
Osteomyelitis
88
OSTEOMYELITIS DR SAGAR TOMAR Llrm medical college,meerut,up
-
Upload
sagar-tomar -
Category
Health & Medicine
-
view
158 -
download
5
Transcript of Osteomyelitis

OSTEOMYELITIS
DR SAGAR TOMAR
Llrm medical college,meerut,up

INTRODUCTION
Nelaton (1834) : coined osteomyelitis
The root words are
osteon (bone)
myelo (marrow)
these are combined with itis (inflammation) to
define the clinical state in which bone is infected
with microorganisms.

DEFINATION
Osteomyelitis is an inflammation of bone caused
by an infecting organism.
The infection may be limited to a single portion of
the bone or may involve numerous regions, such as
the marrow, cortex, periosteum, and the
surrounding soft tissue.

CLASSIFICATION
Attempts to classify are based on
(1) the duration and type of symptoms
(2)the mechanism of infection
(3)the type of host response

OSTEOMYELITIS
Acute: <2weeks Early acute
Late acute(4-5days)
Subacute: 2weeks—6weeks
Less virulent – more immune
Chronic: >6 weeks
Based on the duration and type of symptoms

CLASSIFIED ACCORDING TO MECHANISM
Osteomyelitis may be (waldvogel
classification)
1. Hematogenous (bacteremia)
2. contiguos (from adjacent root such
as open fracture or seeded implant)
3. chronic

BASED ON HOST RESPONSE
PYOGENIC
NON-PYOGENIC

ACUTE HEMATOGENOUS
OSTEOMYELITIS
Acute hematogenous osteomyelitis is the most
common type of bone infection and usually is seen
in children
It is caused by a bacteremia, which is a common
occurrence in childhood. Bacteriological seeding of
bone generally is associated with other factors such
as localized trauma, chronic illness, malnutrition, or
an inadequate immune system.

RISK FACTORS

Single pathogenic organism hematogenous osteomyelitis,
Multiple organisms direct inoculation or contiguous focus infection.
In infants:Staphylococcus
aureusStreptococcus
agalactiaeEscherichia coli
In children over one year of age:
Staphylococcus aureus, Streptococcus pyogenesHaemophilusinfluenzae1
adultsStaphylococcus aureus is
common organism isolated.
Etiology
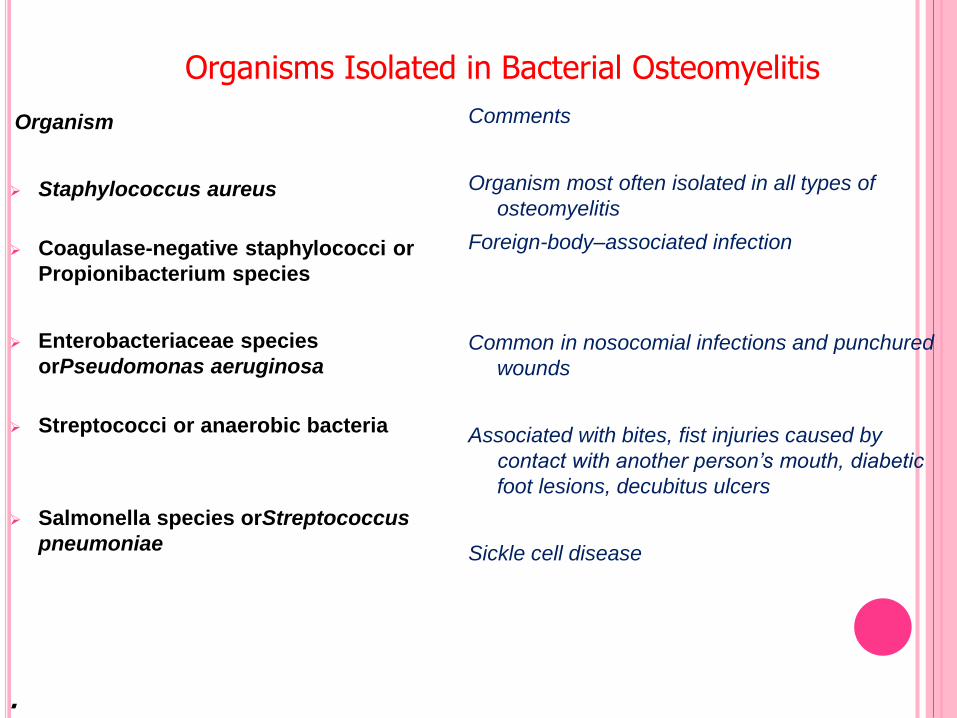
Organism
Staphylococcus aureus
Coagulase-negative staphylococci or
Propionibacterium species
Enterobacteriaceae species
orPseudomonas aeruginosa
Streptococci or anaerobic bacteria
Salmonella species orStreptococcus
pneumoniae
Comments
Organism most often isolated in all types of
osteomyelitis
Foreign-body–associated infection
Common in nosocomial infections and punchured
wounds
Associated with bites, fist injuries caused by
contact with another person’s mouth, diabetic
foot lesions, decubitus ulcers
Sickle cell disease
Organisms Isolated in Bacterial Osteomyelitis
.

