
told by family, friends to wean

3/7/2021
8
© IABLE 43
Reasons Why Weaning
Happens Early
• Breastfeeding Problems– Low production– Breast pain
• Lack of knowledge• Lack of support
– Pressure from family and spouse– Poor medical advice
• Lack of confidence– Uncomfortable nursing in public
• Going back to work
© IABLE 44
Parent-led Weaning
• Wean by dropping feedings
• Wean by stopping nursing and just pump
© IABLE 45
Dropping Feedings
• The lactating parent drops one feeding, and gives formula or stored milk
• The pumps slightly to comfort as needed
• Once comfortable, drop another feeding at another time of day
• When down to last feeding, may need to pump a day or two later
© IABLE 46
Weaning by Just Pumping
• Take the baby off the breast, and just pump
• Gradually increase interval of time between pumping sessions, and only pump to comfort
• After dropping last pumping, may need to pump several days later
© IABLE 47
Which Weaning Method is Best?
• Parent’s preference and situation– Traveling, working long hours, etc
• Just pumping may be faster
• Parents with over-production and/or recurrent plugs may choose pumping
• Older babies may become upset with the pumping method
© IABLE 48
Breast Comfort During Weaning
• Always pump to comfort, never fully drain
• Medications to reduce supply:
– Sage, peppermint
– Pseudoephedrine
– Contraception with estrogen

3/7/2021
9
© IABLE 49
Child- Led Weaning
• Typically older babies and children
• The parent continues to nurse whenever the baby or child wants to nurse
• The parent may not have a plan or date in mind for weaning
© IABLE 50
Toddler Nursing
• Variety of nursing styles– Toddlers drive nursing pattern
• Frequency varies
– The lactating parent determine nursing pattern• The parent decides when nursing can happen
• Educating parents about options often helps the parent nurse longer– Parents learn that they can have some control
© IABLE 51
Weaning Toddlers
• Start with having a nursing routine
• Start by dropping the easiest nursing times– Distract with playing, toys, treats
– Separation from toddler
– Change routines at home
– Anticipatory guidance for children over 2
© IABLE 52
Breastfeeding Champion Role
in Weaning
• Support the lactating parent in finding a solution for weaning
• Offer community resources for support
© IABLE 53
Tandem Nursing
• The lactating parent continues to nurse the infant/ toddler through pregnancy
• Nutritional counseling is recommended
• The parent nurses both infant and toddler for as long as desired
– Toddler often nurses after the baby
– Toddler can help maintain production
– Toddler stays healthier
– Typically no concerns about infant growth after birth
© IABLE 54
Induced Lactation Initiating lactation without pregnancy
– Most common with adoptions or surrogacy
• Hormones to stimulate breast growth
• Meds to increase prolactin • Begin pumping
regularly after stopping hormones
• Add galactogogues
• Breastfeed when infant is present
• Continue galactogogues
12
3

3/7/2021
10
© IABLE 55
Re-Lactation
• Initiate breastfeeding after weaning– Adoption– Parental illness– Infant intolerance to formula– Change of heart– Supply donor milk to relative/friend
• For people with a h/o healthy production, expect ~6-8 weeks to re-establish milk production
Lactating Parents’ Diet and Breastfeeding
• Drink water to thirst
– Urine should appear clear or pale yellow
– Dark urine can indicate insufficient fluid intake (unless
colored by supplements)
• Foods with essential fatty acids (DHA), particularly
fish, should be eaten 2-3 times a week
• If dietary restriction or malabsorption, discuss with
health care provider
– Vegan
– Stomach bypass surgery
• Rapid significant weight loss may decrease supply
Lactating Parent’s Diet and Infant
Fussiness
• Most foods do not cause GI symptoms in the
infant
– Occasional gas with cruciferous veggies
• Dairy can increase GERD symptoms
– No need to stop all dairy- reduce # of servings
• Coffee, tea, chocolate -watch for infant
irritability
© IABLE 58
Complementary Foodand Supplements
© 2016 The Milk Mob. 59
Supplements for the
Breastfed Baby
• Vitamin D- needed by all infants
• 400 units for all infants, from birth
• Formula contains vit D
• Breastmilk is low in vit D unless the parent’s level is high
• Iron
• Small for gestation age
• Premature or 35-37 weeks
• Ill/blood loss
© IABLE 60
Risks of Starting Complementary Foods Before 6 months of Age
• Earlier return of menses for the parent
• Increased risk of colds, diarrhea, wheezing
• Decreased protection from breastfeeding because of lower volumes of breastmilk

