Osteoarthritis Final Report - University of Oklahoma · used is viscosupplementation in which...
63
Osteoarthritis Senior Capstone Design Project Submitted to: Dr. Miguel Bagajewicz University of Oklahoma “The Hyaluronan Solution to a Devastating Problem” By: Chris Clark And Kim Fink Spring 2006
Transcript of Osteoarthritis Final Report - University of Oklahoma · used is viscosupplementation in which...

Osteoarthritis
Senior Capstone Design Project
Submitted to:
Dr. Miguel Bagajewicz University of Oklahoma
“The Hyaluronan Solution to a Devastating Problem”
By: Chris Clark And Kim Fink
Spring 2006

1
Executive Summary
The primary goal of this project was to create a treatment for osteoarthritis that is superior to those currently found on the market. There are nearly 23 million of people in the US alone that suffer from this degenerative joint disease, and this number is continually increasing. Although most people with osteoarthritis are over the age of 65, anyone is susceptible and can develop the disease for a number of reasons including impact injury, obesity, and genetic defects. The actual mechanism for the development of osteoarthritis is not fully understood but one thought is that the viscoelastic properties of synovial fluid, the fluid that separates the articular surfaces of the knee joint, are reduced. Since the actual cause of the disease is unknown, current treatments are not able to stop or reverse the degeneration. One of the newest treatments being used is viscosupplementation in which derivatives of hyaluronic acid, the primary component of synovial fluid, is injected into the knee to restore the viscoelastic properties. These current treatments must be administered once per week for 3-5 weeks and only last for approximately 6 months. This leads to accumulating costs in addition to the inconvenience to patients causing an increase in demand for more successful treatments. Therefore, our task was to create a novel solution to provide longer-lasting effects over other products. The treatment being proposed is more stable – meaning less likely to degrade – than current treatments due to a novel crosslinker being introduced. A hyaluronic acid derivative will be made through “bottom-up” synthesis and modified with 2-vinyl. Then ammonium peroxydifulfate will be introduced as a crosslinker to create a hydrogel. This treatment will use hyaluronan as a basis for the structure due to its chemical properties and biocompatibility. Through the properties of hyaluronan and the crosslinking associated with the structure a viscosity of around 16 Pa·s will be reached under moderate shear rates. This value of viscosity has been found to be adequate through the lubrication theory. The structure will have a molecular weight around 3 million Daltons which will consist of approximately 6700 monomers and 1000 crosslinks. It has been found through economic analysis of the competition that in order for our product to be competitive our product would have to cost around $2,400 per total treatment. Through the application of microeconomics equations it has been found that the demand for our product at this price should range from 350,000 people in the beginning all the way up to 625,000 people. Using this expected demand and looking at the possibility that the expected demand could be wrong by a deviation of 200,000 people, risk was assessed to the Net Present Value. It was found that the mean expected Net Present Value was around $240 million after 10 years. We also aim to receive approval from the FDA and modeled this process by looking at different possible scenarios. By analyzing the risk of failure it was found that it would be most profitable and less risky to have 10 workers and 85 experiments to go through each module of the FDA process.

2
Table of Contents
I. Introduction……………………………………………………………… ….3
II. Anatomy of the Human Knee………………………………………………3
III.1 The Joint………… ……………………………………………………3
III.2 Articular Cartilage………………………………………………....... 4
III.3 Synovial Fluid……………………………………………………… ...6
III. Osteoarthritis……………………………………………………………….8
IV. Traditional Treatments…………………………………………………….9
V. New Treatments…………………………………………………………...11
VI. Our Solution…………………………………………………………….....12
VII. Lubrication Theory………………………………………………………..23
VIII. FDA Approval Process……………………………………………………27
IX. FDA Risk Analysis………………………………………………………...46
X. Demand…………………………………………………………………….48
XI. Cost Analysis………………………………………………………………51
XII. Conclusion…………………………………………………………………57
References………………………………………………………………………....59

3
I. Introduction
An estimated 47.8 million Americans currently suffer from arthritis, an often debilitating
joint disease, costing the United States’ economy nearly $6.1 billion per year.44 With the
average life span ever-increasing, Americans will likely work longer, even well into their 60s
and 70, leading to two-thirds of the working population being afflicted by arthritis.44
Osteoarthritis, the most common form of arthritis accounting for over 50% of the patients, is a
degenerative joint disease that can cause severe pain and hinder people from everyday activities
such as working, gardening, and playing with grandchildren. This paper provides the
background information necessary to understand this disease, discusses the problems with
current treatments, and offers a novel solution of intra-acticular injections of a derivative of
hyaluronic acid intended to increase efficacy of treatments, lower lifetime costs, and return social
activity to those suffering with osteoarthritis.
II. Anatomy of the Human Knee
Although extremely important to the study of osteoarthritis, the structure of the knee is
introduced here only to provide enough background information necessary to understand and
recognize any terms or ideas discussed later in the paper. We will begin with the joint itself in
order to build a complete picture of the main components affected by the disease.
II.1 The Joint
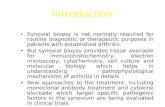
The knee joint is a type of synovial joint – one in which the ends of two bones are
free moving, joined only by connecting ligaments and a fluid-filled cavity called the
synovial space.4 Figure II.a shows the bones – the femur, tibia, fibula, and patella – the
major ligaments and tendons – the anterior cruciate ligament, collateral ligament, and
patella tendon – and the meniscal and articular cartilage.5

4
II.2 Articular Cartilage
II.2 Articular Cartilage
Although very thin, approximately only 2-3 mm thick for an average healthy
knee, the main function of articular cartilage is to transfer loads from one surface to
another preventing direct contact between opposing bones.19 Its flexibility allows for
pressure to be distributed over a larger area instead of at a concentrated point, while its
elasticity allows for the return of its original shape upon removal of the load. These two
properties are due to the highly organized extracellular matrix (ECM) that makes up the
articular cartilage. The ECM has a biphasic characteristic as it is comprised of a porous
solid phase of collagen, proteoglycans, and chondrocytes, and a liquid phase of mostly
water. This two-phase characteristic of cartilage is vital because when at a relaxed state,
the extracellular matrix is filled with water, but once a load is applied, the water is
flushed out of the porous ECM, leaving a stiff solid structure to support the load. Then
when pressure is removed, the water rushes back into the ECM returning the cartilage to
its original shape.
Collagen, a triple helical protein, makes up about 20% of the wet weight of
articular cartilage and is responsible for the tensile and shear strength of the extracellular
matrix.
Figure I I.a – The major bones, ligaments, and cartilage ofthe hu man knee extended (left) and bent (right). 5

5
Proteoglycans, accounting for 10-15% wet weight, are “bottlebrush”
macromolecules composed of a glycosaminoglycan backbone and noncovalently attached
core proteins with covalently attached smaller glycosaminoglycans.12
Glycosaminoglycans (GAGs) are unbranched polysaccharides found throughout the
body, and will be discussed in more detail later. The proteoglycans give compressive
strength to articular cartilage and provide the pores into which water flows and becomes
trapped.11
Condrocytes contribute only 5% wet weight but are essential to its maintenance
because they are the cells responsible for secreting the necessary components for
regeneration.11 However, without a vascular or nervous system in the cartilage these
cells do not receive the nutrients and signals necessary to activate proliferation in times of
needed repair. Therefore, once damaged it is very difficult for cartilage to be restored,
hence the need for this study.
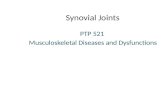
As previously mentioned, the extracellular matrix of articular cartilage is highly
structured as seen in Figure II.b. The zones of the cartilage are shown with a short
description of each.12
(i) Synovial Cavity – Very thin space between articular surfaces containing synovial fluid (to be discussed later)
(ii) Lamina Splendens (Articular surface) – highly fibrous, numerous collagen fibrils parallel to surface to resist tension
(iii) Tangential Zone – Flatter chondrocytes, thicker fibrils parallel to surface
(iv) Transitional Zone – Thickest zone, spherical condrocytes, collagen fibers perpendicular to surface to hold zones together
(v) Tidemark – Change in cartilage stiffness from transitional to calcified (vi) Subchondral Bone – The surface layer of bone covered with articular cartilage
Figure II.b – Zones of normal articular cartilage; shows the joints of the knee separated by the synovial cavity (i) 12

6
II.3 Synovial Fluid
Although articular cartilage has been the focus of many other studies of
osteoarthritis, the focus of this paper will be on the synovial fluid which also plays a vital
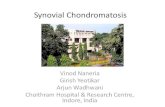
role in understanding and treating the disease. The synovial fluid is found in the synovial
space as was seen in Figure II.b and is contained inside the synovial membrane as shown
in Figure II.c. This semi-permeable membrane covers the non-cartilaginous surfaces
inside the joint cavity reaching around the entire ends of the femur and tibia. Although
more viscous than water, synovial fluid provides low-friction lubrication for the gliding
articular surfaces to help reduce wear of the cartilage.
Components
The main components of synovial fluid are water, proteins, and a particularly
important glycosaminoglycan, hyaluronic acid. The body’s natural hyaluronic acid (HA)
is a linear polysaccharide consisting of the two monomers D-glucuronic acid and N-
acetyl-D-glucosamine with a molecular weight of 105-107 Daltons and length of 500-
25,000 disaccharide units and appears in healthy synovial fluid at a concentration of 2-4
Figure II.c – Normal joint showing synovial fluid and synovial
membrane

7
mg/ml.18 One of the most important characteristics of HA is its polyanionic nature and
multiple reactive sites. The carboxylate group (-COOH) on each D-glucuronic acid
monomer carries a negative charge causing repulsion within the molecule itself while
attracting water molecules through hydrogen bonding. The backbone of hyaluronic acid
is stiff due to these intermolecular and solvent interactions. The axial hydrogen atoms
arrange in a non-polar, relatively hydrophobic face, while the equatorial side chains form
a polar hydrophilic face creating a coil-like conformation.18 The three reactive sites are
shown in Figure II.d and will be the possible sites for modification.
Figure II.d – HA molecule (2 disaccharide un its shown) indicating active sites 49
Because of the hydrogen bonding holding the HA molecules together and the
repulsion between the negative charges on the D-glucuronic acid monomer, HA forms a
mesh-like viscoelastic network that reconfigures upon loading and unloading.18 The
viscosity of hyaluronic acid in solution ranges based on molecular weight and shear rate.
For example, the relative viscosity – the viscosity of the pure substance divided by the
viscosity of the solvent – for HA with molecular weights 140, 500, and 2000 kDa is 1.11,
1.17, and 1.53, respectively, when the solvent is water at normal body temperature.39
Properties
The synovial space in the human knee joint is very narrow with an average width
of approximately 25-50 µm, but this can be as small as 0.8-1.5 µm in the high-load-

