Orthoses, Materials, and Foot Function · ber of layers, or form of the material used. A good...
10
SEPTEMBER 2004 • PODIATRY MANAGEMENT www.podiatrym.com 131 have been made in the diagnosis and treatment of mechanical prob- lems pertaining to gait, and thus the design and use of foot orthoses and insoles. Computer technology, new materials, and advances from orthotic laboratories have played a significant role in patient care. Foot Orthoses and Insoles By definition, an orthosis is a device that is used to protect, sup- port, or improve function of parts Continued on page 132 Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin- uing Medical Education by the Council on Podiatric Medical Education. You may enroll: 1) on a per issue basis (at $17.50 per topic) or 2) per year, for the special introductory rate of $109 (you save $66). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the near future, you may be able to submit via the Internet. If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred- its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test at no additional cost. A list of states currently honoring CPME approved credits is listed on pg. 140. Other than those entities cur- rently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be acceptable by any state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensure the widest acceptance of this program possible. This instructional CME program is designed to supplement, NOT replace, existing CME seminars. The goal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscripts by noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: Podia- try Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected]. Following this article, an answer sheet and full set of instructions are provided (p. 140).—Editor Goals and Objectives After reading this article the podia- tric physician should be able to: 1) Know the definition of the term orthosis and be familiar with the differ- ent types used in the treatment of foot pathology. 2) Know what are considered to be natural orthotic materials, their prop- erties and proper use in fabricating foot orthoses. 3) Know what are considered to be synthetic orthotic materials, their com- position, properties, and advantages and disadvantages when used in the fabrication of foot orthoses and insoles. 4) Understand a method of evaluat- ing plantar pedal pressure using a computerized in-shoe sensor system. 5) Recognize various pedal patholo- gies that can result from excessive forefoot pressure during ambulation. 6) Evaluate the effects of different types of foot orthoses and insoles on plantar pedal pressure by interpreting computer-generated pedal pressure displays. Continuing Medical Education O rthoses and insoles are the mainstay of mechanical foot therapy as it has developed over the last century. Over the past two decades, tremendous advances By Mark A Caselli, DPM Orthoses, Materials, and Foot Function Different uses require the unique properties inherent in the various types of devices available. ORTHOTICS ORTHOTICS
-
Upload
phungkhanh -
Category
Documents
-
view
213 -
download
0
Transcript of Orthoses, Materials, and Foot Function · ber of layers, or form of the material used. A good...
SEPTEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 131
have been made in the diagnosisand treatment of mechanical prob-lems pertaining to gait, and thusthe design and use of foot orthosesand insoles. Computer technology,new materials, and advances fromorthotic laboratories have played a
significant role in patient care.
Foot Orthoses and InsolesBy definition, an orthosis is a
device that is used to protect, sup-port, or improve function of parts
Continued on page 132
Welcome to Podiatry Management’s CME Instructional program. Our journal has been approved as a sponsor of Contin-uing Medical Education by the Council on Podiatric Medical Education.
You may enroll: 1) on a per issue basis (at $17.50 per topic) or 2) per year, for the special introductory rate of $109 (yousave $66). You may submit the answer sheet, along with the other information requested, via mail, fax, or phone. In the nearfuture, you may be able to submit via the Internet.
If you correctly answer seventy (70%) of the questions correctly, you will receive a certificate attesting to your earned cred-its. You will also receive a record of any incorrectly answered questions. If you score less than 70%, you can retake the test atno additional cost. A list of states currently honoring CPME approved credits is listed on pg. 140. Other than those entities cur-rently accepting CPME-approved credit, Podiatry Management cannot guarantee that these CME credits will be acceptable byany state licensing agency, hospital, managed care organization or other entity. PM will, however, use its best efforts to ensurethe widest acceptance of this program possible.
This instructional CME program is designed to supplement, NOT replace, existing CME seminars. Thegoal of this program is to advance the knowledge of practicing podiatrists. We will endeavor to publish high quality manuscriptsby noted authors and researchers. If you have any questions or comments about this program, you can write or call us at: Podia-try Management, P.O. Box 490, East Islip, NY 11730, (631) 563-1604 or e-mail us at [email protected].
Following this article, an answer sheet and full set of instructions are provided (p. 140).—Editor
Goals and ObjectivesAfter reading this article the podia-
tric physician should be able to:
1) Know the definition of the termorthosis and be familiar with the differ-ent types used in the treatment of footpathology.
2) Know what are considered to benatural orthotic materials, their prop-erties and proper use in fabricatingfoot orthoses.
3) Know what are considered to besynthetic orthotic materials, their com-position, properties, and advantagesand disadvantages when used in thefabrication of foot orthoses and insoles.
4) Understand a method of evaluat-ing plantar pedal pressure using acomputerized in-shoe sensor system.
5) Recognize various pedal patholo-gies that can result from excessiveforefoot pressure during ambulation.
6) Evaluate the effects of differenttypes of foot orthoses and insoles onplantar pedal pressure by interpretingcomputer-generated pedal pressuredisplays.
Continuing
Medical Education
Orthoses and insoles are themainstay of mechanical foottherapy as it has developed
over the last century. Over the pasttwo decades, tremendous advances
By Mark A Caselli, DPM
Orthoses,Materials, andFoot Function
Different uses require the unique propertiesinherent in the various types of devices available.
