Osher Mini-Med school slides for...
13
6/13/2016 1 COMMUNITAS Transforming the Experience of Pediatric Chronic Illness through mind‐body medicine June 16, 2016 Brittany Blockman, Clinical Fellow Osher Center for Integrative Medicine Neither I nor my immediate family members have a personal financial relationship with a manufacturer of pharmaceutical products or services that will be discussed in this presentation. Presentation Overview My Story The Problem The Solution Impact
Transcript of Osher Mini-Med school slides for...

6/13/2016
1
COMMUNITASTransforming the Experience of Pediatric Chronic Illness through
mind‐body medicine
June 16, 2016
Brittany Blockman, Clinical Fellow Osher Center for Integrative Medicine
Neither I nor my immediate family members have a personal financial relationship with a manufacturer of
pharmaceutical products or services that will be discussed in this presentation.
Presentation Overview
My Story
The Problem
The Solution
Impact

6/13/2016
2
Visions and Visuals
THE PROBLEM
Background
11 million US children and teens live with a chronic condition. (Data Resource Center for Child and Adolescent Health, 2013)
6/13/2016
3
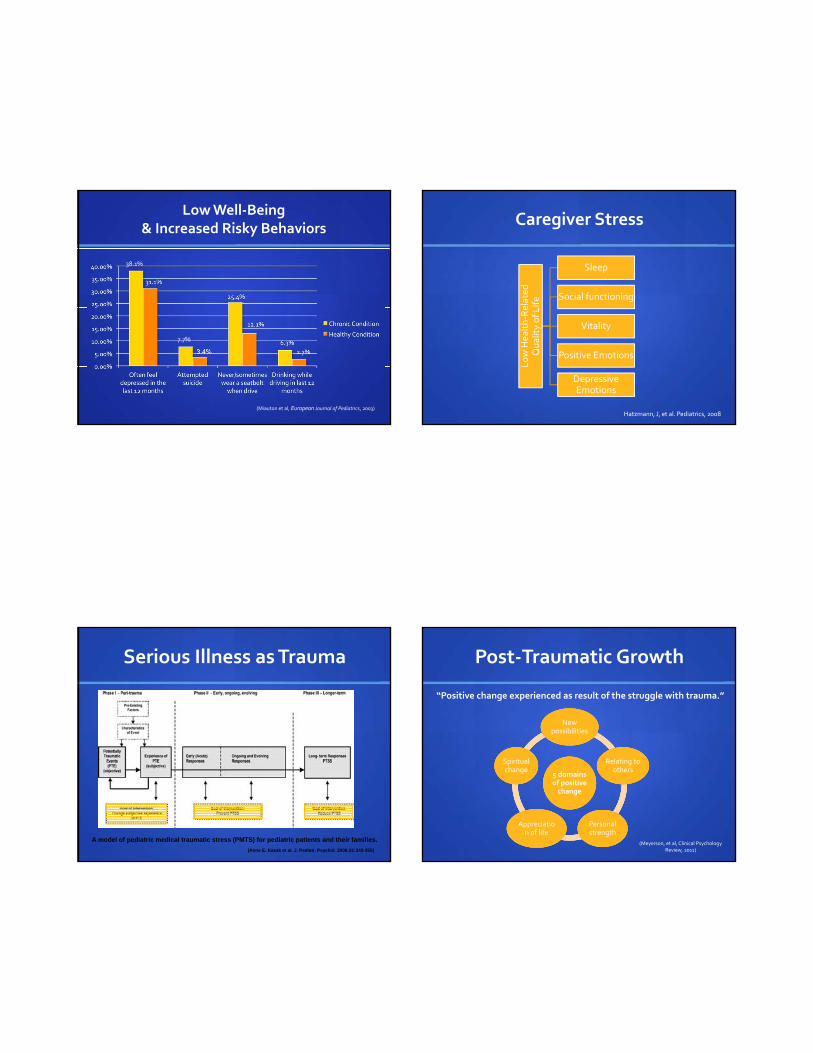
Low Well‐Being & Increased Risky Behaviors
(Miauton et al, European Journal of Pediatrics, 2003)
38.1%
7.7%
Caregiver Stress
Low Hea
lth‐Related
Quality of Life
Sleep
Social functioning
Vitality
Positive Emotions
Depressive Emotions
Hatzmann, J, et al. Pediatrics, 2008
A model of pediatric medical traumatic stress (PMTS) for pediatric patients and their families.
(Anne E. Kazak et al. J. Pediatr. Psychol. 2006;31:343-355)
Serious Illness as Trauma Post‐Traumatic Growth
“Positive change experienced as result of the struggle with trauma.”
5 domains of positive change
5 domains of positive change
New possibilities
New possibilities
Relating to others
Relating to others
Personal strength Personal strength
Appreciation of life
Appreciation of life
Spiritual change Spiritual change
(Meyerson, et al, Clinical Psychology Review, 2011)

