
Otthoni vérnyomásmérés tapasztalatai - III. SZ ... · PDF...
56
Glomerulopathies Dr. András Tislér 2013
Transcript of Otthoni vérnyomásmérés tapasztalatai - III. SZ ... · PDF...

Glomerulopathies
Dr. András Tislér
2013


Glomerular diseases may be classified as:
• Primary renal disease vs. renal manifestation of a systemic disease (i.e. secondary)
• Immune vs. non-immune mechanism mediated
• Proliferative vs. non-proliferative glomerular pathology
– Different pathatological entities
• Clinical syndromes
– Isolated hematuria, nephrotic sy., nephritic sy., RPGN…
– Acute, subacute, chronic, „acute-on-chronic”

Immune mechanisms in glomerular diseases
• Antibody against a local antigen
– Podocyte antigen (membranous GN: phospolipase A2
receptor)
– Glomerular basement menbrane antigen (Goodpasture’s)
– planted antigen (e.g. in membranous SLE)
• Deposition of circulating immune complexes with
inflammation
– E.g. IgA nephropathy, cryoglobuliemia, SLE
• Without immune complexes („pauci immun”), but with
immune mechanism
– ANCA associated diseases

•Non-inflammatory (non-
proliferative) glomerulopathy
•Podocyta damage
•Subepithelial immune complexes
•Inflammatory (proliferative) GN
•Endothel (postinfectious GN)
•Mesangial proliferative (IgA
nephropathy)
•Parietal epithelial cell proliferation
( crescents)
•Membranoprolierative GN
Mechanisms of glomerular injury (bases for the
pathological classification)

Clinical approach to glomerular diseases
Clinical syndrome
Pathology Etiology
Nephrotic Non-proliferative Primary
nephritic Proliferative Neoplasia
RPGN
Acute renal failure sy
Autoimmune
Vasculitis
Isolated proteinuria
isolated hematuria
drugs
Infection

Nephrotic syndrome
• Proteinuria (usually>2-3 g/die)
• Hypalbuminemia
• Oedema
• Hyperlipoproteinemia
• Increased risk of thrombosis
• GFR may be norm.

Most frequent pathology behind the nephrotic syndrome in
adults
• Primary renal disease
– Minimal change glomerulopathy
– Focal segmental GN
– Membranous glomerulopathy
– Fibrillary (immunotactoid) GN
• Systemic disease
– Diabetes
– Amyolidosis
– SLE (type V)

Frequent complications of nephrotic syndrome
•
•Thrombosis (renal vein, deep venous)
• Frequent infections
• Acute prerenal renal failure
•Heavy proteinuria in itself contributes to the
progression of renal disease
• Accelerated atherosclerosis (?)

Management of nephrotic syndrome
• supportive management
• diuretics: Furosemide
Furosemide + thiazide
Furosemide + spironolactone
- ACE inhibitors/ ARBs
- Thrombosis profilaxis: heparin, oral anticoagulation
(if albumuin <20-25 g/L)
- Statins
• specific treatment: depends on pathology and ethiology
(e.g. immunsuppression)