3/7/2021
11
© IABLE 61
Reasons Why Parents May Start Solids Too Early (Before 6 mo)
• Parents think that under 6 months is fine
– Often instructed by provider
• The baby seems hungry
• The baby shows interest in solids
• The baby might sleep better at night
© IABLE 62
Complementary Foods High in Iron
• Breastfed babies need high iron foods– Iron needs increase as baby
grows• Volume of breastmilk/iron has
not increased
– Infants are low on fetal iron stores
– Foods High in Iron• Meat
• Stewed dried fruits
• Lentils, peas, beans
• Dark leafy veggies
• Fortified cereals
© IABLE 63
Conclusions Session 6
• Many reasons why a baby fusses or refuses to latch onto the breast are treatable.
• Babies do not lose the ability to latch onto the breast.
• Infant-led latch is the natural way to encourage a baby back to the breast.
© IABLE 64
Conclusions Session 6
• Parents appreciate learning several options for weaning.
• Breastfed infants should wait until 6 months to introduce complementary foods.
• Breastfed infants need complementary foods that are high in iron.

3/7/2021
1
The OutpatientBreastfeeding
Champion Program• The Instructor has no conflicts of interest to disclose• Nursing credits, continuing education recognition
points (CERPs) for IBCLE, or CPEUs for registered dietitians, are awarded commensurate with participation and complete/submission of the evaluation form.
© IABLE 3
A mother is seen on day 5, 1 day after leaving the hospital s/p cesarean birth. She reports pumping and bottle feeding because her baby has not latched to either breast yet. Every time she puts the baby to the breast, the baby screams. She wonders what to do. You advise:
A. Stop bottle feeding, switch to finger-feeding, and keep trying to put the baby to the breast before finger-feeding.
B. Your baby probably has a problem such as torticollis or a sucking problem. Continue to do what you are currently doing, and see a lactation specialist.
C. Continue to pump + manual expression every 3 hours. Keep your baby skin-to-skin as much as possible and let the baby move down towards the breast when he is interested. You should also see a lactation specialist.
D. A and C
© IABLE 4
A lactating parent who is 2 weeks postpartum reports that the baby refuses to feed from the L side. He fed from both sides the first 3-4 days, then became fussier on the L side over time. Now he is just pumping the L side.What is the most important question to ask this parent?
A. Is your let-down heavier on the Left?B. Is your milk supply lower on the L side?C. Does your baby turn his head equally to
both sides?D. Do you think your baby has any pain
when lying on that side?E. All are important
© IABLE 5
This mom now tells you that the L breast makes more milk and has a heavier let-down. She now realizes that he chokes on that side. You advise all EXCEPT:
A. Try to nurse from the L before it becomes too full.
B. Just keep pumping the L side and nurse from the R side.
C. If the L side is too full before feeding, express the first letdown into a container or towel.
D. Change positions so that the baby is more on-top of the breast rather than underneath it.
© IABLE 6
Mom calls at 7 weeks postpartum, and says that her milk production is Iow. She is taking herbs and pumping after most feedings. She supplements by finger-feeding 1.5 oz of formula after nursing, but this takes a long time. She is worried that her baby won’t nurse if she introduces a bottle. She wants your opinion re what to do.Reasonable advice would include:
A. Would you be interested in learning how to use a feeding tube at the breast?
B. Introducing a bottle is reasonable at this point, but you are correct that the baby might have less interest in nursing, it depends on the baby.
C. I would like to see you to watch a feeding and do a pre and post-feed weight.
D. I suggest you see a breastfeeding specialist for a consult regarding your low production and an infant feeding plan.
E. All of the above

