
Otoscope Magazine of AOA Spring 2010
32
-
Upload
kenneth-scribner -
Category
Design
-
view
164 -
download
0
Transcript of Otoscope Magazine of AOA Spring 2010


WHAT’SINSIDEWHAT’SINSIDE
2010 EXPANSION OFLEGAL REQUIREMENTSIN YOUR ORGANIZATIONAND BEYOND 18Jeff Thompson walks you through the changesoccurring in 2010 with leave, discrimination andprivacy laws.
THINKING OFDOWNSIZING? THINKTWICE BEFORE YOUCUT 8You might want to reconsider cutting your nextemployee. Pat Brown-Oliver explains whydownsizing might not be the best answer.
PATHWAY TO NATIONALHEALTHCARE REFORM:AN OVERVIEW OFAAO-HNS EFFORTS 11The AAO-HNS gives an overview of its efforts toassist in the efforts toward health care reformin the United States.
ACCOUNTING 101:HOW TO READ YOURBALANCE SHEET 21Not a CPA? Don’t worry! Jeff Dudley walks youthrough the basics to reading and understandingyour practice’s balance sheet.
IN EVERY ISSUEFrom the Editor’s DeskPresident’s MessageCOPM NewsAOA News
IN EVERY ISSUEFrom the Editor’s DeskPresident’s MessageCOPM NewsAOA News
Tips & Tricks for BetterGoogle Search 10Take These Steps to Survive anInsurance Audit 15It’s a Jungle Out There . . . AreYou Prepared to Survive? 16
Exploring AlignmentStrategies to Protect AgainstReimbursement Uncertainty 26Welcome to Our NewestMembers 28Upcoming AOA Webinars 29Please Come to Boston 30
AOA NEWSINCLUDES:
AOA NEWSINCLUDES:
TOP 10 WAYS TO MANAGEYOUR ACCOUNTSRECEIVABLE 13Looking to improve your collections? CamilleWhite, COPM, offers 10 tips her office hasimplemented that have shown results.
FORECASTING THEUNKNOWN 6Your fellow ENT managers share what they aredoing to prepare for the uncertain changes inhealthcare.
59.3%
40.7%
Subscription INFORMATIONOto’s Scope is available to membersof AOA at no charge. This magazineis published quarterly approximatelyJanuary, April, July, and October.
Please address all communications to the AOA office at:Association of Otolaryngology Administrators1844 Ardmore Blvd. • Pittsburgh, PA 15221
Phone: 412-243-5156 Fax: 412-243-5160Email: [email protected] Website: www.oto-online.org
NOTICE: Articles for Oto’s Scope can be sent via email or mailed to the AOA office. We welcomeyour submissions. If you need more information, please call the AOA office.
Oto’s Scope is available to membersof AOA at no charge. This magazineis published quarterly approximatelyFebruary, May, August, and November.
Please address all communications to the AOA office at:Association of Otolaryngology Administrators1844 Ardmore Blvd. • Pittsburgh, PA 15221Phone: 412-243-5156 Fax: 412-243-5160Email: [email protected] Web site: www.oto-online.org
NOTICE: Articles for Oto’s Scope can be sent via email or mailed to the AOA office. We welcomeyour submissions. If you need more information, please call the AOA office.

FromtheEditor’sDeskEDITORIAL BOARD
EXECUTIVE EDITORRobin L. Wagner, COPMPittsburgh, PA
EDITORIAL BOARDJames Benson, IVMarienette, WIPat Brown-Oliver, COPMOverland Park, KSCheryl Fatzinger, CMA, MBAWinston-Salem, NCAmanda FouchOklahoma City, OKMary Henshaw, MBA, COPM, CMPEOlathe, KSJoAnn LoForti, RN, MSFresno, CAMarkMilinskiNorfolk, VAJeanne Rothamel, RN, CORLN, COPMWaverly, IALaura TroyerAkron, OHCamilleWhite, COPMMacon, GA
EDITORIAL COORDINATORCaitlin Price
CONTRIBUTING WRITERSJeff Dudley, CEO
Reed Tinsley, CPA
CamilleWhite, COPM
James Benson
Jeffery L. Thompson
Keith Rosen
AAO-HNS
Justin Chamblee, MAcc, CPA
John Gross, FHFMA
Mary Henshaw, MBA, COPM, CMPE
Caitlin Price
Robin L. Wagner, COPM
DESIGN / LAYOUTScribner GraphicsRochester, MN
Spring 2010 Vol. 8, Issue 2
processes to make sure you arecurrent; make sure you have the rightstaff for the right jobs; and generallyhave a plan for the future. If you aren’tgreat in finance, Jeff Dudley has agreat two-part article that will help youunderstand all of the numbers on abalance sheet. Your colleagues in AOAhave many best practices and greatthings happening in their practices toshare with you. The power of the AOAnetwork allows you to get answers tothe issues in your practice both via thewebsite discussion boards and justplain old networking.We hope that you will spend some
time learning about the resourcesthat AOA has to offer. If you aren’t amember of AOA, now is the time to join.More than ever, you need resources,education, and networking to help youprepare for the future. The investmentwill pay for itself in terms of thetime saved developing resources,researching best practices and findingconsultants. We encourage you to jointhe AOA today and utilize the network.
Best regards,
Robin L. Wagner, COPMExecutive Editor, Oto’s ScopeExecutive Director, AOA
Dear Colleagues,There are so many uncertainties
going on in health care right now. Wehave a new health care plan, but thejury is still out on just how this newplan will impact how otolaryngologyphysician offices are currentlymanaged. There is still no fix toMedicare’s SGR. Regulation continuesto increase. It is almost a perfectstorm. How do we go about ourbusiness and succeed in the businessof medicine? How do we plan forwhat we don’t know?The AOA is a great resource to help
you navigate today. We have resources,networking and education to help youand your practice succeed. We arediligently working with the Academy tojoin forces to bring even more educationand resources through the Business ofMedicine. We have successfully workedwith the Academy on a number ofinitiatives this year, including: spread-ing the word to AOA members aboutsome of their initiatives; gathering datafrom both groups to present at CMShearings; and continuing to get theword out on specific items that impactotolaryngology. Our newest initiative isa Business of Medicine Program thatwe will present jointly on Saturday,September 25, 2010, in Boston, MA.We have a great list of topics to helpphysicians and administrators engagetogether in moving practices forward.As you read through this edition of
the Oto’s Scope, you will notice thetheme is for otolaryngology practicesto try and figure out what physicianpractices can do while waiting for allof the stars to align. Don’t just sit backand twiddle your thumbs while you waitfor changes in health care to arrive –act now! Through some of the articles,we suggest that you: be proactive;make sure that you are providing thebest service available; evaluate your
In action lies wisdom and confidence.–Albert Schweitzer
The people who get on in this world are the people who get up and look for thecircumstances they want, and, if they can’t find them, make them. –George Bernard Shaw
4 Spring Edition 2010 Oto’s Scope
Robin L. Wagner, COPM

Dear Colleagues,The AOA has had a healthy
relationship working hand-in-hand withthe AAO-HNS for many years. Eachorganization complements the other,assisting in fulfilling the roles of boththe ENT physician and administrator.Members of the AOA and AAO-HNShave benefitted greatly from network-ing, continuing education, practicemanagement information, and legisla-tive advocacy. Together, we help oneanother to run a successful businesswhile at the same time providing a highlevel of patient care. Now, during thistime of health care law and reform,our efforts to work together are morenecessary than ever.The new health care law brings a lot
of uncertainty to us all – as patients,as providers, and as employers. Manypeople are speculating on what ourfuture reimbursement models will looklike. There is speculation that the inte-grated/capitated global reimbursementmodels of the 1990s will be revived.Others are hopeful that SGR (sustain-able growth rate) will be replaced witha reimbursement formula more fittingto today’s physician/patient environ-ment. I believe the majority of us – asmanagers and physicians – have thesame common goal of providing excel-lent health care while maintaining afair and healthy bottom line.Many practices are “tightening their
belts while they ride out the healthcare storm.” However, many others aretaking this opportunity to grow. Manypractices are thinking of growth interms of increased market share andpatient visit volume, while otherpractices are considering growth interms of adding ancillary services,such as allergy, audiology, hearingaids, radiology, videostrobeography,
President’sMessage
Kelly Ladd, COPM, CMPEAOA President
transnasal, esophogoscopy, sensorytesting, and sleep labs. If you couplethis with the added “patient care value,”the end result is one of increasedrevenue enhancement.We have all entered into the
uncharted waters of healthcare reform,but you can be confident that the AOAwill be leading the way in providingpractice management resources tohelp you chart your course. I hope youwill join us in Boston for our AnnualEducational Conference Sept. 22–25,2010. We have an exciting agendafilled with the latest news and infor-mation regarding health care reformalong with incredible networkingopportunities amongst members fromall around the country. Together, we asadministrators and physicians can usethe tools made available through theAOA to grow and overcome health careadversity in these uncertain times.Sincerely,
Kelly V. Ladd, COPM, CMPEAOA President
AOA OFFICERS
PRESIDENTKelly Ladd, COPMNorthwest ENT & Sinus Center780 Canton Road Suite 330Marietta, GA 30060Phone: (770) 427-0368 ext. 202 | Fax: (678) 581-5969E-mail: [email protected]
PRESIDENT ELECTTodd Blum, MBAEar Nose & Throat Association of South Florida900 NW 13th St. Suite 206Boca Raton, FL 33486Phone: (561) 391-3333 | (561) 338-6271E-mail: [email protected]
SECRETARY-TREASURERJeff Dudley, CPASacramento Ear, Nose & Throat1111 Exposition Blvd. Bldg. 700Sacramento, CA 95815Phone: (916) 736-6670 | Fax: (916) 736-9837E-mail: [email protected]
SENIOR EXECUTIVE COMMITTEEMEMBER-AT-LARGE
Cheryl Fatzinger, CMA, MBAPiedmont ENT Association, PA110 Charlois Blvd.Winston-Salem, NC 27103Phone: (336) 714-1039 | (336) 768-4131E-mail: [email protected]
JUNIOR EXECUTIVE COMMITTEEMEMBER-AT-LARGE
MarkMilinskiEar, Nose & Throat, LTD901 Hampton RoadNorfolk, VA 23507Phone: (757) 623-0526 | (757) 623-0609E-mail: [email protected]
IMMEDIATE PAST PRESIDENTKaren Boyd, CMM, COPMAshland ENT, Allergy & Hearing Aid Center2212Mifflin Ave. Suite 130Ashland, OH 44805Phone: (419) 289-8919 | (419) 289-9563E-mail: [email protected]
PARLIAMENTARIANJoAnn LoForti, RN, MSCentral CA ENT1351 E. Spruce St.Fresno, CA 93720Phone: (559) 432-3724 ext. 228 | Fax: (559) 432-8579E-mail: [email protected]
CONTACT INFORMATIONAssociation ofOtolaryngologyAdministrators1844 Ardmore Blvd.Pittsburgh, PA 15221Phone: (412) 243-5156 | Fax: (412) 243-5160E-mail: [email protected]
Spring 2010 Vol. 8, Issue 2
Change is the only constant; hanging on is the only sin. –Denise McCluggage
Oto’s Scope Spring Edition 2010 5