8
bearing areas.13,14 The volume of synovial fluid varies with age and health of the joint
but averages approximately 1 ml with a relative density close to unity. Healthy human
synovial fluid exhibits non-Newtonian shear-thinning behavior resulting in a decreased
viscosity at higher shear rates.19 Because of this, reporting the viscosity of synovial fluid
as a single value is impossible as it can range from 1-10,000 kg/m·s.39 As with articular
cartilage, the synovial fluid provides low-friction lubrication with a coefficient of friction
of 0.02.39
III. Osteoarthritis
Osteoarthritis is one of the most common of the several musculoskeletal disorders, but
unfortunately for millions of Americans, it is still not fully understood. For years it has been
referred to as simply a “wear-and-tear” disease, but researchers know that it is much more
complex than this term implies. Although osteoarthritis is most prevalent in people over the age
of 65, anyone is susceptible, even children. Several risk factors have been identified such as age,
obesity, injury, prolonged elevated activity, increased bone mineral content, endocrine and
metabolic disorders, and even genetic defects.15 Although the name “osteoarthritis” implies
inflammation, swelling is minor compared to the degeneration of the articular cartilage that leads
to bone-on-bone contact, hardening of underlying bone, and formation of osteophytes, more
commonly known as bone spurs, which are bony protrusions that grow near the end of the joint
as the body attempts to heal itself.
The degeneration progresses slowly through four stages. During the stationary phase, the
joint cavity narrows and small osteophytes begin to form. This narrowing is likely due to the
reduced viscoelasticity of the synovial fluid because of reduced hyaluronic acid concentration
and increased water content.21 Studies have shown that the HA present in osteoarthritic synovial
fluid has decreased molecular weight and increased crosslinking density, which allows the HA to

9
escape through the semi-permeable synovial membrane and also leaves the molecule more
susceptible to degradation. Increased pressure on the rough cartilage surface causes the normally
highly structured extracellular matrix to be disrupted, and the disease progresses. Next the
synovial space is obliterated, and high friction bone-on-bone contact occurs, leading then to the
formation of cysts in the subchondral bone. Finally large osteophytes form throughout the joint
causing pressure on surrounding nerves and severe pain.16 Figure III.a shows a comparison
between a normal healthy knee and a knee with fully developed osteoarthritis.
IV. Traditional Treatments
When first diagnosed, doctors will generally suggest simple treatments to help relieve the
early symptoms of osteoarthritis such as dieting, exercise, reduced activity, and support
devices.17 Dieting and weight loss can help reduce the amount of pressure supported by the
joints and possibly help slow the progression of OA. Exercise is essential to keep the joints
flexible as well as to maintain strong surrounding muscles; although, also important is decreasing
the frequency of strenuous activities will obviously help relieve pain by removing extra stress
Figure III.a – Normal vs. Osteoarthritic Knee

10
and allowing time for swelling to decrease. Furthermore, if a patient is having pain during
normal daily activities they are encouraged to use a walker, cane, brace to help redistribute some
of the load.17
Most people who are seeking medical treatment for osteoarthritis likely have more pain
than that which the above physical treatments are capable of reducing and therefore opt to take
oral analgesics, or pain relievers. Common over the counter pain relievers such as aspirin and
acetaminophens (Tylenol®), taken four times per day at 1000 mg/dose can be equally effective at
reducing inflammation as prescription pain medication.17 Although there are few adverse side
effects of acetaminophens, taking several doses a day for an extended period of time can be quite
costly as well as inconvenient. Different from acetaminophens but often prescribed are
nonsteroidal anti-inflammatory drugs (NSAIDs) which provide slightly better relief for moderate
pain, but have been shown to cause side effects on the kidney and stomach.17 Aspirin is grouped
into this category. A newer class of NSAIDs is the cylcooxygenase (COX-2) inhibitors, such as
the marketed Celebrex® and Vioxx®, which have fewer adverse effects but are more expensive
and have not been shown to be any safer than acetaminophens, as they can cause serious
interactions with other medications leading to gastrointestinal bleeding.17 Most important to
note, however, about oral analgesics is that while they can relieve moderate pain, they cannot
slow the degeneration.
As an alternative to oral pain relievers, patients are often suggested to receive an intra-
articular steroidal injection which can be administered three to four times per year. These have
been proven to significantly reduce pain for up to four weeks, but not necessarily are they able to
restore function. This is due to the power of the active ingredient cortisone to reduce severe
inflammation, but it is thought to possibly quicken the degeneration of the articular cartilage.
Therefore steroid injections are not recommended to be used repeatedly.21

11
With even increasing severity of pain, osteoarthritic patients have the option of
arthroscopic lavage and debridement in which a surgeon inserts a small camera into the knee
cavity, locates the damaged cartilage, washes the area with saline, and collects the loose debris.46
By smoothing out the articular surfaces, the treatment usually relieves pain for nearly 3 years.
However, this procedure, like the steroidal injections, greatly reduces pain, but because the
articular surfaces are already deformed, the range of motion is not fully restored and the
deterioration continues.
After the cartilage has completely deteriorated and the previous treatments have been
exhausted, the patient is forced into a total knee replacement. This invasive surgery involves the
removal of the osteoarthritic joint from of the knee and replacement with a mechanical
prosthesis. Although the parts do loosen over time, this procedure is by far the longest lasting
solution with a lifetime of 15-25 years. However, the costly surgery poses serious health risks
including infection and rejection by the body while requiring extensive physical therapy.
Although these traditional treatments have been widely used and studied, with the
exception of a total knee replacement, they must be used repeatedly, result in accumulating costs,
can cause adverse side effects, and still do not return full functionality to the patient.
V. New Treatments
Recently a new type of treatment for the relief of osteoarthritis has been in use in which
hyaluronic acid is injected into the joint cavity to restore the viscoelasticity to the synovial fluid;
this is known as viscosupplementation. These injections must be administered once per week for
3-5 weeks, depending on the particular product, and repeated after 6 months. The two main
available products are hyaluronan and Hylan G-F 20. Hyaluronan is intended to mimic the
body’s natural linear hyaluronic acid with an average molecular weight of 2x106 Da. Some
subgroups of clinical trials treated with hyaluronan showed positive results, while many others

12
showed no benefit over placebo.21 Hylan G-F 20 consists of crosslinked hyaluronic acid that is
intended to increase the average molecular weight of the HA in the synovial fluid in attempt to
restore its viscoelasticity. Clinical trials with hylan indicated significant superiority of the
injections over placebo as well as NSAIDs.21 Between the two products, crosslinked hylans
seemed to be more efficacious.
Because the exact mechanism of the role of hyaluronic acid in the synovial fluid is not
completely understood, the exact mechanism of how the HA injections provide relief are not
fully known either. However, it has been mentioned frequently that the problem with the current
HA injections is that the solution is not being retained inside the synovial space. This can either
be due transport across the synovial membrane, enzymatic degradation, or simply missing the
synovial cavity when the injection is administered.
Although more effective and less invasive than any other traditional treatment, it would
be beneficial to patients to reduce the frequency of injections by increasing retention time and
slowing degradation rates while maintaining a competitive cost. Our solution to this problem
will now be presented.
VI. Solution (HYAL-VYNE)
We propose the creation of a hyaluronan derivative that is chemically cross-linked by
ammonium peroxydisulfate. The new solution will be superior due to this enhanced cross-
linking. The enhanced cross-linking that is associated with the new solution will increase the
stability of molecule protecting it from degradation. This increased stability will require fewer
injections because of the longer life of the new solution in the body.
The typical chemical structure of HA found in the body has a repeating disaccharide unit
consisting of D-glucuronic acid and N-acetyl-D-glucosamine which can be better seen in Figure
VI.a33.

13
The chemical name is β-D-glucuronyl-(1→3)-N-acetyl-D-glucosamine
(GlcAβ(1→3)GlcNAc, N-acetylhyalobiuronate), which is linked in a β(1→4) fashion. The
molecular weight for this structure is typically around 2 million Dalton. One major advantage of
HA in the joints is its ability to bind large quantities of water, giving rise to its ability to lubricate
the joints and absorb shock.33 This will be explained in more detail later on.
The reason that HA was used in the creation of our new solution was because of HA’s
ability as stated earlier to bind to water. When HA is crosslinked it is able to form a three-
dimensional network of flexible chains. For an example of this crosslinking, look at Figure VI.b.
Figure VI.a – Disaccharide unit
Figure VI.b – Crosslinking Hydrogel Formation

14
Since HA has the ability to absorb water, when it forms this three-dimensional network of
flexible chains it turns the crosslinked material into a hydrogel. One important property of a
hydrogel is its ability to have the swelling controlled. By controlling the swelling, the degree of
hydration and consistency are able to reach properties similar to those of highly hydrated body
tissues.43 It has been found that solutions containing no hyaluronate do not lubricate a soft
tissue system, such as the space between joints, nearly as well as solutions containing
hyaluronate.39 HA in the synovial joints has been found to act as a lubricant and shock absorber,
storing energy between opposing cartilages.30
The new solution was created through a series of steps. The monomer created and used
in our reaction was an oxazoline-type monomer derived from N-acetylhyalobiuronate also
known as HA or hyaluronan. The method that was used to create the monomer that was used in
synthesis of our solution is described by Ochiai, Ohmae, Mori, and Kobayashi.35 Our HA
derivative monomer was created using a total of 8 steps as shown in Figure VII.c. This figure
represents the changes that are occurring to the structure between each step. The steps are
described in more detail after the figure. The figure also shows the final structure of the
substrate monomer that is created from this bottom-up synthesis. This monomer will be the basis
for our cross-linked HA derivative.

15
Substrate Synthesis Procedure
Here are the structures and steps used to create our substrate monomer in relation to the
figure. Each number in parentheses represents the chemical being described or used from the
figure, while each Roman numeral in parentheses represents the actual additives and step in the
reaction forming the substrate monomer:
Substrate Monomer was formed in the following manner:
(i) A solution of 3,4,6-tri-O-acetyl-2-azido-2-deoxy-α-D-glucopyranosyl
trichloroacetimidate (1) and benzyl alcohol in dry toluene in with presence of activated
Figure V II.c – Bottom -up synthesis of hyaluronic acid

16
MS4A is added to a solution of BF3·OEt2 in dry CH2Cl2 at -40 oC. This is then poured
into aqueous NaHCO3, and extracted with CHCl3. The organic layer is washed with
aqueous NaCl and then dried over MgSO4, filtered, and concentrated. The dried residue
is then purified by silica gel column chromatography (10:1 to 4:1 n-hexanes-EtOAc) to
give Benzyl 3,4,6-Tri-O-acetyl-2-azido-2-deoxy-β-D-glucopyranoside (2).
(ii) Compound 2 is then dissolved in 10:1 (v/v) MeOH-CH2Cl2, and then NaOMe in
MeOH is added dropwise. The compound was then neutralized by adding Dowex 50W-
X4 (H+ form). The resulting solution was Benzyl 2-Azido-2-deoxy-β-D-
glucopyranoside (3).
(iii) Compound 3 is then dissolved in MeCN followed by the addition of 2,2-
dimethoxypropane, Drierite, and camphor-10-sulfonic acid. This mixture is then
concentrated and put through silica gel column chromatography (10:1 n-hexanes-EtOAc)
to give Benzyl 2-Azido-2-deoxy-4,6-O-isopropylidene-β-D-glucopyranoside (4).
(iv) Compound 4 is used with the addition of donor 353 in dry CH2Cl2 with activated
MS4A. To this solution BF3•OEt2 in dry CH2Cl2 was added. This mixture is stirred for
30 minutes under an argon atmosphere. This is used to activate the reaction. The
reaction is terminated by the addition of Et3N. The mixture is then filtered through Celite
and poured into aqueous NaHCO3, and extracted with CHCl3. The organic layer is
washed with saturated aqueous NaCl and dried over MgSO4, filtered, and concentrated
resulting in the formation of solution Benzyl (Methyl 2,3,4-Tri-O-acetyl-β-D-
glucopyranosyluronate)-(1→3)-2-azido-2-deoxy-4,6-O-isopropylidene-β-D-
glucopyranoside (5).
(v) Compound 5 is dissolved in 80% aqueous AcOH and diluted with CHCl3. This
mixture is washed with aqueous NaHCO3, and aqueous NaCl. The organic layer is dried

