OUTLINE
68
TOPIC:MANAGEMENT OF UPPER GASTROINTESTINAL BLEEDING PRESENTING UNIT:GASTROENTEROLOGY PRESENTER:UGWUNZE E.O DATE:10 MARCH 2014
-
Upload
nayda-fisher -
Category
Documents
-
view
20 -
download
1
description
TOPIC:MANAGEMENT OF UPPER GASTROINTESTINAL BLEEDING PRESENTING UNIT:GASTROENTEROLOGY PRESENTER:UGWUNZE E.O DATE:10 MARCH 2014. OUTLINE. INTRODUCTION EPIDEMIOLOGY CLASSIFICATION AETIOLOGY CLINICAL FEATURES[HX AND PHYSICAL EXAMINATION] INVESTIGATIONS TREATMENT PROGNOSIS CONCLUSION. - PowerPoint PPT Presentation
Transcript of OUTLINE

TOPIC:MANAGEMENT OF UPPER GASTROINTESTINAL BLEEDING
PRESENTING UNIT:GASTROENTEROLOGYPRESENTER:UGWUNZE E.O
DATE:10 MARCH 2014

OUTLINE• INTRODUCTION• EPIDEMIOLOGY• CLASSIFICATION• AETIOLOGY• CLINICAL FEATURES[HX AND PHYSICAL
EXAMINATION]• INVESTIGATIONS• TREATMENT• PROGNOSIS• CONCLUSION

INTRODUCTION
Upper gastrointestinal bleeding (UGIB)• is a potentially life-threatening abdominal emergency • results in high morbidity and mortality hence requires
admission for urgent diagnosis and management.• approximately 4 times as common as bleeding from
the lower GI tract • bleeding derived from a source proximal to the
ligament of Treitz .• Can be categorized as variceal or non - variceal

EPIDEMIOLOGY
• The incidence of UGIB is approximately 100 cases per 100,000 population per year.
• England.Wales - 20,000 hospital admission per year.
• USA - 100,000 admission per year.• The incidence of UGIB is 2 fold
greater in males than in females.• Mortality increases with older
age[>60yrs] in males and females.

• In Nigeria, a retrospective endoscopic study done on aetiology of UGIB by Mustapha et al in University of Maiduguri TH and FMC Gombe[2003 to 2008] showed :
• A preponderance of male affectation[69.8% vs 30.2%]- 2fold increase in M:F.
• Oesophageal varices were the commonest cause of UGIB ffg by erosive mucosal disease ,then PUD.
• Mortality rate of 17.9%[all mortality in patients with variceal bleeding] compared with 10% in most western studies.

CLASSIFICATION
Nonvariceal bleeding• high pressure arterial haemorrhage - ulcer
mucosal, deep tears • low-pressure venous haemorrhage,
telangiectasia, and angioectasias vascular malformation that represents an abnormal dilation of mucosal and submucosal vessels

Variceal haemorrhage• elevated portal pressure transmitted to
esophageal and gastric varices and resulting in portal gastropathy.
• A complication of end stage liver disease.

AETIOLOGY
Common causes of UGIB• Duodenal (DU) and Gastric ulcers
(GU) (50% of bleeds),DU>GU.• Varices – Gastric , Oesophageal.• Acute gastric/duodenal erosions.
• Mallory weiss tears.• Erosive Oesophagitis.

LESS COMMON CAUSES :• Boerhaave syndrome• GAVE(gastric antral vascular ectasia)(chronic
GIB).• Dieulafoy leison
• Gastric carcinoma,• Gastrinoma• Stomal Ulcer• Oesophageal Ulcer• Oesophageal carcinoma

Rare causes of UGIB.o Benign gastric tumourso Duodenal tumourso Arterial aneurysms, aorto-enteric
fistulao Pseudoxanthoma elasticum.o Hereditary haemorrhagic
telangiectasia(Osler- Weber-Rendu syndrome).

• Haemangiomas• Bleeding disorders • Munchausen Syndrome(factitious
uppr GIT bleed).


MANAGEMENT
• Involves• history taking ,• physical examination• investigations• treatment

HISTORY
A good and careful history taking• Patient history includes• weakness,• dizziness,• syncope assoc with Haematemesis,
(coffee ground vomitus)• melaena (black stools with a rotten
odour),• haematochezia (red or maroon stools)-seen in brisk UGIB and suggests a large
upper tract hemorrhage.

o Previous history of dyspepsia (esp. nocturnal symptoms)
o peptic ulcer disease, o early satiety,o nonsteroidal anti-inflammatory drug
or aspirin use. o hematemesis or meleana w/out
previus hx of dyspepsia• Hx of chronic renal disease.