ORTHOTICSORTHOTICS

thoses offer some degree of both ac-commodative and functional prop-erties. In general, foot orthoses aredesigned to accomplish one ormore of the following:
1) reduce shock,2) reduce shear,3) relieve areas of excessive
plantar pressure,4) stabilize and support the
joints of the foot,5) limit motion of joints.5
Orthotic MaterialsMany different materials are
used in the fabrication of foot or-thoses. These materials are com-monly divided into three basictypes; soft, semi-flexible, and rigid.Examples of soft materials includepolyethylene foams such as Plasta-zote® (Bakalite Xylonite LTD, {BXL}UK), closed-cell neoprene impreg-nated with nitrogen bubbles suchas Spenco (Spenco Medical Corpo-ration, Waco, TX), open cell foamssuch as Poron (Rogers Corporation,Rogers, CT), and gel-like viscoelas-tic polymers such as silicone.Leather and cork materials are usu-ally considered to be semiflexible.Semiflexible materials are some-what accommodative but providemore functional support than thesoft type and do not bottom out asquickly.
Rigid materials include acrylicplastics and thermoplastic poly-mers. They are moldable at hightemperatures and are primarilyfunctional in nature. These are the
most durable andsupportive of thethree types. Thismethod of classi-fying materialsprovides a goodgeneral guidelinefor selecting ma-terials eitheralone or in com-bination for thefabrication of afoot orthosis.
The problem with this classifica-tion system is that it could be mis-leading without a thorough knowl-edge of the properties of each of thematerials. Many of the materialscan range from being soft to rigid,depending on the thickness, num-ber of layers, or form of the materialused. A good example of this is an
orthotic made from Plastazote,which can range from soft (a singlelayer of medium grade) to rigid(laminated layers of rigid grade). Abetter method is categorizing thematerials as either being natural orsynthetic with specific properties as-signed to each material.
Natural MaterialsNatural materials used for the
fabrication of orthoses are thosefound in nature and includeleather, cork, and rubber butter.
LeatherLeather orthoses can be either
functional or accommodative de-pending on material combinationsand casting techniques. The basicshell of a leather orthosis consistsof adding layers of leather to oneanother to form a lamination thatcan be shaped to a positive cast ofthe patient’s foot or molded to thefoot or to the inside of a shoe di-rectly.
The benefits of leather as an or-thotic material are a direct result ofits intrinsic natural characteristics.The collagen fibers that make upleather are woven in a three-dimen-sional pattern. Collagen’s chemicalproperties give leather its distinc-tive porosity or breathability. As aresult, leather can absorb up to 30percent of its weight in water vaporwithout feeling wet. Tanning alsogives leather the ability to retain itsshape and resist the aging process.The refinement of high perfor-mance leather has resulted in fea-tures that include improved waterrepellency, low water absorption,fast and soft drying, and durability.
Other advantages of leather or-thoses include the fact that leatherconforms to foot contours and bony
Continued on page 133
132 www.podiatrym.comPODIATRY MANAGEMENT • SEPTEMBER 2004
Foot Function...
of the body that move.10 Inthe field of podiatric orthope-
dics, the terms orthoses and or-thotics are used to describe a widerange of devices that are placed in-side the shoe. Other terms used fororthoses include inserts, insoles, in-lays, supports, and cushions.
The three basic types of foot or-thoses are pre-fabricated, cus-tomized, and custom-molded. Apre-fabricated orthosis is one that ismass-produced and is intended tobe dispensed to the user withoutmodification. Pre-fabricated or-thoses are usually designed to pro-vide either increased support orshock absorption for a specific areaof the foot, such as an arch supportor heel cushion. They may also pro-vide cushioning to the entire foot,as is the case with the use of a fullinsole.
A customized orthosis usuallyconsists of a pre-fabricated basecomponent that is modified insome way, such as adding ametatarsal pad or heel lift. A cus-tom-molded orthosis is one madefrom a model of the patient’s footmade from some form of three-di-mensional impression-taking proce-dure. These devices are used for pa-tients with more severe or compli-cated foot problems. They are com-monly composed of a shell, thelayer of material next to the footand in total contact with the foot,and posting material, filling thespace between theshell and theshoe. Custom or-thoses can be fur-ther modified byadding materialsto the top of theshell to either re-distribute pressureor provide cush-ioning.
Foot orthosesare often de-scribed as being either accommoda-tive or functional. An accommoda-tive orthosis is designed primarilyto accommodate a rigid foot or footdeformity, or one that is a risk,while a functional orthosis is de-signed to realign a more flexiblefoot by providing joint stabilityand support. In reality, most or-
Contin
uing
Medica
l Edu
catio
n
Foot orthosesare often described as
being eitheraccommodative or
functional.
The benefits ofleather as an orthotic
material are adirect result
of its intrinsic naturalcharacteristics.

SEPTEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 133
wedges and lifts.Korex is a cork latexmixture manufac-tured by Armstrong.Thermocork (ApexFoot Health Indus-tries, Teaneck, NJ) isthe only heat moldedproduct in this groupand is available inthicknesses measur-ing 1/8 to 3/8 inch.Rubber butter whichis composed of latexand leather grindingshas more shock atten-uating propertiesthan the latex andcork mixtures; how-ever, because of itsleather content, it issusceptible to agreater degree ofbreakdown over time8
These materials arealso effective whenused specifically asaccommodations, ei-ther in conjunctionwith a standard-length foot orthosisor alone.
Synthetic MaterialsThe synthetic ma-
terials used in the fab-rication of foot or-thoses were devel-oped to possess de-sired properties notfound in naturally oc-curring materials.