3/7/2021
2
© IABLE 7
Today you are seeing mom and baby 2 weeks postpartum. The baby had trouble latching in the hospital, so was given a nipple shield on day 2. She is still using the nipple shield because when her baby won’t latch without it.
Weight Date
Birth 8 lb 1 oz
Day 2 (hosp discharge) 7 lb 7 oz
Day 3 (office visit) 7 lb 8 oz
Day 14 (today) 7 lb 11 oz
© IABLE 8
Mom wants to know how his weight is. You respond:
A. The baby has not gained sufficient weight. I would like you to give a bottle of formula after each feeding.
B. The baby has not gained sufficient weight. We need to evaluate this further.
C. The baby has not gained sufficient weight. It looks like your milk production is low. I will ask the doctor to give you a medicine for this.
Weight Date
Birth 8 lb 1 oz
Day 2 (hosp discharge) 7 lb 7 oz
Day 3 (office visit) 7 lb 8 oz
Day 14 (today) 7 lb 11 oz
© IABLE 9
This same mother reports that her breasts feel full before feeding, and she always sees milk in the nipple shield after nursing. You’ve decided that you are going to refer them to the lactation consultant. In the meantime, your advice to mom includes:
A. Please pump after feeding to maintain your production. Offer expressed breastmilk to the baby after nursing, however much he’ll take, and lets talk about how to supplement.
B. Lets arrange a weight check in 3 days.
C. I’d like you to work on latch without the shield starting with skin to skin and allowing infant-led latch when the baby is not overly hungry.
D. IF your baby is sleepy during feeding, please keep him awake.
E. All of the above
© IABLE 10
You think about this mom and baby later, and come up with ideas as to why the baby’s weight
is low. What is the least likely reason for the insufficient weight gain?
A. The baby is ill and has a decrease in appetite.
B. The baby is falling asleep at the breast.
C. Mom’s production is low, possibly due to nipple shield use.
D. The baby does not transfer milk well with the shield
© IABLE 11
Mom calls, concerned that her 5 month old baby won’t nurse when she returns from work. She nurses the baby in the am, and pumps 3 times at work. She pumps ~3 oz each session, and believes that her milk production has decreased. The baby takes a 4 oz bottle of expressed milk every 3 hours at daycare. After work, the baby will only feed from a bottle, but will nurse in the middle of the night. You advise:
A. The baby loses the ability to coordinate the suck/swallow at the breast when awake and excited.
B. The baby may be too distracted to nurse at the breast.
C. The baby may be frustrated with the lower milk flow rate from the breast.
D. B & C
© IABLE 12
What would you recommend to this mother?
A. Try nursing before the baby is overly hungry, in a location where there are few distractions.
B. Don’t bottle feed. If the baby is hungry enough, she will nurse at the breast.
C. Arrange a visit to have her pump method checked for effectiveness.
D. Start solids in the evening so that mom does not need to pump and bottle feed.
E. A & C
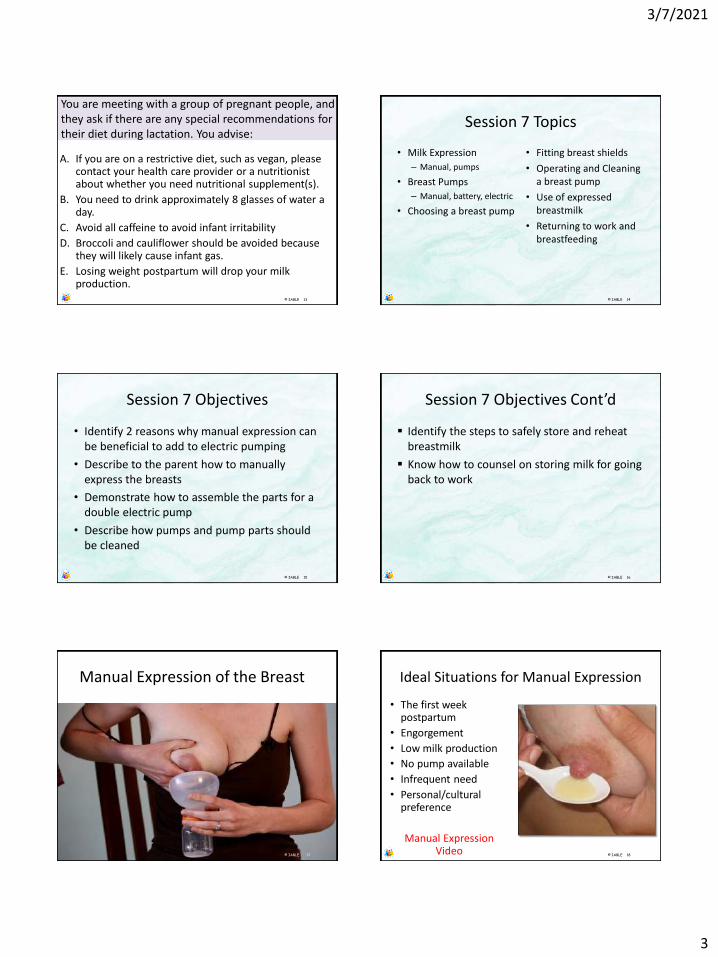
3/7/2021
3
© IABLE 13
You are meeting with a group of pregnant people, and they ask if there are any special recommendations for their diet during lactation. You advise:
A. If you are on a restrictive diet, such as vegan, please contact your health care provider or a nutritionist about whether you need nutritional supplement(s).
B. You need to drink approximately 8 glasses of water a day.
C. Avoid all caffeine to avoid infant irritability
D. Broccoli and cauliflower should be avoided because they will likely cause infant gas.
E. Losing weight postpartum will drop your milk production.
© IABLE 14
Session 7 Topics
• Milk Expression
– Manual, pumps
• Breast Pumps
– Manual, battery, electric
• Choosing a breast pump
• Fitting breast shields
• Operating and Cleaning a breast pump
• Use of expressed breastmilk
• Returning to work and breastfeeding
© IABLE 15
Session 7 Objectives
• Identify 2 reasons why manual expression can be beneficial to add to electric pumping
• Describe to the parent how to manually express the breasts
• Demonstrate how to assemble the parts for a double electric pump
• Describe how pumps and pump parts should be cleaned
© IABLE 16
Session 7 Objectives Cont’d
▪ Identify the steps to safely store and reheat breastmilk
▪ Know how to counsel on storing milk for going back to work
© IABLE 1717
Manual Expression of the Breast
© IABLE . 17 © IABLE 18
Ideal Situations for Manual Expression
• The first week postpartum
• Engorgement
• Low milk production
• No pump available
• Infrequent need
• Personal/cultural preference
Manual Expression Video