6/13/2016
4
Factors Associated with PTG
Post‐Traumatic Growth
Indicators of mental health
Indicators of mental health
Quality of patients' coping
strategies
Quality of patients' coping
strategies
Quality of social support
Quality of social support
(Barskova and Oesterreich, 2009)
THE SOLUTION
To address the unmet psychosocial, quality‐of‐life, and healing needs of young people living with chronic
illnesses and their families
and
Help them harness the potential of illness to be transformers for positive growth
and cultivation of resilience
MISSION
A world in which illness and adversity connect people, rather than isolate them;
In which difficulties make people stronger, more resilient, and whole, rather than breaking them;
In which meaning, purpose, insight can be found in coming together around life’s most challenging
experiences.
VISION

6/13/2016
5
COMMUNITAS PILOT PROGRAM OBJECTIVES
1. Mind‐body and self‐care skills
2. Peer support and sharing
3. Access to adjunct modalities
4. Forum for discussion
5. Increase adherence
What is Mind‐Body Medicine? Efficacy of Mind‐Body Medicine programs
Comparison of Mean Changes/Decreases pre‐post
‐12.3
‐0.1
(Speca M et al, Psychosomatic Medicine , 2000)
6/13/2016
6
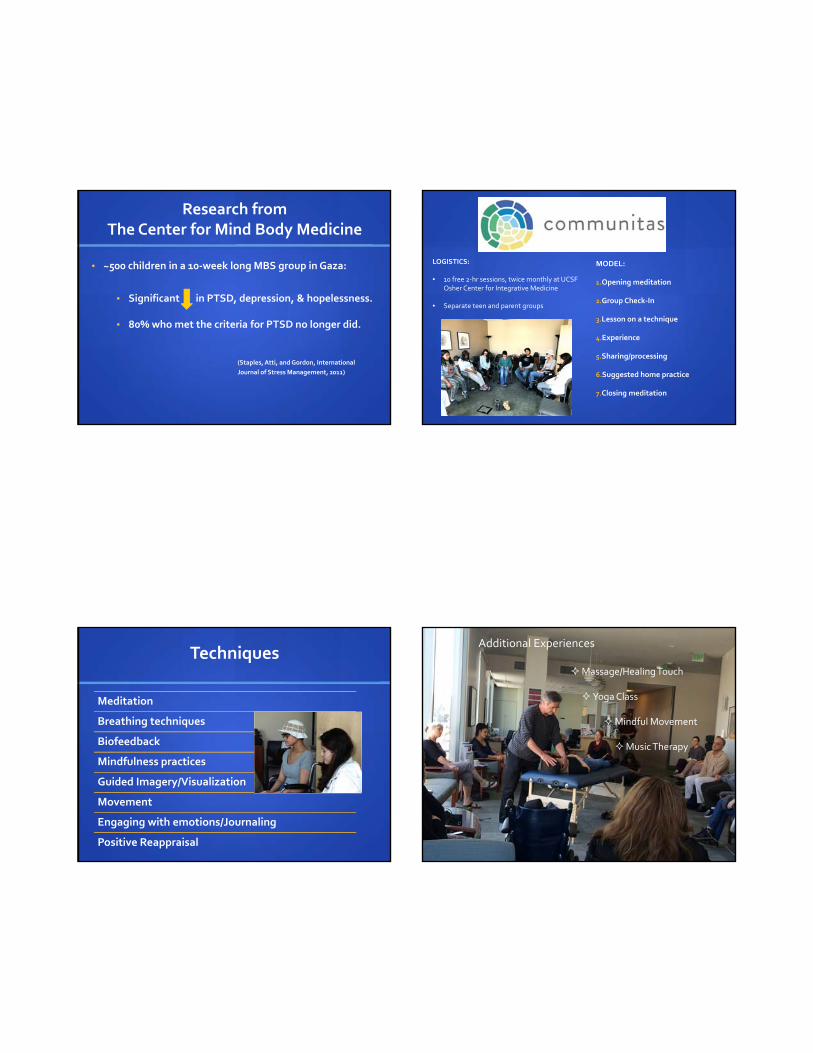
Research from The Center for Mind Body Medicine
• ~500 children in a 10‐week long MBS group in Gaza:
• Significant in PTSD, depression, & hopelessness.
• 80% who met the criteria for PTSD no longer did.
(Staples, Atti, and Gordon, International
Journal of Stress Management, 2011)
Communitas
MODEL:
1.Opening meditation
2.Group Check‐In
3.Lesson on a technique
4.Experience
5.Sharing/processing
6.Suggested home practice
7.Closing meditation
LOGISTICS:
• 10 free 2‐hr sessions, twice monthly at UCSF Osher Center for Integrative Medicine
• Separate teen and parent groups
Techniques
Meditation
Breathing techniques
Biofeedback
Mindfulness practices
Guided Imagery/Visualization
Movement
Engaging with emotions/Journaling
Positive Reappraisal
Additional Experiences
Massage/Healing Touch
Yoga Class
Mindful Movement
Music Therapy