Polyethylene andP o l y p r o p y l e n eThermoplastics
Polyethylene is apolyolephin which issynthesized from themonomer ethyleneoxide. Polyethylene thermoplasticspossess the properties of toughnessand flexibility with good dimen-sional stability, are heat moldable,lightweight, and possess favorableweight/strength ratios. They aregenerally classified as being low,medium, high, or ultra-high densi-ty. They are available for orthosisfabrication primarily as Ortholenand Sub-Ortholen (Teufel,Stuttgard, Germany).
Ortholen is an extremely high
prominences and is well-toleratedby patients of all ages. Leather de-vices can be readily reshaped, re-modeled, and adjusted in the office.The disadvantages of leather or-thoses are that they tend to be morebulky than those made from ther-moplastics for a given degree of mo-tion control. They also tend to breakdown when worn by very active orobese individuals. While they canwithstand a limited amount ofmoisture, they do not hold up wellunder repetitive soaking.11
Rubber ButterRubber butter is a generic sub-
stance formulated by mixing liquidlatex with either cork, wood, orleather shavings, each producing aslightly different material. Rubberbutter-like materials are manufac-tured by several companies and areavailable under various tradenames. Cushion Cork (JMS Plastics,Neptune, NJ) is a latex and corkcombination available in sheetsthat are supplied in thicknessesmeasuring 1/6 to 1/2 inch, andcommonly used for fabricating
Foot Function... d e n s i t ythermoform-ing polyethy-lene with a molec-ular weight of onemillion. It is a verytough material whichis resistant to chemi-cal erosion and isnon-brittle at lowtemperatures. Ort-holen is available inthicknesses of 3 to 6mm., and is heatmolded by heating to350 degrees F. for 10to 15 minutes. Or-thoses fabricatedfrom Ortholen are in-dicated when a func-tional or semi-func-tional device is de-sired as it provides ef-ficient pronation con-trol in situationswhere a moderatelyflexible orthosis is re-quired. Sub-Ortholenis an ultra-high densi-ty thermoformingpolyethylene with amolecular weight of500,000. Although re-
lated to Ort-holen, it hasless toughnessand strengthbut is easierto mold byheating to300 degrees F.Sub-Ortholenis available inthicknesses of1 to 6 mm..8
Polypropy-lene is also apolyolephinsynthes izedfrom the
monomer ethylene oxide. As withpolyethylene, polypropylene is athermoplastic that is heat-formableand heat-adjustable at approxi-mately 360 to 390 degrees F.Polypropylene differs frompolyethylene in that it is a polymerof greater density and molecularweight, causing it to have a higherstiffness-to-thickness ratio. This re-sults in polypropylene having gen-erally less rapid and less severe plas-
Continued on page 134
Continuing
Medical Education
Carbon graphiteorthotic devices are
fabricated bylaminating verythin sheets of
carbon graphite fibercloths using aliquid resin.
Figure 1b. F-Scan recordingusing the shoe alone, demon-strating high pressure areasunder metatarsal heads
Figure 1a. F-Scan insole sensor beingplaced in an athletic shoe with themanufacturer’s supplied shoe sockliner.

Carbon GraphiteCarbon graphite orthotic de-
vices are fabricated by laminatingvery thin sheets of carbon graphitefiber cloths using a liquid resin. Thenumber of laminations varies de-pending on the strength desired,but for most foot orthosis applica-tions, the shell is approximately 2mm. in thickness. This produces athin rigid shell that is appreciablythinner than other thermoplasticorthoses.
TL-2100 (Performance Materi-als Corp., Camar-illo, CA) is man-ufactured withan acrylic-basedt h e r m o p l a s t i cresin system re-inforced withcarbon fiber andcombined in asandwich config-u r a t i o n .This allowst h e r m o -formabilityand heatadjustabili-ty similar tothat ofpolypropy-lene. Thegraphite re-
inforcement provides stiff-ness for support and strengthfor durability. There are fourversions of TL-2100 avail-able: Ultrastrength, sonamed because it is manufac-tured with approximately50% more graphite than theother versions, Rigid, Semi-Rigid, and Semi-Flexible.Thicknesses range from 1.8to 2.8 mm..9
Polyethylene FoamsPolyethylene foams are synthet-
ic materials also classified as poly-olefins. These are closed-cell foamsthat are nontoxic, resistant tochemicals and fluids, light, andwhen heated to suitable tempera-tures, are moldable. They are readi-ly washable and discourage bacteriagrowth. Orthotic shells may be fab-ricated using one type of polyethy-lene foam or by laminating differ-ent foams together. A variety ofpolyethylene foams are available inassorted durometers or hardnesses.Polyethylene foams are manufac-tured under different trade names,with each company implementingits own system to name the materi-als various durometers. Some of themore commonly encountered tradenames of polyethylene foams arePlastazote, Evazote, Pelite (allBakalite Xylonite LTD,{BXL}, UK),
and Aliplast( A l i m e d ,N e d h a m ,MA).6
Plastazotewas first usedas an orthoticmaterial byA m e r i c a npodiatrists in1969 after Dr.Paul Brandfound it to besuccessful forlimb preserva-tion in lep-rosy patients.Plastazote isheat-moldableat 140 degreesF. and is self-accommodat-ing to lesionsand bonyprominencesas well asbeing verylightweight.Plastazote isavailable inthicknesses of1/16 to oneinch. It is alsoavailable inthree durome-ters: medium,firm, and
134 www.podiatrym.comPODIATRY MANAGEMENT • SEPTEMBER 2004
Foot Function...
tic, or shape, deformationthan the polyethylenes.9
RohadurRohadur nylon acrylic is a
copolymer consisting of methyl-methacrylate and acrylonitrile. Itwas first developed for orthopedicuse by the Rohm Haas Company ofGermany in 1951 as Thermolast-1.Sheets of this material were market-ed by various companies undersuch trade namesas Plexidur, Nylo-plex, Sadur, andCyrodur (all JMSPlastics, Neptune,NJ). In 1976,T h e r m o p l a s t - 1was found to bepossibly carcino-genic in its manu-facturing processand was thereforereformulated anda new Rohadurresin was intro-duced as Thermo-last-II. Rohadurthermoplastic isheat moldableand indicated fororthotic devicesin which functional control is desired.