3/7/2021
4
© IABLE 19
Advantages to Manual
Expression
Advantages to Pump
ExpressionHands are easily available Expression might be faster
Only parts to wash are hands Improved comfort if manual
expression hurts
Can be done anywhere, no need for
electricity
Can be done hands free if using an
electric pump
Costs nothing Easier for people with physical
limitations
Increases milk production and fat
beyond pumping
Increases milk supply
Reduced risk of nipple trauma
No associated noise© IABLE. 19 © IABLE 20
Manual Breast Pumps
• No electricity used
• Vacuum is created by squeezing a handle or lever
• Most are single sided
• The individual has control over duration of each cycle and frequency of cycles
© IABLE 20
The Haakaa Milk Collector
• Soft, silicone
• Apply to the breast after squeezing
• Draws milk during a letdown
• Use on the other breast when pumping/nursing on one side• Only use if infant won’t nurse
from that breast or is done on that side• No stealing from the infant!
• May be traumatic due to high negative pressure and wide opening
© IABLE 22
Battery or Electric Powered Breast Pumps
Easier than a clothes washing
machine!
Proper use imperative to protect
milk production
Proper fit needed to
prevent injury!
© IABLE 23
Control Options for Electric or Battery Operated Breast Pumps
• Stimulation/massage mode• Stimulates let down w/fast, light suction• Not all pumps• Some pumps automatically start on them, others don’t
• Amount of suction• Most if not all pumps allow suction control• Ideal suction at -150 to -200mmHg during expression mode
• Rate of cycles• Some allow fast vs slow rate of pumping
• Single or double pumping
© IABLE 24
Electric Breast Pump
Stimulation mode
Speed/rate of suction cycles Degree of suction
pressure
✓ Stim mode✓ Suction control✓ Control over cycle rate

3/7/2021
5
Options for single/double pumping
Control over vacuum, not rate
Stimulation mode
✓ Stim mode✓ Suction control❑ No control over cycle rate
© IABLE 26
✓ Stim mode✓ Suction control❑ No control over
cycle rate
© IABLE 27
❑ No Stim mode✓ Suction control✓ Control over cycle rate
© IABLE 28
3 pre-set cycle rates
Controls for suction
Stimulationmode
✓ Stim mode✓ Suction control✓ 3 pre-set cycle rates
© IABLE 29
Wearable Pumps
ProsConvenient
Quiet
Rechargeable
ConsCan spill
Limited flange sizes
Limited volume
Expensive
© IABLE 30
✓ Stim mode✓ Suction control❑ No control over cycle
rate