6 Spring Edition 2010 Oto’s Scope
perhaps be better to tell you whatYOUR colleagues are doing to preparefor these vague uncertainties, andshare the changes that they see comingin the next 12 months and how theyare planning for the future. After all,that is the power of the AOA network.Businesses forecast frequently.
Using complex business and mathe-matical models, they can extrapolateinto the future and predict what is goingto happen. We agree that using thesemodels helps the past predict the future;however, because health care is under-going many changes, we thought itwould be best to find out what peoplein the typical otolaryngology practiceare doing to stay ahead in theseuncertain times.
The Present
The future might seem rather cloudy,but many administrators are beingproactive and taking action right now.According to a survey conducted bythe AOA in the spring of 2010, most
Changes are occurring at a rapidrate in the otolaryngology prac-tice. Regulatory changes, health
care reform, and economic conditionsall play vital roles in the climate of ENTpractices. So what are the leaders ofthese practices to do? Should we allgo get out our magic ball, seek out afortune teller, or maybe hit the casinoto gamble on the future? Or should wehunker down to prepare for the storm?Those are all scenarios that feel a littlelike the otolaryngology practice intoday’s world. Well, we thought it might
FE
AT
UR
EA
RT
IC
LE
READER R I• AOA survey shows whatadministrators are doing nowto prepare for the unknown.
• Popular trends include:implementing EMRs, addingancillary services, and utilizingtechnology for efficiency.
respondents are preparing for thefuture by looking to cut costs in allareas of practice management. Whilemany are tightening their belts —through attrition and not expandingservices or personnel — others arelooking at ways to decrease overheadstrategically without compromisingquality or patient service. Examplesincluded merging satellite offices,renegotiating contracts and leases,and tightening down efficiency andprocesses. Some practices havecreated walk-in clinics for patientswith poor reimbursing insurance whileothers are focusing on accountsreceivable retraining to make sureeveryone understands their role inA/R collections.Although administrators and prac-
tices are evaluating processes tooperate more efficiently, practicesas a whole are also seeing an overalldecrease in revenue. Nearly 56% of
ForecastingtheUnknown:HowENTAdministratorsarePreparingforChangesinHealthCareBy Robin L. Wagner, COPM, and Caitlin Price
05
1015202530354045
Postponing anyexpansion of services,
physicians, etc
Postponingcapital
expenditures
Frozen hiringfor now
Not replace positions when employees
were lost
Decreasingoperating
budget
Downsized practice
Other (please specify)
Have you done or are you doing any of the following in 2010 for your practice? Please check all that apply.
%o
fR
esp
on
den
ts
continued on page 7

Oto’s Scope Spring Edition 2010 7
cycle and staff retraining).
� Opening communication withhospitals, other ENT offices, andmulti-specialty clinics to exploreopportunities.
� Increasing patient education andmarketing to educate patients onancillary services.
� Evaluating patient access andpatient scheduling for efficiency.
� Keeping an eye on having the rightemployees in the practice andallowing them to participate inimproving efficiency.
� Physician and physician extenderrecruitment to assist with ancilla-ries and patient volumes and access.
� Working with the physicians on aplan for the future.While some practices are choosing
to “wait out the storm,” dozens ofpractice administrators are preparingfor the future. But the administratorshouldn’t be the only one focused onthe uncertainties: Everyone in thepractice — from the person schedulingthe appointment and to the medicalassistant to the administrator and tothe physician — must be on his or hertoes and think about how to do thingsdifferently. Have your staff begin askingthemselves questions as they are goingthrough their day. Some simple ques-tions to consider are: Is this processrepetitive? Is there a better way to dothis? Can we automate this process?Ask each staff person to take a closelook at his or her own position, atwhat they do every day. You might besurprised at the cost-cutting ideasthat come from “the trenches.”
respondents noted a decrease in reve-nue in the last year. Many commentedthat they are flat in revenue growth orit has slowed. Respondents stated thattheir practices are also experiencingmore uninsured patients this year:52.4% reported an increase in unin-sured patients and an increase inMedicaid in the last year. This meansmore work and less revenue for seeingthe same number of patients in manyoffices. Administrators are also report-ing a higher no-show rate, especiallythose with high deductibles insuranceplans, making the deduction thatpeople are thinking twice before goingto a doctor.In spite of what might seem dismal
by the numbers above, many practicesare managing to find areas to grow.Approximately 41% of respondentsreported opportunity for growth in theeconomic downturn. How are they doingthis? By adding ancillary services! Ofthe respondents, 36% are adding orexpanding their hearing aid service,while another 54% stated that theyare expanding one or a combinationof hearing aid sales, allergy, cosmeticlines, CT scanners, and sleep labsinto their practices. These ancillaryservices are also necessitating theneed to add additional physicians andphysician extenders in a third of thoseseeing opportunities for growth.
The Future
Practice administrators will be facedwith many harrowing challenges in thenext few years. We wanted to know thethinking behind their planning. There-fore, we asked how administratorsthink practice management will havechanged by 2012. While there were
no mathematical models employed orfortune tellers in the group, the themewas common: Everyone predicted thatbusiness efficiency must get better,technology must be used to leverageefficiency, and everyone must managethe accounts receivable and bottomlines carefully. Are we all worried? Ofcourse! Should practices merge with ahospital, MSO, or another practice?Can they survive as a small practice?The jury is still out!Most administrators stated that they
will want to keep their eye on trendsand keep discussions open with theirphysicians. However, until health careis sorted out, most administrators aregoing to focus on evaluating the entirepractice in regards to processes,technology and potential areas forgrowth that can help efficiency andthe bottom line.
Prepare Now for the Future
When asked what practices are doingto prepare for the future, the majorityof practice administrators are workinghard to be proactive and are concen-trating on many different opportunitieswithin their practice to navigate thestorm effectively, including:
� Implementing technologies such asElectronic Medical Record.
� Implementing a website thatcontains patient materials andelectronic means to communicatewith patients efficiently.
� Renegotiating insurance contracts.
� Evaluating efficiency in the accountsreceivable and billing cycles (somethrough technology, I.E. practicemanagement systems; and somethrough evaluation of the billing
FFoorreeccaassttiinngg tthhee UUnnkknnoowwnn continued from page 6
FE
AT
UR
E A
RT
IC
LE
59.3%
40.7%
In the economic downturn, have you seen the opportunity for growth?
continued on page 8
44.4%55.6%
Are you seeing a decrease in revenue?
Yes

8 Spring Edition 2010 Oto’s Scope
One administrator gave this advice:“Focus on ‘lean.’ Focus on identifyingproblems, using a methodical approachto improve the process and use all stafffor this technique. Everyone, physi -cians especially, need to be involvedand participating.”Not knowing what’s in store for
the otolaryngology practice can be
frustrating and worrisome. Althoughwe cannot predict exactly what thefuture will bring in healthcare, devel op -ing a plan and getting everyone in yourpractice on board will only enhanceyour practice operations and bring yourteam together to work through this.
FFoorreeccaassttiinngg tthhee UUnnkknnoowwnn continued from page 7
HU
MA
N R
ES
OU
RC
ES
managers, say, “Surely we have toomany employees,” or how about, “the employees are paid too much.”Here is where pencils start to get
sharpened, and this line item of over -head can be reduced! As practices beginto look at each category of employees,another common thought is, “Aren’tthere too many people in the billingdepartment? These folks do not havedirect patient contact, so maybe, justmaybe, we can make some cuts here.”Or how about in our reception area –We sometimes hear ideas such as, “Do we really need four receptionistsat check-in and check-out when weonly see 80 patients a day?” (Or how -ever many you might have.) And thenthere is the phone area – surely thephones don’t ring that much. Can’t we do this with at least two feweremployees in that position? Practicestend to lose those employees that have direct patient care, but does thismake sense? Practices tend to feelmore comfortable about eliminatingpositions such as schedulers, insur -
ance pre-certification clerks, or eventhe audiology assistant.If any of these scenarios sound
familiar — or you have had the samethoughts yourself — then perhaps it is time to take a look at the pros andcons of decreasing staff. Does cuttingstaff make sense, particularly those inareas without direct patient care? Willreducing in these areas benefit yourpractice in the long run? I don’t knowabout your practice in particular, buttypically, physician offices tend to runlean and hire employees who can andwill do multiple job functions. The costsof “downsizing” might be more than theemployee payroll you are saving. Sure,with downsizing, you might save thosebenefits such as health insurance, 401Kmatch, and PTO. But then you need tofactor in an increase in overtime,decreased morale, and probably themost important, risking patient satis -faction, both in the quality of care they
READER R I• Decreased morale could havenegative effect even if you’resaving money
• Look for strong employees totake on several jobs
This article is not going to talkabout surgery, but rather how to“prep” your practice for financial
stability today and tomorrow. So, wheredo we begin? Well, the first instinct isto look at the large ticket items on yourexpense sheet and immediately say,“we need to cut the bottom line by 5%,10% or 15%.” Your fixed items arepretty hard to cut: For example, rentcan’t be cut for many of us unless yourlease is about to expire, or if you havean opportunity to start negotiations onthis for one reason or another. So thenext large ticket item on the expensesheet, which is always so tempting togo after, is employee expense! Often we hear physicians, and sometimes
continued on page 9
Thinking of Downsizing?Think Twice Before You CutBy Pat Brown-Oliver, COPM