In addition to its use in fabricat-ing orthoses to control pronation,Rohadur is commonly used in thefabrication of gait plates, which areused in the treatment of in-toe gait.Rohadur is available in sheets mea-suring 2, 2.5, 3, 3.5, 4, 5, and 6mm. in thickness, with the 3 to 4mm. thickness most frequentlyused.8
Contin
uing
Medica
l Edu
catio
n
Poron retainsits form stability
and always returns toits original position,
even after permanentload, while
polyethylene foamssuch as Plastazote tend
to permanentlycompress or “bottom
out.”
Figure 2b. F-Scan recordingwith functional orthosis inathletic shoe. Note the sig-nificant decrease in sub-metatarsal pressure, but in-crease in pressure plantarhallux, probably due to im-proved foot biomechanicswith propulsion through cen-ter of hallux.
Figure 2a. Functional foot orthosis made with a polyethylene shell, neo-prene rearfoot posting, 1/16” Poron top cover, and 1/8” Poron forefootextension to toes
Continued onpage 135

SEPTEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 135
culate accord-ing to theweight lying onthe material.
Poron re-tains its formstability and al-ways returns toits original posi-tion, even afterp e r m a n e n tload, whilepolyethylenefoams such as
rigid. The medium and firm durome-ters are commonly used in the fabri-cation of accommodative and dy-namic insoles, while the rigid durom-eter is used in the fabrication of semi-functional orthotic devices. Evazoteis available in only one durometerwhich is very self-accommodatingand lightweight. Pelite is available infour durometers and is commonlyused as a liner for prosthetics. Aliplastis comparable to Plastazote and sup-plied in four durometers.8
Polyurethane FoamsPolyurethane foam is a ther-
mosetting, non-heat-moldable foamthat is manufactured either as anopened or closed-cell foam. Theopened-cell type is the most com-monly used. Poron, an open-cellpolyurethane foam made from acombination of polyether andpolyester resins, was developed bythe Rogers Company of Connecticututilizing a patented process. It is usedwherever the reduction of pressurefrom static ord y n a m i cforces is to beachieved, asin the pro-duction offoot orthosesor shoe in-lays. Thispolyurethanefoam is stablein form, elas-tic, shock-ab-sorbing, odor-less, andwashable. Asan opened-cell foam,medical gradePoron dissi-pates heatwell, and bya l l o w i n gwater vaportransmission,enables per-spiration tobe transmit-ted awayfrom the foot.This opened-cell naturealso allowsthe air to cir-
Foot Function... Plastazote tend topermanently com-press or “bottom out.”When used as a shock-at-tenuating soft tissue supple-ment for the plantar aspectof the foot, it is available inthicknesses ranging from1/16 to 1/2 inch in a singledurometer. The material ismanufactured both perforat-
Continued on page 136
Continuing
Medical Education
Figure 4a. Accommodative foot orthosis made with a 2-ply leather shellplaced on firm Plastazote with a 1/8” Poron forefoot extension.
Figure 4b. F-Scan recordingwith accommodative orthosisin athletic shoe. Note decreasein submetatarsal pressure ascompared to shoe alone, butnot as great a decrease aswith the functional or semi-functional devices. Note alsothe decrease in pressure onthe plantar hallux.
Silicone rubberoffers excellent
viscoelasticproperties capable
of providing shock absorption.
Figure 3b. F-Scan recordingwith semi-func-tional orthosisin athletic shoe.Note that thereis slightly lessdecrease in sub-metatarsal pres-sure than withthe functionalorthosis, but thedecrease in pres-sure plantar hal-lux is probably due to its less functional design.