6/13/2016
7
Communitas Pilot Program January – June 2014
THE IMPACT
METHODS: Study Objectives
1) To examine the effects of Communitas on teens with life‐altering chronic illnesses and their parents in the following realms:
physical and mental wellbeing
coping
stress
mindfulness
resilience
2) To examine the feasibility and acceptability of Communitas.
METHODS: Study Design
Single‐center, non‐controlled, pre‐post pilot study
Data gathered using validated instruments and video interviews at:
1) Baseline
2) Immediately post‐intervention 3) 3 months after final session

6/13/2016
8
Teens living w/ life‐altering chronic physical illness, along w/ their available guardian(s).Teens living w/ life‐altering chronic physical illness, along w/ their available guardian(s).
13‐19 years of age, English‐speaking13‐19 years of age, English‐speaking
Cognitively intact enough to participate in a meaningful way.Cognitively intact enough to participate in a meaningful way.
Recruitment via referrals from UCSF inpatient and outpatient providers and community organizations.Recruitment via referrals from UCSF inpatient and outpatient providers and community organizations.
METHODS: Participants and Recruitment
METHODS: Outcome Measures
• Attendance and study retentionFEASIBILITY & ACCEPTIBILITYFEASIBILITY & ACCEPTIBILITY
• NIH PROMIS Global Health ScalePHYSICAL & MENTAL WELLBEING
PHYSICAL & MENTAL WELLBEING
• The Profile of Mood StatesMOODMOOD
• The Brief Cope ScaleCOPINGCOPING
• The Perceived Stress Scale STRESSSTRESS
• The Mindful Attention Awareness ScaleMINDFULNESSMINDFULNESS
• The 14‐ Item Resilience ScaleRESILIENCERESILIENCE
METHODS: Data Analysis
Paired t tests to assess changes from baseline to immediately post‐intervention & 3 months post‐intervention.
Cohen's d effect sizes (mean difference/SD):
Small: 0.2
Medium: 0.5
Large: 0.8
RESULTS: Referrals/Enrollment
49 referrals
18 Enrolled
10 came to first session
9 attended at least 4 of the sessions
1 dropped out after 1 session
7 dropped out before program began
31 Not enrolled

