Ortho Patho Meet on Fibrous Dyspalsia by Dr. Saumya Agarwal
44
ORTHO PATHO MEET PRESENTER : Dr. SAUMYA AGARWAL Junior resident Dept of Orthopaedics J.N.Medical College and Dr. Prabhakar Kore Hospital and MRC, Belgaum
-
Upload
kles-jn-medical-college-and-dr-prabhakar-kore-hospital-and-medical-research-centre -
Category
Health & Medicine
-
view
193 -
download
0
Transcript of Ortho Patho Meet on Fibrous Dyspalsia by Dr. Saumya Agarwal

ORTHO PATHO MEET
PRESENTER : Dr. SAUMYA AGARWAL
Junior resident Dept of Orthopaedics J.N.Medical College and Dr. Prabhakar Kore Hospital and MRC, Belgaum

NAME : XYZ
AGE : 20 Yrs
SEX : MALE I.P NO. : 659161
ADDRESS : RESIDENT OF BELGAUM
OCCUPATION : FARMER

CHIEF COMPLAINTS
Patient complaints of pain at right hip while working for a long time since 4 months.

HISTORY OF PRESENTING ILLNESS
• Patient was apparently alright 4 months back when
he started complaining of pain in right hip.
• Pain was insidious in onset, gradually progressive,
aggravated on working and relieved on rest.

• No history of :1) Trauma / injury at the site of deformity2) Fever3) Significant Loss of body weight4) Steroid intake5) Other joint pain

PAST HISTORY
• No history of similar complaints in the past.
• Not a Known case of Diabetes Mellitus, Hypertension
and Ischemic heart disease.
• Not a known case of Tuberculosis, hyperthyroidism and
other chronic illness.
FAMILY HISTORY
• Nothing significant

PERSONAL HISTORY
• Diet : Mixed
• Appetite : Not decreased
• Sleep : Undisturbed
• Bowel & Bladder : Normal and regular
• Takes alcohol occasionally , non smoker

GENERAL EXAMINATION
• Patient is conscious, cooperative and well oriented to time , place and person .
• Moderately built• Afebrile• Pulse – 76 /min• Blood pressure - 116/80 mmHg• Respiratory rate – 20 / min• No pallor / cyanosis / edema / icterus /
clubbing / lymphadenopathy

SYSTEMIC EXAMINATION
• CVS : S1 S2 heard, No murmurs
• RS : Air entry equal on both sides
• PA : Soft, Non tender, no organomegaly, Bowel
. sounds heard
• CNS : No focal neurological deficit

LOCAL EXAMINATION
• Gait – normal
• Attitude – neutral
• INSPECTION – Left Hip – normal
• Right hip -
• No any swelling / sinus / scar / discharge / inflammatory
changes
• No evidence of shortening of both lower limbs.

• PALPATION –
• No any local rise of temperature
• No Tenderness – present over the right hip
• Range of movement of right hip – normal
• Range of movement of right knee – normal
• No muscle wasting
• Toe movements – present
• Distal pulses – felt on both sides
• No neurological deficit

INVESTIGATIONS
• Hb – 12.4 gm%• TLC – 8920/ cumm• RBC - 4,50000 / cumm• ESR – 14• Platelet count – 2,53000/ cumm• PCV - 36.3• Blood Group – B +

• S. Creatinine – 0.9
• Blood Urea – 19
• S. Sodium – 138 meq/l
• S. Potassium – 4.8 meq/l
• S. Calcium - 9.8
• S. Alkaline phosphatase – 300

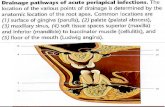
X-Ray Pelvis AP view Showing Right Hip

X-Ray Right Hip lateral view

X-Ray Findings
• A lytic lesion seen in neck of femur showing well defined geographic type of destruction with sclerotic rim.
• Intramedullary radiolucencies with haziness seen.