Figure 3a. Semi-functional foot orthosis made with thinner polyethyleneshell, Poron longitudinal arch reinforcement, lower durometer neoprenerearfoot posting, 1/16” Poron top cover, and 1/8” Poron forefoot exten-tion to toes
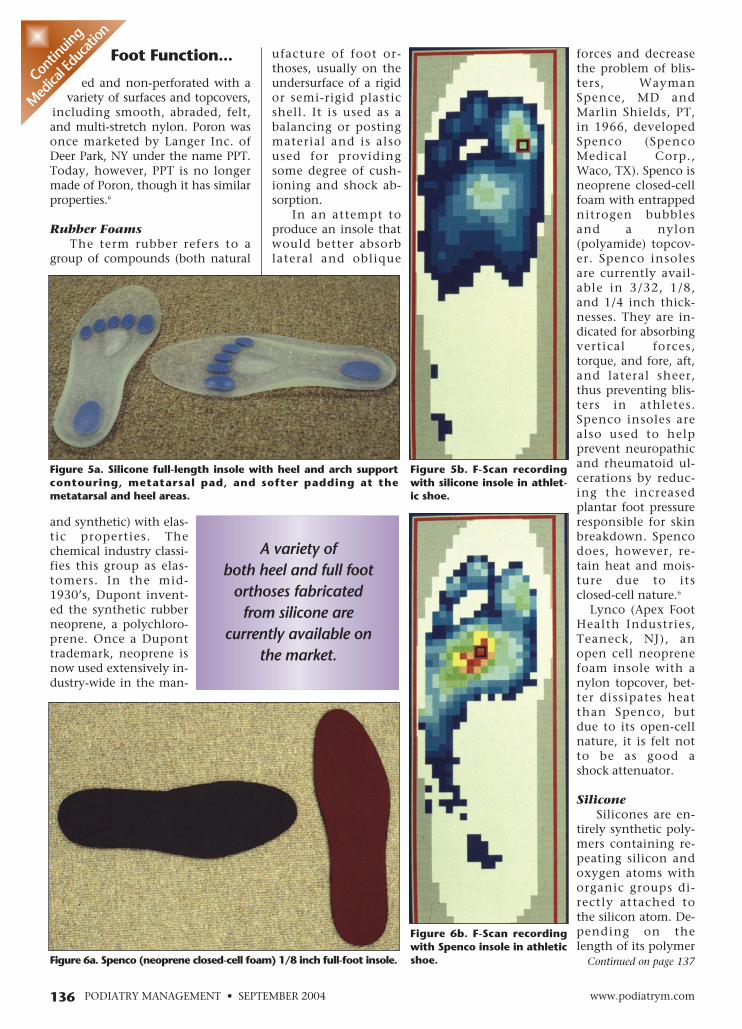
ufacture of foot or-thoses, usually on theundersurface of a rigidor semi-rigid plasticshell. It is used as abalancing or postingmaterial and is alsoused for providingsome degree of cush-ioning and shock ab-sorption.
In an attempt toproduce an insole thatwould better absorblateral and oblique
forces and decreasethe problem of blis-ters, WaymanSpence, MD andMarlin Shields, PT,in 1966, developedSpenco (SpencoMedical Corp.,Waco, TX). Spenco isneoprene closed-cellfoam with entrappednitrogen bubblesand a nylon(polyamide) topcov-er. Spenco insolesare currently avail-able in 3/32, 1/8,and 1/4 inch thick-nesses. They are in-dicated for absorbingvertical forces,torque, and fore, aft,and lateral sheer,thus preventing blis-ters in athletes.Spenco insoles arealso used to helpprevent neuropathicand rheumatoid ul-cerations by reduc-ing the increasedplantar foot pressureresponsible for skinbreakdown. Spencodoes, however, re-tain heat and mois-ture due to itsclosed-cell nature.6
Lynco (Apex FootHealth Industries,Teaneck, NJ), anopen cell neoprenefoam insole with anylon topcover, bet-ter dissipates heatthan Spenco, butdue to its open-cellnature, it is felt notto be as good ashock attenuator.
SiliconeSilicones are en-
tirely synthetic poly-mers containing re-peating silicon andoxygen atoms withorganic groups di-rectly attached tothe silicon atom. De-pending on thelength of its polymer
Continued on page 137
136 www.podiatrym.comPODIATRY MANAGEMENT • SEPTEMBER 2004
Foot Function...
ed and non-perforated with avariety of surfaces and topcovers,
including smooth, abraded, felt,and multi-stretch nylon. Poron wasonce marketed by Langer Inc. ofDeer Park, NY under the name PPT.Today, however, PPT is no longermade of Poron, though it has similarproperties.6
Rubber FoamsThe term rubber refers to a
group of compounds (both natural
and synthetic) with elas-tic properties. Thechemical industry classi-fies this group as elas-tomers. In the mid-1930’s, Dupont invent-ed the synthetic rubberneoprene, a polychloro-prene. Once a Duponttrademark, neoprene isnow used extensively in-dustry-wide in the man-
Contin
uing
Medica
l Edu
catio
n
A variety ofboth heel and full foot
orthoses fabricated from silicone are
currently available onthe market.
Figure 6b. F-Scan recordingwith Spenco insole in athleticshoe.
Figure 5b. F-Scan recordingwith silicone insole in athlet-ic shoe.
Figure 6a. Spenco (neoprene closed-cell foam) 1/8 inch full-foot insole.
Figure 5a. Silicone full-length insole with heel and arch supportcontouring, metatarsal pad, and softer padding at themetatarsal and heel areas.

SEPTEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 137
as quickly as other ma-terials used for thesame purpose, thusmaking it an excellentsubstitute for the natu-ral viscoelastic bodytissues. Silicone rubberhas the ability of re-maining flexible atvery low temperaturesand is not distorted byheat up to 400 degreesC. (752 degrees F). Or-thoses made from sili-cone can be heatedand cooled without
chain and the degree of cross-link-ing, silicone can be present inmany different types of commercialproducts ranging from fluids torubbers. Silicone rubbers are com-positions containing a high-molec-ular-weight dimethyl silicone linearpolymer and are commonly used inthe fabrication of foot orthoses.Products containing silicon poly-mers tend to be relatively expen-sive. In the case of orthotic devices,those made of true silicone tend tobe more costly than similar prod-
ucts made from othermaterials such as poly-urethane foams. Sili-cone, however, hasmany properties thatmake it highly desirablefor use in the manufac-ture of orthoses.