6/13/2016
9
RESULTS: Demographics & Feasibility
Demographic Value
Patient ParticipantsParent Participants
N = 10 1 drop‐out not included in final analysisN = 8 1 drop‐out not included in final analysis
Average Age 14.8 years (range 13‐18)
Sex 67% Female
Time from Diagnosis 7.9 years (range 0.5 ‐16 years)
Public Insurance 67%
Sex of Parent 75% mothers
Average Attendance Teen: 7.3 sessions (range 4‐10)Parent: 7.5 sessions (range 4‐10)
RESULTS: Illnesses Represented
N=10Juvenile Idiopathic arthritis
Cerebral palsy
Type I Diabetes
Brain Tumor
Muscular Dystrophy
Cystic Fibrosis
Interstitial Lung Disease
Spinal Cord Injury
Wegener’s Granulomatosis
Leukemia
RESULTS: Physical and Mental Wellbeing
INSTRUMENT Baseline Mean
Pre‐postMean Change (SD)
Effect Size P Value
NIH Promis Self‐Reported Physical Health
13.15 +1.56 (1.99) +0.78 0.047
NIH Promis Self‐Reported Mental Health
13.00 +2.33 (2.55) +0.92 0.025
= statistically significant
RESULTS: Mood
INSTRUMENT Baseline Mean
Pre‐postMean Change (SD)
Effect Size
P Value
Profile of Mood States: Tension 1.40 ‐0.78 (0.62) ‐1.25 0.006
Profile of Mood States: Anger 1.36 ‐0.54 (0.65) ‐0.82 0.039
Profile of Mood States: Depression 0.93 ‐0.36 (0.88) ‐0.45 0.215
Profile of Mood States: Fatigue 1.22 ‐0.33 (0.58) ‐0.57 0.125

6/13/2016
10
RESULTS: Coping
INSTRUMENT BaselineMean
Pre‐postMean Change (SD)
Effect Size P Value
Brief Cope Scale:Distraction/Disengagement
2.94 ‐0.44 (0.53) ‐0.84 0.035
Brief Cope Scale:Denial
1.89 ‐0.33 (0.66) ‐0.50 0.169
Brief Cope Scale:SubstanceAbuse
1.22 ‐0.22 (0.44) ‐0.50 0.169
Brief Cope Scale:Positive Reframing
2.72 +0.33 (0.83) 0.40 0.262
RESULTS: Stress, Resilience,& Mindfulness
INSTRUMENT Baseline Mean
Pre‐postMean Change (SD)
Effect Size P Value
PerceivedStress Scale
13.3 ‐3.89 (3.09) ‐1.26 0.005
Resilience Scale 3.78 +0.48 (0.64) +0.74 0.056
Mindful Attention Awareness Scale
4.70 + 0.31 (0.49) +0.64 0.092
Would you want to participate in a program like this again?
8/9 teens said Yes.8/8 parents said Yes.
Study Limitations
No control group
Small sample size
Based on patient reporting
Multi‐component intervention

6/13/2016
11
Pilot: Phase 2
An abundance of THANK YOUS…
Funding
Mount Zion Health Fund: $26,100
The Patient Care Fund: $10,000