Oto’s Scope Spring Edition 2010 9
TThhiinnkkiinngg ooff DDoowwnnssiizziinngg?? TThhiinnkk TTwwiiccee BBeeffoorree YYoouu CCuutt continued from page 8
receive and overall satisfaction withyour practice. For example, downsizingin the billing department can result ina reduction in your cash flow fromprocedures not getting precertified,lack of claims follow-up, and delays inservices being billed. Remember, whentwo people take on the job of three,something is going by the wayside.Cutting out one front desk person canresult in delays in the waiting room andunhappy patients and physicians. Youwant your front desk personnel, whoare our first impressions, to appearcalm, efficient, and, most of all, happyto be here. That impression is the mostcost-effective advertising we can have.We want our phone personnel to givethat same impression over the phonelines: that we are happy to assist themin any way we can. Short tempered,over-worked employees do not projectthe image we want.
So then, if cutting back on staff isn’t the answer, what is? Although it’salways been a good idea to take a look at each employee’s performance,perhaps it’s important now more thanever. Specifically, are there one or twoemployees who just haven’t performedlike the rest of the team? Would theirabsence be less noticeable and couldyou “easily” incorporate their functioninto one of those other stellar employ -ees? You might want to talk to themindependently to give them a heads up.Make sure all of the employees
know and understand that healthcareis going to change. You need them toget on board and go that extra step,taking on a little more and getting it all done. Now it is time to recognizethose employees who can multi-taskand perhaps let them know that thereis an opportunity for them to excel andthat you do appreciate their effort.
Cutting salaries and stopping raisesor bonuses are steps to be taken whenthe time is right, and it makes goodbusiness sense. But I caution you toturn to this as a last resort. Losingyour employees who have helped togrow your practice or causing moraleto plummet can be far more detri -mental than that one employee’s salaryyou are looking to save.
Pat Brown-Oliver, COPM, is theManager of Business Services at Headand Neck Surgical Associates, Inc., in Overland Park, KS. She is also theChair of the COPM Advisory Board and Education for AOA.
HU
MA
N R
ES
OU
RC
ES
10 Spring Edition 2010 Oto’s Scope
Perform Calculations – Tofigure out what 6.764 percent tax
on a $65 product, enter “$65 x6.764%” and the answer will show inthe display box.
Convert measurements – Howmany ounces in a gallon? Enter
“ounces in gallon.”
Currency conversions – Curiouswhat your money will get you in
another country? Use Google to convertcurrency! Enter “120 dollars in Euros”to see how far your dollar gets you inEurope.
Track flights – Track your flightfor timeliness by entering your
airline and flight numbers.
Time Zone Differences –Challenged by world time? Enter
“time” and then the name of the city.
Locatepackages –
Track deliveries byentering “track” plusthe tracking numberfor direct link to thestatus page.
Look upaddresses for free –
Type in the person’s home phonenumber. If he or she is listed in thewhite pages, Google will display themailing address. There is also a spoton the home page to delete yourinformation is you don’t want itdisplayed.
Area code lookup – Everyonegets a call from an area code they
don’t recognize. Enter the area code,and Google will let you know where itis and show you a map of the area.
Find specific types ofdocuments — Search for PDFs,
Excel spreadsheets and PowerPointpresentations. Use filetype:pdf,filetype:xls, or filetype:ppt to find filesin those specific formats. Example: HRmanual filetype:PDF
Find a verbatim phare – Usequote marks (“ ”) around the
phrase you wish to search. Example:“EHR incentives”
Find narrowed-downinformatrion – Type a minussign (-) before words you wish
to exclude from your search. Googlewill eliminate any entries that containwords preceded by the minus sign.Example: coding -game –computer
Spelling Aid – Enter a wordinto Google to check your
spelling. Enter “HIPPA” and it willsuggest “HIPAA”.
Are you always looking for a way to make your job easier? Do you love learning about newtips and shortcuts to make managing more efficient? Believe it or not, Google can help!There are lots of little tricks to get the most out of your day on the computer, whether for work or for play. Google can be used for a variety of small tasks – not just to search!Below are several ways that you can make the most of Google.
Tips & Tricks for Better Google Search
TE
CH
NO
LO
GY
LE
GIS
LA
TIO
N
a platform to work strategically from toachieve healthcare reform legislationthat would strengthen access to, andthe delivery of, quality healthcare forthe nation, while still preserving thepatient-physician relationship. The coalition, consisting of approxi -
mately 20 medical specialty groups andrepresenting more than 240,000 sur -geons and anesthesi olo gists, submittedmyriad comments and suggestions forimproving healthcare reform proposalsas they emerged from the U.S. Congress.In an effort to better engage andinform AAO-HNS members regardingreform developments, the Academydesigned a new healthcare re form web page to outline and house all the
Aca demy’s efforts and position state ments.The webpage, www.entnet.org/hcr, also includes links to the Academy’slegislative alerts.
Activities in the U.S. House of Representatives
The first healthcare reform bill,“America’s Affordable Health ChoicesAct,” was introduced July 14, 2009.Based on the vast scope of thehealthcare reform proposals, multiplecommittees in the U.S. House ofRepresentatives retained jurisdictionover various portions of the bill. As aresult, three committees — Energy andCommerce, Ways and Means, and Edu -cation and Labor — each held hearingsand mark-up sessions to discuss theimpact and constructs associated withthe legislation. By the end of July, eachcommittee had voted in favor of the billand reported it from committee. OnJuly 22, 2009, the AAO-HNS delivereda letter to the Tri-Committee Chairmenoutlining serious concerns with H.R.3200 regarding its potential impact onthe physician-patient relationship. Inaddition, the AAO-HNS recognizedphysician-friendly provisions in the bill, such as language to permanentlyreplace the flawed Sustainable GrowthRate (SGR) formula, the absence of“budget neutrality” across the physi -cian spectrum, and resisting thepressure to create an IndependentMedicare Advisory Commission withinthe Executive Branch.
continued on page 12
Throughout 2009, the AAO-HNS anda surgical coalition workedcollaboratively to develop joint
principles for healthcare reform. Thesejoint principles provided the group with
READER R I• AAO-HNS and surgical coalitionworked to develop jointprinciples for reform
• Overview of activities in theU.S. House of Representativesand U.S. Senate since 2009
• AAO-HNS efforts continue atwww.entnet.org/hcr
Pathway to National HealthcareReform: An Overview of AAO-HNS Efforts
Oto’s Scope Spring Edition 2010 11

Following the initial debate on H.R. 3200, House leadership worked to combine the three committee-passedversions of the bill. The final Househealthcare reform package, H.R. 3962,the “Affordable Healthcare for AmericaAct,” was introduced on Oct. 29, 2009.Following a period of lively floor debateon Nov. 7, 2009, the House passed H.R.3962 by a vote of 220 yeas – 215 nays.The vote was largely on a party-linebasis; 39 Democrats voted against thebill and only 1 Republican voted infavor. Throughout the debate, abortionfunding and immigration languageemerged as two of the most conten -tious issues. Although Democratleaders viewed the affirmative vote asa major victory, many of the provisionsin H.R. 3962 were considered “dead on arrival” in the U.S. Senate.In an effort to reduce the overall
cost of healthcare reform legislation,House leaders stripped the Medicarephysician payment provisions from H.R. 3962 and introduced the languagein a stand-alone bill, H.R. 3961. The“Medicare Physician Payment ReformAct of 2009” incorporated the samelanguage originally included in thehealthcare reform legislation and waspassed in the House on Nov. 19, 2009,by a vote of 243 yeas – 183 nays. TheAAO-HNS strongly supported thepassage of H.R. 3961.
Activities in the U.S. Senate
Although the U.S. House of Repre -sentatives passed its healthcare reformpackage, the latter part of 2009 wasspent in a “wait and see” game regard -ing reform activities in the U.S. Senate.The slim Democrat majority in theSenate left little margin for error interms of developing legislation thatcould garner the 60 votes required fornumerous procedural hurdles.The Senate Finance Committee
and the Health, Education, Labor andPensions (HELP) Committee holdjurisdiction over healthcare reformefforts in the chamber. Both commit -tees introduced and passed separatehealthcare reform bills that were latermerged to create the Senate’s compre -hensive reform package. The “PatientProtection and Affordable Care Act”
PPaatthhwwaayy ttoo NNaattiioonnaall HHeeaalltthhccaarree RReeffoorrmm:: AAnn OOvveerrvviieeww ooff AAAAOO--HHNNSS EEffffoorrttss continued from page 11
LE
GIS
LA
TIO
N
(H.R. 3590) was introduced on Nov. 18, 2009, and debate promptlybegan the following week. The AAO-HNSand the surgical coalition attempted for many months to influence thedevelopment positively of the Senatehealth care reform proposals. Unfortu -nately, many of the most troublingreform provisions were included in thebroad reform package. In particular,the troubling provisions in H.R. 3590included:
� The creation of an IndependentMedicare Advisory Board chargedwith the development and imple -mentation of binding Medicarepayment policies withoutCongressional oversight or judicialreview;
� Mandatory Physician QualityReporting Initiative (PQRI) withpunitive penalties for non-partici -pation and no clearly definedfeedback program;
� “Budget-neutral” bonuses for pri -mary care and general surgery atthe expense of other physicians; and
� The inclusion of a 5 percent excisetax on elective cosmetic procedures,thus burdening physicians with taxcollection requirements and invitingthe Internal Revenue Service intothe examination room.
Based on the aforementionedprovisions and many others, the AAO-HNS and the surgical coalitionopposed H.R. 3590. Although the AAO-HNS and the coalition recognized andsupported the need for substantivehealthcare reform, it was imperativethat government officials focus on the“right” reforms. AAO-HNS leadershipfirmly believed that reform effortsshould not insert federal bureaucratsinto private relationships betweenphysicians and their patients, orinadvertently hinder access to qualityhealthcare in this nation.As the end of 2009 approached,
Senate leaders continued to worktowards final passage of H.R. 3590.The constructs of a public option (in any form), language relating to the funding of abortions, and thepossibility of a Medicare “buy in” werethe major issues that emerged in thefinal weeks of the legislative session,jeopardizing the likelihood of theSenate passing a comprehensive billversus a pared-down version. Senateleaders ultimately held the chamber insession to pass a healthcare reformpackage before the end of the year. A“Manager’s Amendment” to H.R. 3590 eliminated the budget-neutral bonusesto primary care and the 5 percent taxon elective cosmetic procedures,
continued on page 14
12 Spring Edition 2010 Oto’s Scope