Silicone rubber offersexcellent viscoelasticproperties capable ofproviding shock absorp-tion by dissipating theenergy evading the bodyduring ambulation. Itaccomplishes this taskwithout bottoming out
Foot Function... drying orc r a c k i n g .Other impor-tant characteris-tics include a highdegree of chemicalinertness which al-lows the silicone de-vices to be soaked inmany types of solu-tions for both clean-ing and disinfectingwithout loss of anyfunction. This chem-ical inertness also re-duces the chance ofallergies upon con-tact with the skinand does not sup-port bacterial growthor odor. They dotend to have the dis-advantage that theyretain heat and can-not be ground foradjusting.2
A variety of bothheel and full foot or-thoses fabricatedfrom silicone arecurrently availableon the market. Al-though they differsomewhat in appear-ance, they are all de-signed primarily forboth shock attenua-tion and weight dis-persion. Several ofthe silicone orthosesincorporate preciselypositioned softerpadding, targetingthe metatarsal andheel regions of thefoot where shockload is highest. Somefull-length insolesalso include contour-ing that providesboth heel and archsupport, as well asshock absorption.
Evaluating theEffects of Orthosesand Insoles on FootFunction
Recent techno-logical advance-ments have providedobjective methods of
Continued on page 138
Continuing
Medical Education
Figure 8a. Poron (opened-cell polyurethane foam) 1/4 inch full-foot insole.
Figure 7a. Poron (opened-cell polyurethane foam) 1/8 inch full-foot insole.
Figure 8b. F-Scan recordingwith Poron 1/4 inch insole inathletic shoe.
Figure 7b. F-Scan recordingwith Poron 1/8 inch insole inathletic shoe.
Many studiesalso linked excessive
sub-metatarsal pressure associated with the peripheral neuropathy seen in
diabetes as a cause of plantar pedal
ulceration.

that results from a contracted ham-mertoe condition. The plantarweight-bearing area under themetatarsal often begins to form aprotective callus, and eventually adeep, painful plantar keratoma maydevelop.3,4 Many studies have alsolinked excessive sub-metatarsalpressure associated with the periph-eral neuropathy seen in diabetes asa cause of plantar pedal ulceration.With loss of normal sensation, thediabetic fails to be aware of exces-sive plantar pressure.1
Metatarsal stress fractures arealso the result of increased repeti-tive pressure on the sub-metatarsalarea of the foot. These were initiallythe most commonly diagnosedstress fractures when they werethought to occur only in militaryrecruits. Although these fracturesremain relatively common in the
military, they also involve a signifi-cant number of athletes.7 The pres-ence of diabetes appears to result inthe increased prevalence ofmetatarsal stress fractures in theathlete. The most frequently frac-tured of the metatarsal bones arethe second and third.1
The Use of Orthoses and Insolesin the Management of ExcessiveLesser Metatarsal PlantarPressure
The following figures demon-strate the effects of various foot or-thoses and insoles on the plantarpedal pressure of a patient exhibit-ing excessive sub-lesser metatarsalplantar pressure. F-Scan readingswere taken at the push-off phase ofgait when the sub-lesser metatarsalpressure was at its peak. The mea-surements were recorded using theF-Scan In-Shoe sensor with the pa-tient wearing an all-purpose typeathletic shoe. The readings were
taken first with the shoe alone con-taining the manufacturer-suppliedshoe sockliner, then with varioustypes of foot orthoses and insolesreplacing the sockliner. The or-thoses were custom made from animpression cast of the patient’s feetand fabricated from a variety ofboth natural and synthetic materi-als as described. They representwhat would be considered eitherfunctional, semi-functional, or ac-commodative devices. The insolesare made of some of the varioustypes of biomaterials described inthis paper.
References1 Caselli MA. Foot management guide-
lines for the diabetic athlete. Podiatry Man-agement 17(9): 45-58, 1998.
2 Caselli M. Silicone. Biomechanics2(1): 55-58, 1995.
3 Caselli MA, George DH. Foot deformi-ties: biomechanical and pathomechanicalchanges associated with aging, part 1. ClinPodiatr Med Surg 20(3): 487-509, 2003.
4 Caselli MA, Levitz SJ, Clark N, LazarusS, Valez Z, Venegas, L. Comparison of Vis-coped and Poron for painful submetatarsalhyperkeratotic lesions. JAPMA 87(1) 6-10,1997.
5 Janisse DJ. Orthoses, shoewear, andshoe modifications. In: Myerson MS(ed).Foot and Ankle Disorders. Philadelphia: WBSaunders Co.; 2000. pp 195-212
6 Jones LS, Caselli M. Foam zone.Biomechanics 3(1): 73-77, 1996.
7 Leach RE, Zecher SB. Stress fractures.In: Guten GN(ed). Running Injuries.Philadelphia: WB Saunders Co.; 1997. pp30-46
8 Levitz SJ, Whiteside LS, Fitzgerald TA.Biomechanical foot therapy. Clin PodiatrMed Surg 5(3): 721-736, 1988.
9 Olson WR. Orthotic materials. In Val-massy RL(ed). Clinical Biomechanics of theLower Extremities. St. Louis: Mosby; 1996.pp 307-326
10 Pedorthic Footwear Association: Pe-dorthic Definitions. Columbia, MD: Pedor-thic Footwear Association; 1996.
11 Pribut S. Leather as an orthotic mate-rial. Biomechanics 4(4): 61-65, 1997.
138 www.podiatrym.comPODIATRY MANAGEMENT • SEPTEMBER 2004
Foot Function...
accurately determining the ef-fects of orthoses and insoles on
specific features of foot function,specifically pedal plantar pressure.In order for a device to be of valuein assessing pedal plantar pressure,it must be capable of measuring thepressure at the shoe-foot interfaceor the orthotic/insole-foot interfaceduring ambulation. There are cur-rently a number of systems on themarket that are capable of accom-plishing this task.