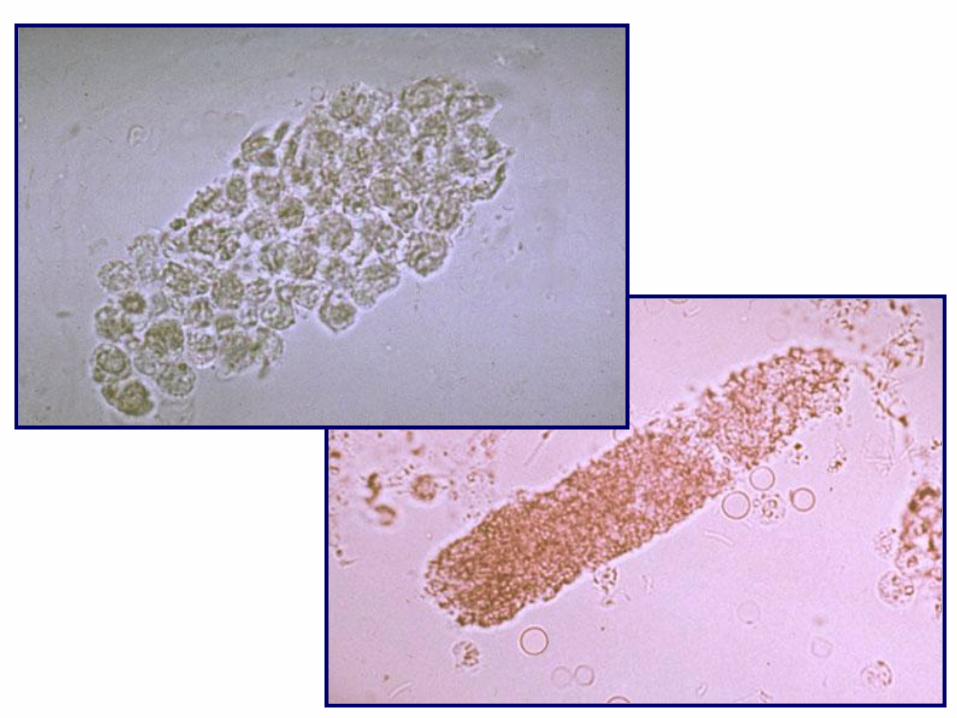
Acute glomerulonephritis (nephritic) syndrome
• Hematuria
(dysmorphic RBCs, acanthocytes)
• Proteinuria
• Cylindruria
(cellular, RBCcasts)
• Hypertension
• Oedema
• Oliguria
• Decreased GFR

Frequent pathologies behind the acute nephritic syndrome
(but may present in other syndromes as well)
• Post-streptococcal GN
•acute diffuse proliferative – endocapillary proliferative
• IgA nephropathy
•Mesangial proliferative
• Membranoproliferative GN
• SLE: focal vs. diffuse proliferative GN (types II-IV)

Isolated hematuria syndrome
• Glomerular causes (non glomerular
causes – stone neoplasm, papillary
necrosis etc. should be excluded)
•Thin basement membrane disease
•IgA nephropathy
• Alport syndrome
• persistent microhematuria
•dysmorphic RBCs, acanthocytes
•Variable proteinuria (from minimal to
nephrotic range)
•Variable decrease in GFR

Rapidly progressive GN syndrome (crescentic GN)
• Progressive loss of GFR (weeks, months)
• Active urinary sediment
– RBCs, cellular and granular casts
– Variable proteinuria
• Frequent systemic symptoms
– vasculitis
– upper-lower airway
– Pulmonary (bleeding)
– Arthritis
– fever

Causes of rapidly progressive GN syndrome
I. Anti-GBM antibodies (linear deposition
on immunfluorescence)
• Goodpasture syndr.,
II. Immune complex mediated GN (granular deposition on IF)
• Primary GN: IgA GN, Membranoproliferative GN
• Postinfectios: sepsis, abscess, endocarditis, HBV,
• Autoimmune: SLE
III. ANCA associated GN (no immune deposition = pauci immune)
• Wegener’s granulomatosis
• Microscopic polyangiitis
• Churg Strauss syndr

Clinical approach to glomerular diseases
Clinical syndrome
Pathology Etiology
Nephrotic Non-proliferative Primary
nephritic Proliferative Neoplasia
RPGN
Acute renal failure sy
Autoimmune
Vasculitis
Isolated proteinuria
isolated hematuria
drugs
Infection

•Non-inflammatory (non-
proliferative) glomerulopathy
•Podocyte damage
•Subepithelial immune complexes
•Inflammatory (proliferative) GN
•Endothel (postinfectious GN)
•Mesangial proliferative (IgA
nephropathy)
•Parietal epithelial cell proliferation
( crescents, extracapillary)
•Membranoprolierative GN
Mechanisms of glomerular injury (bases for the
pathological classification)