17
over MgSO4, filtered through Celite, and concentrated. The residue is then purified by
silica gel column chromatography (1:1 to 1:4 n-hexanes-EtOAc) to give Benzyl (Methyl
2,3,4-Tri-O-acetyl-β-D-glucopyranosyluronate)-(1→3)-2-azido-2-deoxy-β-D-
glucopyranoside (6) 78%.
(vi) Compound 6 is put in MeOH containing palladium(II) hydroxide on activated
carbon. The reaction takes place in a hydrogen atmosphere giving a mixture with
compound 6.
(vii) The mixture is filtered and rinsed with MeOH. Then Et3N and acryloyl chloride
were added to the mixture. After the addition of pyridine the mixture is concentrated to
give (Methyl 2,3,4-Tri-O-acetyl-β-D-glucopyranosyluronate)-(1→3)-1,4,6-tri-O-
acetyl-2-acrylamido-2-deoxy-D-glucopyranose (Crude Product).
(viii) The crude product is treated with Ac2O and pyridine. Then MeOH is added to
stop the reaction. The residue is purified by silica gel column chromatography resulting
in the formation of (Methyl 2,3,4-Tri-O-acetyl-β-D-glucopyranosyluronate)-(1→3)-
1,4,6-tri-O-acetyl-2-acrylamido-2-deoxy-D-glucopyranose (7) (54%).
(ix) Compound 7 is added to dry 1,2-dichloroethane and then treated with trimethylsilyl
triflate (TMSOTf) in dry 1,2-dichloroethane using an argon atmosphere to cause the
reaction. To stop the reaction Et3N is added. This residue is purified through silica gel
column chromatography to give 2-Vinyl-4,5-dihydro-[4,6-di-O-acetyl-1,2-dideoxy-3-O-
(methyl 2,3,4-tri-O-acetyl-β-D-glucopyranosyluronate)-α-D-glucopyranoso][2,1-d]-
1,3-oxazole (8) (78%).
(x) Compound 8 is treated with NaOMe in MeOH and stirred until dry. This in turn
yields 2-Vinyl-4,5-dihydro-[1,2-dideoxy-3-O-(sodium β-D-glucopyranosyluronate)-
α-D-glucopyranoso][2,1-d]-1,3-oxazole ( crude substrate monomer).

18
(xi) The remaining methyl ester from step (x) is hydrolyzed in a carbonate buffer to form
2-Vinyl-4,5-dihydro-[1,2-dideoxy-3-O-(sodium β-D-glucopyranosyluronate)-
α-D-glucopyranoso][2,1-d]-1,3-oxazole (substrate monomer).
Polymerization
The idea of “transition-state analogue substrate” from Ochiai, Ohmae, Mori, and
Kobayashi was used in the enzymatic polymerization of the substrate monomer. It was found
from previous studies that ovine testicular HAase (OTH) can be used for successful enzymatic
polymerization of similar monomers. This enzymatic polymerization leads to a HA derivative
having an approximate Mn (number average molecular weight) of 9100 (containing about 44
saccharides) and approximate Mw (weight average molecular weight) of 19,500 after purification
which is much larger than the typical HA polymer with a Mn of 6000 and Mw of around 14,000.35
The time required for this reaction to completely consume the monomer is approximately 48 h.
The enzymatic polymerization effect can be seen in Figure VII.c below.
Enzymatic Polymerization Procedure
A solution of substrate monomer is put in a carbonate buffer and incubated with OTH.
After approximately 48 h, the reaction mixture is heated at around 90 °C for 5 min to inactivate
the enzyme. The resulting structure is the hyaluronic derivative.
The new hyaluronic derivative that will be used in the formation of our solution was
created with an addition of a new functional group which is represented by R in Figure VII.c.
Figure VII.c – Enzymatic polymerization of HA

19
The new functional group replaced the methyl group that is found in synthetic HA. The
synthesis for this hyaluronic derivative came from Ochiai, Ohmae, Mori, and Kobyashi.35 This
new functional group that was introduced was a 2-vinyl. The formation of this 2-vinyl came
from steps [(vi)-(viii)] that were shown earlier. The reason we chose to use the hyaluronic
derivative containing 2-vinyl was because of the 2-vinyl’s ability to be used to form crosslinks
with several different chemicals. The use of the 2-vinyl also gave the new hyaluronic derivative
the ability to react with ammonium peroxydisulfate, which forms a strong crosslink. This
crosslinking can be seen in Figure VII.d. The new crosslinking introduced in our material is a
chemical crosslink formed through the reaction of ammonium peroxydisulfate and the vinyl
group of our polymer. The reason for using ammonium peroxydisulfate as the crosslinking
reagent is because ammonium peroxydisulfate contains disulfide bonds which have been found
to have the ability to stabilize a structure against denaturation.25 Another reason for the use of
ammonium peroxydisulfate is because it has been shown to be non-toxic or biocompatible in the
human body which means that it is more likely to make our final product be safe in the human
body and easier to get through the FDA approval process.25 One more reason for using
peroxydisulfate for our crosslinker is because it has been found to be a very efficient system,
which gives rapid formation of a gel.38 As stated earlier this gel formation is important because
of the properties associated with a gel. The gel provides a structure that is less subseptible to
chemical denaturation and has the ability to mimic tissue in the human body.43 From looking at
previous experiments done by other scientists on peroxydisulfate the time required for the
crosslinking to occur should be around 400 seconds using a concentration of .05 mol/L for
ammonium peroxydisulfate. This time will vary with concentration increasing with decreasing
concentrations of ammonium peroxydisulfate.36 The reason for using an ammonium
peroxydisulfate concentration of .05 mol/L as a basis for the time required for crosslinking is

20
because after calculating the required concentration of peroxydisulfate in relation to the
concentration of the new HA derivative to get the desired percent crosslinking of the final
product, it was found that a concentration of approximately .055 mol/L of ammonium
peroxydisulfate is required for a concentration of .28 mol/L of the polymerized HA derivative in
water. The percent of crosslinking associated with the new material will be 15% with this
concentration of ammonium peroxydisulfate assuming that the concentration of the HA polymer
is kept constant. This percentage of crosslinking is associated with the number of crosslinks.
For our material we will have 3 crosslinks for every 20 substrate monomers or 24 crosslinks for
our molecule. The reason for the low percent of crosslinking is because if crosslinking becomes
too high the structure will become stiff and inflexible.
Crosslinking Procedure
The HA derivative with the addition of ammonium peroxydisulfate under oxidizing conditions
such as an air interface leads to a spontaneous chemical crosslinking reaction resulting in the
formation of our new HA derivative final product.
This crosslinking introduced is done through a process know as free radical
polymerization which is also more commonly known as a method of chemical crosslinking. The
importance of this chemical crosslink is that it decreases the molecular freedom of the material.
Figure VII.d – Free radical crosslinking of hyaluronic acid units

21
This means that the chemical has less freedom to react with other substances that may be present
in the surrounding environment such as the knee’s synovial fluid. The reduction of molecular
freedom helps to stabilize the material by reducing the chance of degradation through bond
breaking from occurring. The crosslinking also helps to shield the active sites from enzymatic
degradation. Some of the changes that can accompany a chemical crosslink include a decrease in
solubility. Also a chemically crosslinked polymer in the presence of a solvent tends to swell as
the solvent penetrates the network that was shown earlier. This in turn creates a hydrogel
because of the solvent for this new material being water.
The viscosity of the substrate monomer should be fairly close to the current viscosity of
synthetic HA monomer due to the fact that the addition of a 2-vinyl is a relatively small change
in the base structure of hyaluronan. The significant increase in viscosity will be attributed to the
crosslinking and polymerization of hyaluronan. This is the reason that polymerization and
crosslinking are so important for the new material. From previous studies it has been found that
crosslinking a material to form a gel can lead to an increase in the zero shear viscosity of the
base material by about 80 times the original value.29 For the normal HA polymer the zero shear
viscosity has been found to be 0.2 Pa·s @ 37oC.29 By relating the idea of the zero shear
viscosity being approximately 80 times the original polymer’s viscosity after crosslinking, it
resulted in the new HA derived polymer’s zero shear viscosity after sterilization being around 16
Pa·s @ 37oC which is comparable to our competitor’s treatment viscosities. This is important
because it has been found through studies that the viscosity of current treatments appear to be
adequate. This viscosity has also been tested using the lubrication theory to find whether or not
this value would be adequate. The lubrication theory is explained later on. The main problem
with current treatments has been the treatment life. Current treatments have problems with
degradation which through the use of ammonium peroxydisulfate will be fixed. Ammonium

22
peroxydisulfate has been found to have the ability to protect a structure against denaturation and
degradation.25 This benefits the stability of the hydrogel that is formed through crosslinking.
Basic steps for final material on a lab basis
The construction of the final material will be performed in a step manner as follows:
1. Basic construction of the substrate monomer as described earlier.
2. Polymerization of the monomer using OTH to create the HA derivative.
3. The polymer will be diluted in a pure water solvent for remaining steps and final
injection.
4. Crosslinking the HA derivative using ammonium peroxydisulfate with a molar
concentration relationship of 20:100 (disulfate / HA monomer). The concentration of
our polymerized HA derivative should be around 2.8*10-4 mol/ml and our concentration
of ammonium peroxydisulfate should be around 5.5*10-5 mol/ml.
5. Repeat crosslinking step 3, 150 times. This will provide a large molecule connected
through a crosslinking network. This will also result in a structure with an approximate
weight of 3 million Daltons which is comparable in size to current treatments.
6. The final step in the creation of this new material is sterilization which consists of the
removal of remaining unreacted peroxydisulfate along with any by products before in
vivo application.
The final product our newly described solution will be an intra-articular injection also
known as viscosupplementation for patients with osteoarthritis. The reason that our treatment
will be done in this manner is because increases the likely hood of being approved by the FDA.
It is more likely to be approved because there are already intra-articular injections for
osteoarthritis treatment approved and on the market.31 Another reason for using this method of