WHY STAPHYLOCOCCUS MOST COMMON?
S.aureus and S.epidermis ----- elements of normal skin flora
S.aureus -----increased affinity for host proteins (traumatised bone)
Enzymes (coagulase, surface factor A) ----- hampers hosts immuneresponse .
Inactive “L” forms ------dormant for years
“Biofilm” (polysaccharide “slime” layer) ---- increases bacterialadherence to any substrate .
Large variety of adhesive proteins and glycoproteins ----- mediatebinding with bone components.

BACTERIAL RESISTANCE BY BIOFILM
If a planktic bacteria (free floating bacteria )
encouters a suitable inert material such as dead or
necrotic tissue ,foreign bodies, or any avascular
body part either by direct contamination,contiguos
spreading or hematogenous apreading
It attaches itself via vander wall forces (irrevesible
crosslinks)
(devitalised bone devoid of periosteum presents
collagen matrix to which bacteia can attach

Bacteria now begin to produce
mucopolysaccharides layer over themselves
called BIOFILM OR SLIME
the bacteria begin to COLONISE
A colonised bacteria can remain viable: when(a) the inoculum is larger than threshold levels,
(b) host defense mechanisms are impaired,
(c) the tissue on which the bacteria colonize is traumatized (or necrotic),
(d) a foreign body is present, and
(e) the surface (or tissue) is acellular or inanimate (e.g., dead bone, cartilage,
and biomaterials)

After colonisation bacteria begin to develop into
mature colonies.these colonies are resistant to
antibiotics because
---antibiotics are unable to cross mucopolysaccaride layer
(glycocalyx)
---bacteria within slime are dormant or have decreased
metabolic rate and also undergo phenotypic changes active
process such as cell membrane formation which are targeted
by antibiotics would be decreased.
---antibiotic concentration of 1500 times normal is required to
penetrate both biofilm and bacterial cell wall

Illustration of the biofilm bacterial colonization process.
First, the bacteria need to find an inert surface (e.g., implant or
dead tissue). Implants or dead tissue that have been integrated by
the host with some type of surface are not inert and will resist
colonization. Then, the colonization process will continue until
mature colonies are formed. Once mature, the colonies can
change based on environmental signals or signals between
colonies.

PATHOLOGY:
the most common site is lower femoral metaphysis
Other sites- upper tibial
upper femoral
upper humeral metaphyis

PATHOGENESIS:
Direct inoculation of microorganisms into bone penetrating injuries and surgical contamination are most common causes
Hematogenous spreadusually involves themetaphysis of longbones in children or thevertebral bodies inadults
OsteomyelitisMicroorganisms in bone
Contiguous focus of infectionseen in patients with severevascular disease.