Clinical diagnosis
Syndrome
Acute nephritis sy.
Nephrotic sy.
Isolated proteinuria,
haematuria sy.
Rapidly progressive
glomerulonephritis
Chronic renal failure sy.
Acute renal failure sy.
Morphological
diagnosis
Postinfect. GN
Minimal change
Focal segmental GS
Membranous GN
Membranoprolif. GN
Crescens GN (necrotic)
Mesangial prolif GN
Diabetic nephropath
Amyloidosis
Myeloma
Acute tubular necrosis
Etiological
diagnosis
Primary (unknown)
Hepatatis C
Hepatitis B
SLE
Neoplasm
Vasculitis
Wegener gr.
Goodpasture sy.
Diabetes
Amyloidosis
Myeloma
Ischemia
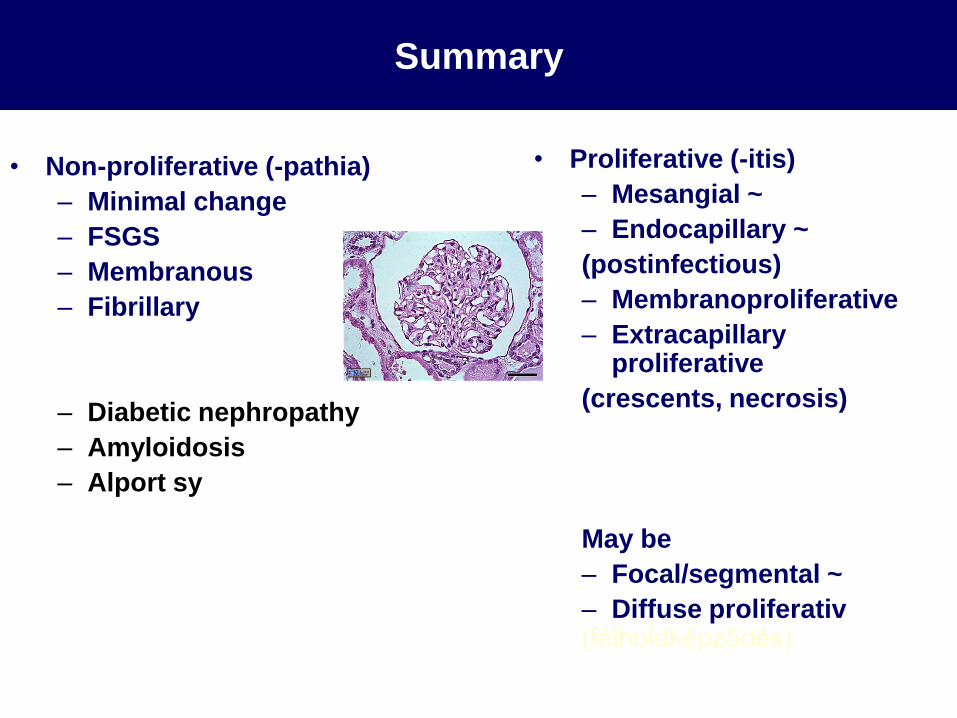
Summary
• Non-proliferative (-pathia)
– Minimal change
– FSGS
– Membranous
– Fibrillary
– Diabetic nephropathy
– Amyloidosis
– Alport sy
• Proliferative (-itis)
– Mesangial ~
– Endocapillary ~
(postinfectious)
– Membranoproliferative
– Extracapillary proliferative
(crescents, necrosis)
May be
– Focal/segmental ~
– Diffuse proliferativ (félholdképződés)

Hystology and clinical syndrome
Nephrosis Nephritis
Minimal change dis. ++++ -
Membranous GN ++++ +
Diabetic gl.sclerosis ++++ +
Amyloidosis ++++ +
FSGS +++ ++
Fibrillary GN +++ ++
Mesangioproliferative ++ +++
Membranoproliferative ++ +++
Proliferative (foc./diff.) ++ +++
Extrakapillaris (RPGN) + ++++

Minimal change disease
•
•Idiopathic nephrotic sy. (most frequently)
•Secondary
• M. Hodgkin
•allergy (pollen, beesting, food, dust)
• drugs: NSAID, ampicillin, gold, penicillamine
•Infections: HIV, EBV, schistosomiasis
• Immunisation
• Dermatitis herpetiformis


