
Osteoporosis July 2010
23
OSTEOPOROSIS • An extremely common disease • Characterised by low bone mass & loss of bone tissue that may lead to weak & fragile bone • If left untreated , it can progress without causing any pain until a bone breaks (fracture) • Most likely fractures – the hip bone, a bone in the spine or wrist • Hip fracture requires hospitalisation & major surgery – leads to serious walking disability & sometimes death • Fractures of spine or vertebrae can sometimes result in loss of height, severe back pain & deformity • Develops very slowly over a long period • Preventable & treatable
-
Upload
ooi-ah-guan -
Category
Documents
-
view
213 -
download
0
description
Osteoporosis
Transcript of Osteoporosis July 2010

OSTEOPOROSIS• An extremely common disease• Characterised by low bone mass & loss of bone tissue that
may lead to weak & fragile bone• If left untreated , it can progress without causing any pain
until a bone breaks (fracture)• Most likely fractures – the hip bone, a bone in the spine or
wrist• Hip fracture requires hospitalisation & major surgery – leads
to serious walking disability & sometimes death• Fractures of spine or vertebrae can sometimes result in loss of
height, severe back pain & deformity• Develops very slowly over a long period• Preventable & treatable

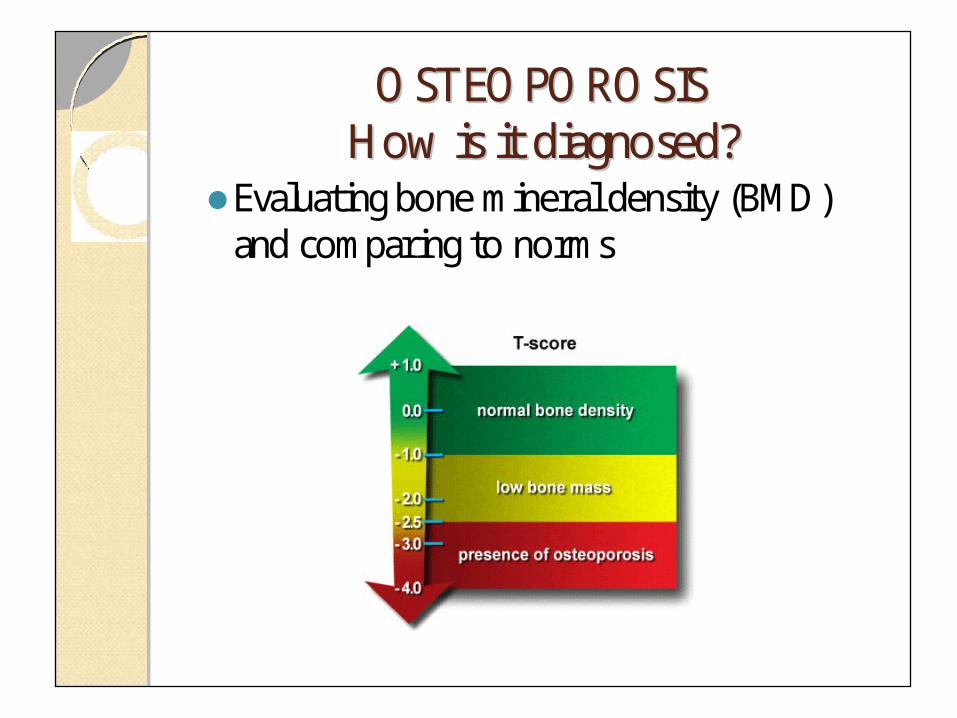
DIAGNOSIS• DEXA Scan – Dual Energy X-ray Absorptiometry - measure bone density compared to
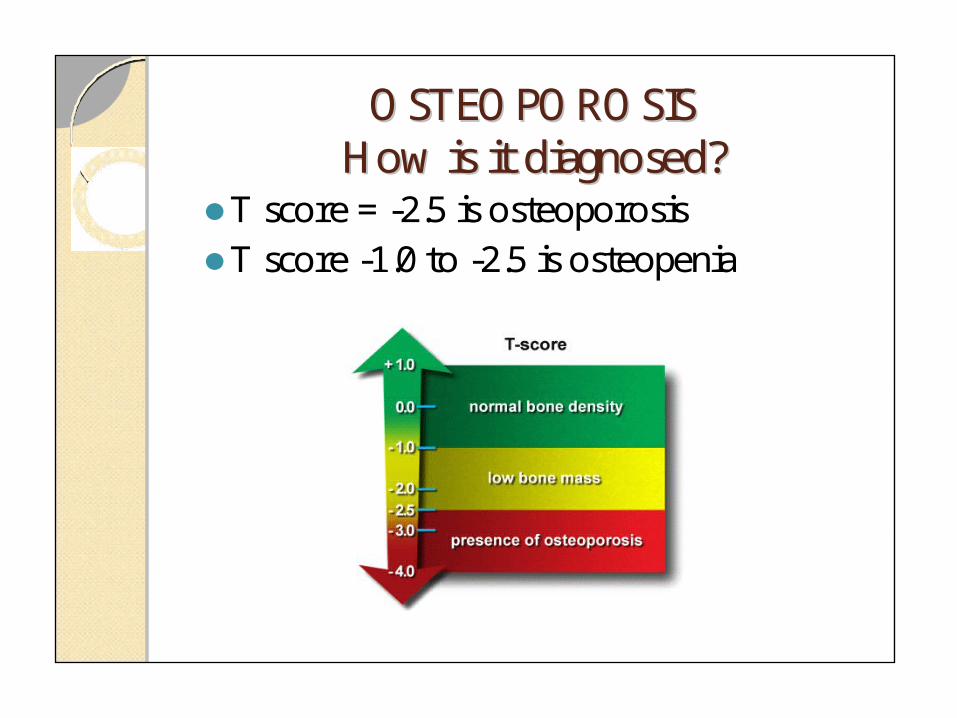
normal range - fast, simple & accurate T-score : -1.0 or greater – normal -1.0 and -2.5 – low bone mass
(osteopenia) - 2.5 and below – osteoporosis
• Ultrasound & CT Scan- also provide a reliable indication of bone mass

