
Outline&& The&role&of&mental&illness&in& recidivism - Home - CEP Probation · 2017-12-18 · months...
11
11/12/2017 1 The role of mental illness in recidivism Seena Fazel, Department of Psychiatry, University of Oxford Outline • Background – recidivism and role of mental illness • New study • ImplicaJons • Risk assessment ReconvicJon rates are high Fazel & Wolf, PLoS One 2015 Reoffending rates not decreased over Jme in E&W Ministry of JusJce, StaJsJcs bulleJn 2012.
-
Upload
nguyendang -
Category
Documents
-
view
213 -
download
0
Transcript of Outline&& The&role&of&mental&illness&in& recidivism - Home - CEP Probation · 2017-12-18 · months...

11/12/2017
1
The role of mental illness in recidivism Seena Fazel,
Department of Psychiatry, University of Oxford
Outline
• Background – recidivism and role of mental illness
• New study • ImplicaJons • Risk assessment
ReconvicJon rates are high
Fazel & Wolf, PLoS One 2015
Re-‐offending rates not decreased over Jme in E&W
Ministry of JusJce, StaJsJcs bulleJn 2012.

11/12/2017
2
Previous reviews downplay clinical factors Are psychoJc disorders associated with recidivism?
Fazel, Scz Bull 2012
New study
• Swedish populaJon • High quality naJonal registers that can be linked accurately
• Similar rates of violent reoffending, mental illness and substance abuse in prisoners; lower rates of incarceraJon
Methods Population and data sources
INCLUSION CRITERIA
• All prison releases between 2000 and 2009
• Age 15-75
FOLLOW UP
• Violent crime at 1,2 and 5 years
SWEDISH REGISTERS
• Total Population Register
• Patient Register
• Cause of Death Register
• National Crime Register
• Longitudinal Integration Database

11/12/2017
3
QuesJons
• Is there an associaJon between mental disorders and violent reoffending?
• To what extent is this associaJon confounded? And by what?
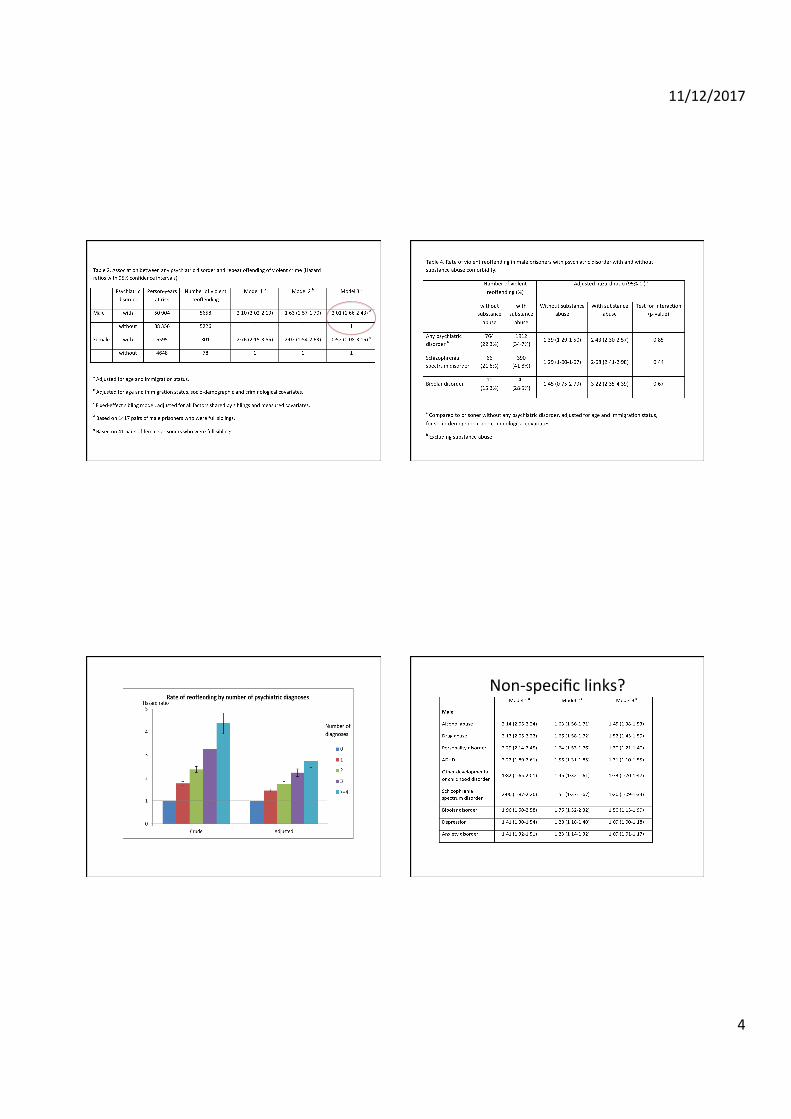
• Are there differences by individual diagnoses?