Minimal change nephropathy
• T-cell dysfunction?
• Podocyte effacement
• ? Podocyte slit membrane
damage
• ? Non-immune permeability
factor factor
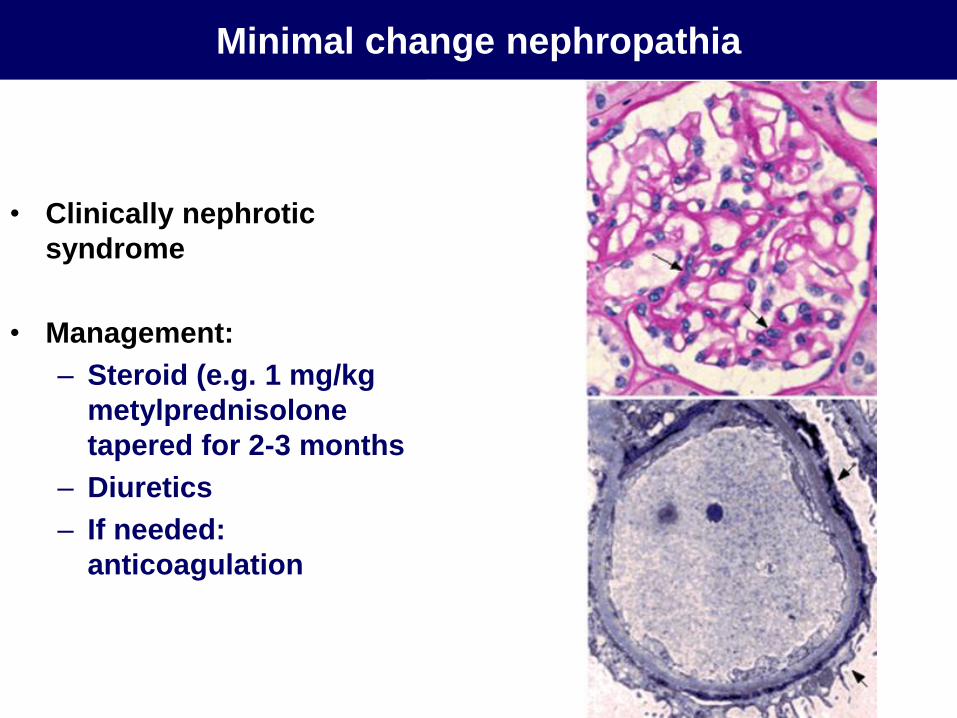
Minimal change nephropathia
• Clinically nephrotic
syndrome
• Management:
– Steroid (e.g. 1 mg/kg
metylprednisolone
tapered for 2-3 months
– Diuretics
– If needed:
anticoagulation

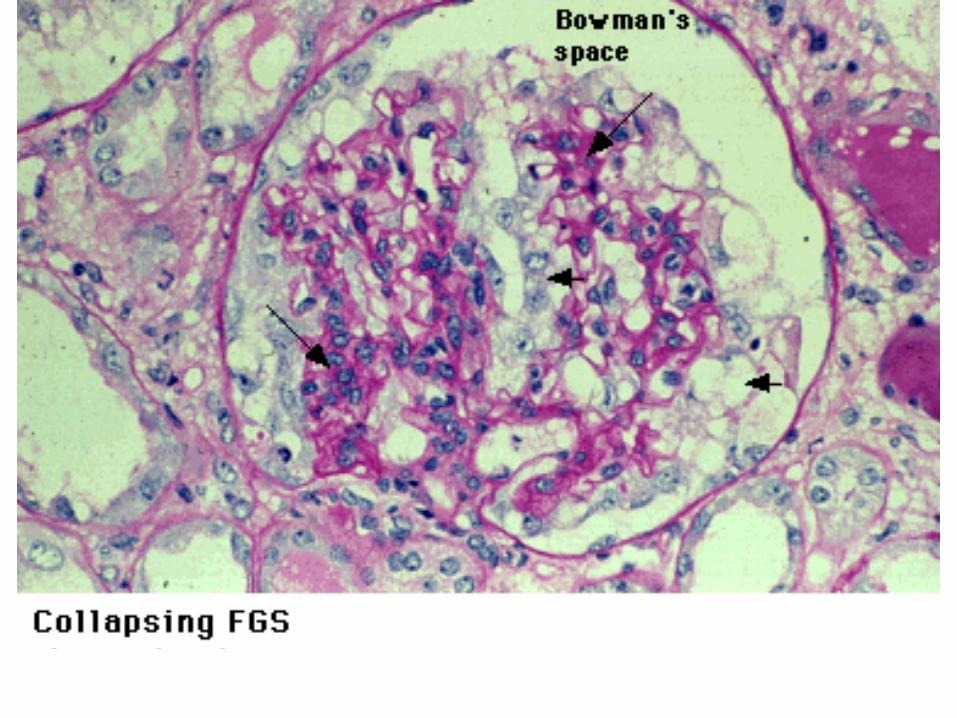
Focal segmental glomerulosclerosis (FSGS)
• Idiopathic nephrotic sy.
•Secondary
•HIV
• Heroin
• decreased nephrone number
• Obstructive uropathy, vesicoureteral reflux
• Obesitas
• ageing