DIFFERENTIAL DIAGNOSIS
1) Osteo fibrous dyspalsia2) Osteoid Osteoma3) Osteochondroma4) Non Ossifying Fibroma5) Fibrous Dysplasia6) Unicameral bone cyst7) Aneurysmal bone cyst

1) Osteo fibrous dyspalsia
Points in Favour : Age : 1st and 2nd decades Male preponderence Imaging : eccenteric intracortical osteolysis with
expansion of cortex
Points Against : pain is absent Site : diaphysis of long bones


2) Osteoid Osteoma Points in Favour :• Age : 2nd and 3rd decades• Male : female :: 3:1• Site : lower extremity, long bones, diaphyseal/
metaphyseal• Pain Points Against :• Imaging : cortical radiolucent nidus <1.5cm
with marked cortical thickening


3) Oteochondroma Points in Favour : Age : 2nd and 3rd decades Male preponderence Site : metaphysis of long bones
Points Against : Mass is present Imaging : pedunculated or sessile bone
lesion that communicates with intramedullary canal


4) Non Ossifying Fibroma Points in Favour :• Age : 1st and 2nd decades• Site : Metaphysis of long bones• Asymptomatic
Points Against :• Imaging : geographic , eccentric lesion located
in metaphysis of long bones well defined sclerotic margins.


5) Fibrous Dysplasia Points in Favour : • Age : 1st to 3rd decades• Male : female :: 1:1• Site : femur, tibia• Pain• Imaging : ground glass appearance with well
defined sclerotic rim


6) Unicameral Bone Cyst Points in Favour :• Age : 1st and 2nd decades• Male : female :: 2:1• Site : proximal femur, proximal humerus• Asymptomatic unless pathological fracture
Points against: • Imaging : centrally located , purely radiolucent
lesion , no cortical destruction.


7) Aneurysmal Bone Cyst
Points in Favour :• Age : 1st – 2nd decades• Pain
Points Against :• Female preponderence• Site: proximal humerus, distal femur, proximal
tibia, spine• Imaging : eccentric expansile radiolucent lesion


Fibrous Dysplasia
HISTORY :• The term fibrous dysplasia was originally
proposed by Lichtenstein in 1938.• He along with Jaffe, McCune, and Albright,
described this disorder of bone, as well as other extra skeletal abnormalities with which it is occasionally associated.

DEFINITION :• Fibrous Dysplasia is a benign, nonfamilial
disorder characterized by the presence of expanding intramedullary fibro-osseous tissue in one or more bones.
INCIDENCE :• Not known• Accounts for 5-7% of clinical benign tumors • Occur more frequently in girls than boys

AGE :• Affects 1st - 3rd decades
SITE :• Fibrous dysplasia can affect any bone • Femur and Tibia being most common

HISTOPATHOLOGY
• Irregular woven bone spicules with a fibrous stroma.
• Trabeculae of woven bone surrounded by cellular fibroblastic tissue.
• There is no osteoblastic rim at the bone-stromal interface.


• Fibrous Dysplasia can be classified into one of four categories :
1. Monostotic : single bone2. Polyostotic : multiple bones3. Craniofacial fibrous dysplasia : skull and facial
bones alone4. Mandible and maxilla alone

CLINICAL PRESENTATION
• Pain• Deformity• Cutaneous pigmentation• Endocrine abnormalities

IMAGING
• Ground glass appearance with well defined sclerotic rim
• may be completely lucent (cystic) or sclerotic• well circumscribed lesions• no periosteal reaction


TREATMENT
• Prophylactic fixation of impending fractures• Correction of deformity• Bisphosphonates for severe cases

McCune-Albright Syndrome
• The triad of :• precocious puberty (endocrinopathy), • Café au lait spots, and • polyostotic bone involvement

Mazabraud syndrome
• Mazabraud’s syndrome is a rare disorder characterized by fibrous dysplasia, which can develop in a single bone (monostotic) or in multiple bones (polyostotic), associated with one or more soft-tissue myxomas.