23
injection is that the location that the gel is placed in the body is easier to control through intra-
articular injection.
Advantages
The reason that this new crosslinking method is important is because of the disulfates’
ability to stabilize a structure against denaturation and because it gives our solution a viscosity
that is desired for its use.25 This stabilization from denaturation will help keep the new HA
derivative from degrading. This will in turn lead to a longer life span for the HA that is being
injected and in turn lead to fewer treatments being required for the patients.
VII. Lubrication Theory
To assess the effect HYAL-VYNE will have on the lubrication of the knee joint,
lubrication theory was studied to predict the minimum film thickness. The minimum film
thickness in any system is the distance between two surfaces separated by a lubricating substance
when a compressive force is applied. This will be calculated for the two articular surfaces of the
knee with our new hydrogel as the lubricant to ensure that the increased viscosity will not create
too much separation and not restrict the patient’s movement.
Several types of lubrication exist, so the first step is to determine which applies to the
synovial joint. The main types that could possibly apply to our system are hydrodynamic,
boundary, and elastohydrodynamic. Hydrodynamic lubrication was first used to explain the low
friction of human joints.47 It is based on the pressure forces formed between two surfaces in the
wedge configuration that occurs with cylindrical bearings. The idea is that the moving surface
will carry with it a fluid layer at the same velocity, and that this velocity will diffuse through the
rest of the fluid. Therefore the fluid entering the gap between the wedge and the moving surface
must partially move backward causing a pressure that supports the load. However, this model
has been found to work best for high speeds and low loads while the joint is characterized by low

24
speeds and high loads. Although it is now widely accepted that hydrodynamic lubrication does
not apply for biological joints, it was the only system available for nearly 30 years.
Another attempt at classifying the lubrication of the knee joint was boundary
lubrication.47 This type is different from hydrodynamic lubrication as it depends mostly on the
quality of the moving surfaces and the lubricating fluid. However, the viscosity of the lubricant
and geometry of the system are unimportant. Boundary lubrication can explain the low
coefficient of friction encountered in the synovial joint as motion begins, but it does not take into
consideration non-Newtonian behavior that exists in natural synovial fluid as well as the new
hydrogel.
To better characterize systems that include a solid surface covered with an elastic
material, elastohydrodynamic lubrication was developed. This type applies to systems of solid
surfaces of low geometric conformity that undergo elastic deformation and have a minimum film
thickness on the order of 1 µm.48 Within elastohydrodynamic lubrication are 4 regimes that can
be used to simplify the solution of the complex equations: (1) rigid-isoviscous, (2) rigid-
piezoviscous, (3) elastic-isoviscous, and (4) elastic-piezoviscous. Because the pressures incurred
in the knee joint are not high enough to cause a non-uniform viscosity in the synovial space, our
system falls into the elastic-isoviscous regime. The geometry of the knee joint can be estimated
as two convex bodies that would touch at a point if allowed. For point contact in the elastic-
isoviscous regime, the minimum film thickness can be determined by first calculating the film
thickness parameter, gHmin,
[ ]κ31.067.0min 85.0170.8 −−= egg EH
where gE is the elasticity parameter, and κ is the ellipticity, both defined below.
2/1U
WgE = (VII.1)

25
636.0
0339.1
=
x
y
R
Rκ (VII.2)
In the above equations, W is the load parameter, U is the velocity parameter, and Rx and Ry are
the radii of the ellipse in the x and y directions, respectively. We have estimated the ends of the
femur and tibia to be spheres with 20 mm radius. The load and velocity parameters are defined as
'2ER
wW
x
= (VII.3)
'
0
ER
VU
x
µ= (VII.4)
where w is the compressive load, E’ is the effective elasticity modulus, µ0 is the viscosity of the
lubricant, and V is the velocity parameter. E’ and V are defined as
−+
−=
2
22
1
21 11
2
1'
EEE
νν (VII.5)
( )22 ν+= uV (VII.6)
where E1 and E2 are Young’s modulus for each surface, v1 and v2 are the Poisson ratios for each
surface, and u is the speed of the moving surface. Based on typical values for the human knee
and articular cartilage, the parameters used in these equations are as follows:
Poisson’s ratio: v1 = v2 = 0.45
Young’s modulus: E1 = E2 = 12 MPa
Speed: u = 0.03 m/s
Radius: Rx = 0.002 m
Load: w = 3.26 MPa
The only parameter that was actually based on our new hydrogel was the viscosity. We used 16
Pa·s for these calculations as it was found from similar studies to exist under conditions such as

26
walking. For this reason, the compressive load was chosen to be 3.26 MPa which is typical of an
adult male during walking. With all the parameters defined, the minimum film parameter is
( )
( ) ( )
( )( )( )( )
( ) ( )[ ] 50339.131.07min
72.1
7
6
7
62
6
22
22
1050.685.011086.77.8
1086.70245.0
1023.1
0245.0m 002.0Pa 100665.0
2034.0sPa 16
1023.1m100665.0m 002.0
Pa 1026.3
2034.045.003.0
MPa 0665.012
45.01
12
45.01
2
1'
×=−×=
×=×=
=×
⋅=
×=×
×=
=+=
=
−+−=
−eg
g
U
W
V
E
H
E
The film thickness parameter is related to the actual film thickness by
x
H
RHh
HU
Wg
⋅=
=
(VII.7, 8)
where H is another film thickness parameter, and h is the film thickness. Therefore, the
minimum film thickness for our new gel in the synovial joint is
( )
( )( ) mh
H
µ6.2106.2002.00013.0
0013.01023.1
0245.01050.6
6
7
5
=×==
=
××=
−
If these same calculations are done for natural synovial fluid using a viscosity of 10 Pa·s,
which is typical for walking, a minimum film thickness of 1.9 µm is obtained. This indicates

27
that the increased viscosity of HYAL-VYNE will not affect the minimum film thickness
significantly and the range of motion should be retained.
VIII. FDA Approval Process
As was mentioned in the objective of this project, one of the requirements, and possibly
the most crucial to the survival of the project, is the approval of the Food and Drug
Administration (FDA) for the new product HYAL-VYNE. This process takes extensive amounts
of time and money, with risk of complete failure. The average cost of the entire FDA approval
process, from pre-clinical testing to actual review by the FDA to post-approval costs for a new
drug is $800-900 million as reported in 2003 taking anywhere between 4 and 12 years23. Before
beginning, our new gel of crosslinked hyaluronic acid derivative must be classified as either a
drug or a device. According to the Food, Drug, and Cosmetic Act, a drug is an article
“…intended for use in the diagnosis, cure, mitigation, treatment, or prevention of disease in man or other animals; and…articles (other than food) intended to affect the structure or any function of the body of man or other animals…,”22
while a device is defined as
“…an instrument, apparatus, implement, machine, contrivance, implant, in vitro reagent, or other similar or related article, including any component, part, or accessory, which is… intended for use in the diagnosis of disease or other conditions, or in the cure, mitigation, treatment, or prevention of disease …and which does not achieve its primary intended purposes through chemical action within or on the body of man or other animals and which is not dependent upon being metabolized for the achievement of its primary intended purposes.”22
Based on these definitions, as well as on the classification of the similar products Synvisc and
Hyalgan49, the intra-articular hydrogel falls under the definition of a medical device because of
its intent to treat and slow the progression of a disease (osteoarthritis), and because it does not
achieve this primary purpose through metabolic processing.
The branch of the FDA that deals with medical devices is the Center for Devices and
Radiological Health (CDRH), which places devices into three categories based on the control

28
required to ensure safety and effectiveness of the device. A description of each classification as
provided by the CDRH follows.
Class I – General Controls:
This class is subject to the least stringent control as these devices pose minimal
risk to consumers and are most often simpler in design than those in Class II and
III. They are subject to the general controls which include establishment
registration, medical device listing, and labeling. A premarket notification must
be filed before marketing. Examples in this class include elastic bandages, latex
gloves, and hand-held surgical tools.
Class II – Special Controls:
This class is also subject to the general controls described for Class I devices but
these regulations alone may not be sufficient to ensure safety and effectiveness
although methods to do so are already in existence. These devices may also be
subject to special controls such as special labeling, mandatory performance
standards, and postmarket surveillance. Examples in this class include powered
wheelchairs and surgical drapes.
Class III – Premarket Approval:
This class is subject to the most stringent control as the general and special
controls alone cannot provide sufficient information to ensure the safety and
effectiveness of these devices. These devices often have the purpose of
supporting or sustaining human life and/or preventing impairment of health while
posing a risk of injury or illness. All Class III devices require a premarket
approval. Some examples in this class are replacement heart valves, silicon breast
implants, and implanted cerebella stimulators.

29
Because OsteoGel does pose serious risks such as localized pain, infection, and rejection by the
body, it will fall under the Class III medical devices and will require premarket approval.
For FDA approval of Class III devices, the premarket approval (PMA) is used to review
the extensive non-clinical and clinical data to assure that the device is safe and effective and will
ultimately determine approval for marketing. The FDA is officially given 180 days to review a
submitted PMA, but this often takes longer. If the PMA is denied, the applicant – the person,
company, or institution seeking approval – has 30 days to petition the decision in order to be
reconsidered. Because approval is based on the content provided in the PMA, it is vital to
provide adequate technical data in addition to thorough background information and device
purpose and description. Although not the only deciding factor, the technical section must
provide the data necessary for the FDA to make their decision. This is normally divided into two
sections: non-clinical laboratory studies and clinical investigations. The non-clinical section
should contain information on microbiology, toxicology, immunology, biocompatibility, stress,
wear, and other laboratory or animal tests, while the clinical investigations section should
include study protocols, safety and effectiveness data, adverse reactions, complications
encountered, device failures, patient information and complaints, data tables, and statistical
analyses50
There are two types of PMA that can be submitted, traditional and modular. With a
traditional PMA all necessary data are first collected then presented all at once to be reviewed for
approval. This type of PMA is most often used for devices that have already undergone clinical
testing and/or have previously been approved by a medical regulation organization of another
country. With a modular PMA, the necessary contents are broken down into specific
components, or modules, where the research group completes one subset of experiments, submits
the results, and waits for approval while concurrently working on the next module. This type of

30
submission is best for products that are still in the early stages of clinical trials. While the
modular PMA may take more total review time than the traditional PMA, we will follow the
modular type for this project since we are in the still in the pre-clinical stage. Also to avoid the
risk of spending extensive amounts of time and money to complete the entire testing process
before submitting for review, we see it best to ensure approval after smaller portions are
complete so that in the case of FDA denial, only that particular module will need to be revised
and repeated.
The modular premarket approval will be divided into three discrete sections. The FDA
does not provide an actual form to follow for each module, but instead requires a PMA shell to
first be submitted. The PMA shell provides an outline of the testing that will be performed in
each module and gives a time line of approximately when each module will be completed. A
team from the FDA will review the PMA shell and provide assistance to develop a customized
plan to fit the particular device and situation. We have designed each module in attempt to best
manage the time and scope involved for each one; this is summarized in our PMA shell shown in
Table VIII.a
Table VIII.a - PMA Shell
HYAL-VYNE
Module Number Contents Time to Complete
1
Nonclinical Laboratory Studies: • Physical and Chemical Property Tests • Degradation Tests • Toxicity Tests
3 Years
2
Nonclinical Laboratory Studies: • Animal Testing • Sterilization and Packaging • Injection Procedure
3 Years
3
Clinical Studies: • Human Patient Testing • Physician Instructions • Patient Instructions
5 Years

31
Because of the numerous possible scenarios that could occur during these experiments,
we have created a model based on the work of Kim, Shreve, and Yankovich for a relatively
similar proposal.50 Before beginning the actual laboratory testing for FDA approval, several
choices must be made. Most important are the number of PhDs and lab technicians that will be
employed to conduct the experiments as well as the number of experiments they will perform.
This is an important decision because with a PhD salary of $66,000/year and a lab technician
salary of $26,000/year, this will account for a large portion of project expenses. The number of
each type of experiment to be performed is important because while the more experiments that
are run the more consistent the results will be, at the same time the greater the total cost and time
spent will be. Therefore, three different combinations of employees will be considered – 1 PhD
and 10 lab techs, 1 PhD and 5 lab techs, 1 PhD and 2 lab techs – along with three selections for
the number of experiments – 100, 85, 50 – that will be performed to prove consistency of results.
Figure VIII.a shows a decision tree for the number of employees, number of experiments, and
the amount of time required based on these decisions.