OSTEOPOROSISOSTEOPOROSISHow is it diagnosed?How is it diagnosed?
Gold Standard – bone densiometry(central DEXA) scan
OSTEOPOROSISOSTEOPOROSISHow is it diagnosed?How is it diagnosed?
Evaluating bone mineral density (BMD) and comparing to norms
OSTEOPOROSISOSTEOPOROSISHow is it diagnosed?How is it diagnosed?
T score = -2.5 is osteoporosisT score -1.0 to -2.5 is osteopenia

OSTEOPOROSISOSTEOPOROSISWho should be screened?Who should be screened?
Women age 65 and olderMen age 70 and olderPost-menopausal women age <65 with a
single additional risk factorWomen going through menopause with
significant risk factorsMen age 50-70 with risk factorsPrevious low-impact fractureLong-term use of high-risk medication

SYMPTOMS OF OSTEOPOROSIS
• Joint pain• Loss of height over time• Fracture• Difficulty standing / sitting up straight –
stooping position of elderly people is a visible sign of possible osteoporosis




RISK FACTORS OF OSTEOPOROSIS• Sex – women 2x more likely to develop
osteoporosis• Age - peak bone mass in 20’s after that ↓• Race – white or southeast Asians greater risk• Family history – gene is involved• Frame size – very thin or small at greater risk
because less peak bone mass• Lifetime exposure to estrogen – more estrogen
exposure less risk e.g. women who have late menopause

RISK FACTORS OF OSTEOPOROSIS- contd
• Eating Disorder – anorexia or bulimia• Medications – steroids, hyperthyroidism, loop diuretics• Low calcium consumption• Sedentary life style – even childhood activity level
affects bone mass• Chronic alcoholism – main cause of osteoporosis in men• Depression – faster loss of bone mass• Smoking – higher incidence• Caffeine - ↑ amount of calcium excreted. Caffeine also
found in fizzy drinks

Treatments for osteoporosis• Calcium & Vitamin D• Hormone Replacement Therapy• Selective Estrogen Receptor Modulators (SERMs)• Bisphosphonates• Calcitonin• Parathyroid Hormone• Others