FIN
AN
CIA
L
Invest in a strong practicemanage ment system with com -prehensive reporting capabilities.
Load all of your payer feeschedules into the practicemanagement system. Your systemshould allow for multiple years to beloaded. If you do not have all of yourfee schedules and payment guide-lines — including multiple surgeryrules — get them.
Pre-register patients when theappointment is made in order to obtain and verify insuranceinformation and referral authori -zations prior to the visit. Issuesrelated to eligibility and referralsare easier to handle in advancerather than waiting until the patientis there and the physician is waiting.
In addition to pre-certification,verify surgical and diagnosticbenefits as well as deductible andcoinsurance information. Use thisinformation to calculate what the
patient’s responsibility is expectedto be (based on your payer contract)and require this to be paid in fullbefore the procedure or test is performed. We do this in ouroffice for all surgeries, in officeprocedures, CT Scans, ENGs andAllergy Testing.
Post office visit charges daily— and surgery and hospital charges at least weekly — comparing thephysician’s schedule to submitted op notes and charges to ensure the capture of all charges.
Set up and use Electronic Remit -tance Advice (ERA) and Elec-tronic Funds Transfer (EFT) for all payers that offer it. Carefully setup ERA to avoid any unintentionalwrite offs.
Create specific edits in yourpractice management system sothat users are warned or stoppedbefore claims are created if an errorexists. (This is in addition to whatyour clearing house will do forgeneral payer requirements.)
� CPT/ICD-9 edits such as modifier-50 are not allowed with CPT69210, or for 69210 only ICD-9380.4 is valid. When valid denialsor bundling occur, ask yourself,“Can I create a claim edit for this?”
� Service Location/ProviderSpecific Edits — Edits for servicelocation billing policies, for asTax ID differences, or for account -ing for physician revenue. Forexample, in our office, CT chargesand revenue are shared equallyamong all physicians, and we bill
continued on page 14
Over the past few years, our officehas seen a steady improvement inour key A/R statistics, from our
collection percentages to our days inA/R. During that time, we haveidentified some specific activities wedo that helped to drive theseimprovements. These of course are inaddition to the usual recommendations,such as collect co-pays and previousbalances at check in, regularly workA/R reports, and denied or incorrectlypaid EOBs, etc. Here are the top 10ways my office found that can improveaccounts receivable and improveoverall collections performance.
READER R I• 10 ways to improve A/R andoverall collections performance
• Effective processes – and theright people – make thedifference
Oto’s Scope Spring Edition 2010 13
Top 10 Ways to Manage Your Accounts ReceivableBy Camille White, COPM
1
2
3
4
5
6
7
Managing Staff Effectively
� Hire the right staff — be willingto make a change when yourecognize when you do not havethe right staff. Sometimessomeone who is great in the frontoffice is not going to be good atinsurance collections. Try tomatch a person’s strengths withthe job description.
� Aggressive, knowledgeable,organized, detailed insurancecollection reps can do wondersfor your A/R. Identify those onyour staff and do your best tomotivate and reward them to staywith you.
� Provide feedback and regularlymeet to review performance, as a group and individually. OurBusiness Office Manager meetsmonthly with each insurancecollections rep to go over theirindividual reports, review trends,and discuss any particular payeror patient issue. This keeps the
manager in tune with what isgoing on and holds the repaccountable.
� Assist staff in developing ways tomanage their tasks effectively. Inthe business office, no one is everreally finished at the end of theday. Your staff needs to know howto prioritize, schedule and stay on top of the variety of tasks thatthey are responsible for.
By implementing and followingguidelines along with these and similaractivities in our office, our days in A/Rwent from averaging 45 days three tofour years ago (which we thought wassuper), to averaging 36 days now. Effec-tive processes — plus the right people— make all the difference. I am veryproud of our office staff and the workthat they do every day for our practice.
Camille White, COPM, AOA 2009-2010 Web Liaison, is the Practice Administrator at The ENT Center ofCentral GA and Central GA Head &Neck Surgery Center in Macon, GA.
those through a separate servicelocation called ENT AncillaryServices to separately report on those charges.
Daily activities must include:
� Submitting electronic claims aswell as correcting and resubmit -ting any with errors.
� Working all denials to ensure thattime requirements for the payerare met. Make sure everyoneknows what those time limits are,for filing as well as appealing.
Don’t be the bank— try to avoidsetting up patient payment plans.Offer alternative financing through a third party. Yes, there are feesassociated with this (you do nothave to offer all of their plans), butoverall, you will still end up gettingpaid more than you would have ifyou set up a payment plan on yourown. Managing them is costly toyour practice, and a large majorityof your patients will not keep them.
TToopp 1100 WWaayyss ttoo MMaannaaggee YYoouurr AAccccoouunnttss RReecceeiivvaabbllee continued from page 13
14 Spring Edition 2010 Oto’s Scope
PPaatthhwwaayy ttoo NNaattiioonnaall HHeeaalltthhccaarree continued from page 12
among other things. However, sincethe Amendment failed to address theAAO-HNS’ remaining concerns, theAcademy maintained its oppositionto the legislation. The Manager’sAmendment passed on Dec. 24,2009, by a vote of 60-39.
Last Steps
Following final passage of theSenate’s healthcare reform package,there was vast speculation regarding
Congress’ next steps. Since theHouse and Senate passed drasticallydifferent bills, many believed thatthe two chambers would not be ableto coalesce around principles thatwould enable them to complete work on healthcare reform. Also,the Democrats’ early 2010 loss of a 60-seat majority in the Senatefurther complicated efforts. It became apparent that in order
to advance a bill to the President,the House would have to pass theSenate’s healthcare reform bill (H.R.3590). As a result, Democratleaders in the House adopted astrategy to pass the Senate billalong with a “corrections” packagedesigned to garner the necessaryvotes to pass the bill in the House.The package was written to adhereto the rules of the “reconciliation”budget process. By utilizingreconciliation, the Senate would beprotected from a Republicanfilibuster and only needed a simple
majority, or 51 votes, to pass thebill. The House passed the Senatehealthcare reform bill (219-212)and the reconciliation package (220-211) on March 21, 2010. The Senatepassed the reconciliation package(56-43) on March 25, 2010, and thePresident signed the two bills intolaw on March 23 and March 30,2010, respectively. Although work on healthcare
reform from a legislative perspectivehas ended, the implementationphase will be a lengthy process. TheAAO-HNS’ Government Affairs andHealth Policy teams will continue tocollaborate with the surgicalcoalition, Congress, and thosewithin the Executive Branch toachieve critical corrections to thebill and protect the interests of AAO-HNS members and their patients.For more information, visit the AAO-HNS’ Healthcare Reform Informationwebpage at www.entnet.org/hcr.
FIN
AN
CIA
L
8
10
9
management (E&M) coding complainthistory form to help your providersproperly document and code theservices they render. These forms are available from organizations thatprovide coding seminars and fromcompanies who produce forms formedical offices.
Keep Your Software Up-to-Date
More and more coding andsubmission is done on computer, sohaving software that is current isessential to avoiding and passingaudits. Software that doesn’t allow useof truncated codes and links to CPTand ICD-9 is a most valuable asset.
Perform Your Own Audits...on YourExplanation of Benefits (EOB)
By scrutinizing the rejections youreceive, you can gather valuableinformation that you can use to trainyour staff. Once you know what iscausing your claims to be rejected, youcan take steps and set up safeguards to help avoid making those errors andprevent rejections. All this meanscleaner claims that are less likely to be audited or will pass an audit if one occurs.
Keep Your Medical Records Current
If you can afford to, have aprospective audit done for every claimyou submit. That’s the ideal way toprepare for the possibility of a realaudit, but if you can’t, the next bestthing is to perform random post-claimaudits on a periodic basis. Considerauditing each provider every six to 12 months. Nurses and physicians can audit each others’ records fordocumentation that supports thechosen codes. Errors found on claims
There is no such thing as an audit-proof claim. However, there aresteps you can take to help your
practice avoid audits or pass the onesyou’re subjected to.
Train, Train, Train
Surviving an audit is a little likefinishing a marathon. The bettertrained you are, the more likely you are to finish — even do well. Codingisn’t something that only your codershould know and understand. Practicemembers, including clinical staff andfront desk personnel, should all have a working knowledge of ICD-9, CPT,and HCPCS, as well as carrierregulations. If these staff membersaren’t comfortable with these codingentities, more training is necessary.This can either be obtained fromcoding seminars or from an outsideconsultant who can then be availableto assist when questions arise. Ifmoney is tight, consider having yourbest office coders attend seminars, and then spend some time trainingcoworkers in the fine art of appropriatecoding. It would certainly be a plus forthis person to be a certified coder.
Keep Your Forms Up-to-Date
Encounter forms should be inspectedregularly to be sure they are accurate,useful, and working efficiently for yourpractice. Use the evaluation and
Take These Steps to Survive an Insurance AuditBy Reed Tinsley, CPA
READER R I• 5 steps to avoid or pass audits• Steps can put you in betterposition should you be audited
that have already been submitted must be reported to the carrier forcorrection.Yes, you could do all this and still be
audited. On the other hand, you couldskip all this, be audited, and be in moretrouble than you’ve ever imagined. No,these steps will not audit-proof yourclaims or your records, but adhering tothem can certainly put you in a betterposition should that auditor ever comeknocking on your practice door.
Reed Tinsley, CPA is a Houston-based CPA, Certified Valuation Analyst,and healthcare consultant. He worksclosely with physicians, medicalgroups, and other healthcare entitieswith managed care contracting issues,operational and financial management,strategic planning, and growth strate-gies. His entire practice is concen-trated in the health care industry.Please visit www.rtacpa.com
OP
ER
AT
IO
NS
Oto’s Scope Spring Edition 2010 15

1. In 2009, what % of all medicalclaims were denied on firstsubmission?a) about 5%b) about 10%c) about 14%d) 20% or more
2. What % of the claims denied onfirst submission are notcorrected and successfullyresubmitted?a) less than 5%b) 10% to 15%c) 20% to 30%d) 40% to 50%
3. Assuming an otolaryngologypractice with three (3) FTEphysicians: If 1 out of 4 co-paysare not collected at the time ofservice, how much revenue islost?a) about $50,000 per yearb) about $83,333 per yearc) about $116,667 per yeard) about $150,000 per year
4. Again, assuming an otolaryn -gology practice with three (3)FTE physicians: If just 5% ofpatients who could have beencoded as “new” patients arecoded at the same level ofservice as established patientsinstead, how much revenue islost?a) about $4,500b) about $9,000c) about $13,500d) about $18,000
READER R I• ENT practices could add 6-figures to bottom line
• AOA to introduce A/R Manual atAnnual Educational Conference
5. 205 members of the IllinoisAcademy of Family Physicianscoded six (6) progress notesthat had already been coded by five (5) expert coders. Howmany of the 205 physicianscoded all six (6) progress notescorrectly?a) 1b) 19c) 56d) 92
6. Considering our typical threeFTE physician otolaryngologyprac tice again, based onnational studies, how muchrevenue is lost due to under -coding each year?a) about $82,000b) about $132,000c) about $182,000d) about $232,000
7. Based on benchmarking studies,practices with more staff perFTE MD will...a) have less total medical revenuebecause overhead will behigher.
b) have about the same totalmedical revenue as practiceswith less staff per FTE MD.
c) have more total medical revenueper FTE MD.
continued on page 17
16 Spring Edition 2010 Oto’s Scope
It’s A Jungle Out There...Are You Prepared to Survive?By James T. Fatzinger, MBA
FIN
AN
CIA
L
QUIZ: It’s a Jungle Out There…
Are You Prepared to Survive?
No one needs to tell you how toughit is to keep patients happy,maintain staff benefits, prevent
providers from grumbling aboutshrinking compensation, and — ingeneral — keep the lights on in yourpractices. The lingering effects of therecession, the shifting of health carecosts from employer-paid premiums toemployee out-of-pocket expense,Medicare cuts…the list goes on and on.But what if someone were to tell you
that you’re probably leaving money onthe table? And we’re not talking chumpchange here! Many practices could —and should — be able to add six-figurenumbers to their bottom line…for thework they’re already doing! It’s thetruth!Don’t believe me? Give the quiz, “It’s
a Jungle Out There…Are You Preparedto Survive?” to your most business-savvy physician. Trust me; you’ll gethis/her undivided attention!
Now that you have your physician’sattention, ask him/her to (a) send you to “Leading the Way,” the AOA-28Annual Educational Conference inBoston, September 22-25; and/or, ifyou’re not already a member of AOA,(b) pay for your membership so youcan take advantage of members’reduced registration rates. There youwill not only learn the answers to thequestions on the quiz above — you’ll
8. When compared to benchmarks,how much revenue does theaverage otolaryngology practicelose due to the aging profile ofits A/R?a) about $10,000b) about $30,000c) about $50,000d) about $70,000
9. Based on national studies, whatis a patient account for $250that is 180 days past due worth?a) $180b) $120c) $75d) $0
10. In the 46 months betweenMarch 2005 and January 2009,the number of lives coveredunder high deductible healthplans (also referred to as“consumer-driven” or“consumer-directed” healthplans) increased...a) 67%b) 167%c) 267%d) 677%
learn what you can do to address the revenue opportunities this quizpoints out. Also at “Leading the Way,” the AOA
will unveil a brand-new resource, theAOA Accounts Receivable Manual. Likethe quiz above, this resource will payfor itself many times over. It will bechock full of best-practice information,policy templates, tools to help youmanage your A/R, sample collectionletters, training scripts, and much more.We can all agree “it’s a jungle out
there.” The question is: “Are youprepared to survive?”
James. T. Fatzinger, MBA, is the principal of Effective Solutions, Inc., a practice management consulting firm based in Advance, NC, specializing in developing cost-effective, customized solutions for medical groups. He is on the faculty of Metropolitan State University in Minneapolis and St. Paul, MN, and the author of “Managing a Diverse Workforce,” “Practical Research Methods for Managers,” and “Manage-ment Principles and Practices.” Jimcan be reached at (336) 940-3521 or [email protected].
Oto’s Scope Spring Edition 2010 17
IItt’’ss AA JJuunnggllee OOuutt TThheerree.. ....AArree YYoouu PPrreeppaarreedd ttoo SSuurrvviivvee?? continued from page 16
FIN
AN
CIA
L