3/7/2021
6
© IABLE 31
Pump Expression Video
© IABLE 32
Manual Vs Electric Pumps
Electric pumps o double pumping stimulates
higher productiono fastero need electricityo louder
Manual pumpso slower, takes longero hand fatigueo quiet
© IABLE 33
Factor SuggestionLowest cost Manual pump
Intermittent use for a stay-at-home parent
who plans to mainly nurse
Manual pump
Primary need is to increase milk
production
Double electric pump
Baby is separated from Parent; NICU Consider renting a hospital grade electric
pump*
Parent is back to work Double electric pump
Parent bottle feeds many feedings/day Double electric pump
No access to an electrical outlet Manual or battery operated pump
Easy to transport Lightweight pump in its own carrying case
© IABLE 33 © IABLE 34
Ease of Use
Size
Variety of Shield Sizes
PortabilityVersatility with Bottle
SizesSound
Options for Pump Cycles
# of Parts to Clean
Does Insurance Pay for It?
Is it Multiuser?
Factors to Consider When Choosing a Pump
© IABLE 35
FittingBreast Shields Most are standard
24mm size
Nipple should Not become stuck in shaft
Good Seal
Comfort and No nipple trauma are KEY
Center the Nipplein the Shield
© IABLE 36
Duckbills are essential for
vacuum
Must be Cleaned well,
INTACT, and in PLACE

3/7/2021
7
© IABLE 37
Steps When Using a Pump
• Wash hands with soap and water– Usually no need to
wash breast
– Use clean pump parts
• Assemble pump parts
• Find a comfortable place to pump
© IABLE 38
Other Pumping Tips
• Hands-free system• Start w/low suction or stimulation phase • Increase to highest comfortable vacuum• Manual expression during or after pumping as
needed
© IABLE 39
Freq/Duration of Pumping
• Pump every 3 hours• Average duration = 12-20
minutes• Average session = 2-3 let-
downs• High production
– limit volume expressed
• IF pumping takes 25+ minutes, check flange size and vacuum setting
CDC Guidelines for Cleaning Pump Parts
CDC Guidelines for Sanitizing Once a DayFor Infants Who are Premature, Ill, or < 3 months
• Boil for 5 minutes, remove with tong
• Steam in a microwave bag or plug-in steam system
• Dishwasher on sanitize cycle
• Bleach
– 1 tsp of bleach in 16 cups of water• Submerge completely and soak for 2 minutes
– Do not rinse, to avoid re-contamination• Bleach will break down as it dries and is safe
– Dry on a clean paper towel or unused dish towel
© IABLE 42
Milk Storage Containers
• Hard plastic bottles
– BPA- free
• Glass bottles
• BM storage bags
– Protect with added bag
– Avoid food-grade freezer bags
• Wash bottles in hot soapy water or dishwasher

3/7/2021
8
© IABLE 43 © IABLE 44
Additional Principles of Human Milk Storage
• Fresh is best!
• Freeze in 2-4 oz volumes
• New milk (chilled) can be added to older milk
• Leave room in container when freezing
• Write date and baby’s name before freezing
© IABLE 45
Using Expressed Milk
• Fresh– Heat in warm water
• Frozen– Defrost in a warm water bath
or overnight in refrigerator
– Use within 24 hours after thawed
– Use within a few hours after it is warmed
• Never reheat in a microwave!!
© IABLE 46
Toss or Donate Stored Milk?
• Reasons to not use stored milk:
– Baby is allergic to a substance in parent’s milk, e.g. food or medication
• Milk can be donated
• Very rare need to toss milk from a yeast or bacterial infection
© IABLE 47
All Stored Breastmilk has a Smell
• Due to an enzyme lipase breaking up the fat in the milk.– Not due to excessive lipase– Keep the bottle/bag airtight to decrease odor
• The longer it is stored in frig or freezer, the more it smells– Fresh milk is the least smelly
• Scalding milk is NOT recommended– Scalding destroys milk properties
• Most babies don’t care about the smell– We eat stinky foods- cheese, fish, eggs, cooked
broccoli/cauliflower
© IABLE 48
Return to Work• Discuss lactation needs with
employer– Longer lunch times to nurse
the baby
– Altered work schedule
– Part time work the first few weeks
• Find a supportive daycare– Many states have toolkits for
breastfeeding-friendly daycare centers (WI, RI, MN, CO, etc)
Source: US Breastfeeding Committee