32
Stage One Variables
Determine Number of workers
1 PhD10 Lab Technicians
$415,000
1 PhD5 Lab Technicians
$245,000
1 PhD2 Lab Technicians
$143,000
Determine Number of Experiments
Determine Number of Experiments
100 Experiments$170,000100 Days
85 Experiments$150,00090 Days
50 Experiments$100,00065 Days
Determine Number of Experiments
100 Experiments$170,000105 Days
85 Experiments$150,00095 Days
50 Experiments$100,00070 Days
100 Experiments$170,000150 Days
85 Experiments$150,000140 Days
50 Experiments$100,000120 Days
Begin Pre-FDA Experimentation
The specific tasks included in each module along with probabilities assigned for success
and for failure due to various scenarios are presented in the following sections so that later a risk
analysis for the entire FDA approval process can be performed. The probabilities that will be
seen in each module are assigned based on anticipated difficulty of the particular experiment,
predictability of results, and most importantly on the number of experiments performed.
Probabilities are given for each set of number of experiments – 100, 85, 50 – with the likelihood
of success decreasing with decreasing number of experiments; the fewer experiments that are
performed, the larger the deviation of results, and therefore the greater the possibility of rejection
Figure VIII.a – First stage decision: Number of emp loyees and experiments

33
by the FDA. It is important to note that the number of employees does not affect the success or
failure rates. This decision only determines the amount of time and money required for each set
of experiments.
Module 1
Module 1 will consist of extensive laboratory tests to determine material properties such
as compressive and tensile strength, viscosity, elasticity, coefficient of friction, and molecular
weight of HYAL-VYNE as well as degradation rates and toxicity to cells. These experiments
are summarized below.
• Polymer Synthesis
The synthesis procedure for the novel HA derivative has already been described
in detail (see section VI) and therefore will not be repeated here. However, after the
enzymatic polymerization of the substrate monomer, it is important to know the actual
degree of modification of the N-acetyl reactive site with the newly introduced 2-vinyl
functional group. This will be quantified using H-NMR spectroscopy with the Varian
Inova-500 spectrophotometer. Because the hydrogens of the 2-vinyl group will resonate
at a different frequency than those of the methyl group of a non-substituted HA
monomer, two different peaks will be produced on the H-NMR spectrum. To determine
the degree of modification, the relative integrations of the 2-vinyl and methyl protons will
be analyzed.
It is unlikely the FDA would deny the proposal based on the polymer synthesis,
but these experiments will provide data to prove consistency in the product produced
from the devised steps. These experiments are also helpful in ruling out the possibility of
an improperly modified polymer or contaminants in the case of failure in other steps.

34
The H-NMR experiments will take a minimal amount of time since only a very
small sample is required for analysis, which can be performed at the same time as other
experiments.
• Degree of Crosslinking
Although we have previously predicted a theoretical degree of crosslinking of the
new HA hydrogel, the actual degree of crosslinking will be determined by a method
similar to that described by Miyamoto et al.51 1 g of the gel will be dissolved in 1.0 ml of
1.0 M sodium hydroxide and shaken on an orbital shaker for at least 1 hour. Next 1.1 ml
of 1.0 M HCl will be added to the solution, followed by extraction of the HA sample with
ethyl acetate. Then solvent will be evaporated. The sample will then be analyzed using
high performance liquid chromatography (HPLC) equipped with an ODS column and a
UV detector from Toshoh Corp.
• Force Profiles
A Surface Forces Apparatus (SFA) Mark III will be used with a geometry similar
to that of the human knee to create a force profile using our new HA gel as the lubricant.
The SFA Mark III consists of two crossed cylinder plates separated by a gap of distance
D in which the gel is placed. A normal force is applied to the upper plate while the lower
plate is connected to a spring, and the induced deflection is measured to determine the
force between the two plates for various gap distances. This information will be used to
assure that the gel will be able to hold loads typical of the knee joint, which can reach a
maximum of 473 psi during walking, or up to 50% higher in extreme motions such as
running or stair climbing.47 Because the gap distances in the synovial joint can vary from
50 to <0.8 µm, D will be varied from 100 µm to 0.01 µm to develop a force profile over
the entire range of distances experienced in the knee.

35
• Viscosity Measurements
Because we are attempting to provide improved viscoelastic properties over
existing synovial fluid, viscosity measurements will also be taken using the SFA Mark III
in order to ensure that the viscosity of HYAL-VYNE is in fact equal to or greater than
that of natural synovial fluid, which has a viscosity of 300 cP or more depending on
shear. This is done by applying a sinusoidal normal motion of specified amplitude and
frequency to the upper plate of the apparatus. Normal walking cycles have a frequency
of approximately 1 Hz, so our gel will be tested for a frequency range of 0.01 Hz (to
simulate rest) to 10 Hz (significantly faster than normal running). The viscosity is then
calculated for these conditions by
2/12
221
12)(
−
=A
A
vR
KDD o
πη
where η(D) is the viscosity at gap distance D, K is the spring constant, R is the radius of
the curved plate of the apparatus, v is the frequency, Ao is the applied amplitude, and A is
the amplitude of the vibrating surface. To best mimic the human knee, the radius R of
the plate will be 25 mm.
• Hydrogel Degradation
To analyze the rate of degradation of the new crosslinked HA hydrogel, the gel
will be subjected to enzymatic degradation experiments as suggested by Leach et al.52 To
test the enzymatic degradation, the hydrogel will be incubated at 37°C in solutions of
various concentrations of the enzyme hyaluronidase (2.6 µg/ml, 5 µg/ml, 50 µg/ml, and
500 µg/ml in citrate buffer) to create a profile of percent mass degraded relative to
concentration of enzyme. Hyaluronidase (HAase) is the enzyme secreted naturally in the
synovial fluid and appears at an average concentration of 2.6 µg/ml and has an active life

36
of approximately 5 hours. First, the gel samples will be placed in 24-well plates and
soaked in citrate buffer overnight to reach their equilibrium swelling. The next day, the
gels will be removed, dried of excess buffer with filter paper, and weighed to determine
their initial mass. Then 0.5 ml of bovine testicular hyaluronidase will be added to the
samples. The well plates will be gently agitated on an orbital shaker at 37°C. After
every hour since HAase was added, the gel will be removed from the well, excess
enzyme solution blotted away, the gel reweighed, and fresh HAase solution added. This
will be done for 48 hours for each enzyme concentration in triplicate to obtain consistent
results. Three control samples of the gel in citrate buffer only and three samples of
synthetic HA (unmodified, no crosslinks) in the each of the concentrations of HAase will
also be included for comparison.
Because of the functional group modification and more importantly the crosslinks
that are introduced to hyaluronic acid, we anticipate a significantly reduced degradation
rate; however, if the FDA yields this as a reason for denial of the PMA, we will reassess
the chosen modification and crosslinking densities. The degree of modification with 2-
vinyl can be altered by changing the concentrations and reaction times from steps vi, vii,
and viii in the “bottom-up” synthesis. The degree of crosslinking can be changed by
changing the concentration of ammonium peroxydisulfate and/or the number of times the
crosslinking step is repeated. For this reason, there is a relatively high probability that
failure will occur due to rapid degradation times; however, because this problem can be
readdressed easily, the probability of this being a reason for failure in later modules is
significantly lessened.
• Cytotoxicity Tests

37
To test the toxicity at the cellular level, we will use the elution method which is
widely used for medical device testing.53 L929 mouse fibroblast cells will be grown in
cell culture medium to produce a monolayer of cells attached to the bottom of culture
flasks. The new hydrogel will be placed in cell culture medium and incubated at 37°C
for 24 hours. The culture medium from the gel samples containing any extractable
fragments will then replace the culture medium of the cells. Each day after exposure, the
cells will be monitored under a microscope to check for cell death (dead cells will detach
from the flask bottom) and changes in configuration such as cell size and appearance for
1 week.
If these tests indicate significant toxicity due to the HA gel, we will first run the
experiment again to try to rule out the possibility of random contamination. If the
problem persists, we will then test for impurities such as reagents remaining from the
synthesis steps by using H-NMR spectroscopy as discussed earlier.
These tests will take approximately 5 months to complete since the cells will need
to be cultured for 7 days prior to and 3 days after exposure and only 5 flasks will be
tested at one time so that in the case of contamination, only this small number will need
to be retested.
Figure VIII.b shows the possible pathways that could occur after Module 1 is submitted
to the FDA. The probability of each path of the module is given for each number of
experiments; the probability for success is higher when more experiments are performed.
However, because a greater number of experiments also corresponds to higher costs and more
time, there must be an optimum that will produce the minimum net present cost. Microsoft
Excel was used to generate values for this for each possible pathway through the PMA modules
and will be discussed after the modules are presented.