PATHOGENESIS
Whatever may be the inciting cause the bacteria reaches the
metaphysis of rapidly growing bone & provokes an inflammatory
response.
why metaphysis is involved
1. Infected embolus is trapped in U-shaped small end arteries located
predominantly in metaphyseal region
2. Relative lack of phagocytosis activity in metaphyseal region
3. Highly vascularised region ---minor trauma—hemorrhage ----locus
minoris resistantae---excellent culture medium
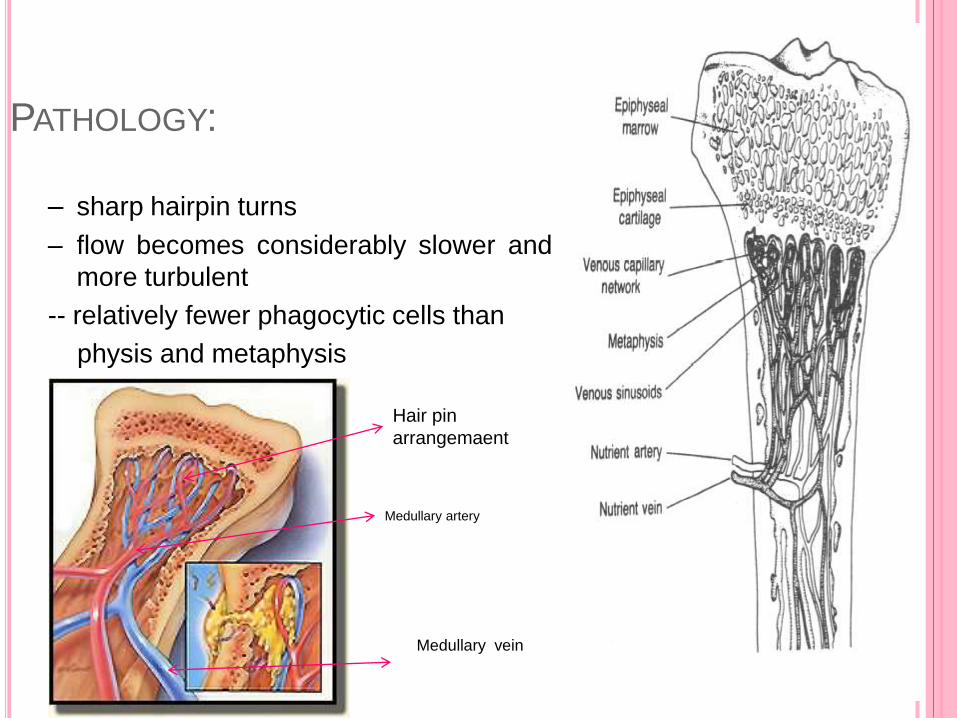
PATHOLOGY:
– sharp hairpin turns
– flow becomes considerably slower and
more turbulent
-- relatively fewer phagocytic cells than
physis and metaphysis
Medullary artery
Medullary vein
Hair pin
arrangemaent

PATHOLOGYThese are end-artery branches of the nutrient artery
Obstruction
Avascular necrosis of bone
tissue necrosis, breakdown of bone
acute inflammatory response due to infection
Squestra formation
Chronic osteomyelitis

THE INFLAMMATORY RESPONSE TO OSTEOMYELITIS:
Prostaglandin-E production has been shown to be five to thirty fold
higher in infected bone than in normal bone
postulated to be responsible for bone resorption and sequestrum
formation
Effective phagocytosis is defense in patients with osteomyelitis
Intramedullary oxygen tensions important for phagocytic function
oxygen tensions of <30 mm Hg impair normal phagocytic function

PATHOLOGY:
Pathologic features of chronic osteomyelitis are :
SEQUESTRUM is a devitalized avascular segment of bone, surrounded, by pus /infected granulation tissue and is more dense than surrounding bone .Because of avascularity , sequestrum does not decalcify , is more radio opaque and heavy , so sinks in waterIts outer surface is usually jagged / irregular due to erosive process by proteolytic enzymes in granulation tissue
Features: Dead piece of bone Pale Inner smooth ,outer rough Surrounded by infected granulation tissue trying to eat it Types-
ring(external fixator) tubular/match-stick(sickle) coke and rice grain(TB) Feathery(syphilis) Colored(fungal) Annular(amputation stumps)

PATHOLOGY:
Involucrum :is derived from the word “volvere” i.e. to wrap .It is
the result of reactive new bone formed by periosteal
reaction , in an attempt to wall off the infection by
forming a thick tense wall ,effectively sealing it off the blood stream just like a wall of abscess.
It is jagged on its inner surface but
smooth on its outer surface
Cloacae are single or multiple openings in involucrum and
are caused by rupture of periosteum due to pus
under tension .Exudates , sequestra are extruded
through the cloacae on the surface

CLINICAL FEATURES
calor, rubor, dolor, tumor
Heat, red, pain or tenderness, swelling
Initially, the lesion is within the medually cavity, there isno swelling, soft tissue is also normal.
The merely sign is deep tenderness.
Localized finger-tip tenderness is felt over or around themetaphysis.
it is necessary to palpate carefully all metaphysic areasto determine local tenderness,

DIAGNOSIS OF ACUTE OSTEOMYELITIS
PELTOLA AND VAHVANEN’S CRITERIA (if 2/4
are found)
1. Purulent material on aspiration of the affected
bone
2. Positive finding s of bone tissue or blood culture
3. Localised classic physical findings
a. bonny tenderness
b. overlying soft tissue edema ,erythema
4 Positive radiological imaging

DIAGNOSIS
LABORATORY DIAGNOSIS
Include - complete blood count
- erythrocyte sedimentation rate (ESR)
- C- reactive protein (CRP)
The white blood cell count will show a marked
leucocytosis as high as 20,000 or more
Peak elevation of the ESR occurs at 3 to 5 days
after infection and returns to normal approximately
3 weeks after treatment is begun.