One of the commonly used sys-tems is the F-Scan In-Shoe System(Tekscan, Inc., Boston, MA). Thissystem utilizes an ultra thin(7/1000 in.) pressure sensitive in-sole sensor containing 960 individ-ual pressure sensing points. The F-Scan software records and calcu-lates stance times and pressures atthe shoe-foot interface. Increasingpressure is depicted by colorchanges ranging from violet (lowestpressure) to red (highest pressure)along the standard color spectrum.In-shoe plantar pressure can thusbe a valuable tool in detecting bothareas of increased plantar pressureand the ability of shoegear, insoles,and orthoses to off-load these high-pressure areas.1
One of the most common areasof the foot that is associated withpathology due to excessive pres-sure, especially during the push-offphase of gait, is the plantar surfaceof the lesser metatarsals. Condi-tions such as metatarsalgia, hyperk-eratosis, ulcerations, and stress frac-tures have been attributed to exces-sive pressure in this area.
Metatarsalgia is described as alocalized or generalized pain in theregion of the distal aspect of one ormore of the metatarsals duringweight bearing. Pain may be the re-sult of either positional or func-tional malalignment of themetatarsals. The most commontype of metatarsalgia involves along lesser metatarsal bone (typical-ly second or third) that projectspast the theoretically perfect curve.The increased pressure and frictionfrom this long metatarsal occurduring the push-off phase of gait,when the foot is fully loaded.Metatarsalgia may also be causedby a plantar-flexed lesser metatarsal
Contin
uing
Medica
l Edu
catio
n
Dr. Caselli is StaffPodiatrist at theVA Hudson Val-ley Health CareSystem and isAdjunct Profes-sor at NYCPM.He is a Fellow ofthe AmericanCollege of SportsMedicine.
Metatarsal stressfractures are also the
result of increasedrepetitive pressure on
the sub-metatarsal areaof the foot.

SEPTEMBER 2004 • PODIATRY MANAGEMENTwww.podiatrym.com 139
ed and reshapedC) They tend to be morebulky than those made fromthermoplasticsD) They are poorly toleratedby patients
6) Rubber butter is a genericsubstance formulated by mixingliquid latex with all but whichone of the following?
A) CorkB) Plastic shavingsC) Leather shavingsD) Wood
7) Which one of the following isnot a property of the polyethy-lene thermoplastics?
A) Good shock absorberB) Dimensional stabilityC) Light weightD) Durable
8) Ortholen and Sub-Ortholenare polyethylene thermoplasticsthat are heat moldable at whattemperatures?
A) 100 to 150 degrees F.B) 200 to 250 degrees F.C) 300 to 350 degrees F.D) 450 to 500 degrees F.
9) Foot orthoses made frompolypropylene thermoplastic canbe made thinner than thosemade from polyethylene becauseof polypropylene’s:
A) Higher heat moldabletemperatureB) Greater density andmolecular weightC) Lighter colorD) Rougher surface
10) The material most commonlyused for the fabrication of gaitplate orthoses is:
1) A pre-fabricated orthotic de-vice that is modified to meet aspecific patient’s needs is consid-ered:
A) A pre-fabricated orthosisB) A customized orthosisC) A custom orthosisD) An insole
2) Which one of the followingcannot be accomplished with theuse of foot orthoses?
A) Reduce shockB) Limit motion of jointsC) Mobilize rigid jointsD) Stabilize and supportjoints
3) Which one of the followingrepresents an example of a softmaterial that might be used inthe fabrication of a foot ortho-sis?
A) Opened cell polyurethanefoamB) Polyethylene thermoplas-ticC) RohadurD) Sub-Ortholen
4) One of the advantages ofusing leather in the fabricationof foot orthoses is its breathabili-ty. This property is due to:
A) Special tanning processused in preparing leatherB) Thinness of leatherC) The lamination method offabricating leather orthosesD) The three-dimensionalpattern of leather’s collagenfibers
5) The primary disadvantage ofleather foot orthoses is that:
A) They conform to foot con-tours and bony prominencesB) They can be easily adjust-
A) Rigid PlastazoteB) Sub-OrtholenC) Polypropylene thermoplas-ticD) Nylon acrylic
11) Polyethylene foams are com-monly used to fabricate orthosesand insoles for neuropathic dia-betic patients due to which oneof the following properties?
A) Availability in varyingthicknessesB) Heat-moldabilityC) Self-accommodating na-tureD) Lightweight
12) Which one of the followingis not a property of polyurethanefoams?
A) Heat-moldableB) Good shock absorbersC) Do not permanently de-formD) Dissipate heat
13) Poron polyurethane foam al-lows perspiration to be transmit-ted away from the foot due toits:
A) Good shock-attenuatingpropertiesB) Opened-cell natureC) Multistretch coverD) Elasticity
14) The synthetic rubber neo-prene is primarily used in themanufacture of foot orthoses as a:
A) TopcoverB) Forefoot extensionC) Posting materialD) Shell
15) Spenco, a neoprene foam,
Continuing
Medical Education
E X A M I N A T I O N
See answer sheet on page 141.