Sample descripJve staJsJcs
Male Female
Number of individuals 43840 3486
Any psychiatric disorder (%) 42.3 64.1
Alcohol abuse (%) 21.2 27.8
Drug abuse (%) 21.9 41.3
Personality disorder (%) 5.3 10.1
ADHD (%) 1.3 1.5
Other developmental or childhood disorder (%) 2.2 4.0
Schizophrenia spectrum disorder (%) 2.8 3.7
Bipolar disorder (%) 0.5 1.0
Depression (%) 5.8 12.0
Anxiety disorder (%) 7.4 15.3
0.00
0.20
0.40
0.60
0.80
1.00
Priso
ners
witho
ut re
offen
ding
0 2 4 6 8 10Year after release
Male prisoner without psychiatric disorderMale prisoner with psychiatric disorderFemale prisoner without psychiatric disorderFemale prisoner with psychiatric disorder
Kaplan-Meier survival estimates
Higher rates of violent recidivism Probability of violent reoffending by Jme aaer release
11/12/2017
4
Non-‐specific links?

11/12/2017
5
Findings are generalizable to other countries ImplicaJons
• NaJonal violence prevenJon strategies should include prison health
• Very lidle familial confounding suggesJng causality
• Non-‐specificity by diagnosis suggests shared mechanisms (emoJonal dysregulaJon?)
• MulJmorbidity important
Overall implicaJons
• ExplanaJons of reoffending – criminological, psychological, medical/public health
• What next for risk assessment? • What next for risk management?
New Scien1st, 2013
11/12/2017
6
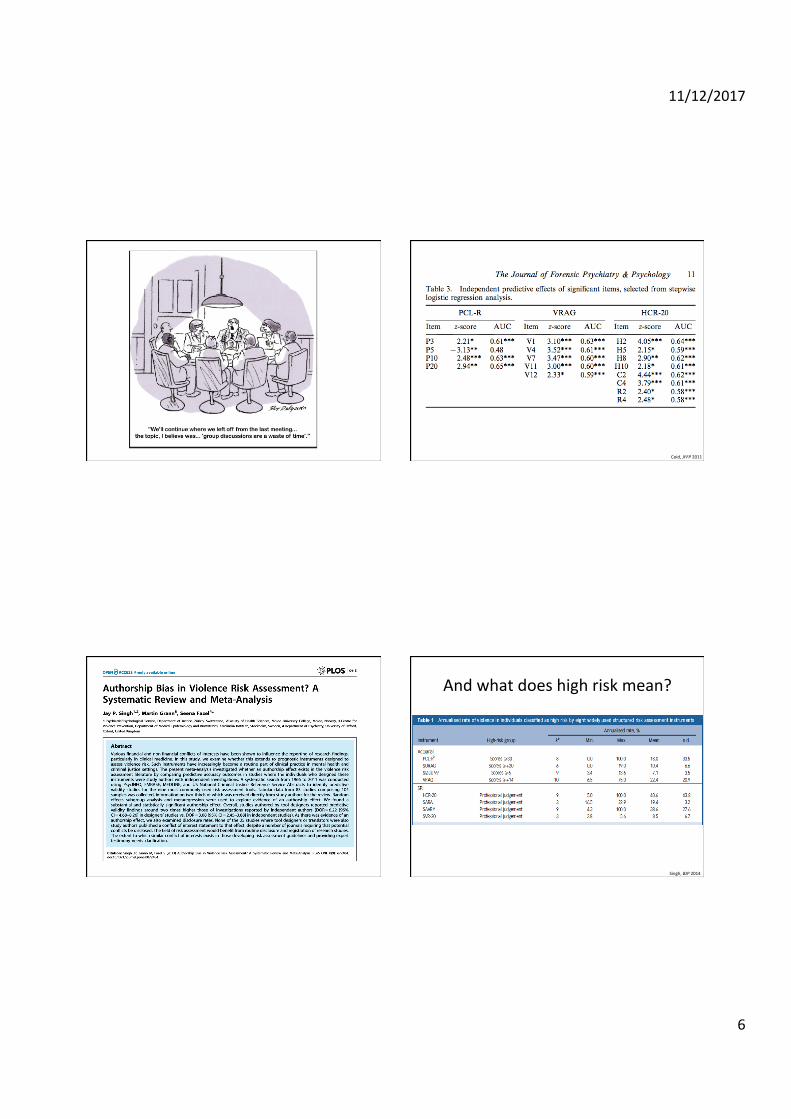
Coid, JFFP 2011
And what does high risk mean?
Singh, BJP 2014

11/12/2017
7
Problems
• Costly (direct and indirect) • Time consuming • Not transparent • PublicaJon bias • Evidence base is variable • Guru-‐like system of training • Meaningless cut-‐offs? • Don’t improve outcomes
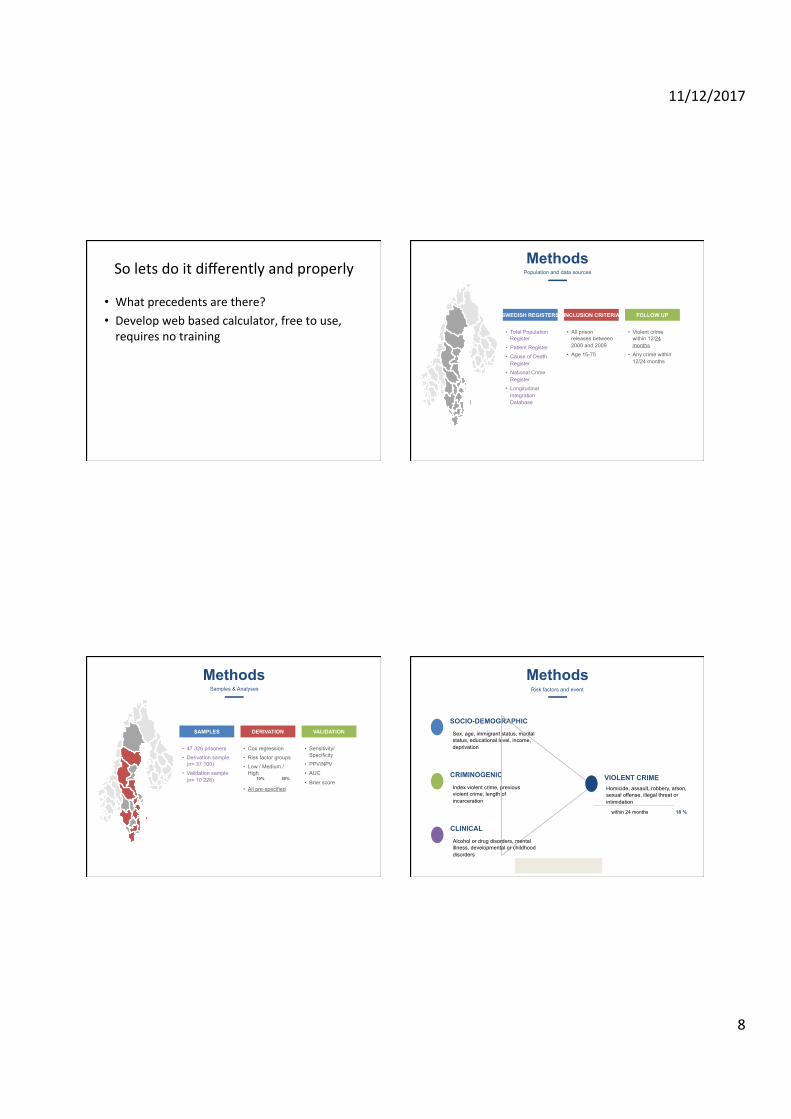
So lets do it differently and properly
• What precedents are there?