ERYTHROCYTE SEDIMENTATION RATE
The ESR becomes elevated when infection is
present
Fractures or other underlying diseases can cause
elevation of the ESR.
The ESR also is unreliable in neonates, patients
with sickle cell disease, patients taking
corticosteroids, and patients whose symptoms have
been present for less than 48 hours

C-REACTIVE PROTEIN
CRP, synthesized by the liver in response to
infection, is a better way to follow the response of
infection to treatment.
CRP increases within 6 hours of infection, reaches
a peak elevation 2 days after infection, and returns
to normal within 1 week after adequate treatment
has begun

PLAIN RADIOGRAPH
The earliest changes are swelling of the soft tissue, periosteal thickening and/or elevation, and focal osteopenia.
The more diagnostic lytic changes are delayed and are associated with subacute and chronic osteomyelitis.
Osteoporosis is a feature of metabolically
active living bone; the segment that fails to
become osteoporotic is metablically inactive
and possibly dead.
Soft tissue swelling--- 1-3 days
Periosteal reaction---10-12 daysOsteomyelitis of the tibia of a
young child. Numerous
abscesses in the bone show as
radiolucency.

SINOGRAPHY:
Sinography can be performed if a sinus track
is present
Roentgenograms made in two planes after
injection of radiopaque liquid into sinus.
Helpful in locating focus of infection in
chronic osteomyelitis.
A valuable adjunct to surgical planning

RADIONUCLEOTIDE SCAN
The most common is 99mTc phosphate, which can
detect osteomyelitis within 48 hours after clinical
onset of infection.
The uptake of this compound is related primarily to
osteoblastic activity, although regional blood flow
also plays a role in skeletal uptake.
The three-phase bone scan consists of images
taken in
(1) the flow phase,
(2) the immediate or equilibrium phase
(3) the delayed phase

RADIONUCLEOTIDE SCAN
Flow phase- shows blood flow
Immediate or equilibrium - shows relative flow
and distribution of radio isotope into extracellular
matrix
Delayed phase-shows osteoblastic activity
Osteomyelitis shows increase uptake in all three
phase

MRI
MRI has very high sensitivity and specificity for the
diagnosis of osteomyelitis.
three types of images
T1 image- shows fat as a high bright signal
T2 image- shows water as a bright signal
STIR image – produced by suppressing the fat
signal
The classic findings of osteomyelitis on MRI are a
decrease in the normally high marrow signal on T1
images and a normal or increased signal on T2
images

MRI
The reported abnormal images reflect an increase
in water content, resulting from edema in the
marrow cavity. Marrow fat is replaced by edema
and cellular infiltrates that are lower in signal than
fat on T1 images and higher in signal than fat on T2
and STIR image

ULTRASONOGRAPHY
may detect a subperiosteal collection of fluid in
early stages of osteomyelitis.
To establish if joint effusion is present
To localise needle aspiration

CT SCAN
detecting smaller areas of cortical destruction,
Small foci of gas or foreign bodies,
sequestra formation (areas of necrotic bone separated by granulation tissue from living bone)
involucra (a layer ofliving bone that has formed along the sequestrum),
cloacae (an opening in the involucrum through which the sequestrum and granulation tissue may be discharged)
surrounding soft-tissue abscesses and
the replacement of the normal bone marrow fat with pus.

CULTURAL STUDIES
Key to the successful management of osteomyelitisis the isolation of the involved pathogens before the initiation of antibiotics in order to tailor optimal antimicrobial therapy
Cultures of superficial wounds or sinus tracks should not be relied on because they have been shown to be poor indicators of deep infection and usually are polymicrobial.
The preferred specimen in most bacterial and yeast infections is aspirated fluid (joint or purulent fluid). A deep wound biopsy or a curetted specimen after cleaning the wound is acceptable.

TREATMENT
1. General treatment: nutritional therapy or
general supportive treatment by intaking
enough caloric, protein, vitamin etc.
2. Antibiotic therapy
3. Surgical treatment
4. Immobilization

TREATMENT
NADE’S PRINCIPLES
1. an appropriate antibiotic will b effective before pus formation
2. Antibiotics will not sterilize avascular tissues or abscess and
such areas require surgical removal
3. If such removal is effective, antibiotics should prevent there
reformation and therefore primary wound closure should be
safe.
4. Surgery should not further damage already ischeamic bone
and soft tissue.
5. Antibiotics should be continued after surgery.