Treatment of idiopathic nephrotic sy. (MCD, FSGS)
Induction
Prednisolon 1 mg/kg 8-12-(16) weeks, tapering
If steroid dependence (recurrence upon decreasing dose), frequent
relapse or resistance
•Cyclophosphamide 1,5-2 mg/kg 8-12 weeks
•Chlorambucil 0,1-0,2 mg/kg
Alternatives
•Cyclosporin-A 4-5 mg/kg + prednisolon
•Plasmapheresis: in resistant FSGS (if perm. factor +)
Newer alternatives
•FK 506 (Prograf) 2x5 mg
•Mycophenolate mofetil (CellCept) 2 x 0,75-1 g
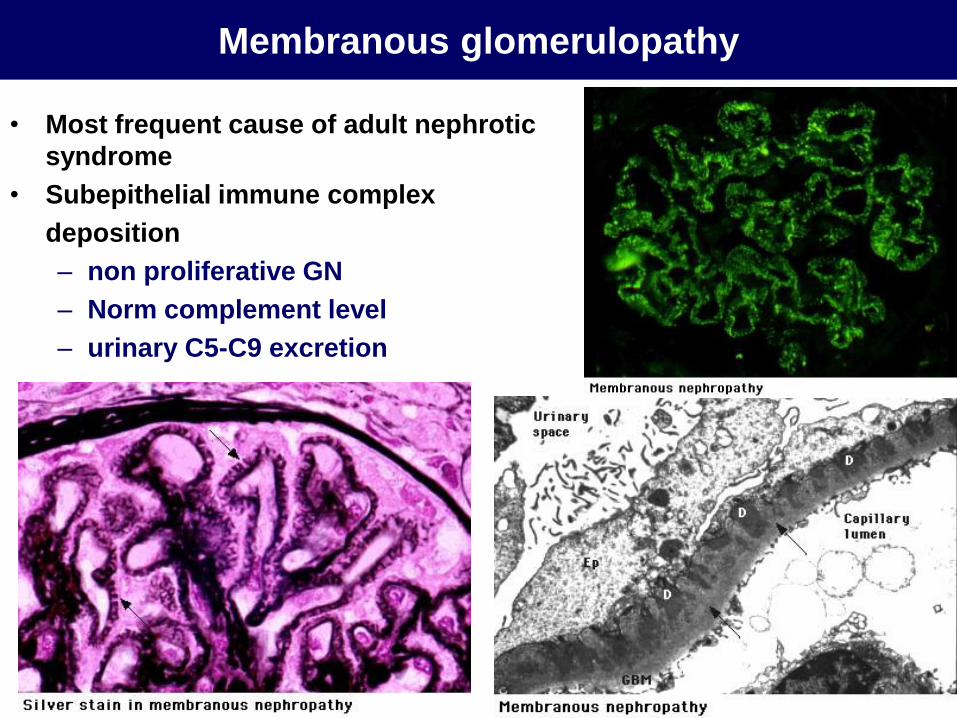
Membranous glomerulopathy
• Most frequent cause of adult nephrotic
syndrome
• Subepithelial immune complex
deposition
– non proliferative GN
– Norm complement level
– urinary C5-C9 excretion

Membranous nephropathia
• Idiopathic (most frequent): anti-phospholipaseA2
antibodies
•Neoplasms (solid tumors):
•lung, gastrointestinal, breast, NHL, CLL, melanoma,
hypernephroma
•Infections:
•HBV, HCV, TBC, abscess, syphilis, malaria, scabies
•Autoimmune diseases:
•SLE (type V)
• Drugs:
•NSAID, penicillamine, gold, captopril

Primary membranosus glomerulopathy
• Animal model: Heymann nephritis
– Antibody against a protein in the podocyte – anti-megalin
• Pathomechanism in humans
– Antibody against a protein in the podocyte: (anti-) phospholipase
A2 receptor

Clinical course of MN
Spontaneous remission: 20%
Spontaneous partial remission: 25-40%
End stage renal disease: 5y: 14%
10y: 35%
15 y: 41%
Poor prognostic factors: tubulointerstitial damage
increased creatinine
heavy proteinuria
glomerular sclerosis
older age
Prognostic markes: high urinary C5b-9, IgG