laws has been laid by the appointmentof employee-friendly individuals topositions of power at governmentalagencies. An example is the newSecretary of Labor, Hilda L. Solis, who has been already quoted as saying, “As Secretary of Labor, I amcommitted to the vigorous enforcementof our laws and will make use of thefull weight of my authority to find andprosecute violators.” Her appointmentwas soon followed by the hiring of 250new investigators in the Department of Labor’s Wage & Hour Division(WHD) to monitor wage and hourviolations including overtime, minimum
wage and prevailing wage violations.Additionally, Wilma Liebman wasappointed as Chair of the NationalLabor Relations Board (NLRB). In this the age of technology, thesegovernment agencies will be able tomore readily share information acrossdepartmental lines, thereby hittingemployers from all sides. Last, butcertainly not least, with the Senateconfirmation of a new U.S. SupremeCourt Justice, the new administrationhad the opportunity to select thenewest U.S. Supreme Court Justice,Sonia Sotomayor.
continued on page 19 What could possibly top 2009’schanges to the American withDisabilities Act, overhaul of the
Family Medical Leave Act Regulations,mandatory E-verify, and threatenedpro-union legislation? 2010. We expect2010 to be quite an eventful year foremployers with new legislationincluding bills, executive orders, andcourt decisions (from the new SupremeCourt). While it is hard at this point todetermine the complexities of thesepotential laws, the currentadministration has focused heavily onthe increased enforcement of existingemployment laws by governmentagencies and the expansion of lawsalready in place. Put simply, thus far,all that is known is that employers willface a tougher world. The following is a summary of the areas where we believe expansion of lawmaking will occur.The groundwork for implementation
and expansion of new employment
READER R I• 2010 to bring implementationof new employment laws
• Expansion of leave laws,discrimination laws and privacylaws
• Laws include: Family andMedical Leave Act of 1993;Employment Non-Discrimi na tionAct; Paycheck Fairness Act;and more.
18 Spring Edition 2010 Oto’s Scope
HU
MA
N R
ES
OU
RC
ES
2010: Expansion of Legal Requirements in Your Organization and BeyondBy Jeffery L. Thompson
Additionally, many proposed billshave sought to expand the Family andMedical Leave Act of 1993. Proposedexpansion of FMLA protection includes:
� Application to employers with 25employees (currently an employermust have 50 employees to becovered);
� Expanding coverage to grand par -ents, same-sex domestic partnersand even part-time employees;
� Expanding leave for participation in academic activities and medicalappointments (up to 4 hours in a 30 day period) of a son or daughter;
� Adding domestic violence as acovered reason for leave; and
� Creating a paid FMLA system,similar to the state unemploymentsystems providing for up to eightweeks of paid leave.
At this time, we predict that some, if not all, of the above expansions willbe passed in some form over the nextthree years.
Expansion of Discrimination Laws
As America grows more and morediverse, cultural lines begin to beblurred. It is no surprise that Ameri canlaws are evolving to account for thischange. For years now, Congress has
debated legislation, similar to Title VII
of the Civil Rights Act, to prohibitemployment discrimination based on sexual orientation and possiblygender identity. The “EmploymentNon-Discrimination Act” would protectemployees from discrimination basedupon sexual orientation or genderidentity, although it does not requireequal benefits for same sex-couples. A similar bill recently failed to pass the Senate by one vote, and it is antici -pated that this, or a similar bill, will be introduced for vote again in the near future, now that the Democraticmajority has increased, and given the change in the presidency.Additionally, legislation has been
proposed that would strengthen the“punishment” mechanism of Title VII ofthe Civil Rights Act against employers.Currently, Title VII of the Civil RightsAct and the Americans with DisabilitiesAct allow compensatory and punitivedamages based on the size of theemployer, but with caps being from$50,000 to $300,000. Proposed legi -slation, titled “The Equal RemediesAct,” would repeal the caps, makingunlimited compensatory and punitivedamages available for violations ofTitle VII and the ADA, regardless of thenumber of employees in the organiza -tion. This could significantly affectsmall, medium, and large employersalike. In January 2009, the Paycheck
Fairness Act (“PFA”) passed in theHouse of Representatives, simulta -neously with the Lily Ledbetter Law.While the Lily Ledbetter Law (whicheffectively did away with the state oflimitations for discriminatory paydecisions) was passed, the PaycheckFairness Act stalled in the Senate. ThePFA will significantly limit the defensesto Equal Pay Act claims, add non-retali ation provisions, authorizeaddi tional compensatory or punitivedamages and other penalties, make iteasier to bring class action suits, andrequire the Department of Labor todevelop “guidelines” for employers touse in setting compensation.
continued on page 20
On the horizon for private healthcare practices we foresee a significantamount of expansion in three areas –expansion of employee leave laws,expansion of discrimination laws, andexpansion of privacy laws.
Expansion of Leave Laws
The trend of employers allowingemployees flexibility in taking leave inorder to achieve the perfect work/lifebalance is expanding. By way ofExecutive Order, on January 30, 2009,President Obama launched a WorkingFamilies Task Force aimed at raisingthe living standard of middle classworking families. The task force willfocus on policies to benefit the middleclass to create good paying jobs withflexible, safe and fair workplaces. Thisphilosophy can further be seen inproposed bills on Congress. The“Healthy Families Act” would requireemployers with 15 or more employeeswho work more than 30 hours perweek to provide seven paid sick days to employees to care for themselvesand their family’s medical needs. The definition of family is liberal –applying to anyone “whose closeassociation with the employee is theequivalent of a family relationship.”Employees would be able to take thisleave on a pro-rated basis as it isearned upon being hired. The lawwould allow employees to sueemployers for non-compliance.
22001100:: EExxppaannssiioonn ooff LLeeggaall RReeqquuiirreemmeennttss iinn YYoouurr OOrrggaanniizzaattiioonn aanndd BBeeyyoonndd continued from page 18
Oto’s Scope Spring Edition 2010 19
HU
MA
N R
ES
OU
RC
ES

covered breaches; clarification of thenotifi cation requirements, includingwho is required to issue and receivenotifications; and mandates for employeetraining and complaint processes. Pursuant to HITECH and the final
rule, the new regulations were effectiveSept. 23, 2009. While business associ -ates and covered entities must complywith the new breach notifi ca tionrequirements effective Sept. 23, 2009,fines will not be imposed until 180 daysafter publication. Additional regulationsare expected later this year to provideguidance with regard to other HITECHprovisions, which will become effectivein 2010. We certainly expect HIPAA tobe a hot topic in the years to come.As you can see, the projected
path for 2010 leads to expansion of employee-friendly laws. This trendwill challenge human resourceprofessionals, office managers,owners, and administrators to develop
and assure compliance, while at thesame time minimizing the disruption to organizational effectiveness.
Jeff Thompson is a partner with theMacon office of Constangy, Brooks & Smith, LLP. www.constangy.com. Mr. Thompson’s practice focuses onrepresenting management in employ-ment, litigation, labor matters, provid-ing general advice to clients as well astraining clients on preventative meas-ures to avoid litigation. Mr. Thompsonhas represented firm clients in bothState and Federal Court as well as before administrative agencies such as the Equal Employment Opportunity Commission, the Georgia Departmentof Labor and the National Labor Rela-tions Board. He can be reached [email protected]
Expansion of Privacy Laws
With the expansion of the Internetand computer-reliant businesses, it isno surprise that laws protecting privacymust be updated to reflect thesechanges. When President Obamasigned the “American Recovery andReinvestment Act” into law on Feb. 17,2009, it contained a section entitled“Health Information Technology forEconomic and Clinical Health Act”(“HITECH”), which, among other things,made significant changes to the HIPAAprivacy and security rules, particularlyregarding breaches of protected healthinformation (“PHI”). As part of HITECH,the Department of Health and HumanServices was required to issue finalbreach notifi ca tion requirements. OnAug. 24, 2009, the interim final ruleregarding the breach notificationrequirements were published in theFederal Register. Included in the finalrule was a more detailed explanation of
22001100:: EExxppaannssiioonn ooff LLeeggaall RReeqquuiirreemmeennttss iinn YYoouurr OOrrggaanniizzaattiioonn aanndd BBeeyyoonndd continued from page 19
20 Spring Edition 2010 Oto’s Scope
HU
MA
N R
ES
OU
RC
ES
FIN
AN
CIA
L
always balance.So let’s break down the components
and terminology of the formula, andthen we will discuss what to look at onthe balance sheet.First, the Assets consist of current
assets and non-current assets.
Current Assets
By definition, your current assetswill have a “life span” of one year orless. What that means is that anythingclassified as a current asset will or canbe easily converted to cash, liquidatedor depleted in one year or less. Theseassets include cash and cash equiva -lents, accounts receivable, inventoryand prepaid expenses.
• Cash, the king of most of ourpractices, is probably the easiest ofthe assets to understand, but cancreate the most problems for us:Simply, this is the money in yourbank accounts and the petty cashdrawers in your office.
• Cash equivalents are very safe assets that are easily converted intocash and have little or no penalty for doing so. Examples of cashequivalents are: money marketaccounts, certificates of depositmaturing in one year or less, or U.S. treasuries with a one year orless maturity.
• Accounts receivable in a medicalpractice primarily consist of thecharges owed to the practice byinsurance companies, patients orthird-party payers. Most privatepractices are on the cash basis ofreporting for income tax purposes,which means income is recordedwhen cash is received, and expensesare recorded when cash is paid out.
As a result you typically do not seeaccounts receivable on the balancesheets. That does not mean youignore these receivables, as they arethe key to your king (cash).
You can easily add them to yourbalance sheet by recording them netof your adjustments. For example, ifyou have $250,000 in receivables,and your collection rate averages40%, then you would record them at$100,000 ($250,000 * 40%). If youdo this, you will also need to addthis same amount to your retainedearnings (the $100,000 representsearnings yet to be recognized in theincome statement) to balance thebalance sheet. You might have somemiscellaneous receivables recordedfor money advanced to a physicianor an employee, but remember:These obligations should be repaidto the practice within one year to beclassified as a current asset.
• Inventory would represent anygoods that the practice might haveon hand to sell to patients, such ashearing aids or some other durablemedical equipment for sale. This isanother asset that you probably willnot see in most practices.
• Prepaid expenses consist of prac -tice expenses that you have alreadypaid for but do not want to expenseentirely in the month that were paid.Good examples of this are yourgeneral liability insurance, med/malinsurance and property taxes.
Non-Current Assets
Non-current assets are assets thatare not easily turned into cash or
continued on page 22
You don’t need to be a CertifiedPublic Accountant (CPA) or anInvestment Banker to be able to
understand the financial statements ofan ENT practice. Your practice gene -rates them either monthly through itsown accounting software and staff, oryou have them compiled periodically byyour tax CPA. Regardless of how yourstatements are generated, you need toreview them on a monthly basis.Most practices generate financial
statements that include a BalanceSheet and Income Statement. Somewill also create a Statement of CashFlows. A fourth statement that might beused is the Statement of Share holders’Equity. Whether your practice createsjust the first two or all four statements,it is important to understand what youare reading. By doing so, you will beable to uncover problems and correctthem in a timely manner.
Balance Sheet
So what is a balance sheet? Abalance sheet is simply what thepractice owns (assets) and owes(liabilities). The difference between thetwo is your shareholders’ equity. Putinto a simple formula:
Assets = Liabilities + Shareholders’ Equity
This equation solves the simpleprinciple of a balance sheet: It must
READER R I• Learn the basics to readingyour balance sheet
• Definitions of assets, liabilities,shareholder’s equity
• Putting it into practice to readyour balance sheet
Oto’s Scope Spring Edition 2010 21
Accounting 101: How to ReadYour Balance Sheet By Jeff Dudley, CEO
Now that we’ve covered the assetson the balance sheet, let’s look at whatbalances our equation by starting withliabilities. There is a similar themewith liabilities that we saw with assetsin their two main components:obligations payable within a year(current liabilities), and those duebeyond a year (long-term liabilities).
Current Liabilities
• Accounts payable are the mostcommon current liability. Theserepresent the aggregate of all theinvoices for goods and services youhave purchased for the benefit of thepractice.
• Accrued expenses are alsocommon and represent certainexpenses that you want to recognizein the current period, but have notreceived the invoice for. Mostcommon items are things such asaccruals for bonuses, profit sharing,wages, insurance and servicecontracts.
• Line of credit facilities with yourbank are typically on an annual
basis, so any amount owed would bea current liability.
• Current portion of long-term debtwould be that portion of term debtthat will be repaid in the next 12months.
Long-term Liabilities
• Long-term debt is the mostcommon item we see as a long-termliability and would be net of anycurrent portion of long-term debtabove.
• Capital Leases are leases in whichthe leaseholder effectively acquiresownership interest in the assetbeing leased — may also be found in this classification, again net ofany current payments due.
The remaining component of thebalance sheet equation isshareholder’s equity.
Shareholder’s Equity
• Capital stock represents theamount of initial and subsequentinvestments of money into thebusiness by the shareholders.
• Retained earnings are theaccumulation of the practice’s after-tax income or loss since inception.In other words, each year thepractice will recognize eitherincome or a loss. This number isadded to the previous year’saccumulated total. That totalamount represents the “retained”income used for reinvestment in thebusiness.
By definition, the sum of capitalstock and retained earnings is callednet worth and can be calculated bymodifying our balance sheet formula asfollows:
Assets - Liabilities = Shareholders’ Equity(Net Worth)
Using your new-found knowledge
With a better understanding of thekey terminology in the balance sheet,we can turn our attention to looking atan example balance sheet and whatyou can learn from reviewing it:
continued on page 23
are not expected to be turned into cashwithin a year, and/or have a life-spanof more than one year. • Tangible assets, the most commonnon-current asset, are recognized byyou in the form of furniture, officeequipment, computers, buildingsand land. These are often classifiedon the balance sheet as propertyand equipment.
• Investments, such as in a surgerycenter or office buildingpartnership, would also be non-current assets, as these types ofassets are not easily converted tocash within one year.
• Intangible assets are another typeof non-current asset that you mightsee on your balance sheet, mostlikely in the form of goodwill andpossibly a patent or copyright.These assets are not physical innature and are often the result ofacquiring a practice (goodwill) orinvesting in a process that createssomething of value (patents orcopyrights). Both of these are veryuncommon in our arena.
AAccccoouunnttiinngg 110011:: HHooww ttoo RReeaadd YYoouurr BBaallaannccee SShheeeett continued from page 21
22 Spring Edition 2010 Oto’s Scope
FIN
AN
CIA
L
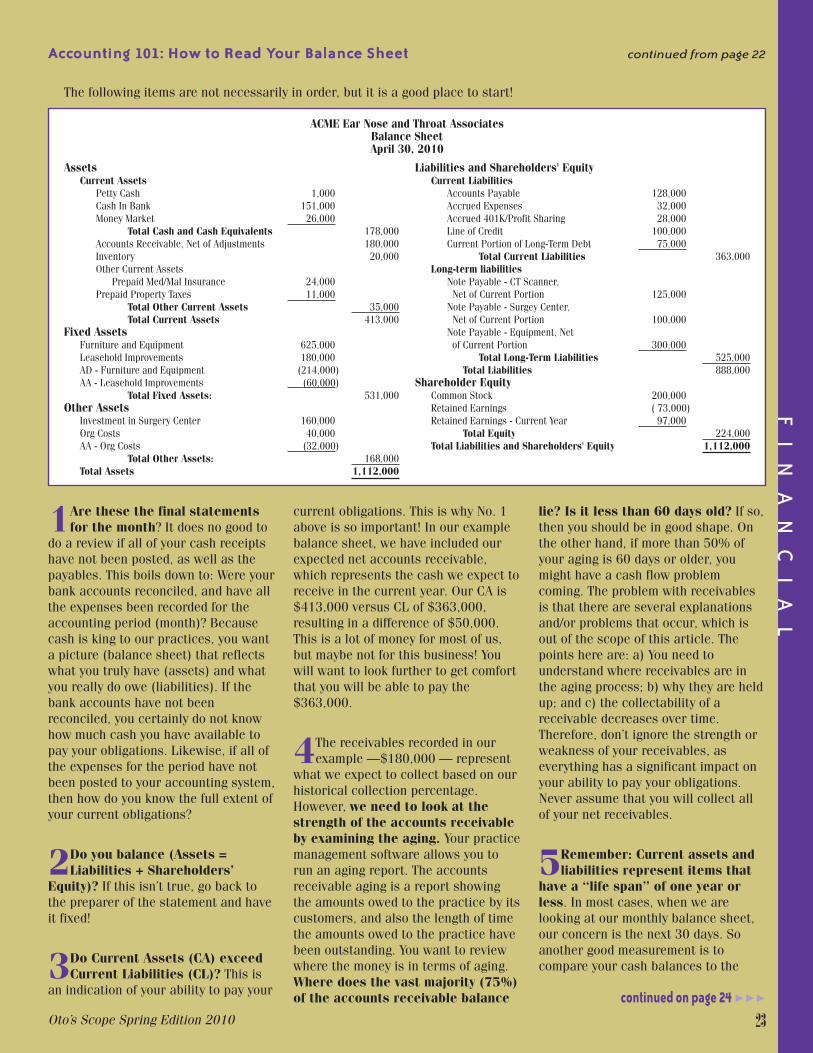
current obligations. This is why No. 1above is so important! In our examplebalance sheet, we have included ourexpected net accounts receivable,which represents the cash we expect toreceive in the current year. Our CA is$413,000 versus CL of $363,000,resulting in a difference of $50,000.This is a lot of money for most of us,but maybe not for this business! Youwill want to look further to get comfortthat you will be able to pay the$363,000.
4The receivables recorded in ourexample —$180,000 — represent
what we expect to collect based on ourhistorical collection percentage.However, we need to look at thestrength of the accounts receivableby examining the aging. Your practicemanagement software allows you torun an aging report. The accountsreceivable aging is a report showingthe amounts owed to the practice by itscustomers, and also the length of timethe amounts owed to the practice havebeen outstanding. You want to reviewwhere the money is in terms of aging.Where does the vast majority (75%)of the accounts receivable balance
lie? Is it less than 60 days old? If so,then you should be in good shape. Onthe other hand, if more than 50% ofyour aging is 60 days or older, youmight have a cash flow problemcoming. The problem with receivablesis that there are several explanationsand/or problems that occur, which isout of the scope of this article. Thepoints here are: a) You need tounderstand where receivables are inthe aging process; b) why they are heldup; and c) the collectability of areceivable decreases over time.Therefore, don’t ignore the strength orweakness of your receivables, aseverything has a significant impact onyour ability to pay your obligations.Never assume that you will collect allof your net receivables.
5Remember: Current assets andliabilities represent items that
have a “life span” of one year orless. In most cases, when we arelooking at our monthly balance sheet,our concern is the next 30 days. Soanother good measurement is tocompare your cash balances to the
continued on page 24
1Are these the final statementsfor the month? It does no good to
do a review if all of your cash receiptshave not been posted, as well as thepayables. This boils down to: Were yourbank accounts reconciled, and have allthe expenses been recorded for theaccounting period (month)? Becausecash is king to our practices, you wanta picture (balance sheet) that reflectswhat you truly have (assets) and whatyou really do owe (liabilities). If thebank accounts have not beenreconciled, you certainly do not knowhow much cash you have available topay your obligations. Likewise, if all ofthe expenses for the period have notbeen posted to your accounting system,then how do you know the full extent ofyour current obligations?
2Do you balance (Assets =Liabilities + Shareholders’
Equity)? If this isn’t true, go back tothe preparer of the statement and haveit fixed!
3Do Current Assets (CA) exceedCurrent Liabilities (CL)? This is
an indication of your ability to pay your
AAccccoouunnttiinngg 110011:: HHooww ttoo RReeaadd YYoouurr BBaallaannccee SShheeeett continued from page 22
FIN
AN
CIA
L
Oto’s Scope Spring Edition 2010 23
Assets Current Assets
Petty Cash 1,000 Cash In Bank 151,000 Money Market 26,000
Total Cash and Cash Equivalents 178,000 Accounts Receivable, Net of Adjustments 180,000 Inventory 20,000Other Current Assets
Prepaid Med/Mal Insurance 24,000 Prepaid Property Taxes 11,000
Total Other Current Assets 35,000 Total Current Assets 413,000
Fixed Assets Furniture and Equipment 625,000 Leasehold Improvements 180,000 AD - Furniture and Equipment (214,000) AA - Leasehold Improvements (60,000)
Total Fixed Assets: 531,000Other Assets
Investment in Surgery Center 160,000 Org Costs 40,000AA - Org Costs (32,000)
Total Other Assets: 168,000Total Assets 1,112,000
ACME Ear Nose and Throat AssociatesBalance SheetApril 30, 2010
Liabilities and Shareholders' EquityCurrent Liabilities
Accounts Payable 128,000Accrued Expenses 32,000Accrued 401K/Profit Sharing 28,000Line of Credit 100,000Current Portion of Long-Term Debt 75,000
Total Current Liabilities 363,000Long-term liabilities
Note Payable - CT Scanner, Net of Current Portion 125,000Note Payable - Surgey Center, Net of Current Portion 100,000Note Payable - Equipment, Net of Current Portion 300,000
Total Long-Term Liabilities 525,000Total Liabilities 888,000
Shareholder EquityCommon Stock 200,000Retained Earnings ( 73,000)Retained Earnings - Current Year 97,000
Total Equity 224,000Total Liabilities and Shareholders' Equity 1,112,000
The following items are not necessarily in order, but it is a good place to start!