6/13/2016
12
TEAM: CONTENT ADVISORS
Jim Gordon, MD Founder/Director of The Center for Mind‐Body MedicineFormer Chairman of the White House Commission on Complementary and Alternative Medicine PolicyPsychiatry and Family Medicine Professor, Georgetown Medical School
David Becker, MD, MPHUCSF primary care pediatrician and IM specialistPediatrician, UCSF Osher Center for Integrative Medicine
TEAM: RESEARCH MENTORS
Judith Moskowitz, PhD, MPH Social Psychologist focused on emotion and coping
in the context of health‐related chronic stress former research at Osher Center; now at
Northwestern
Frederick M. Hecht, MD Research Director of the UCSF Osher Center for
Integrative Medicine HIV and integrative medicine researcher Internal Medicine Physician, UCSF and SFGH
TEAM: Co‐Facilitators and Volunteers
Cliff Smyth, MA PhD Candidate, Mind‐Body Medicine, SaybrookUniversity
Kelsey Menehan, LCSW Faculty at The Center for Mind‐Body Medicine
15 volunteers from the medical school and UCSF community
COMMUNITY: Partners/Supporters

6/13/2016
13
More thank you’s!
Advisors: Anda Kuo, Amy Whittle, Clem Donahue, and Jamal Harris
Statistician: Mike Acree, PhD
Lead Program Assistants: Elizabeth Sanseau and Milana Pebenito
Research Assistants: Arielle White, Sandeepa Sriram, Elise Taylor, David Noorvash, John Best
Volunteers: Kaitlyn Krauss, FolashadeWolfe‐Muldupe, Wolf Mehling,Erika Padilla‐Morales, Marisol Romero
My partner Josh, family, and friends!
Comments or Questions?
References
Boekaerts M, Roder I. “Stress, coping, and adjustment in children with a chronic disease: a review of the literature.” .Disabil Rehabil 1999 Jul;21(7):311‐37
Compas BE, et al. “Coping with chronic illness in childhood and adolescence.” Annu Rev Clin Psychol. 2012;8:455‐80.
Hatzmann J, Heymans HS, Carbonell A, van Praag BM, Grootenhuis MA. Hidden consequences of success in pediatrics: parental health‐related quality of life‐results from the care project. Pediatrics. 2008;122:e1030–8.
Lavigne, JV and J Faier‐Routman. “Psychological Adjustment to pediatric physical disorders: A meta‐analytic review.” Journal of Pediatric Psychology 17(2) 1992: 133‐157.
Meyerson, DA, et al. Posttraumatic growth among children and adolescents: a systematic review. Clin Psychol Rev. 2011 Aug;31(6):949‐64. Epub 2011 Jun 13.
Miauton, L., Narring, F, and PA Michaud. “Chronic Illness, Lifestyle, and emotional health in adolescence: Results of a cross‐sectional survey on the health of 15‐20 year‐olds in Switzerland.” European Journal of Pediatrics 162(10) 2003:682‐689.
References, cont’d
Modi, et al. “Pediatric Self‐Management: A Framework for Research, Practice and Policy: A Conceptual model of pediatric self‐management.” Pediatrics 2012
Patterson, J and RW Blum. “Risk and Resilience among children and Youth with disabilities.”Archives of Pediatrics and Adolescent medicine 150(7) 1996: 692‐698
M. Speca, L. E. Carlson, E. Goodey, and M. Angen, “A randomized, wait‐list controlled clinical trial: the effect of a mindfulness meditation‐based stress reduction program on mood and symptoms of stress in cancer outpatients,” Psychosomatic Medicine, vol. 62, no. 5, pp. 613–622, 2000.
Starfield, B et. Al. “Health Status of well versus ill adolescents.”Archives of Pediatric and Adolescent Medicine” 150(12) 1996: 1249‐1256.
Surís JC, “Health risk behaviors in adolescents with chronic conditions.” Pediatrrics 2008 Nov;122(5):e1
Taylor, RM, “The experience of living with a chronic illness during adolescence: a critical review of the literature.” Journal of Clinical Nursing Special Issue: Children & Young Persons 2008 vol 17(23): 3083–3091.
Tedeschi, Richard G.; Kilmer, Ryan P. Assessing Strengths, Resilience, and Growth to Guide Clinical Interventions. Professional Psychology: Research and Practice, Vol 36(3), Jun 2005, 230‐237.