38
Module 1 Testing$500,0001 year
Module 2
Module 1 testing$500,0003 years
Abandon Project
Failure due to polymer synthesis
4%, 5%, 7%
Failure due to mechanical properties
9%, 12%, 15%
Approval Granted
60%, 45%, 30%
Approval Granted
90%, 85%, 75%
Failure due to polymer synthesis
2%, 3%, 5%
Failure due to purification problems
9%, 11%, 15%
Change polymer synthesis procedure$15,0001 months
Change crosslinking procedure$60,0003 month
Change purification procedure$12,0001 months
Reapply for Module 1
Failure due to crosslinking reaction
3%, 6%, 9%
Failure due to degradation
5%, 6%, 11%
Abandon Project Abandon Project
Failure due to degradation
12%,15%, 21%
Failure due to poor cell survival
6%, 8%, 12%
Add additional crosslinks$40,0002 months
Abandon Project
Module 2
Module 2
Module 2 (see Figure VIII.c on the next page) will consist of animal testing where the
new crosslinked hyaluronic acid derivative will administered to guinea pigs, rabbits, pigs, and
dogs. The tests will be conducted in order of increasing biological complexity starting with the
smallest animals, and once satisfactory results are obtained, the next larger animal will be used,
and so on, concluding with dogs, which should have the greatest similarity to humans. The
Figure VIII.b – Module 1: Laboratory Testing

39
experiments to be run for this section are outlined below followed by the pathways for Module 2
with probabilities assigned for anticipated failures due to biocompatibility, retention time,
degradation, and injection procedure.
• Biocompatibility and Biodegradation Tests
To evaluate the biocompatibility and biodegradation of the crosslinked HA
derivative in animal models, the gel will be injected subcutaneously into guinea pigs
similar to the method described by Miyamoto et al.51 A group of 40 6-week old guinea
pigs (20 male, 20 female; Elm Hill Breeding Labs, Chelmsford, MA) will be given
sodium pentobarbital for general anesthesia, then a large area of dorsal skin will be
shaved. The injections will be administered in 0.2 ml samples through a 25-gauge
needle. The guinea pigs will be divided into two groups of 20 (equal gender in each
group). Group 1 will receive 3 injections at separate locations with samples of the new
gel of crosslink densities 15%, 20%, and 25%. Group 2 will serve as a sort of control
group each receiving samples of noncrosslinked HA derivative, unmodified HA, saline,
and competitor product Hylan G-F 20. Each day the injection locations will be observed,
looking for signs of bioincompatibility such as erythema (redness of the skin due to
inflammation), edema (swelling due to fluid accumulation), and vesiculation (blistering),
as well as signs of degradation seen as a reduction in initial protrusion of skin from the
injection material. At the end of days 3, 7, 14, 21, and 28, 4 animals from each group (2
males, 2 females) will be sacrificed and samples of their injection sites removed. These
specimens will be placed in 10% neutral buffered formalin, paraffin embedded, and
sectioned. Part of these sections will be stained with hematoxylin and eosin while the
others will be reviewed histologically. The hematoxylin and eosin stains allow for
microscopic examination to score the degree of inflammation based on the number of

40
cells accumulated in the skin sample. Histological review of the sections will show the
dispersion of the gel into surrounding tissue, indicating the degree of degradation during
the specific time period.
If the FDA determines that HYAL-VYNE is not biocompatible based on the
results obtained in Module 2, the project will be abandoned due to the high probability
that if the gel is non-biocompatible in animals, it will also be so in humans. On the other
hand, if the FDA declines approval due to rapid degradation, we will reconsider using a
higher crosslinking density to introduce more sulfate groups. However, there is not much
room left for change in this area because as more crosslinks are added to the molecule,
the more stiff the gel becomes, possibly becoming too stiff and losing its functionality.
Therefore, we will also consider changing the crosslinker used, ammonium
peroxydisulfate, to another sulfate-containing crosslinking agent in attempt to keep the
sulfate’s stability against degradation.
Since the longest the guinea pigs will be used in this test is 28 days, it is estimated
that these biocompatibility and biodegradation tests will take 30 days to complete with an
approximate cost of $6,000.
• Immunogenicity Test
To determine whether the injected gel causes an immunogenic response, i.e. the
production of antibodies to fight the foreign substance, the method of Miyamoto et al will
be used.52 A tissue sample from the guinea pigs from the biocompatibility tests that were
sacrificed after 28 days will be tested for the presence of antibodies by passive cutaneous
anaphylaxis (PCA) analysis. This will detect any biologically active antibodies,
especially immunoglobulin G1 and immunoglobulin E, by adding a dye solution to the
test serum. If a blue spot is observed, the test is positive for antibodies. Each of the

41
injection areas on the 8 animals from Day 28 will be tested along with 1 male and 1
female that had not be subjected to any injections.
If consistent positive results are obtained from the PCA analysis, the project will
be abandoned due to the high probability that if the gel produces an immunogenic
response in animals, it will do so also in humans.
This portion of the Module 2 testing is estimated to take 1 day at a cost of $400.
• Effectiveness
The effectiveness of the new hydrogel will be tested on rabbits, pigs, and dogs.
The rabbits will first be administered the injection by a veterinary surgeon. After each
animal receives the injection, they will be monitored for signs of change in mobility
relative to their actions prior to treatment. Because we want to know how long the
effectiveness of the treatment lasts, we will monitor some of the animals for as long as 6
months. If it appears that the animals are still in pain and do not increase their activity,
the FDA may deny request for approval. In this case we may have to reevaluate the
crosslinking density because the gel likely is not being retained in the synovial cavity. If
there appears to be no improvement after injection, another possible problem could lie
within the injection procedure. The surgeon may have not gotten the hydrogel into the
proper space, therefore allowing the gel to disperse throughout the body. In this case we
will need to examine other possible methods of administration.
This part of Module 2 will take the most amount of time, possibly up to 3 years in
order to get sufficient data on the effectiveness and treatment life of the new injection.

42
Module 2 Testing$500,0003 years
Module 3
Module 2 testing$500,0002 years
Failure due to lack of retention
12%, 15%, 19%
Failure due to biocompatibility issues
4%, 7%, 8%
Approval Granted
65%, 50%, 38%
Approval Granted
70%, 63%, 45%
Failure due to injection procedure
7%, 9%, 11%
Reevaluate molecular size
$40,0002 month
Additional purification, sterilization$15,0001 months
Test new injection procedures$50,0002 months
Reapply for Module 2
Failure due to in vivotoxicity
5%, 8%, 9%
Failure due to degradation
7%, 11%, 15%
Abandon Project
Alter polymer formulation or M.W.
to find optimal$30,0002 months
Abandon Project
Failure due to biocompatibility
5%, 7%, 12%
Failure due to in vivotoxicity
5%, 7%, 12%
Failure due to degradation
10%, 12%, 16%
Abandon Project Abandon Project
Failure due to injection procedure
10%, 11%, 15%
Purchase advanced equipment$200,0001 month
Module 3
Reapply for Module 2
Module 2 testing$500,0001 year
Approval Granted
90%, 80%, 60%
Failure due to surgical procedure
10%, 20%, 40%
Module 3 Abandon Project
Figure VIII.c - Module 2: Animal Testing

43
Module 3
The final stage before approval is granted consists of extensive human clinical trials. In
this stage people suffering from osteoarthritis will be administered the treatment or placebo to
determine the efficacy and safety of the treatment. Again, each scenario has been assigned a
probability so that a complete analysis of the module pathway and the costs associated with each
path can be generated (Figure VIII.d).
• Safety
HYAL-VYNE will be injected into the synovial cavity of the knee joint of 100
human patients. On days 1, 7, 21, and 28 (where day 0 = day of injection) the patients
will be examined to check for signs of infection, excessive swelling and tenderness, and
fever. Swelling and pain near the injection site is normal for similar products and will
likely occur with HYAL-VYNE as well, but this should clear up within about a week and
can be treated with anti-inflammatory drugs. If inflammation persists after the second
week in several patients, the FDA may find this as reason to deny approval, and the
project will have to be abandoned. Fever is often in indication of infection, so patients
experiencing fever will be treated with antibiotics. If the fever subsides, there likely was
an infection present. Again, if this occurs in several patients, the FDA will likely find
this as reason to deny approval, and the project will have to be abandoned. Patients will
also be asked if any other problems have been noticed since administration such as
abdominal pain, nausea, diarrhea, headaches, body aches, fatigue, or dizziness. Since
hyaluronic acid is created naturally in the body and because it should not be metabolized,
we do not anticipate these side effects to arise but obviously need to note them if they do.
• Effectiveness

44
Before receiving the injection, each patient will be asked to rate their current pain
and ability to perform certain activities such as walking, stair-climbing, bending,
standing, etc. Once the patients have been administered the new HA injection, they will
be asked to return on days 1, 7, 21, and 28 to examine the effectiveness of the gel at
relieving their symptoms of osteoarthritis and returning their mobility. They will rate
their pain on a scale of 1-10, ten being the most painful. The patients will also be asked
to rate their range of motion, that is, how much more or less they are able to extend and
flex the knee as well and their ability to apply weight during normal activities such as
those listed above. These will also be rated on a scale of 1-10, ten being not able to move
at all.
If several patients do not experience significant pain relief and return of mobility,
the FDA will possibly deny approval. If this is the case, it is likely due to lack of
retention after injection and we will have to reassess our decisions for crosslinking
density and molecular weight and then reapply for Module 3. It is fairly unlikely that this
will happen because of the numerous tests already completed in Module 1 and 2.

45
Module 3 Testing$4,000,0005 years
Medical Market
Module 3 testing$4,000,0004 years
Abandon Project
Failure due to low retention time
15%, 20%, 22%
Failure due to rapid degradation
20%, 25%, 33%
Approval Granted
55%, 40%, 30%
Approval Granted
70%, 60%, 35%
Failure due to damaged surrounding tissue
5%, 9%, 15%
Failure due to inflammation of
surrounding tissue
10%, 15%, 15%
Change molecular size, crosslink
density$300,0006 months
Increase functional group substitution, crosslink density
$500,0008 months
Treat with anti-inflammatory medication$300,0006 months
Reapply for Module 3
Failure due to rapid degradation
13%, 16%, 25%
Increase functional group substitution,
crosslink density$50,0001 month
Failure due to lack of benefit over current
treatments
10%, 18%, 28%
Change polymer constiuent
concentrations$750,0006 months
Improve degradative properties of polymer
$500,0001 year
Reapply Module 3 and Testing$4,000,0002 years
Failure
10%, 20%, 30%
Abandon Project
Failure due to low retention time
12%, 15%, 25%
Change molecular size, crosslink
density $500,0001 year
Reapply for Module 3
Module 3 testing$4,000,0003 years
Approval Granted
80%, 70%, 55%
Failure due to poor efficacy
10%, 12%, 17%
Approval Granted
90%, 80%, 70%
Medical Market
Medical Market
Medical Market
Figure VIII.d - Module 3: Clinical Trials

46
IX. FDA Risk Analysis
Before the FDA process can be completed first stage decisions must be made such as
number of employees and number of experiments. These variables were important because they
were needed to determine the time and money that would be required for the FDA process to be
completed. To decide the best combination of workers and experiments, a risk analysis was
done. The risk was based upon the possibility of failure or success of the project with respect to
the net present value (NPV) of the project. There were 9 possible scenarios associated with this
risk analysis. The possible scenarios can be seen in Table IX.a with the number in each center
box being associated with the number of days required for completion of the given number of
experiments with the combination of workers. The days required were estimated by looking at
the time it takes for each experiment to run and the time that can be cut down by each worker.
100 Experiments 85 Experiments 50 Experiments
10 workers 100 90 65
5 workers 105 95 70
2 workers 150 140 120
The overall probabilities of success or failure were determined by looking at each module
and the probabilities associated with each step in the module occurring. In our case there were
more than 1800 pathways in which success or failure could occur. When the numbers of
experiments and workers is considered there are more than 9000 possible ways that success can
possibly be reached. To narrow down the best choice for the number of workers and
experiments risk analysis was performed. Figure IX.a shows risk associated with 5 lab
technicians. From looking at the figure it can be seen that 85 experiments with 5 techs is the
riskiest combination in comparison with 50 and 100 experiments. The scenario consisting of 85
Table IX.a Time required in days for various combinations of experiments and workers