So let’s look to see how where we are.
Cash $ 178,000 A/P due in 30 days (118,000)Accrued Expenses ( 20,000)Current L-T Debt ( 6,250)Cash Available $ 33,750
It looks like we are in decent shape,and if we wanted to pay down on the line of credit, we could feelcomfortable in paying $15,000 to$25,000 this month.
If, in the above example, we foundthat we had a deficit in cash availa -ble (more obligations than cash),you would want to look deeper forthe reasons behind this situation.That would require looking intoother areas that affect the abovebalances. For example, your paya -bles due in 30 days might have somethat actually are due beyond 30 days,thus overstating the $118,000 above.This might happen because of data
entry error or maybe the A/P clerk isgoing on vacation and wants to do acheck run to cover the next 45 days.Your doctor(s) might have come offa month where a lot of them were onvacation and charges were low, thusaffecting your current cash balance.The month could have been duringspring break and you just were slow. If you understand yourbusiness, you know where to getyour answers, and it will help youunderstand your situation.
I believe that your CAs and CLs arethe keys to managing the business —from the first day of the month to thelast day of the month — because somuch of what we do daily ends up inthese areas: patient visits, employees,medical supplies, the lights in thebuilding, etc. All of these flow throughthe CA or CL side of the balance sheet.With that said, we cannot ignore therest of the balance sheet.
liabilities due over the next 30 days.You will need to start by running anaccounts payable (A/P) aging report toget the portion due in the next 30 days.An accounts payable aging report helpsthe management to evaluate which oftheir payments are going to be due atwhich date. This helps the manage-ment to assign or manage the amountrequired to pay the vendors when theyare due. Assume we have $118,000 ofA/P due in 30 days, and our accruedexpenses and accrued 401K/profitsharing require another $20,000 incash payments this coming month. Isthere anything else we need to add?Don’t forget the current month ofprincipal payments on your long-termdebt. Because this represents the next 12 months, we will just divide the $75,000 by 12, which gives us$6,250. Do we plan on paying downour line of credit? In most cases, thatanswer come after we perform thisanalysis.
AAccccoouunnttiinngg 110011:: HHooww ttoo RReeaadd YYoouurr BBaallaannccee SShheeeett continued from page 23
FIN
AN
CIA
L
24 Spring Edition 2010 Oto’s Scope
The long-term portion
Let’s take a look at the longer-term portions of our balance sheet. Usually, we incur debt to pay for durable goods(medical equipment, furniture and leasehold improvements). In our example, we have $805,000 in fixed assets with a bookvalue of $531,000, meaning that we have expensed (through depreciation and/or amortization) $274,000 of the original cost
Assets Current Assets
Petty Cash 1,000 Cash In Bank 151,000 Money Market 26,000
Total Cash and Cash Equivalents 178,000 Accounts Receivable, Net of Adjustments 180,000 Inventory 20,000Other Current Assets
Prepaid Med/Mal Insurance 24,000 Prepaid Property Taxes 11,000
Total Other Current Assets 35,000 Total Current Assets 413,000
Fixed Assets Furniture and Equipment 625,000 Leasehold Improvements 180,000 AD - Furniture and Equipment (214,000) AA - Leasehold Improvements (60,000)
Total Fixed Assets: 531,000Other Assets
Investment in Surgery Center 160,000 Org Costs 40,000AA - Org Costs (32,000)
Total Other Assets: 168,000Total Assets 1,112,000
ACME Ear Nose and Throat AssociatesBalance SheetApril 30, 2010
Liabilities and Shareholders' EquityCurrent Liabilities
Accounts Payable 128,000Accrued Expenses 32,000Accrued 401K/Profit Sharing 28,000Line of Credit 100,000Current Portion of Long-Term Debt 75,000
Total Current Liabilities 363,000Long-term liabilities
Note Payable - CT Scanner, Net of Current Portion 125,000Note Payable - Surgey Center, Net of Current Portion 100,000Note Payable - Equipment, Net of Current Portion 300,000
Total Long-Term Liabilities 525,000Total Liabilities 888,000
Shareholder EquityCommon Stock 200,000Retained Earnings ( 73,000)Retained Earnings - Current Year 97,000
Total Equity 224,000Total Liabilities and Shareholders' Equity 1,112,000
Fixed Assets
Book Value
Long-term debt
Depreciation/Amortization
continued on page 25