Calcium Supplements• Slower rate of bone loss• Reduction of fractures in some pt• Adjunct to other osteoporosis treatment• Ca requirement is greatest in childhood, pregnancy & breastfeeding• Post menopausal women & older men also need to consume more
calcium• Calcium requirement : Adults < 50 years – 1000mg/day
> 50 years – 1200mg/day Women > 65 years – 1500mg/day
• Calcium preparationms --- Calcium citrate, Ca gluconate, Ca carbonate• Risk : mild GI upset, constipation, ?? Kidney stones
OSTEOPOROSISOSTEOPOROSISPreventionPrevention
Am I getting enough calcium??8 oz. glass of milk = 300mg?6 oz. cup yogurt = 300mg?1 oz or 1 cu in. cheese = 200mg?8 oz. fortified orange juice = 300mg
Vitamin D
• Sunlight is the best source of vit D• It is essential for intestinal absorption of calcium• Daily recommendation 400 -800 iu/day- esp in low
sunlight exposure, elderly, low vit D intake• ↓ risk of fracture in healthy elderly• Vit D derivatives e.g. calciferol, calcitriol (Rocaltrol),
alfacalcidol (One-Alpha) – effective alternative but expensive
Hormone Replacement Therapy (HRT)• For women going through menopause• Prevent bone density loss• Bone density loss greatest at beginning of menopause• Estrogen when initiated in the immediate post-menopausal
period can prevent osteoporosis• S/E : ↑ risk of stroke, heart disease, thromboembolism &
breast cancer• Can be estrogen alone or estrogen-progestogen in pt with
itact uterus• Progestogen added to reduce endometrial cancer • E.g. Prempak – an estrogen-progestogen therapy – no longer
the therapy of choice for osteoporosis in post-menopausal women
Bisphosphonates• Risedronate (Actonel), alendronate (Fosamax), ibandronate
(Bonviva) have been approved for osteoporosis• ↑ bone density loss by ↓ bone resorption and ↑ production
of new bone cells• ↓ risk of vertebral & non-vertebral fractures• These drugs are poorly absorbed• Elimination fr the body is SOLELY through renal clearance – so
contraindicated in pt with severe renal impairment

Bisphosphonates- contd• Dose : Alendronate – 70mg once a week or 10mg/day
Risedronate – 35mg once weekly Ibandronate – 150mg once a month• Tablets should be swallowed whole, do not chew or crush• Food significantly interferes with absorption , therefore
should be taken on empty stomach with 6-8 oz of water at least ½ hr before breakfast
• Cause esophagitis – pt should not lie down for an hour after taking med – prevent reflux
• S/E : abd pain, nausea, inflamed esophagus & esophagus ulcers

Calcitonin• Hormone made by the thyroid gland• Inhibit the cells that break down bones - osteoclasts• Improves bone architecture, relieves pain & increase function• Available in both injectable & nasal spray• Approved for treatment of osteoporosis in late menopausal
women• E.g. Miacalcic Nasal Spray – dose : 200 UNITS (1 Spray) into
one nostril daily• Downside : tolerance occurs with continuous use

Selective Estrogen Receptor Modulators (SERM)
• SERMs mimics the good effects of estrogen on bones• Raloxifene ( Evista) has been approved for prevention of osteoporosis• It reduces the occurrence of vertebral fracture in post-menopausal
women• No significant effect on CV, stroke & breast cancer• ↑ occurrence of hot flushes, risk of thromboembolism (comparable to
that of estrogen)• Dose : 60 mg daily• Special precaution : co-administration with systemic estrogen is not
recommended Not to be taken with cholestyramine
• Tamoxifen – is not FDA approved for osteoporosis management – but it has beneficial effects on bones
Parathyroid Hormone• Teriparatide (Forteo) –a form of parathyroid hormone that
help stimulate bone formation• Approved for use in post-menopausal women & men at high
risk for osteoporotic fractures• Shown to have greater increase in spine density greater
decrease in risk of non-vertebral fracture then with alendronate
• Also useful in glucocorticoid-induced osteoporosis• Dose : 20mcg once daily by SC inj in thigh or abdomen• Use with caution in pt with renal impairment• Contraindicated in pt with high PTH or who had radiation• AR : nausea, pain in the limb, headache, dizziness
Strontium Ranelate (Protaxos)• Stimulate bone formation & reduce bone resorption• ↓ risk of vertebral & hip fracture• Dose : 2g/day – a powder dissolve in water and taken once
daily• Take on empty stomach between meals, preferably at
bedtime at least 2 hr after food/milk or Ca supplement• Used when bisphosphonate not tolerated or is
contraindicated• Not recommended in severe renal impairment• S/E : headache, nausea, diarrhoea, dermatitis, memory loss,
seizures• Can sometimes cause severe allergic reactions


