47
experiments and 5 techs led to a probability of around 0.37 for not making money. The 50 and
100 experiment scenarios were shown to have about the same probability as each other having
probabilities of around 0.26. It can also be seen from the figure that 85 experiments and 100
experiments had the chance to be the most profitable giving net present values of around $295
million
5 Lab Technicians
0
0.1
0.2
0.3
0.4
0.5
0.6
-25 -5 15 35 55 75 95 115 135 155 175 195 215 235 255 275 295
NPV (million$)
5 techs 100 exp
5 techs 85 exp
5 techs 50 exp
The optimal combination that was found for our circumstances was found using 10 lab
techs and 85 experiments. The risk associated with 10 lab technicians can be seen in Figure
IX.b. From the graph it can be seen that the risk of losing money for 100, 85, and 50
experiments is very close with a probability of 0.26. With our optimal choice it was found that
the NPV could reach as much as $295 million. The reason that this combination of 10 lab techs
and 85 experiments was optimal was because it gave the least amount of risk for the time
Figure IX.a Risk Analysis on 5 lab technician s

48
required to complete the FDA process. By having more lab techs the time was able to be
decreased for the FDA process which helps to get our product out on the market more quickly.
10 Lab Technicians
0
0.1
0.2
0.3
0.4
0.5
0.6
-25 -5 15 35 55 75 95 115 135 155 175 195 215 235 255 275 295
NPV (million $)
10 techs 100 exp
10 techs 85 exp
10 techs 50 exp
X. Demand
The demand for our solution was determined through a series of steps. The first step in
determining the demand was a happiness function. The happiness function for the new
treatment was based off of the current treatment with a happiness value of 40%. It was
determined by assigning values to three different variables. The three variables were treatment
life, cost, and pain of injections. Treatment life was the most important of the three variables
given a weight of .75, while the other two variables were given values of .125. These variables
were all related to different parameters such as amount of crosslinking, size of injections, amount
polymerized, and length of polymer chains. The purpose of the happiness function was to
provide a relationship between current treatments and our treatment. The relationship between
these two values can be seen in X. 1 which was used to find a value called β.
Figure IX.b Risk analysis on 10 lab technicians

49
happinesstreatmentnew
happinesstreatmentold
__
__=β (X.1)
It was assumed that β would change from year to year because of competition improving
treatments to compete with our treatment. It was also assumed that after 5 years this new
treatment will be replaced by a treatment that is better. Another variable that was important that
was used with β was α. The value α was important because it was based on how much someone
was going to know about our treatment in relationship to current treatments. For example if both
treatments were known about equally then the value would be 1, but if our treatment is know half
as much as current treatments then the value is 0.5. The value of α was assumed to increase each
year because of advertisement and information about our treatment spreading through word of
mouth. Table X.i below shows values of α and β that were used over the 5 year period.
Year α β
0 0 0.645
1 0.15 0.715
2 0.4 0.785
3 0.89 0.855
4 0.99 0.925
5 1 0.995
These values were applied to equations X.2 and X.3. Important values that had to be
determined before these equations could be used were our treatment price (p1), our competition’s
treatment price (p2), the total market demand for our product (D), and currently what is being
spent on a yearly basis for treatments (Y). From research it was found that our current
Table X.a. Values of α and β over the life of the treatment

50
competition’s treatment cost about $1250 per year and that around 7 million people per year visit
physicians for OA treatments. It was also found that approximately $1.5 billion a year is spent
on viscosupplementation treatments. With this information it was determined that for our
treatment to be competitive it should be priced at about $2400 per treatment because of the
longer life of our treatment. Using the gathered information we were able to apply equations X.
2 and X. 3 to find our treatment’s demand (d1) and our competition’s demand (d2).
Ydpdp ≤+ 2211 (X. 2)
β
α
αβ2
12211 d
ddpdp = (X. 3)
Combining X.2 and X.3 led to the formation of X.4 and X.5. These equations were used to find
d1 and d2 which had to fit within the boundaries of X.6.
α
βα
112
1
21
21 dd
p
p
p
Y
p
pd
−
= (X. 4)
12
1
2
2 dp
p
p
Yd −= (X. 5)
Ddd ≤+ 21 (X. 6)
Using X.4 a graph was able to be created that related demand. This graphical relationship was
used to find the demand. The demand was determined to be the place of intersection between the
two lines that were graphed where the maximum demand occurred. For example in year 1 you
can see from graph 1 that the demand is around 370,000 people. This same idea was applied to
years 2, 3, 4, and 5. From using the same principles it was found that in year 2 the demand
would be approximately 620,000 people and in years 3, 4, and 5 it would be a maximum at
around 625,000 people.

51
demand in the market
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
0 100,000 200,000 300,000 400,000 500,000 600,000
d1
d1
From calculating the demand for our treatment (d1) we were able to solve for the competitions
demand (d2). These demands were checked in X.6 to make sure that they were not greater than
the overall demand.
XI. Cost Analysis
Although the primary goal of this research is to develop a novel, more effective method
of relieving the symptoms of osteoarthritis, attention must be given to the economics involved.
To analyze this project from a business point of view, the total capital investment, total product
cost, annual cash flow, net present worth, return on investment, and pay-out time will be
discussed in this section.
Total Capital Investment
The total capital investment (TCI) is the money required to start a business
operation before revenue is available and is equal to the sum of the fixed capital
investment (FCI) and the working capital (WC).8
Graph X.a - Demand in the market at year 1

52
WCFCITCI += (XI.1)
The fixed capital investment is that necessary to obtain, develop, and equip the facilities
to be used for production, while the working capital is that needed to sustain operation.8
To obtain a preliminary estimate, the method of percentage of delivered-equipment costs
as in Peters and Timmerhaus will be used with an anticipated accuracy of ± 20-30
percent, which is an acceptable approximation at this early stage of the proposal.8
Fixed Capital Investment
The fixed capital investment can be divided into direct and indirect costs, and
these can be estimated as a percentage of the total FCI as given by Peters and
Timmerhaus (241).
To obtain a better assessment for the cost of our process, the direct and indirect
costs were estimated as a percentage of the delivered equipment costs after a list of
purchased equipment was generated as shown in TableXI.i. The list includes major
laboratory equipment and accessories needed for pre-clinical experiments, as well as
many of those required for clinical testing. There of course are items that will be added
as the need arises, hence the inclusion of miscellaneous cost. The prices shown were
found from online product catalogues of Fisher-Scientific and VWR.8,10 The percentage
estimates presented in Peters and Timmerhaus (251) are for solid, solid-fluid, and fluid
processing plants, so because these are not suitable representations for biochemical
processes, an economic study done in the biotechnology industry was used to obtain
better ratios. TableXI.ii on the following page shows these ratios and the calculated
costs.

53
Table XI.a – Estimated equipment costs 8,10
Equipment Quantity Unit Cost Total Cost
Autoclave 1 $ 4,330.00 $ 4,330.00
Torque rheometer 1 $ 40,000.00 $ 40,000.00
Centrifuge 1 $ 2,995.00 $ 2,995.00
Computers 4 $ 1,200.00 $ 4,800.00
Culture Flasks 100 $ 1.30 $ 130.00
Eppendorf pipets 4 $ 345.00 $ 1,380.00
Falcon tubes 500 $ 0.45 $ 225.00
Glassware, stirrers, etc Multi $ 750.00
Hemacytometer 1 $ 215.00 $ 215.00
Incubator 2 $ 6,245.00 $ 12,490.00
Laminar hood 1 $ 7,421.00 $ 7,421.00
Liquid N2 1 $ 2,610.00 $ 2,610.00
Microscope 1 $ 750.00 $ 750.00
Orbital shaker 2 $ 550.00 $ 1,100.00
Osmometer 1 $ 8,418.00 $ 8,418.00
Pasteur pipets 1000 $ 0.08 $ 80.00
Printer/Fax/Scanner 1 $ 300.00 $ 300.00
Reaction Vessel 1 $ 2,000.00 $ 2,000.00
Refrigerator/Freezer 1 $ 1,417.00 $ 1,417.00
Scale 1 $ 3,957.00 $ 3,957.00
Spectrophotometer 1 $ 6,700.00 $ 6,700.00
Sterile pipets (various sizes) 1600 $ 0.34 $ 544.00
Stirrer/Hot Plate 2 $ 420.00 $ 840.00
Syringes 100 $ 0.27 $ 27.00
Vortex 1 $ 248.00 $ 248.00
Water bath 1 $ 2,245.00 $ 2,245.00
Water purification 1 $ 4,000.00 $ 4,000.00
Total Equipment Cost $ 109,972.00

54
Table XI.b - Estimated TCI based on delivered-equip ment cost
Components % of Delivered-Equipment Cost
Cost
Direct Costs
Purchased equipment 100 $ 109,972.00
Purchased-equipment installation 41 $ 45,088.52
Instrumentation (installed) 40 $ 43,988.80
Piping (installed) 35 $ 38,790.20
Electrical (installed) 10 $ 10,797.20
Buildings (including services) 40 $ 43,188.80
Yard improvements 15 $ 16,195.80
Service facilities (installed) 40 $ 43,188.80
Total direct costs 280 $ 353,190.12
Indirect Costs
Engineering and supervision 82 $ 90,737.04
Construction expense 116 $ 127,847.52
Contractor's fee 26 $ 28,672.72
Contingency 53 $ 58,025.16
Total indirect costs 277 $ 304,282.44 Fixed-capital investment $ 657,472.56 Working capital (15% of TCI) $ 116,730.45 Total Capital Investment $ 773,203.01
Total Product Cost
The total product cost (TPC) includes all costs associated with processing and
selling the product, recovering the capital investment, and continuing research and
development.8 These can be subdivided into manufacturing costs and general expenses.
Table XI.iii below shows estimates for these costs with a total product cost of
$244,600,000. The injections to be produced per year were determined from the demand
model as described earlier in the demand section.