Immunosupression in membranous nephropathy
Proteinuria 3,5 g/die: no immunosupression, but diuretics,
ACEI, ARB, if needed anticoagulation
Proteinuria 3,5 g/d, asymptomatic: 6-12 mo conservative
Rx, risk assessment based on proteiuria - creatinine change
High risk:
Increased creatinine
Severe nephrosis ( 10 g/die)
Thromboembolic complication
Immunosuppression

Postinfectious glomerulonephritis
• Following Streptococcus,
Klebsiella,Coxakie, Plasmodium,
Aspergillus infection
• Deposition if circulating immune
complexes
• Exudative inflammation (endocapillary
proliferation)
• Complement (alternatív) activation

Membranoproliferative glomerulonephritis
• Type I.
– Mesangial and subendothelial deposition of circulating
immune complexes with proliferative inflammation, GBM
doubling
– Complement activation (klasszikus)
– Secundary forms
• SLE, cryoglobulinemia, chronic HCV infection, abscesses,
endocarditis, paraprotein deposition (MM Waldenström)
• Type II. („dens deposit disease”)
– Continous alternative complement activation due to a
activating antybody against C3 convertase (C3 nephritgen
factor faktor) or other mechanisms (C4 is norm)
– Partial lypodystrophy

Membranoproliferativ glomerulonephritis

Membranoproliferative glomerulonephritis

Cryoglobulinemia
• Palpable purpura, myalgia, arthralgia (Meltzer triad)
– Livedo reticularis, neuropathia
– Hypocomplementemia
• Renal disease usually with type II. cryoglobulinemia
(seen in chronic HCV infection or CLL)
– Membranoproliferative GN
– hyalin thrombus
– „fingerprint” pattern in the deposits

Cryoglobulinemia

IgA nephropathy
• Most frequent primary GN
• On microscopy mezangiál proliferative GN with predominant IgA deposition
• Clinical presentation is usually isolated hematuria
• As part of systemic disease: Henoch-Schönlein purpura
• increased IgA level
• Measangial IgA deposition
• Increased galactose-sialic acid content in the hinge region if IgA
– ↓clearance

IgA nephropathy

IgA nephropathy
• Idiopathic: Berger disease (IgA nephropathy)
Henoch Schönlein purpura
• Alkoholic liver disease
• Celiac disease
• IBD: Crohn, Colitis ulcerosa
• Dermatitis herpetiformis
• Mycosis fungoides
• M. Bechterew

IgA clinical course
ESRD: 5 y: 10%
10 y: 15%
15 y: 25%
20 y: 33%
Poor prognostic factors: Glomerular sclerosis
Intersitialis fibrosis
crescent formation
> 3,5 g/d proteinuria
increased creatinin
Hypertonsion
Kor
ACE gene DD allele