investment for $160,000, with a loan of $120,000 on it. Your main concernswill be: Is the investment generatingenough cash flow from distributions tocover my debt service? If I had to sellit, would I receive more the $160,000?If the answer to both is yes, life if good!If not, then your real concern is thecash flow. When do you see it gene rat -ing enough cash to pay the debt? Maybeit was a new center and cash flow hasnot ramped up; maybe there have beensome issues with utilization that impactcash flow. The problem here is that it isan investment, and we typically do nothave much control over its operations.So what does that say? Do your duediligence before committing and borrow -ing funds so that you don’t have toworry about the cash flow!The last thing on the balance sheet
that we have not touched on is share -holders’ equity. This can be a source of“funds” to assist in the cash flow of thebusiness, meaning if there are profits,you might retain them in the form ofretained earnings, which would ulti -mately turn to cash to pay for obliga-tions. Or there might be additionalcapital contributions by the share -holders. The problem most of us have,is that we usually do not have signifi-cant retained earnings because anyearnings are usually passed through to the physicians as wages in order to avoid double taxation. (Earningsretained in a corporation are taxed andif they are distributed afterwards in theform of dividends.) Most physiciansprobably don’t want to write checks foradditional capital contributions! Themessage here: Manage the rest of thebalance sheet and Shareholders’ Equityfalls out – remember our equation:
Assets - Liabilities = Shareholders’ Equity(Net Worth)
In other words, if we are collectingour cash and not spending orborrowing beyond our ability to repay,Assets will exceed liabilities, leavingpositive Shareholders’ Equity.In summary, we could get into a
bunch of financial ratios and reallyconfuse the heck out of you! However,that is financial reading for anotherday. You do not have to be a finance
guru to identify problems on thebalance sheet. Your key to sleeping atnight involves understanding yourreceipts and payment cycles. Withoutcharges, you have no A/R, whichresults in no cash, which means youcan’t pay the bills to keep the lights onand staff happily employed. What youdon’t want in our CA versus CLanalysis is a situation where the cashside of the equation (cash andreceivables) is deteriorating, and thepayable side is increasing. This iswhere a look at historical data helps.What was our situation last month, lastyear, etc.? If your receipts cycle is strong, you
have a good collection percentage,good turnaround time between billingand receipts, and good processes inplace, you should rest peacefully atnight!
Jeff is responsible for the day-to-dayoperations and focuses his attentionon financial matters and strategicplanning of the organization. Mr. Dudley reports directly to the Presi-dent and Board of the group. Mr. Dudley joined SacENT in December2000, his first venture into healthcare.However, he brings more than 20 yearsof experience in financial and opera-tions management. Mr. Dudley joinedthe Association of Otolaryngology Ad-ministrators (AOA) in 2001, and hasserved on Leadership Counsel since2004, currently as Secretary/Treasurer.
Mr. Dudley has a Bachelor ofScience in Business Administrationfrom California State University, Chico and a Masters of Science inAccountancy from California StateUniversity, Sacramento. He spent 4 years with KPMG Peat Marwick andobtained his California Certified PublicAccountants license during that time.This license currently has an inactivestatus.
to our income statement. Our long-term debt is $600,000, which includesthe current portion of long-term debt of $75,000. In this amount, we have a$120,000 loan (including the currentportion) for our investment in a surgerycenter. The number we are interestedin is the $480,000 ($600,000 in longterm debt minus $120,000 loan) inlong-term debt on assets that have abook value of $531,000. You alwayswant the book value of assets to exceedthe debt you have on them. This willcreate built-in positive cash flow onyour balance sheet. How is that? Your fixed assets are
expensed to your income statementevery month through depreciation andamortization. This activity results intaking income (cash) away from yourprofits (wages to your doctors) andleaving it in the bank account to theprincipal portion of the debt. Thus, yourdebt service, principal and interestpayments — in a perfect world — willmatch what is expensed each month:the depreciation/amortization andinterest. (I say in a perfect worldbecause usually the timing differencesbetween the depreciation/amortizationexpenses that you recognize for taxpurposes likely will not match exactlyyour principal payments each year.) What the above analysis tells us,
though, is a high-level overview of ourability to pay long-term debt withoutlooking for other sources. If, in ourexample, long-term debt exceeded thebook value of assets, you would need to look for other sources of cash toultimately pay the debt. That couldcome from the sale of assets for a gain, the excess of CA or CL, retainedearnings or additional capitalcontributions.Other assets typically do not have a
huge impact on most private medicalpractices. You may or may not have aninvestment in something, like a surgerycenter in this example. You just want to make sure that you do have otherassets recorded on your balance sheetand that you will gain some form ofeconomic benefit over the comingyears. Otherwise, the asset should bedisposed of or written off. In ourexample, we have a surgery center
AAccccoouunnttiinngg 110011:: HHooww ttoo RReeaadd YYoouurr BBaallaannccee SShheeeett continued from page 24
FIN
AN
CIA
L
Oto’s Scope Spring Edition 2010 25

Other means might include lookingexternally, but still focusing on theprivate practice. For instance, manypractices are considering merging withothers to form larger single-specialtyor multi-specialty groups to takeadvan tage of the strengths that comewith greater numbers. Such strengthsinclude greater purchasing power, abetter ability to negotiate with payers,and less call coverage. The mergerand acquisition strategy is clearly onethat can work and carries many bene -fits, but the time, energy, and costexpended reaching this point can be asignificant drawback. The process oftaking various practices that have verydifferent identities, philosophies (bothclinical and operational), overheadstructures, income distribution plans,and trying to meld them together is no small feat. It requires extensive
planning and due diligence in order tosucceed, so much that many practicessimply don’t have the energy to godown this road. Yet, taking action toensure their practice is sustainablegoing forward is still needed.As a result, many physicians and
practices are looking for hospitalsupport; not in the form of employ -ment, but a less invasive approach tocollaboration. There are many compli -ance issues that require adherencewhen collaborating (at least in afinancial sense) with a hospital. Thetransaction must be “above board,”meaning it is consummated at fairmarket value and in no way involvesthe potential value of referrals. Thesekey compliance issues are outlined in the Stark Laws and Anti-kickback
continued on page 27
With changes continuing inMedicare reimbursement andhealthcare reform uncertainty,
physicians are seeking ways to insulatetheir practices and compensation ofwhat may lie ahead. While hospitalemployment is one method of accomp -lishing this, many physicians havelimited interest in such a close hospitalaffiliation. Physicians often perceiveemployment arrangements as “loss oftotal control” of their practice, one ofthe many aspects of practicingmedicine they appreciate most.As a result, physicians are looking
toward other means of protectingthem selves and their income. Physi -cians and practices can accomplishthis many ways internally. Thisincludes expanding service offeringsand hours of service, becoming opera -tionally leaner, and adopting newtechnologies - allowing more efficiency.
READER R I• Physicians looking for optionsto protect themselves andpractices
• Alignment strategies: Pay forCall, Service Line Management,Clinical Co-Management,Medical Directorship,Professional ServicesAgreement for ComprehensiveServices
Exploring Alignment Strategies to Protect Against Reimbursement UncertaintyBy Justin Chamblee, MAcc, CPA
26 Spring Edition 2010 Oto’s Scope
OP
ER
AT
IO
NS

Statutes. Further, if they are part -
Statutes. Further, if they are part -nering with a tax-exempt hospital,there are certain Internal RevenueService guidelines that must beadhered to. Physicians can partner with hospi -
tals many ways in a legally compliantmanner. These transactions tend to be mutually beneficial as the practiceis recognized (monetarily) for a keyservice performed, while the hospital is able to ensure that particular servicewill be available to their communitygoing forward. It is very important forphysicians to be aware of key align -ment strategies and begin exploringtheir potential, if they are not alreadyin place, such as:
� Pay for Call — Due to the in creasedpressure placed on physicians as aresult of higher levels of uninsuredpatients using the emergencydepartment (ED) as their primarymeans of healthcare, as well asshrinking call panels, many hospi -tals are beginning to providecompensation to physicians for EDcall coverage. In many cases, this is only after a certain number ofuncompensated days are providedeach month. For this to occur, alegitimate burden associated withthe ED call coverage must exist.Further, the focus on these
EExxpplloorriinngg AAlliiggnnmmeenntt SSttrraatteeggiieess ttoo PPrrootteecctt AAggaaiinnsstt RReeiimmbbuurrsseemmeenntt UUnncceerrttaaiinnttyy continued from page 26
nering with a tax-exempt hospital,there are certain Internal RevenueService guidelines that must beadhered to. Physicians can partner with hospi -
tals many ways in a legally compliantmanner. These transactions tend to be mutually beneficial as the practiceis recognized (monetarily) for a keyservice performed, while the hospital is able to ensure that particular servicewill be available to their communitygoing forward. It is very important forphysicians to be aware of key align -ment strategies and begin exploringtheir potential, if they are not alreadyin place, such as:
� Pay for Call — Due to the in creasedpressure placed on physicians as aresult of higher levels of uninsuredpatients using the emergencydepartment (ED) as their primarymeans of healthcare, as well asshrinking call panels, many hospi -tals are beginning to providecompensation to physicians for EDcall coverage. In many cases, this is only after a certain number ofuncompensated days are providedeach month. For this to occur, alegitimate burden associated withthe ED call coverage must exist.Further, the focus on thesearrangements is to alleviate the
burden associated with seeingunassigned patients. In no way isany of the potential compensationintended to remunerate the physi -cians for taking care of their ownpatients who present in the ED.
There are several different ways thatED call coverage is compensated.The most traditional, and widelyused, method is a daily stipend.Essentially, this is compensation fora 24-hour period of call coverage.Thus, the physician covering the EDthat day would be eligible to receivethe stipend (subject to the inclusion/fulfillment of any gratis days). Manyhospitals are also exploring avariable payment process whereinthe compensation provided is tieddirectly to the uninsured patientsseen and services provided in theED. Thus, the physician will only be paid for actual work performed.Typically, this is on a per wRVUbasis or is tied to the Medicarereimbursement rates. While thisvariable payment helps to align the compensation with the burden,in many cases it is ineffective inenticing physicians to take ED call,as it does not address the overallpersonal burden of being on call.Meaning, there is a toll on aphysician’s quality of life fromproviding ED call coverage, even if they do not have to come see a patient in the ED.
� Service Line Management —Many hospitals do not want to simplypay for call, but they want to partnerwith a practice to provide ED callcoverage, as well as certain admin -istrative and non-billable clinicalactivities. Typically, these areencapsulated in a professionalservices agreement with compen sa -tion provided either in total or basedon the individual services provided.Many service line managementarrangements are coupled withother initiatives that involve qualityor cost-saving incentives. This way,the service line in question receivesexcellent oversight from physicians,but also the physicians and hospitalcan work together to achieve clini -
Oto’s Scope Spring Edition 2010 27
OP
ER
AT
IO
NS