11/12/2017
8
So lets do it differently and properly
• What precedents are there? • Develop web based calculator, free to use, requires no training
Methods Population and data sources
INCLUSION CRITERIA
• All prison releases between 2000 and 2009
• Age 15-75
FOLLOW UP
• Violent crime within 12/24 months
• Any crime within 12/24 months
SWEDISH REGISTERS
• Total Population Register
• Patient Register
• Cause of Death Register
• National Crime Register
• Longitudinal Integration Database
Methods Samples & Analyses
DERIVATION
• Cox regression
• Risk factor groups
• Low / Medium / High 10% 50%
• All pre-specified
VALIDATION
• Sensitivity/Specificity
• PPV/NPV
• AUC
• Brier score
SAMPLES
• 47 326 prisoners
• Derivation sample (n= 37 100)
• Validation sample (n= 10 226)
Index violent crime, previous violent crime, length of incarceration
CRIMINOGENIC
Sex, age, immigrant status, marital status, educational level, income, deprivation
SOCIO-DEMOGRAPHIC
Homicide, assault, robbery, arson, sexual offense, illegal threat or intimidation
VIOLENT CRIME
Alcohol or drug disorders, mental illness, developmental or childhood disorders
CLINICAL
Methods Risk factors and event
18 % within 24 months

11/12/2017
9
Results Included risk factors
MALE 93 %
MEAN AGE 36 yrs
IMMIGRANT STATUS 31 %
LENGTH OF INCARCERATION
VIOLENT INDEX OFFENCE 38 %
PREVIOUS VIOLENT CRIME 53 %
UNMARRIED 65 %
EDUCATION
EMPLOYMENT 25 %
DISPOSABLE INCOME
NEIGHBOURHOOD DEPRIVATION
ALCOHOL USE DISORDER 22 %
ANY MENTAL DISORDER 22 %
DEVELOPMENTAL/CHILDHOOD DIS 3 %
1
2
3
DRUG USE DISORDER 23 %
ANY SEVERE MENTAL DISORDER 3 %
Variable Adjusted Odds Ratio
Sex (female) 0.51 (0.45-0.57)
Age (per 5 years) 0.84 (0.83-0.85)
Immigrant status 0.97 (0.92-1.02)
Length of incarceration 6-11 months 12-23 months 24+ months
0.85 (0.81-0.90) 0.69 (0.63-0.75) 0.55 (0.48-0.64)
Violent index offence 1.53 (1.46-1.59)
Previous violent crime 2.41 (2.29-2.54)
Unmarried 1.08 (1.02-1.15)
Education level 9-11 years 12+ years
0.83 (0.79-0.87) 0.65 (0.57-0.75)
Results Risk factor odds ratios
Variable Adjusted Odds Ratio
Employment 0.68 (0.63-0.72)
Disposable income Zero Low (<20º) Medium (20º - 80º) High (>80º)
1.69 (1.11-2.57) 1.68 (1.11-2.53) 1.45 (0.96-2.19) 1.57 (0.92-2.67)
Neighbourhood deprivation 1.03 (1.01-1.04)
Alcohol use disorder 1.41 (1.33-1.49)
Drug use disorder 1.51 (1.44-1.59)
Any mental disorder 1.09 (1.03-1.15)
Any severe mental disorder 1.10 (0.99-1.22)
Results Validation and web tool
NPV PPV
Specificity
99 %
Sensitivity
37 %
70 % 67 %
c-index (AUC)
.76

11/12/2017
10
Results Comparison with other tools
SENSITIVITY 67%
SPECIFICITY 70%
POSITIVE PREDICTIVE VALUE 37%
NEGATIVE PREDICTIVE VALUE 99%
AREA UNDER THE CURVE 0.76
SENSITIVITY 92%
SPECIFICITY 36%
POSITIVE PREDICTIVE VALUE 41%
NEGATIVE PREDICTIVE VALUE 91%
AREA UNDER THE CURVE 0.72
VIOLENCE TOOLS Mean values for HCR-20, SARA,
SAVRY, and VRAG*
OXRECOXFORD RISK OFRECIDIVISM TOOL
*Fazel et al., BMJ 2012
Conclusions • Scalable tool • Overall similar predicJve abiliJes to current approaches
• More effecJve targeJng than current tools – sensiJvity 67%
• IdenJfies those with drug and alcohol needs, and mental health problems
• Simple way of providing BASELINE risk • Needs to be complemented with more individualised needs assessments
Published paper
www.thelancet.com/psychiatry Vol 3 June 2016 535
Articles
Lancet Psychiatry 2016; 3: 535–43
Published OnlineApril 13, 2016http://dx.doi.org/10.1016/S2215-0366(16)00103-6
See Comment page 493