Continued on page 140
140 PODIATRY MANAGEMENT • SEPTEMBER 2004
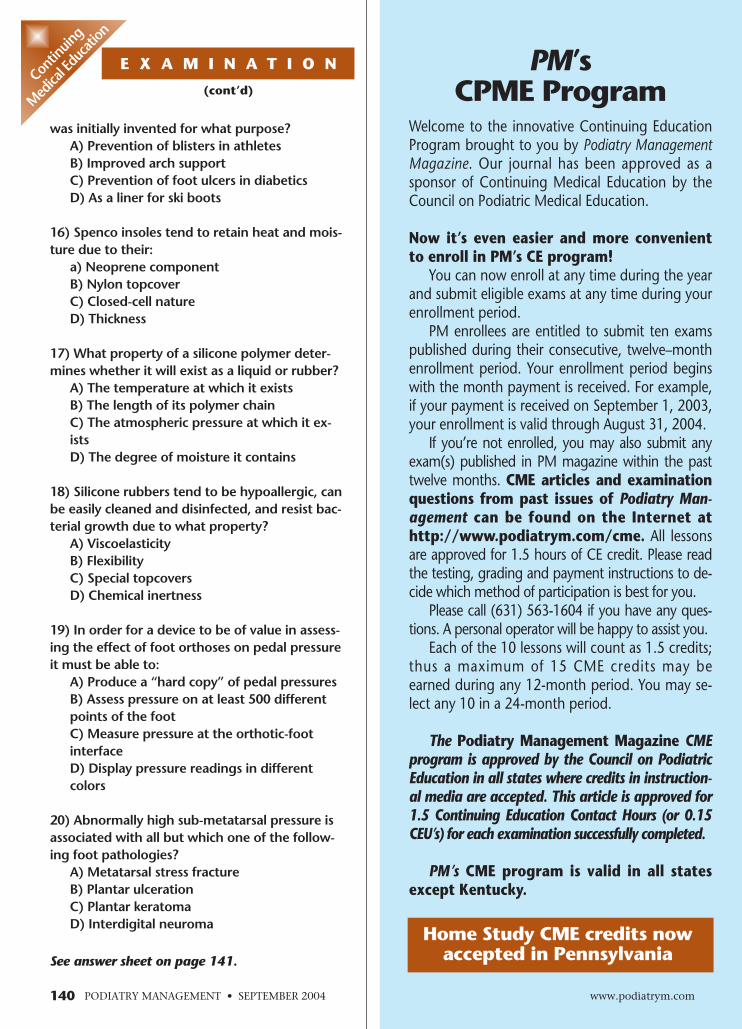
was initially invented for what purpose?A) Prevention of blisters in athletesB) Improved arch supportC) Prevention of foot ulcers in diabeticsD) As a liner for ski boots
16) Spenco insoles tend to retain heat and mois-ture due to their:
a) Neoprene componentB) Nylon topcoverC) Closed-cell natureD) Thickness
17) What property of a silicone polymer deter-mines whether it will exist as a liquid or rubber?
A) The temperature at which it existsB) The length of its polymer chainC) The atmospheric pressure at which it ex-istsD) The degree of moisture it contains
18) Silicone rubbers tend to be hypoallergic, canbe easily cleaned and disinfected, and resist bac-terial growth due to what property?
A) ViscoelasticityB) FlexibilityC) Special topcoversD) Chemical inertness
19) In order for a device to be of value in assess-ing the effect of foot orthoses on pedal pressureit must be able to:
A) Produce a “hard copy” of pedal pressuresB) Assess pressure on at least 500 differentpoints of the footC) Measure pressure at the orthotic-footinterfaceD) Display pressure readings in differentcolors
20) Abnormally high sub-metatarsal pressure isassociated with all but which one of the follow-ing foot pathologies?
A) Metatarsal stress fractureB) Plantar ulcerationC) Plantar keratomaD) Interdigital neuroma
E X A M I N A T I O N
(cont’d)
See answer sheet on page 141.
Contin
uing
Medica
l Edu
catio
n
PM’sCPME Program
Welcome to the innovative Continuing EducationProgram brought to you by Podiatry ManagementMagazine. Our journal has been approved as asponsor of Continuing Medical Education by theCouncil on Podiatric Medical Education.
Now it’s even easier and more convenientto enroll in PM’s CE program!
You can now enroll at any time during the yearand submit eligible exams at any time during yourenrollment period.
PM enrollees are entitled to submit ten examspublished during their consecutive, twelve–monthenrollment period. Your enrollment period beginswith the month payment is received. For example,if your payment is received on September 1, 2003,your enrollment is valid through August 31, 2004.
If you’re not enrolled, you may also submit anyexam(s) published in PM magazine within the pasttwelve months. CME articles and examinationquestions from past issues of Podiatry Man-agement can be found on the Internet athttp://www.podiatrym.com/cme. All lessonsare approved for 1.5 hours of CE credit. Please readthe testing, grading and payment instructions to de-cide which method of participation is best for you.
Please call (631) 563-1604 if you have any ques-tions. A personal operator will be happy to assist you.
Each of the 10 lessons will count as 1.5 credits;thus a maximum of 15 CME credits may beearned during any 12-month period. You may se-lect any 10 in a 24-month period.
The Podiatry Management Magazine CMEprogram is approved by the Council on PodiatricEducation in all states where credits in instruction-al media are accepted. This article is approved for1.5 Continuing Education Contact Hours (or 0.15CEU’s) for each examination successfully completed.
PM’s CME program is valid in all statesexcept Kentucky.
www.podiatrym.com
Home Study CME credits nowaccepted in Pennsylvania