3/7/2021
9
© IABLE 49
The Break Time for Nursing Mothers US Fair Labor Standards Act
• No defined frequency for breaks
• Break time must be ‘reasonable’ in duration
• Employer not required to pay for uncompensated breaks
• Mainly applies to hourly workers
• Not in bathroom• Sink not required• ‘Functional
space’• Shielded from
view• Free from
intrusion from others
• Available when needed
https://www.dol.gov/sites/dolgov/files/WHD/legacy/files/whdfs73.pdf
• Allowed for 1 year
© IABLE 50
Return to Work
• Learn tips from other lactating parents at the workplace
• Take as much postpartum leave as possible
• Store 1-4 oz of breastmilk/day starting at 3 weeks pp
• Store in 2-4 oz increments
• Introduce a bottle before going back to work
Source: US Breastfeeding Committee
© IABLE 51
Promoting a Letdown at Work
Source: US Breastfeeding Committee
‘Experience’ the baby• Photos/video• Article of clothing/blanket• Audio of the baby
• Massage/tickle breasts• Rub nipples• Warm packs
Get Comfy!• Music• Eat/drink• Distract • Feel safe
© IABLE 52
Conclusions Session 7
• Pump selection is based on individual needs
• Manual expression with pumping should be encouraged
• Parents often need guidance on proper breast shield size
• Offer counseling to mothers on breastmilk storage for work
• Parents often need guidance and preparation for going back to work and breastfeeding

3/7/2021
1
The OutpatientBreastfeeding
Champion Program
1
• The Instructor has no conflicts of interest to disclose
• Nursing credits, continuing education recognition points (CERPs) for IBCLE, or CPEUs for registered dietitians, are awarded commensurate with participation and complete/submission of the evaluation form.
Short Review ofSession 7 Topics
3
Which one is Accurate Advice about Using a Breast Pump?
A. The pump parts should be sterilized in boiling water daily.
B. The parent should pump for at least 10 minutes after the milk stops flowing.
C. Increase the pump vacuum to the highest comfortable setting.
D. All pumps start in a stimulation phase, and then automatically switch to expression phase.
4
Which of the Following is True regarding Breastmilk Storage?
A. Freshly expressed breastmilk is not safe to sit out at room temperature.
B. Frozen breastmilk that was thawed in the refrigerator, is good in the refrigerator for 3 days.
C. Breastmilk that has been in the freezer for 1 year is acceptable for consumption.
D. Expressed breastmilk is safe in a refrigerator for at least 8 days.
5
A mother of a 2 week old asks you when she should start pumping to store for work. Reasonable advice
includes:
A. Begin storing a few ounces a day starting at around 3 weeks.
B. Start storing about 15 oz a day so you have a freezer full when returning to work.
C. Don’t pump and store milk because it will drive your supply up too much. Wait until you start working.
6

3/7/2021
2
What is true about The Break Time for Nursing Mothers Law?
A. The law requires that employers have a sink available in the space to pump/nurse.
B. The law requires the employer to pay the employee for lactation break time.
C. A bathroom, even if private, is not a permissible location under the Act.
D. All of the above
7
Session 8 Topics
• Medications during Lactation
• Alcohol
• Tobacco Abuse
• Marijuana Use
• Using an Equity Lens in healthcare for populations
8
Session 8 Objectives
• Understand 2 basic principles of medications in human milk.
• Recite 2 reliable sources of information for medication use while breastfeeding.
• List 3 classes of substances that are contraindicated during breastfeeding.
• Identify components of an equity lens when working with populations.
9 10
Basic Principles of Meds and Human Milk
• Volume of distribution
• Half-life of drug- how long it hangs around
• Infant absorption
• Effect on milk production
11
Volume of Distribution
• Meds move from the parent’s blood into bmilk
• More likely to go into breastmilk if:
12
o Absorbed from the parent’s guto Drug is fat solubleo Little protein bindingo Small molecule