Department of Psychiatry, Warneford Hospital (Prof S Fazel MD, Z Chang PhD) and Department of Primary Care Health Sciences (T Fanshawe PhD), University of Oxford, Oxford, UK; Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden (Z Chang, Prof N Långström PhD, Prof P Lichtenstein PhD, Prof H Larsson PhD); Department of Medical Sciences, Örebro University, Stockholm, Sweden (Prof H Larsson); Research and Evaluation Department, Swedish Prison and Probation Administration, Sweden (Prof N Långström); and School of Population and Health Sciences, University of Birmingham, UK (S Mallett PhD)
Correspondence to:Prof Seena Fazel, Department of Psychiatry, Warneford Hospital, University of Oxford, Oxford, OX3 7JX, [email protected]
Prediction of violent reo! ending on release from prison: derivation and external validation of a scalable toolSeena Fazel, Zheng Chang, Thomas Fanshawe, Niklas Långström, Paul Lichtenstein, Henrik Larsson, Susan Mallett
SummaryBackground More than 30 million people are released from prison worldwide every year, who include a group at high risk of perpetrating interpersonal violence. Because there is considerable inconsistency and ineffi ciency in identifying those who would benefi t from interventions to reduce this risk, we developed and validated a clinical prediction rule to determine the risk of violent off ending in released prisoners.
Methods We did a cohort study of a population of released prisoners in Sweden. Through linkage of population-based registers, we developed predictive models for violent reoff ending for the cohort. First, we developed a derivation model to determine the strength of prespecifi ed, routinely obtained criminal history, sociodemographic, and clinical risk factors using multivariable Cox proportional hazard regression, and then tested them in an external validation. We measured discrimination and calibration for prediction of our primary outcome of violent reoff ending at 1 and 2 years using cutoff s of 10% for 1-year risk and 20% for 2-year risk.
Findings We identifi ed a cohort of 47 326 prisoners released in Sweden between 2001 and 2009, with 11 263 incidents of violent reoff ending during this period. We developed a 14-item derivation model to predict violent reoff ending and tested it in an external validation (assigning 37 100 individuals to the derivation sample and 10 226 to the validation sample). The model showed good measures of discrimination (Harrell’s c-index 0·74) and calibration. For risk of violent reoff ending at 1 year, sensitivity was 76% (95% CI 73–79) and specifi city was 61% (95% CI 60–62). Positive and negative predictive values were 21% (95% CI 19–22) and 95% (95% CI 94–96), respectively. At 2 years, sensitivity was 67% (95% CI 64–69) and specifi city was 70% (95% CI 69–72). Positive and negative predictive values were 37% (95% CI 35–39) and 89% (95% CI 88–90), respectively. Of individuals with a predicted risk of violent reoff ending of 50% or more, 88% had drug and alcohol use disorders. We used the model to generate a simple, web-based, risk calculator (OxRec) that is free to use.
Interpretation We have developed a prediction model in a Swedish prison population that can assist with decision making on release by identifying those who are at low risk of future violent off ending, and those at high risk of violent reoff ending who might benefi t from drug and alcohol treatment. Further assessments in other populations and countries are needed.