• Vomiting may point to Mallory weiss tears.
• Weight loss, dysphagia, anorexia may be associated with malignancy .

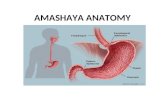
PHYSICAL EXAMINATIONo Objectives of the physical exam.o Assess the Haemodynamic state of patient
and Determine the degree of shock.• Pulse and Bp should be checked supine
and Upright positions to note effect of blood loss.
• A systolic Bp < 100mmHg and pulse > 100/min indicate a 20% depletion of blood volume or more.
• Tachycardia and Hypotension, indicate hypovolaemia.

o Other signs of shock includeo cool extremities,o oliguria,o chest pain,o presyncope, o confusion, o delirium.o Haematemesis and malaena to be noted.o Anaemia – indicates chronic blood loss

o Signs of chronic liver disease should be noted –
o spider angiomata.o gynaecomastia.o splenomegaly.o ascites.o pedal oedema.
o Asterixis.

o Signs of malignancy should be noted and portend a poor progress –
o nodular liver,o abdominal mass,o firm lymphadenopathy suggestive.o Subcutaneous emphysema with a
history of vomiting suggestive of Boerhaave syndrome (Oesophageal perforation).
o Telangiectasias – may indicate rare Osler Weber-Rendu Syndrome.

INVESTIGATIONS
• FBC: Hb may be normal or low.• Grouping and crossmatching of blood based
on the rate of active bleeding(e.g 2 – 6 units).• BUN-to-creatinine ratio: value > 36 in a pxt
without renal insufficiency is suggestive of UGIB.

• Coagulation profile: PT, APTT,INR(coagulopathy, advanced liver disease)
• Platelet count.• LFT.• Serum calcium:hypercalcemia increases acid
secretion.• Gastrin level.

ENDOSCOPYo Early endoscopy within 24hrs and after
resuscitation.o Urgent in patients with shock, liver disease,
continued bleeding.o Cause of bleeding detected in > 80%o Can detect more likely cases to rebleed.o Varices can be injected at first endoscopyo Bleeding ulcers may be injected or vessels
coagulated.o Improve rebleed but do not significantly improve
mortality rebleed .Other Investigations.o Chest radiographs, Abd-x-Ray < supine, upright.o Barium studies – can affect endoscopy

Bleeding pud

Mallory-Weiss tear

Oesophageal varices

• CT scan and ultrasonography – cirrhosis, cholecystitis, pancreatitis, with pseudocyst and haemorrh, aorto- enteric fisfula, etc.
o Nuclear medicine scan - areas of active bleeding
o Angiography – Important as salvage therapy, embolization of bleeding vessel in failed endoscopic therapy.
o Nasogastric lavage ; o confirm recent bleeding, active bleeding etco Can reduce patient’s need to vomito Character of nasogastric lavage fluid > severity
of bleeding

HISTOLOGICAL FINDINGS.
o Bleeding vessel in ulcer.o Fibrinoid necrosis, pseudoaneurysmal dilation of vessel.
o Take biopsy samples from edge of gastric ulcer to rule out cancer.
o H pylori lesion – chronic active gastritis with organisms in stained sample

PRINCIPLES OF MANAGEMENT1.Assessment
*Brief and essential history *Physical examination
2.Resuscitation *I.V. fluids – crystalloids, colloids, blood
*Urethral catheterisation *C.V.P. line
3.Re-assessment4.Endoscopy – OGD (diagnostic/therapeutic)
5.Other investigations6.Definitive treatment
7.Follow - up

RESUSCITATION



















Endoscopy
• Injection of epinephrine or sclerosants,• heater-probe coagulation,• bipolar electrode coagulation,• laser coagulation• endoscopic application of clips, • use of banding devices, • argon plasma coagulation.

surgery• The indications for surgery in patients with bleeding
peptic ulcers are as follows:• Severe, life-threatening hemorrhage not responsive to
resuscitative efforts• Failure of medical therapy and endoscopic hemostasis
with persistent recurrent bleeding• A coexisting reason for surgery, such as perforation,
obstruction, or malignancy• Prolonged bleeding, with loss of 50% or more of the
patient's blood volume• A second hospitalization for peptic ulcer hemorrhage

• The common operations for the management of a bleeding gastric ulcer include:
• (1) truncal vagotomy and pyloroplasty with a wedge resection of the ulcer,
• (2) antrectomy with wedge excision of the proximal ulcer,
• (3) distal gastrectomy to include the ulcer, with or without truncal vagotomy, and
• (4) wedge resection of the ulcer only.