3/7/2021
3
Half-Life of Drug
• How long does it hang around?
–Choose meds that are short-acting
• Antidepressants
• Anti-anxiety meds
13
Infant Absorption
Choose medications that are not well absorbed from the infant gut
14
Meds- General Guidelines
• Most medications that are OK during pregnancy are fine
during lactation
– Decongestants are an exception
• Use evidence-based resources for medications during
lactation
– Lactmed- National Library of Medicine- free
– Medications in Mothers’ Milk by Tom Hale- $
– Infant Risk Center - infantrisk.com- free
– Mother To Baby - mothertobaby.org- free
– E-lactancia.org (from Spain, English and Spanish)- free
• Usually meds that are OK for infants are OK for lactation
• Choose the best med in a category
15
The List of Unsafe Meds is Short!
• Chemotherapy for maternal cancer
• Radioactive meds
• Codeine, tramadol
• Recreational drugs
– Occas marijuana is an exception
• Prolactin-lower meds such as
bromocriptine/cabergoline
• Always look up medications to be sure!
16
Alcohol During Breastfeeding
• Breastmilk level=blood level
• Alcohol in BM decreases infant’s intake
• Safe Rules:
– No more than 2 drinks a day, but don’t do this daily
– Each drink over 1-2 hours
– Eat food when drinking
• 5 drinks can decrease let-down and drop milk production
17
Smoking During Breastfeeding
• Smokers can breastfeed
• Increased risk of SIDS
• Decreased milk production– Dec’d PRL
– Dec’d blood flow to breast
• Possible decreased fat in breastmilk
• Reduce exposure by smoking right after feeding, not before
• Low dose nicotine replacement is preferred
18

3/7/2021
4
Marijuana During LactationAmerican Academy of Pediatrics 2018
• Marijuana use is not recommended during lactation
– Not enough info on transmission of marijuana into breastmilk
– Concerns that exposure to marijuana in breastmilk may have negative effects on the infant brain
– Infants and nursing mothers should avoid environments with second hand marijuana smoke
19
Notice the Triage Tool for Over-the-Counter Meds
20
Inequity in Breastfeeding Rates
• Lower breastfeeding rates among:
– African American women
– Lower socioeconomic groups
– Populations with lower education
– Geographic
• Southern USA
21States that have reached HP 2020 goals
What is Equitable Health Care?(US Institute of Medicine)
• Care that does not vary in quality because of:
– Race
– Gender
– Income
– Location
• Equal ≠ Equitable
22
Equitable Health Care Is Not The Same As Equal Health Care
With Permission from the Interaction Institute for Social Change
Create a Culture of Equity
24
Photo by Artem Zhukov Unsplash
Identify Opportunities to Improve
Breastfeeding Support in Your Community
Take Action to Improve Health Equity Using an
Equity Lens

3/7/2021
5
Apply an Equity Lens
• Equity lens
– Analyzes impact of policies and programs on vulnerable populations
• Work with individuals within the population(s)
– Enhances understanding
– Addresses trauma- informed care
– Builds trust in target populations
25 26
Examples of Working with Others in Populations toApply an Equity Lens
Communicate with and involve leaders- You learn that a rural Latinx population with a history of low breastfeeding rates has a major barrier- The local employer who expects all workers back 30 days after birth, and there are poor accommodations for lactation breaks
Trauma informed care- Your goal is to start a transgender lactation support group. You find out that transgender individuals are very uncomfortable discussing the option of lactation with local healthcare providers, given their history of receiving insensitive healthcare.
Build Trust – A public health department may have difficulty executing a postpartum in-home lactation support program in a Native American population without trained individuals of the community providing the in-home care.
Lets Apply an Equity Lens in a Community Breastfeeding Project
27 28
You Did It!! Congrats!Now Lets Practice a Few Cases…
Case #1
29
Case 1 Discussion
• What are the parent’s concerns?
• What are the parent’s goals?
• How can you empathize with her?
• What advice can you offer her?
– How can this be done in a shared-decision manner?
30

3/7/2021
6
Case #2
31
Case 2 Discussion
• What are mom’s concerns?
• What are mom’s goals?
• How can you empathize with her?
• What advice can you offer her?
– How can this be done in a shared-decision manner?
32
Conclusions Session 8
• Most medications are safe during nursing
• Use evidence-based resources to counsel on medications during breastfeeding
• Mothers who drink alcohol and who smoke may breastfeed, but there are ways to do this safely
• Applying an equity lens allows professionals to be impactful in vulnerable communities.
33