costs were lowered from $10,000down to $5,000, the hospital and physicians may share equally in thesavings, resulting in the physiciansreceiving a $2,500 payment. Oncethe maximum efficiency is achievedwith the cost savings, the gain-sharing arrangements lose theirluster and tend to fade away. Withclinical co-management, the focus is more so on achieving and thenmaintaining the low level of costs. If the costs are maintained at a low level, it continues to trigger apayment to the physicians year overyear. Thus, the focus on maintain -ing costs at a low level continuesindefinitely into the future.
� Medical Directorship — Medicaldirectorships have been around for a long time, but in the past many ofthese positions have been filled byphysicians without compensation.Due to the increased timephysicians are spending in theirpractices to generate a fair marketvalue wage, more hospitals arebeginning to compensate for theseservices to ensure they continue tohave the proper clinical and admini -strative oversight. Typically, theseare compensated on an hourly basisusing a fair market value hourlyrate. Very rarely are there medicaldirectorships that simply pay an
annual stipend. Much more focus ison ensuring that any payment madeis tied to actual work performed.Thus, physicians are required to keeplogs of the time spent performingservices and then submit them tothe hospital for payment. Further,most medical directorships includesome sort of annual maximum pay -ment amount to ensure the hourlypayments made do not becomeexcessive.
� Professional Services Agreementfor Comprehensive Services —This is often referenced as“employment lite,” denoting that apractice still retains its identity as aprivate practice, but turns its billingand collection function over to thehospital. The hospital then bills andcollects for the physician’s services,paying them a fair market valuecollections rate for the services they provide, either in total, perwork-RVU, or some other measure.This is a very attractive model tophysicians as it allows them tolargely retain their autonomy as aprivate practice, but reduce theirexposure, somewhat, to continueddeclines in their income as a resultof the hospital becoming theprimary source of revenue. In manyinstances, a professional servicesarrangement is a “stepping stone”
cal excellence or reduce costswithin the service line.
� Clinical Co-Management — Thisinvolves a hospital and physicianspartnering to achieve certain goalswithin a specific clinical serviceline. Usually, these goals arefocused on quality and operationalmeasures and results in funds beingpaid to the physicians once thesemeasures are achieved. Clinical co-management can also includesome medical directorship compen -sation. An example of a clinicalco-management arrangement couldinclude a focus on cost savings,wherein if the costs within theservice line are reduced and remainat a certain benchmark threshold,this would trigger an incentivepayment to the physicians. Thus,the hospital and physicians wouldbe sharing in any cost savings thatwould be achieved. This is similarto some gain-sharing arrangements,with notable caveats. Mainly, with a gain-sharing arrangement, thehospital and physician would sharein the actual cost savings. Thus, if
continued on page 28
EExxpplloorriinngg AAlliiggnnmmeenntt SSttrraatteeggiieess ttoo PPrrootteecctt AAggaaiinnsstt RReeiimmbbuurrsseemmeenntt UUnncceerrttaaiinnttyy continued from page 27
28 Spring Edition 2010 Oto’s Scope
EasternDonna HankHope Lynn StrautPatranella MajewskiBarry RafanelliTammy MarksAngely RamosLee LarocqueKathleen EddowesTineke Hall
Great PlainsShannon LakinPaula Meisinger
North CentralPredrag SukovicHayley BurtonDavid LuickStephen MeierRachel GajdaWilliam Van KempenSteven SandquistCathy Cheshire
PacificKellie MoremanDarlene DedmonKathie PulleyJudie Inteso
SouthernApril BallardRosalia CalhetaSuzanne MurphyChristopher Lee, MDMary GuestMelissa ParksTricia Long
SouthwestApril RichardsonPatrick Fraley, MDBrenda TumlinsonStacie Chapman
Welcome to Our Newest Members!
OP
ER
AT
IO
NS
Oto’s Scope Spring Edition 2010 29
• Access to a network of ENT administrative professionalsfrom across the country.
• Educational programming specific to otolar yn gologyadministration, including regular webinars and our AnnualEducational Conference.
• Online resources, including downloadable forms, policies,procedures, job descriptions, and more for your practice.
• Regularly updated resources,including our ENT-Specific Salary and Benchmarking Surveys, and our Clinical Support Staff Manual.
Wednesday, June 30 | 1:00 p.m.EasternThe Shove: No Matter Where YouAre, It’s Time to Begin AgainPresented by Susan Good, Au.D.
JULY . . . . .Wednesday, July 14 | 1:00 p.m.EasternICD-10 Transition: Will You BeReady?Presented by Deborah Grider, CPC, CPC-I, CPC-H, CPC-P, COBGC, CEMC, CCS-P
Wednesday, July 21 | 1:00 p.m.EasternMyths and Facts about EMR ImplementationPresented by Judy Boesen and Dr. Lewis Romett
Need Education? Upcoming AOA Webinars
You Can’t Afford Not to Join!
What can AOA offer your practice?
AOA Webinars allow you the oppor tunityto enjoy quality educa tional presen tations,specifically geared toward otolaryngologyprac tice management, from the comfort of your own office. Need credit for yourcontinuing educa tion? Typic ally, you canearn 1.5 CEUs for each AOA webinar thatyou attend. And if you miss a webinar,purchase the recording on CD to listen atyour leisure. You can’t beat the value andconvenience that our webinars offer. Foreven MORE value, AOA members can pur -chase webinar bundles – the more you buy,the more you save. But hurry, because thisoffer ends on June 30!Check out the webinar page of our website
for more information on bundles, record ings,registration, and a complete listing of ourwebi nar offerings, which are updatedfrequently. With an average of one webinarper week, we’re sure to have something topeak your interest. Visit www.oto-online.org/webinars to find out more!Register for one of these upcoming
webinars today and see how easy it can beto get the education you need to take yourcareer to the next level.
JUNE . . . . .Wednesday, June 2 | 1:00 p.m. Eastern The Sniffles, Sneezes and Stuffinessof Sinus and Allergy CodingPresented by Teresa Thompson, CPC
Wednesday, June 9 | 12:00 p.m.EasternMicrosoft Excel: 11 Things an ENTAdministrator Must KnowPresented by Drew Franklin, MBA,CMPE
Wednesday, June 16 | 1:00 p.m.EasternThe Nurse Practitioner in ENT andAllergyPresented by Judith Lynch, MS, MA,APRN-BC, FAANP
Wednesday, June 23 | 1:00 p.m.EasternHow Ancillaries are Changing My PracticePresented by Jeff Dudley
To sign up for a webinar or order CD’s of previous webinars, please go to www.oto-online.org/webinars
�
� �
�
��
�

Today, as president of BusinessResource Center, Jeff presents to more than 100 audiences annually onhow to be leaders, increase revenues,communicate better, and pull togetheras a team. His keynotes, capnotes,seminars, and workshops move peopleto act – like a swift kick in the pants!Back at AOA-28 by popular demand,Jeff will give attendees plenty ofopportunities to learn his trio of topics,including (1) Mastering PresentationSkills, (2) Building Your Practice and(3) Value Driven Leadership.
Dennis Mannering: Who earnedthe coveted “certified speakingprofessional” designation 25 years ago and is considered a true guru ofattitudes and common sense. Dennis isentertaining, down-to-earth, inspiring,and motivational. A master storyteller,he uses stories to solidify that theconcept of “attitude” is the key tosuccess. You’ll be inspired by what youlearn, but more importantly, you’ll beinspired to use what you learn. Afterall, Attitudes Are Contagious!
George Conomikes: Who haswritten articles for more than 20publications on the subject of practicemanagement. He is the editor andpublisher of a pair of newsletters:“Conomikes Reports on MedicalPractice Management & ManagedCare” and “Conomikes MedicareHotline.” George is an economist whoformerly taught at the University ofChicago, where he was also head of the Commerce Department. He alsoauthored two books: “SuccessfulPractice Management Techniques” and“The Answer Book on MaximizingDoctor Profits.”
Bob Vosburgh: Who graduated asthe No. 1 ranked Air Force ROTC cadetfrom Iowa State University, where hegraduated with a degree in AerospaceEngineering. He then went on to theUniversity of Tennessee, where hecompleted his Masters Degree and PhDcoursework in Aerospace Engineering.
Bob’s presentations focus on strategyand leadership with a goal of in -creasing organizational productivity,implementing effective managementtools and motivating your staff.Sometimes, it really does take a rocket scientist!
Karen Zupko: Who is renowned forher dynamic, practical, and humorouspresentation style. She is a seasonedveteran with more than 35 years ofhealthcare advisory experience, includ -ing coaching, consulting, and trainingphysicians and their practice mana -gers. Karen promotes a group culturethat supports collegiality, patientsatisfaction and organizationaleffective ness. She is considered afriend of both the AOA and AAO-HNS,having participated in their annualprograms since 1984. She is thefounder of KarenZupko & Associates,Inc., a consulting firm she grew from a“solo practice” to a team of 17 experts.This year’s topic is “ENTs – From Entre -preneur to Employee,” and it promisesto be one of the program highlights.
Kim Pollock: Who specializes instreamlining the operations ofotolaryngology practices. Over the lastdecade, she has assisted large grouppractices — as well as academic andsolo practices — to improve collec -tions and overall efficiency. She is anexpert in auditing otolaryngologycoding and documentation for allsubspecialties of otolaryngology.Always a favorite of AOA attendees,Kim is the recipient of the prestigiousPresidential Citation Award from theSociety of Otorhino laryngology andHead-Neck Nurses.On behalf of your 2010 AOA Pro -
gram Committee, I encourage each of you to “Please Come To Boston.”I look forward to seeing you there!
Johnnie Gross, FHFMA, is the adminis-trator for Shea Ear Clinic in Memphis,TN, and the AOA Deputy ProgramChair.
Hear ye! Hear ye! Your town crierbeckons one and all to the faircity of Boston for AOA-28,
Sept. 22-25, where your 2010 programcommittee has planned an educationalcomposition of unparalleled quality. If the American Revolution proved any -thing, it proved that a man with a goodstout can accomplish the impossible —and as practice managers, we areexpected to accomplish the impossibleevery day! This year’s slate of talentedspeakers promises to both educate andinspire all attendees, regardless of yourlevel of expertise or years of experi -ence. Learn the latest strategies toaccomplish the impossible and succeedduring this revolution in the industry.Discover the latest in health care reformand what your associates in otolaryn -gology are doing to prepare for it. Joinmore than 300 ENT managers fromacross the nation for an engagingexperience that promises to help yourevolutionize your practice in prepa -ration for the uncertainties that awaitus all. A partial listing of this year’sline-up includes:
Sean Tuohy: The real-life husbandand father who inspired the bestsellingbook and blockbuster movie The BlindSide, starring Sandra Bullock and TimMcGraw. The Blind Side tells the storyof Michael Oher, a homeless teenagerturned first round draft pick NFLfootball player, with the support andlove of an unlikely adoptive family: the Tuohys. Sean, Michael’s adoptivefather, was a record-breaking basket -ball player for Ole Miss before becom -ing a successful entrepreneur and NBAbroadcaster. At the podium, he invitesaudiences to go behind-the-scenes ofthe Tuohy household with a heart -warming message: “In our house, we believe in miracles.”
Jeff Staads: Who began his speak -ing career screaming at the West Pointcadets he trained during his active tour of duty as a paratrooper in theU.S. Army’s 82nd Airborne Division.
30 Spring Edition 2010 Oto’s Scope
AO
A N
EW
S
Please Come To Boston!By: Johnnie Gross, FHFMA

Small Company. BIG NAME.
Xoran makes the complex simple.™
Hundreds of ENT physicians have made the choice to trust Xoran, the market leader and innovator in point-of-care CT imaging solutions. Xoran prides itself on being a small company that can devote it’s time and attention to the most important part of our business, our customers. Above and beyond our excellent customer service, our customers can expect innovative products that improve patient care and streamline practice work ow.
The Xoran MiniCAT™ is a compact, upright volume computed tomography system designed for high-resolution, bone window imaging of the sinuses, temporal bones, and skull base. MiniCAT™ provides immediate access to images at the patient’s point-of-care resulting in a faster diagnosis and treatment.
Xoran has a passion for improving patient care and an unwavering commitment to world-class customer service. Trust the company with years of experience serving the ENT community. For more information about Xoran and the MiniCAT™ call (800) 709-6726 or email [email protected].
Xoran MiniCAT™
Jumpstart your ICACTL Accreditation!August 21 - 22, 2010Chicago, IL

1844 Ardmore Blvd.Pittsburgh, PA 15221

