ANTIBIOTICS THERAPY
PATHOGEN FIRST LINE DRUG SECOND OPTIONS

OPERATIVE INDICATIONS
1. The presence of an abscess requiring drainage
2. Failure of the patient to improve despite
appropriate intravenous antibiotic treatment

COMPLICATIONS
Chronic osteomyelitis- 2% in >3wks, 19% in < 3wks
Septic arthritis
Growth disturbance
Septicemia
DVT
Pulmonary embolism

SUBACUTE OSTEOMYELITIS
This has a more incidious in onset and lacks the
severity of symptoms
Duration between 2-6 weeks
The indolent course of subacute osteomyelitis is
thought to be the result of increased host
resistance, decreased bacterial virulence, or the
administration of antibiotics before the onset of
symptoms

SUB ACUTE OSTEOMYELITIS CLASSIFICATION
Type Gledhill Classification Robert et al. Classification
I Solitary localized zone of
radiolucency surrounded by
reactive new bone formation
Ia—Punched-out radiolucency
Ib—Punched-out radiolucent
lesion with sclerotic margin
II Metaphyseal radiolucencies with
cortical erosion
—
III Cortical hyperostosis in diaphysis;
no onion skinning
Localized cortical and periosteal
reaction
IV Subperiosteal new bone and onion
skin layering
Onion skin periosteal reaction
V — Central radiolucency in epiphysis
VI — Destructive process involving
vertebral body

Anatomical type 1, central metaphyseal
lesion;
type 2, eccentric metaphyseallesion with cortical erosion;
type 3, diaphyseal cortical lesion;
type 4, diaphyseal lesion with periosteal new bone formation, but without definite bony lesion;
type 5, primary subacuteepiphyseal osteomyelitis; and
type 6, subacute osteomyelitiscrossing physis to involve metaphysis and epiphysis

TREATMENT
biopsy and curettage folllowed by treatment with
appropriate antibiotics

BRODIE’S ABSCESS
A Brodie abscess is a localized form of subacute
osteomyelitis that occurs most often in the long
bones of the lower extremities of young adult
Organisms of low virulence are believed to cause
the lesion. S. aureus is cultured in 50% of patients;
in 20%, the culture is negative.
The WBC count and blood culture usually shows no
abnormality but the ESR is sometimes elevated.

BRODIE’S ABSCESS
Bone abscess containing pus or jelly like granulation tissuesurrounded by a zone of sclerosis
Age 11-20 yrs, metaphyseal area, usually upper tibia or lowerfemur
Deep boring pain, worse at night, relieved by rest
On xray-Circular or oval luscency surrounded
by zone of sclerosis
Treatment:
Conservative if no doubt - rest + antibiotic for 6 wks.
if no response – surgical evacuation & curettage,
if large cavity - packed with cancellous bone graft

BRODIE’S ABSCESS
Brodie abscess. (A) AP radiograph of the femur
showing a lucent area (arrow) with cortical thickening
and sclerosis. (B) Axial CT image showing a central
sequestrum (arrowhead) and sinus tract (cloaca)
(arrows) leading through the thickened cortex.

CHRONIC OSTEOMYELITIS
Duration > 6 weeks
The hallmark of chronic osteomyelitis is infected
dead bone within a compromised soft tissue
envelope.(sequestrum)
The infected foci within the bone are surrounded by
sclerotic, relatively avascular bone covered by a
thickened periosteum (involcrum) and scarred
muscle and subcutaneous tissue.
This avascular envelope of scar tissue leaves
systemic antibiotics essentially ineffective

CIERNY AND MADER CLASSIFICATION
Cierny and Mader developed a classification system for chronic osteomyelitis, based on physiological and anatomical criteria, to determine the stage of infection.
Based on host class A- NORMAL
class B- COMPROMISED
class C-PROHIBITIVE
Based on anatomytype 1-MEDULLARY
type 2-SUPERFICIAL
type 3-LOCALISED
type 4-DIFFUSE
pairing of these forms 12 clinical stages
Clinical Stage
(Type+ Class = Clinical Stage)

CLASSIFICATION
Cierny et al -
Includes four anatomic stages
Stage-1, or medullary,osteomyelitis is confined to themedullary cavity of the bone.
Stage-2, or superficial,osteomyelitis involves only thecortical bone.
Stage-3, or localized,osteomyelitis usually involvesboth cortical and medullary bonebut does not involve the entirediameter of the bone.
Stage-4, or diffuse, osteomyelitisinvolves the entire thickness ofthe bone, with loss of stability.