Funding Wellcome Trust, the Swedish Research Council, and the Swedish Research Council for Health, Working Life and Welfare.
Copyright © Fazel et al. Open Access article distributed under the terms of CC BY.
IntroductionTo reduce the mortality and morbidity burden associated with interpersonal violence, the identifi cation of, and intervention with, prisoners at high risk of perpetrating violence provides an approach with considerable public health and safety benefi ts.1 Repeat off ending rates remain high in many high-income countries,2 and have not followed the downward trend of violence reported in these countries.3 In England and Wales, prisoners have been reconvicted at a 2-year rate of 55%–60% for the past decade.3 With about 30 million individuals entering and leaving prison per year worldwide,4 the contribution of this population to societal violence is high, and an estimated 20% of all arrests in the USA,5 and 18% of new crimes in the UK,6 are by former prisoners.
To identify individuals who are at the highest risk of reoff ending and most in need of interventions to reduce future criminality, criminal justice agencies in most
high-income and middle-income countries have used actuarial and clinically informed decision aids. These aids assist with decisions about sentencing, entry into specifi c programmes for prison treatment and aftercare, and the timing of release from detention and need for supervision on release. More than 300 of these risk assessment tools exist, but they are limited by low to moderate accuracy,7 fi nancial and non-fi nancial competing interests aff ecting the research evidence,8 and inconsistent defi nitions of risk classifi cations.9 Typically, these tools identify prisoners at low, medium, and high risk of repeat off ending on the basis of an assessment weighted towards historical non-modifi able factors. Many of the tools are expensive to use and require training to administer. Another problem is that they are usually developed without predetermined protocols, the use of which enhances transparency and reduces bias by clarifying key elements in research design before data acquisition or analysis, and hence increasing
Results Summary • High rates of recidivism • Previous reviews of role of mental illness misleading
• New research using large sample, novel design, reliable exposures and hard outcomes
• All mental disorders associated with violent recidivism
• NaJonal violence strategies, prison health services, and risk assessment need review in light of this
11/12/2017
11
References (open access) • Fazel S, Chang Z, Fanshawe T, Långström N, Lichtenstein P, Larsson H, Malled S.
PredicJon of violent reoffending on release from prison: derivaJon and external validaJon of a scalable tool. Lancet Psychiatry 2016; 3: 535-‐543. PMID: 26946390
• Chang Z, Larsson H, Lichtenstein P, Fazel S. Psychiatric disorders and violent reoffending: a naJonal cohort study of convicted prisoners in Sweden. Lancet Psychiatry 2015; 2: 891-‐900. PMID: 26342957.
• OxRec: www.oxrisk.com/oxrec
Acknowledgements
Achim Wolf Psychiatry, Oxford
Zheng Chang Karolinska Institutet
Henrik Larsson Karolinska Institutet
Paul Lichtenstein Karolinska Institutet
Susan Mallett University of Birmingham
[email protected] Twitter: @seenafazel
Johan Zetterqvist Karolinska Institutet
Niklas Långström Karolinska Institutet
Thomas Fanshawe Primary Care, Oxford






![2015 Recidivism Report - WODC 2016-1a_nw_tcm28-266946.pdf · namely Reclassering Nederland [Dutch Probation Service], Stichting Verslavingsreclassering GGZ [Dutch Addiction Probation](https://static.fdocuments.in/doc/165x107/5f1a68eb157a0e0d05254e2f/2015-recidivism-report-wodc-2016-1anwtcm28-namely-reclassering-nederland.jpg)






![FedCURE Report: Briefing Materials [55 pages]€¦ · CAN PROBATION AND PAROLE SUPERVISION REDUCE RECIDIVISM? ... North Carolina, ... Distribution of District ofCoIumbia Offenders](https://static.fdocuments.in/doc/165x107/5b00db747f8b9ad85d8d32ac/fedcure-report-briefing-materials-55-pages-can-probation-and-parole-supervision.jpg)