• The 3 most common operations performed for a bleeding duodenal ulcer are as follows :
• Truncal vagotomy and pyloroplasty with suture ligation of the bleeding ulcer
• Truncal vagotomy and antrectomy with resection or suture ligation of the bleeding ulcer
• Proximal (highly selective) gastric vagotomy with duodenostomy and suture ligation of the bleeding ulcer

• In Boerhaave syndrome prompt surgical intervention is necessary to prevent mediastinitis and sepsis.
• surgical intervention in Mallory-Weiss syndrome is required to achieve hemostasis in only 10% of cases as bleeding from a Mallory-Weiss tear spontaneously ceases in 50-80% of patients by the time endoscopy is performed.

• In Dieulafoy Lesion contact thermal ablation with a heater probe is the most effective technique, with or without the combined use of epinephrine to slow or stop the bleeding prior to applying the heater probe.
• a combined endoscopic and surgical approach has now been adopted as the preferred method of treatment.

Angiodysplasia Treatment
• Because the lesions are small and superficial, endoscopic therapy is highly successful.
• Endoscopic treatments and devices used for hemostasis include
• lasers,• contact heat probes,• electrocoagulation, • and injection

AORTOENTERIC FISTULA
• Once the diagnosis of aortoenteric fistula is confirmed or seriously considered, emergency surgical intervention is required.
• The perioperative mortality rate is 22-75%,
and major complications are common.

Treatment Complications
• Complications of endoscopic therapy include• aspiration pneumonia and perforation (1% for
the first endoscopic therapy, 3% for the second).
• Bleeding can be caused by drilling into the vessel with the laser, by perforating the vessel with an injection, or by removing the clot with failure to coagulate the vessel.

• Incidence of ventricular arrhythmias during endoscopy - 42% (patients with CAD) versus 16% (controls)
• Complications from emergency abdominal surgery include
• ileus,• sepsis,• poor wound healing,• and myocardial infarction.

• Salvage surgery is associated with a high mortality rate, reflecting the comorbidities of patients who rebleed or continue to bleed.

Post treatment care
• The 2010 international consensus guidelines on UGIB state that selected low-risk patients may be discharged immediately following endoscopy, but high-risk patients should remain hospitalized for at least 72 hours.
• The goal is to maintain the intragastric pH above 6 to maintain the clot.
• This is most easily achieved by intravenous proton pump inhibitor (PPI) therapy.

Post treatment care
• After the acute phase, 72 hours, the coagulated vessel should be stable and the patient can be switched to oral therapy.
• If the patient rebleeds or has ongoing bleeding, then repeat of endoscopic therapy would be considered.
• If this is not successful, then interventional radiology is performed to clot the bleeding vessel. If this fails, then surgery would be considered.

MORTALITY/PROGNOSIS
• The overal mortality –10%• Approximately 80% of ulcers stop
bleeding.• Patient age and comorbidities
increase mortality.• Rebleeding or continuned bleeding
increases mortality.• It is important to separate patient
with low probability of rebleeding from high risk group.


• A pre endoscopic Rockall score of > 0 is an indication for endoscopy while patients with a post-endoscopic Rockall score of less than 3 have a low risk of rebleeding or death and are candidates for early discharge and outpatient follow up , if > 8 it means there is a high risk of death.
• Other prognostication systems include: -Blatchford-Glasgow Score(no need for endoscopy) -Forrest classification -AIMS 65

• The following risk factors are associated with increased mortality,
• recurrent bleeding,• the need for endoscopic hemostasis, or
surgery • Age older than 60 years• Severe comorbidity• Coagulopathy.

• Active bleeding (eg, witnessed hematemesis, red blood per nasogastric tube, fresh blood per rectum)
• Hypotension• Red blood cell transfusion greater than or equal
to 6 units• Inpatient at time of bleed• Severe coagulopathy• Hamorrhagic shock on presentation

CONCLUSION
• Acute gastrointestinal bleeding is a potentially life-threatening abdominal emergency that remains a common cause of hospitalization.
• Requires aggressive resuscitative measures.• Has a high morbidity and mortality if not
promptly and adequately managed.
















![[ Outline ]](https://static.fdocuments.in/doc/165x107/56815a74550346895dc7db61/-outline--56b49f971d862.jpg)