CLASSIFICATION
With this system, a patient with osteomyelitis is classified as an A, B,or C host.
An “A” host has no systemic or local compromising factors. Theyhave a normal response to infection and surgery.
A “B” host is affected by one or more compromising factors.
Bs-systemic compromise
Bl-local compromise
Bls-both sys and local compromise
are compromised and have deficient wound healing capabilities.
A “C” host is so severely compromised that the radical treatmentnecessary would have an unacceptable risk-benefit ratio
DIAGNOSIS
The diagnosis of chronic osteomyelitis is based on clinical, laboratory, and imaging studies.
The “gold standard” is to obtain a biopsy specimen for histological and microbiological evaluation of the infected bone.
Investigations
x ray
ct scan
sinogram
usg
mri
radionucleotide scan

TREATMENT
Involves
Antibiotic suppression
Surgical debridement
Reconstruction
Correct host morbidity
-control blood sugar level in diabetic
-smoking cessation
-treatment of liver or renal malfunction
-optimising nutrition
-treatment of chronic disease

SURGICAL INTERVENTION
Debridement-
- it includes sequestrectomy and curettage
- Removal of all sequestra ,purulent material,and scarred and necrotic tissue until the
PAPRIKA SIGN ( active punctate bleeding bone)
-
- It results in the formation of DEAD SPACE
- methods described to eliminate this dead space are
- (1) bone grafting with primary or secondary closure;
- (2) use of antibiotic PMMA beads as a temporary filler of the dead space before
reconstruction;
- (3) local muscle flaps and skin grafting with or without bone grafting;
- (4) microvascular transfer of muscle, myocutaneous, osseous, and osteocutaneous
flaps; and
- (5) the use of bone transport (Ilizarov technique).

SEQUETRECTOMY AND CURRETTAGE
Sequestrectomy and curettage.
A, Affected bone is exposed, and sequestrum is removed.
B, All infected matter is removed.
C, Wound is either packed open or closed loosely over
drains.

POST SEQUESTRECTOMY
NO STABLISATION IS
NECESSARY WHEN 70% OF
THE ORIGINAL CORTEX
REMAINS INTACT
If >70% cortical volume has
been retained—protect by cast
Greater bone loss-Ext fix
Focal bone loss-open
cancellous BG/conventional
BG
Seg. bone loss—BG/Bone
transport/other devices
Radiologically if cortical
continuity of the involucrum is
50% of the over all cortical
diameter on 2 orthogonal views
then the involucrum is
structurally adequate

SAUCERIZATION
Extension of surgical
debridement
Debrided wounds left open
widely through excision of
overhanging soft tissue and
bone
Wounds drain freely
Abscesses do not form
Limited to areas where it causes
acceptable loss of function e.g.
Tibia and femur
May require stabilization
saucerisation