Therapy of IgA nephropathy
Proteinuria < 1 g /d, no major structural damage:
BP control, ACEI/ARB
Proteinuria > 1 g /d, no major structural damage:
Prednisolon (18-36 hó)
Fish oil
Tonsillecomia (?)
Increasin creatinine (> 2 ml/min/mo):
Prednisolon: mg/kg 2-3 mo tapered for 1-2 y
Diffuse crescents
Metylprednisolon i.v. po. Prednisolon +
Cyclophosphamide 2,5 mg /kg
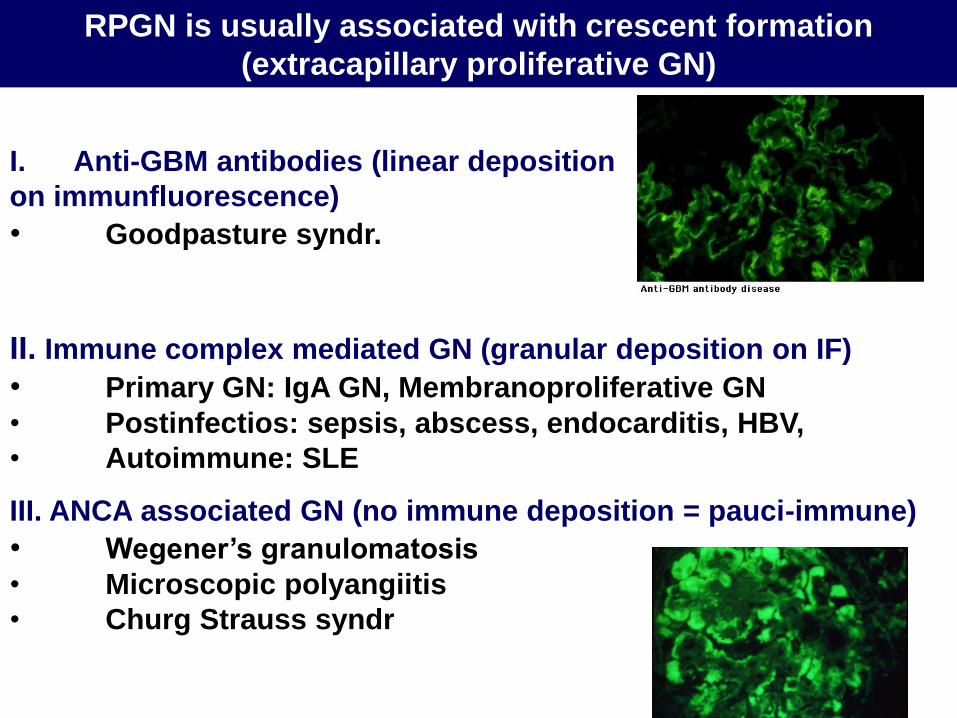
RPGN is usually associated with crescent formation
(extracapillary proliferative GN)
I. Anti-GBM antibodies (linear deposition
on immunfluorescence)
• Goodpasture syndr.
II. Immune complex mediated GN (granular deposition on IF)
• Primary GN: IgA GN, Membranoproliferative GN
• Postinfectios: sepsis, abscess, endocarditis, HBV,
• Autoimmune: SLE
III. ANCA associated GN (no immune deposition = pauci-immune)
• Wegener’s granulomatosis
• Microscopic polyangiitis
• Churg Strauss syndr




Goodpasture’s syndrome
• Rare disease: 1/1million/year
• Pathogenesis
– Antibody formation against the „non-collagenous” region
of alpha 3 chain of type IV collagen found in the
glomerulus and lung. This causes inflammation and
proliferation
– Pulmonary manifestation frequently after infection, or
other pulmonary damage
– In Alport syndrome after transplantation

Goodpasture’s syindrome
• Pulmonary-renal syndrome
– Pulmonary bleeding-RPGN
– anti GBM antitbodies
• Immunofluorescence, ELISA
• Rx
– Cyclophosphamide, steroid,
– Plasma exchange

ANCA positive glomerulonephritis
Wegener’s
granulomatosis
(PAG)
Microscopic
polyangiitis
(MPA)
Churg Strauss
syndrome
ANCA poz. 80-90% 70% 50%
antigen PR3>>MPO MPO>PR3 MPO>PR3
Patology vasculitis
Renal
pathology
Necrotising, crescent formation, „pauci immun” on
immunfluorescence
Upper
airways
Granuloma, necrosis Allergic rhinitis
Lungs Infiltration,
granuloma, bleeding
bleeding Asthma
other Vasculitis
RPGN
Neuropathia
RPGN
Eosinophilia
RPGN
Rx Cyclo, steroid, TMP/SMX, PE

Samll vessel vasculitis
Wegener
uveitis

Wegener’s granulomatosis

SLE

Renal manifestations in SLE
• WHO type I: no renal change
• WHO type II: mesangial proliferative GN
• WHO type III: focal proliferative GN
• WHO type IV: diffuse proliferative GN
• WHO type V: membranous GN
• WHO type VI: chronic renal failure
• Types II-V may be associated with crescent formation and
necrosis indicating poor prognosis and necessitating agressive
immunosuppression
• Non-blomerular manifestation
– Vasculitis
– Intestitial nephritis

Summary
• Non-proliferative (-pathia)
– Minimal change
– FSGS
– Membranous
– Fibrillary
– Diabetic nephropathy
– Amyloidosis
– Alport sy
• Proliferative (-itis)
– Mesangial ~
– Endocapillary ~
(postinfectious)
– Membranoproliferative
– Extracapillary proliferative
(crescents, necrosis)
May be
– Focal/segmental ~
– Diffuse proliferativ (félholdképződés)