55
Raw Materials Factor Quantity/year Cost per rate unit Calculated Cost
Injection materials 350000 $688.29 injection $240,976,535.83 *See Table IX.i for list Total $240,976,535.83 Operating Labor $287/hr 7884 hr/year $2,262,708.00 Operating Supervision 0.15 of operating labor $339,406.20 Utilities $14,000.00 Maintenance and Repairs 0.07 of FCI $46,453.08 Operating Supplies 0.4 of maintenance and repairs $18,267.96 Laboratory Charges 0.15 of operating labor $339,406.20
Variable Product Costs $243,964,777.27
Depreciation Straight line depreciation (not included here)
Taxes (property) 0.02 of FCI $13,129.45 Insurance 0.01 of FCI $6,564.73 Rent 0 Already have plant Fixed Charges $19,194.18 Plant Overhead 0.1 of total product costs $77,820.30 Administrative 0.2 of maintenance, operating labor, operating supervision $529,113.46 Distribution and Marketing 0.1 of total product costs $77,820.30 Research and Development 0.05 of total product costs $38,910.15
General Expenses $723,664.21 Total Product Cost $244,622,635.65
Based upon the estimate that the demand model gave for the number of patients
expected per a year risk was assessed on the NPV based on whether a person would or
would not get the injection. The risk that was used was based upon the idea that this
value could be larger or smaller depending upon how the market reacted. The reaction
was determined to be ± 200,000 people per year receiving the injection. This would lead
to a best and worst case scenario and give an idea of how this would affect the business in
marketing the solution. After risk analysis was done a positive mean net present worth
was observed with a good possibility of still making a profit. This sensitivity analysis
can be seen in Figure XI.a, having a probability as shown by the histogram in Figure XI.b
shown below.
TableXI.c – Total product cost estimation

56
Selling Price
In order to be competitive with other HA injection companies with a cost of
$1300 per year, we estimated our cost to the patient to be $2,400 per treatment. This is
more expensive than the leading hylan injection Synvisc®, which has a wholesale cost
(not including physician expenses) of $660 for the five-week injection series and must be
administered twice per year. The reason for our price being higher was because of the
Distribution for NPV (millions)/M19
Val
ues
in 1
0 ̂-
3
0.000
0.500
1.000
1.500
2.000
2.500
3.000
Mean=222.61
-200 0 200 400 600 800-200 0 200 400 600 800
5% 90% 5% -17.9703 442.2469
Mean=222.61
Distribution for NPV (millions)/M19
0.000
0.200
0.400
0.600
0.800
1.000
Mean=222.61
-200 0 200 400 600 800-200 0 200 400 600 800
5% 90% 5% -17.9703 442.2469
Mean=222.61
Figure XI.a – Distribution of net present worth (without depreciation)
Figure XI.b – Probability of net present worth

57
longer life of our treatment. Our treatment is expected to be superior and last about twice
as long hence the reason for our price being about twice the amount of our competitor’s.
As more patients use our product and more positive results are documented, the demand
for our product will increase making for a very profitable business.
XII. Conclusion
Osteoarthritis creates such a large consumer market in the United States which is
expected to grow as the average age of the population continues to increase, it is without
question that viscosupplementation serves as a potential solution to return patients suffering from
the disease to their normal pain-free active lives. However, because this industry is still in its
early stages, there are several issues with current available treatments that need to be addressed
before these intra-articular injections can truly be effective. Some patients do not feel the relief
provided is worth the pain involved in the injections, which in most cases must be repeated every
6 months. The main problem with current products is their lack of retention time in the synovial
cavity due to either degradation, transport across the synovial membrane, or simply missing the
synovial space during injection. We propose that a superior solution is to use hyaluronic acid
modified with 2-vinyl which will then be crosslinked to form a hydrogel. This crosslinking will
result in a more viscous, more elastic gel that will provide the load support and lubrication
necessary to keep bone-on-bone contact from occurring. We chose to use ammonium
peroxydisulfate because of the proven ability of sulfate groups to buffer against degradation and
prevent denaturation.
We suggest in the future that further research be done on the scale up and
commercialization of HYAL-VYNE to bring the product to the market. This will need to
include a complete business plan with a full design of the production process and investigation of
the market and plant locations. Also of concern is the possibility that ammonium

58
peroxydisulfate will significantly reduce the pH when added to the modified HA. This may be
avoided by using a buffer solution but because it will be injected into the body, it must be non-
toxic and must not affect the integrity of the gel. Since HYAL-VYNE is a novel idea, one final
issue is the patenting of the product to protect the technology. This will greatly increase total
product costs and will need to be included in the cost analysis.

59
References
1. “Report Measures Impact of Knee Conditions.” Knee1.com. 11 November 2003. http://www.knee1.com/news/mainstory.cfm/220/1
2. “Osteoarthritis Fact Sheet.” Arthritis Foundation. 2005.
http://www.arthritis.org/conditions/fact_sheets/OA_Fact_Sheet.asp
4. “Dissectors Answers – Joints of the Upper and Lower Limbs.” University of Michigan Medical School. 2000. http://images.google.com/imgres?imgurl=http://anatomy.med.umich.edu/images/knee_joint_post.jpg&imgrefurl=http://anatomy.med.umich.edu/musculoskeletal_system/joints_ans.html&h=363&w=400&sz=22&tbnid=Ngvb4pYw0_GrKM:&tbnh=108&tbnw=120&hl=en&start=162&prev=/images%3Fq%3Dhuman%2Bknee%26start%3D160%26svnum%3D10%26hl%3Den%26lr%3D%26sa%3DN
5. “Knee Joint – Anatomy and Function.” The Center for Orthopaedics and Sports
Medicine. Marietta, GA. 3 April 2003. http://www.arthroscopy.com/sp05001.htm
6. “Chemical and Other Safety Information.” The Physical and Theoretical Chemistry Laboratory, University of Oxford. 7 March 2006. http://ptcl.chem.ox.ac.uk/MSDS/#MSDS
7. “Product Search – FisherScientific.” 2006. <https://www1.fishersci.com/>
8. Peters, Max S., Klaus D. Timmerhaus, Ronald E. West. Plant Design and Economics for
Chemical Engineers, 5th ed. New York: McGraw Hill, 2003.
9. “End of Small Volume High Value Myth in Biotechnology – Process Design for a Mega-plant Producing γ-Interferon for Mega Profit.”
10. “2006 – 2008 General Catalogue.” VWR.
http://www.vwrsp.com/catalog/index.cgi?parent_id=9000002
11. Mironowicz, Magdalena and Sarah Saw. “Electronic Texbook – Joints: Part 1.” WorldOrtho, Inc. 1997. http://www.worldortho.com/database/etext/joints.html
12. “Articular Cartilage Zones in Normal Articular Cartilage.” Histology Atlas. School of
Physical Therapy, Slippery Rock University. http://www.sru.edu/depts/pt/histo/artic_cartilage.htm
13. Knox, P., J.R. Levick and J.N McDonald. Quarterly Journal of Experimental
Physiology. 73.1, 33-45.
14. Tadmor, Rafael; Nianhuan Chen, and Jacob N. Israelachvili. Journal of Biomedical Materials Research. 61.4, 514-523.

60
15. Hinton, Ralph et al. “Osteoarthritis: Diagnosis and Therapeutic Considerations.” American Family Physician. 1 March 2002.
16. “Osteoarthritis Overview.” eMedicine Consumer Health. <
http://www.emedicinehealth.com/articles/5494-1.asp >
17. “Osteoarthritis: medical information about the symptoms, diagnosis and treatment of degenerative joint disease.” MedicineNet.com 16 April 2004.
18. Hascall, Vincent and Torvard Laurent. “Hyaluronan: Structure and Properties.”
Glycoforum/Science of Hyaluronan-1.
19. Dinnar, U. “Lubrication Theory in Synovial Joints.” CRC Critical Reviews in Bioengineering 1975.
20. Griffith, Robert W., MD. “Knee Osteoarthritis: Is Arthroscopy Any Help?” Health and
Age. 24 January 2003.
21. Wen, Dennis Y., MD. “Hyaluronic Acid Injections for knee Osteoarthritis.” American Family Physician. The American Academy of Family Physicians. 1 August 2000.
22. “Federal Food, Drug, and Cosmetic Act – Chapter II.” US Food and Drug
Administration.
23. “Total Cost to Develop New Prescription Drug, Including Cost of Post-Approval Research, is $897 million.” Tufts Center for the Study of Drug Development. 13 May 2003.
24. “Device Advice – Premarket Approval.” US Food and Drug Administration Center for
Devices and Radiological Health. 1 November 2002.
25. Jones, D.B. and Middelberg, A. P.J. Langmuir 2002, 18, 10357-10362.
26. Kluger, R. and Alagic, A. Bioorganic Chemistry 2004, 32, 451-472.
27. Langer, Robert S.; Elisseeff, Jennifer, H.; Anseth, Kristi; Sims, Derek; “Semi- interpenetrating or interpenetrating polymer networks for drug delivery and tissue engineering” May 3, 1997.
28. Binette, J.S.; Garon, M.; Savard, P.; McKee, M. D.; Buschmann, M. D.; Journal of
Biomechanical Engineering 2004, 126, 475-484.
29. Huin-Amargier C.; Marchal, P.; Payan, E.; Netter, P.; Dellacherie, E.; Journal of biomedical materials research 2006, 76A, 416-424.
30. Uebelhart, Daniel MD.; Williams, James M. PhD.; Current Opinion in Rheumatology
1999, 11(5), 427.

61
31. Soltes, L. and Mendichi, R. Biomedical Chromatography 2003, 17, 376-384.
32. Burdick, J. A.; Khademhosseini, A.; Langer, R.; Langmuir 2004, 20(13), 5153-5156.
33. Ponnuraj, K. and Jedrzejas, M. J. Journal of Molecular Biology 2000, 299, 885-895.
34. Waddell, D. MD; Rein, A. MS; Panarites, C. PhD; Coleman, M. MD; Weiss, C. MD;
The American Journal of Managed Care 2001, 7(10), 981-991.
35. Ochiai, H.; Ohmae, M.; Mori, T.; Kobayashi, S.; Biomacromolecules 2005, 6, 1068-1084.
36. Han, T. Journal Zhejiang University SCI 2004, 5(8), 928-931.
37. Chang, W.; Chang, Y.; Chen, Y.; Sung, H.; Artificial Cells, Blood Substitutes, and
Biotechnology 2004, 32(2), 243-262.
38. Hennink, W.E.; Nostrum, C.F.; Advanced Drug Delivery Reviews 2002, 54, 13-36.
39. Lipowitz, A. J.; “Synovial Fluid”, Ch. 86, 2006, 1-19.
40. Anggiansah, C. L.; Scott, D.; Poli, A.; Coleman, P. J.; Badrick, E.; Mason, R. M.; Levick, J. R.; The Journal of Physiology 2003, 550.2, 631-640.
41. Milas et al. Biopolymers 2000, 59.4, 191-204. 42. Kirker, Kelly R. and Glenn D. Prestwich. Journal of Polymer Science: Part B: Polymer
Physics 2004. 42.23, 4344-4356. 43. Benedetto, Biasco, Pisinano, and Cingolani Nanotechnology 2005, 16, 165-170. 44. “Osteoarthritis Fact Sheet.” Arthritis Foundation. 2005. 45. Prestwich, Glenn D. “Biomaterials for Chemically-Modified Hyaluronan.” GlycoForum
29 March 2001. 46. “Arthroscopic Lavage.” The Knee Guru Dictionary. www.kneeguru.co.uk 47. Dinnar, U. CRC Critical Reviews in Bioengineering 1975, 2.2, 159-177. 48. Szeri, Andras Z. Fluid Film Lubrication Theory & Design. Cambridge University Press:
Cambridge, UK. 1998. p. 267-310. 49. “Is the Product a Medical Device?” Food and Drug Administration, 30 June 1998.

62
50. Shreve, Mark et al. NKOB. University of Oklahoma, ChE 4273. Spring 2005.
51. Miyamoto, Kenji et al. Journal of Biomedical Materials Research: Part A. 70.4, 550-559.
52. Leach, Jennie Baier et al. Biotechnology and Bioengineering. 82.5, 578-589.
53. Wallin, Richard F. and Edward F. Arscott. Medical Device and Diagnostic Industry
Magazine. April 1998.





![Hyaluronic Acid / Viscosupplementation1].pdf · Hyaluronic Acid/Viscosupplementation Response to Topic and Public Comments on Key Questions May 14, 2013 Prepared by: HAYES, INC. 157](https://static.fdocuments.in/doc/165x107/5b898ad37f8b9a655f8c6cab/hyaluronic-acid-viscosupplementation-1pdf-hyaluronic-acidviscosupplementation.jpg)