BASIC METODS TO COVER DEAD SPACE
OPEN BONE GRAFTING
The Papineau technique involves local debridement
followed by a period of open management until a
healthy granulation tissue covers the wound base,
after which fresh autogenous cancellous graft is
packed into the defect, followed by frequent
dressing changes until the graft becomes
incorporated
THREE STAGE OPERATIONStage I: Débridement and Stabilization
Stage II: Grafting
Stage III: Wound Coverage
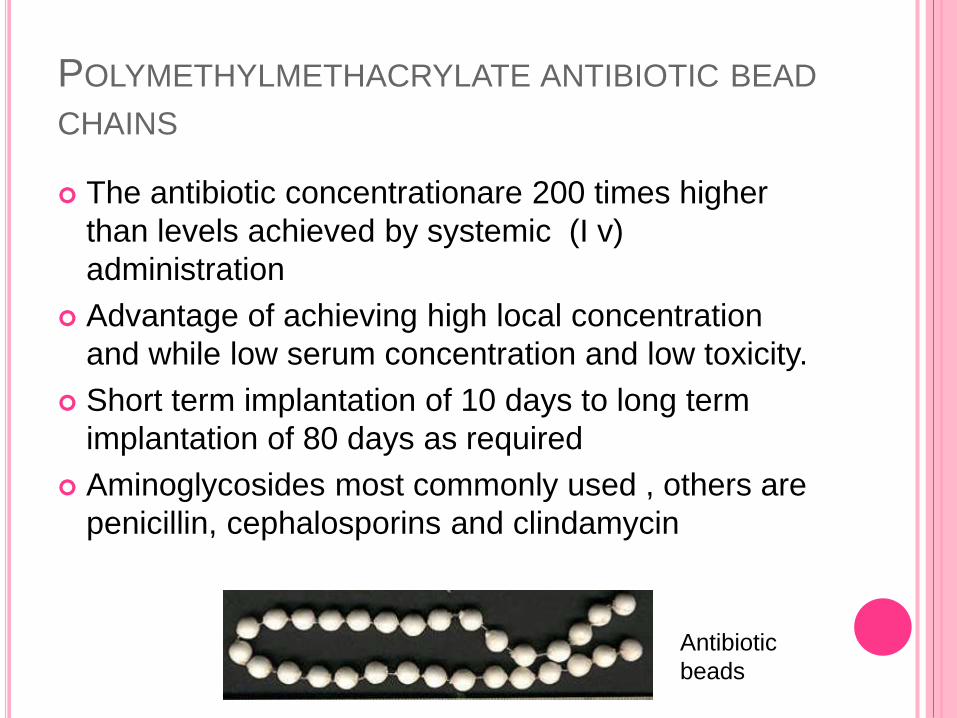
POLYMETHYLMETHACRYLATE ANTIBIOTIC BEAD
CHAINS
The antibiotic concentrationare 200 times higher
than levels achieved by systemic (I v)
administration
Advantage of achieving high local concentration
and while low serum concentration and low toxicity.
Short term implantation of 10 days to long term
implantation of 80 days as required
Aminoglycosides most commonly used , others are
penicillin, cephalosporins and clindamycin
Antibiotic
beads

BIODEGRADABLE ANTIBIOTIC DELIVERY
SYSTEM
Advantage over PMMA beads is that a secondary
procedure is not required to remove the implant.
Antibiotics are mixed with biodegradable substance
such as calcium sulfate or calcium phosphate to
produce reabsorbable beads or injectable filler
Reasobed in 8 weeks

CLOSED SUCTION DRAIN
Success rates of approximately 85% have been reported for the modified Lautenbach method of closed suction antibiotic ingress and egress irrigation systems
A more recent wound closure technique is negative pressure wound therapy (NPWT), which consists of a pump that generates a vacuum and is capable of creating a negative pressure environment within a sealed wound, dressing material used to pack and seal the wound, tubing for fluid removal from the wound area, and a container to collect waste materials removed from the wound

SOFT TISSUE TRANSFER
Soft tissue transfers to fill dead space left behind
after extensive débridement may range from a
localized muscle flap on a vascular pedicle to
microvascular free tissue transfer
The transfer of vascularized muscle tissue
improves the local biological environment by
bringing in a blood supply that is important in the
host's defense mechanisms and for antibiotic
delivery and osseous and soft tissue healing

ILIZAROV METHOD-
This technique allows radical resection of the
infected bone. A corticotomy is performed through
normal bone proximal and distal to the area of
disease. The bone is transported until union is
achieved.

ILIZAROV TECHNIQUE
A case of infected non-union of both bone leg managed by
ilizarov fixator application ,after bone transport the bone union is
acheived

HYPERBARIC OXYGEN THERAPY-HBO
- enhances oxygen-dependent leukocyte killing
through the production of hydrogen peroxide and
superoxide
- optimal tissue oxygen tension enhances
osteogenesis and neovascularization
Most wound healing patients receive one treatment
per day (20 MIN /DAY) for 20 – 30 days.

HYPERBARIC OXYGEN THERAPY

CHAMBER USED FOR HYPERBARIC OXYGEN
THERAPY

Culture Blood ± bone
Initial antibiotic selection
Change or confirm d/o culture results
Poor response
Operative treatment unroofing ,abscess
drainage, IM reaming
4 wks antibiotics
Failure
Retreat as
above
Arrest
Good response
Continue 2 wks parenteral & 4 wks
Oral antibiotics
Treatment algorithm of
Cierny-Mader Stage-1, or
hematogenous, long-
bone osteomyelitis.

Hardware removal
Bone stable
DEBRIDEMENT
INTRAMEDULLARY REAMING
AntibioticsContinue 2 wks
parenteral & 4 wks Oral
Failure
Retreat as above
Arrest
Bone unstable
Suppressive antibiotic treatment until stabilisation
Treatment algorithm of
Cierny-Mader Stage-1
long-bone
osteomyelitis
associated with
infection at the site of
hardware

Superficial debridement
Biopsy & culture
Initial antibiotic selection
Change or confirm based on culture results
Continue antibiotics for 2 wks
± Local MUSCLE
coverage
Treatment
algorithm of
Cierny-Mader
Stage-2 long-bone
osteomyelitis

Biopsy & Culture
Initial antibiotic selection
Change or confirm d/o culture results
6wks antibiotics after major operative
debridement
Failure
Retreat as above
Arrest
Debridement
Hardware removal
Dead space management, beads, bone grafts, & muscle
flaps
Stabilisation
external fixation
Ilizarov technique
Soft tissue coverage
Treatment
algorithm of
Cierny-Mader
Stages-3 and 4
long-bone
osteomyelitis.

OSTEOMYELITIS RELATED TO IMPLANT
FIRST CASE
HARDWARE REMOVAL
retain hardware
continue antibiotics until healed
HARDWARE STABLE
BONE NOT HEALED
IMPLANT RELATED OSTEOMYELITIS

SECOND CASE
remove hardware, antibiotics, temporary stabilization, spacer, and reconstruction when clean
Hardware unstable + bone not healed =

THIRD CASE
remove hardware, debride with effort not to destabilize, control
dead space, and antibiotics
Hardware stable + bone healed

FOURTH CASE
remove hardware, temporary stabilization, spacer, antibi-otics, and
reconstruction when able.
Hardware stable + bone not healed + systemic effects
Consider amputation if unsuitable hostConsider amputation if unsuitable host

CHRONIC MULTIFOCAL OSTEOMYELITIS
In the 1970s it was noted that a number of children
presented with a low-grade form of bone disease that
behaved clinically like an acute osteomyelitis.
Typically it affected the long bones and went on to a
sclerotic reaction. The first episode would settle and
some months or even a few years later there would
be recurrence at another site.
No organisms are grown and the course of the
disease becomes chronic and relapsing.

The clinical importance is to avoid repeated
biopsy once the relapsing nature of the
condition has been recognized.
Plain radiographs are essential to recognize the
bone infection.
Skeletal scintigraphy is a good method of
screening for other lesions
whilst MRI is the best means of judging extent
and activity

SCLEROSING OSTEOMYELITIS OF GARRÉ
A rare type of osteomyelitis occuring in children and
young adults presenting with insidious onset of
pain, pyrexia and swelling.
Symptoms recur at intervals for several years and
subside graudlly . .
Radiological appearance is of intense sclerosis
resulting in thickned bone.
There is predilection for involvement of mandible
and shaft of long bones.

SALMONELLA OSTEOMYELITIS
Subacute form
More commonly in children with sickle cell anaemia
Occurs during the convalescent phase after an
attack of typhoid fever
Mutiple bones are affected ,bilaterally symmetrical
Radiologically- diaphyseal sclerosis

Salmonella osteomyelitis
Bone destruction of radial shaft and dense sequestrum (arrow)

TUBERCULOUS OSTEOMYELITIS
Tuberculous bone infection occurs secondarily
as a resolt of hematogenous spread from a
primary source such as lung or genitourinary
tract.
Bone infection is most typically slow growing
and indolent. Tuberculous ‘caries’ is seen where
the margin of the bone is scalloped and eaten
away. Large ‘cold’ abscesses occur. This means
that the patient is surprisingly well given the
size of the collection

Little or no surrounding reactive bone with presence of
osteopenia
Affects epiphysis, metaphysis and diaphysis.
Eccentric area of osteolysis is seen in metaphysic
Transepiphyseal spread of lytic lesion
No sequestrum formation is seen.
Occasionally, destruction in the mid diaphysis of a short
tubular bone of the hand or foot(tuberculous dactylitis)
may produce a fusiform enlargement of the entire
diaphysis is called as spina vetosa.

M. tuberculosis. Sagittal T1-weighted (A) and T2-weighted (B) MR
images showing bone erosions and a large inhomogeneous
posterior soft tissue abscess

THANK YOU













![Periacetabular Brucella Osteomyelitis - file.scirp.org · spondylitis, bursitis, tenosynovitis and osteomyelitis [3-6]. Brucella osteomyelitis may appear as a radiolucent area and](https://static.fdocuments.in/doc/165x107/5d52ce1188c993277b8b9aaa/periacetabular-brucella-osteomyelitis-filescirporg-spondylitis-bursitis.jpg)


