Orphans and Vulnerable Children Brochurebehaviour change using HIV prevention messages...
28
IMPROVEMENTS INTHE LIVES OF SOUTH AFRICAN ORPHANS AND VULNERABLE CHILDREN “Without the drop-in centre, I wouldn’t be here. I would have long ago left school or maybe I could have long ago died of hunger and poverty and diseases.” —A teenaged orphan FROM THE CHILDREN’S MOUTHS IPHC INTEGRATED PRIMARY HEALTH CARE PROJECT
Transcript of Orphans and Vulnerable Children Brochurebehaviour change using HIV prevention messages...

ImProVementS In tHe lIVeS oFSoUtH aFrICan orPHanS andVUlneraBle CHIldren
“Without the drop-in centre, I wouldn’t behere. I would have long ago left school ormaybe I could have long ago died ofhunger and poverty and diseases.”
—A teenaged orphan
FROMTHECHILDREN’SMOUTHS
IPHCIntegrated PrImary HealtH Care ProjeCt

ACKNOWLEDGMENTS
management Sciences for Health (mSH) thanks all the children and organisationsinvolved in the research for this report. In particular the orphans and vulnerablechildren (oVC) and caregivers at Inkwanca Home Based Care in Chris Hanidistrict, and Khanyiselani development trust and masakhane Women’sorganisation in Sisonke district.
mSH extends its appreciation to glynis Clacherty and associates for conductingthe field research and working with the mSH oVC technical advisor, rodwellShamu, in compiling this report. Special mention goes to Kgetheng dlamini forinterviewing and recording the children’s voices and translating them fromvernacular languages.
mSH is grateful to the United States agency for International development(USaId) for the support under the US President’s emergency Plan for aIdSrelief (PePFar).the funding supports the delivery of comprehensive servicesfor oVC and the research for and publication of this report.
mSH endeavours to continue strengthening South african community-basedorganisations to meet the objective of helping oVC to live normal andproductive lives.
n. mazaleniChief of Party, management Sciences for Health, South africa
this booklet is a project ofthe national department ofHealth and is made possibleby the support of theamerican people throughthe United States agency forInternational development(USaId).the contents arethe sole responsibility of theIntegrated Primary HealthCare (IPHC) Project and donot necessarily reflect theviews of USaId or theUnited States government.
COVER PHOTO AND PHOTO BELOW BY MSH STAFF
1
BACKGROUND&METHODS . . . . . . . . . . . . . . . . . . . . . . . .2
the IPHC Project: Helping orphans andVulnerableChildren . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Interviewing Children . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Why Collect Children’sVoices? . . . . . . . . . . . . . . . . . .4methods Used by glynis Clacherty and associates . . .4ethical Considerations . . . . . . . . . . . . . . . . . . . . . . . . .4the activities Used to elicit the Children’s opinions 5
THECHILDREN SPEAK . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6Hardships I Faced Before Finding the Centre . . . . . . . . . . .6I get Help with my education . . . . . . . . . . . . . . . . . . . . . .6I get Help with my Homework . . . . . . . . . . . . . . . . . . . . .7the Food Is good Here . . . . . . . . . . . . . . . . . . . . . . . . . . .8I go on outings and Picnics . . . . . . . . . . . . . . . . . . . . . . . .9I take trips . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9I enjoy different, Fun activities . . . . . . . . . . . . . . . . . . . . . .9I learn Important life Skills . . . . . . . . . . . . . . . . . . . . . . . .9I Found a Place to Call Home . . . . . . . . . . . . . . . . . . . . . .10I Have Someone to talk to . . . . . . . . . . . . . . . . . . . . . . . .11I Have the Company of other Children from myCommunity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11my Health Is Important Here . . . . . . . . . . . . . . . . . . . . . .11everyone Who IsVulnerable Is Welcome atthe Centre . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12I am Cared For and Protected . . . . . . . . . . . . . . . . . . . . .13I Feel good about myself . . . . . . . . . . . . . . . . . . . . . . . . .13
THEORGANISATIONSANDTHECENTRES . . . . . . . .14masakhane Women’s organisation . . . . . . . . . . . . . . . . . .14Inkwanca Home-Based Care . . . . . . . . . . . . . . . . . . . . . . .15
In Her Words . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16Khanyiselani development trust . . . . . . . . . . . . . . . . . . . .18
In Her Words . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20Centre Staff discuss mSH Support . . . . . . . . . . . . . . . . .22
CONCLUSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24
APPENDIX: Organisations Supported by theIPHC Project . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25
CONTENTS

The IPHC Project: HelpingOrphans and VulnerableChildren
In March 2006, with generous support fromUSAID and PEPFAR, MSH initiated perform-ance-based funding1 for an Orphans and
Vulnerable Children (OVC) Project through theIntegrated Primary Health Care (IPHC) Project.The OVC project started with six home-basedcare (HBC) organisations based in four provincesof South Africa. By December 2006, the number oforganisations had increased to 23, and coverage in-cluded five provinces and eight districts. (The ap-pendix lists these 23 organisations and theirlocations.)The organisations have drop-in centresfor children to come to after school and, in somecases, operate early learning or day care centresfor the younger children.
Since 2006 MSH has assisted more than 19,000OVC, using more than 9 million South African randin grant funding to the 23 organisations.The servicesrendered to these children include the following:
• CLINICALNUTRITION interventionsthat cover medical aspects of nutrition typi-cally associated with food insecurity (such asmalnourishment)
• FOOD PROVISION,mostly from soupkitchens, to children participating in activitiesat drop-in centres
• SHELTER interventions that include identify-ing potential caregivers or reintegrating chil-dren who are currently in institutional carethrough family tracing and foster care
• CHILD PROTECTION interventions thataim to minimise stigma and social neglect facedby OVC, as well as abuse and exploitation
2
NORTH WEST
LIMPOPO
MPUMALANGA
KWAZULUNATAL
FREESTATE
LESOTHO
GAUTENG
NORTHERNCAPE
WESTERNCAPE
EASTERNCAPE
CAPRICORN 2 1,421
SEKHUKHUNE 3 4,149
GERT SIBANDE 4 1,595
BOJANALA 5 3,338
UTHUNGULU 2 1,724
SISONKE 2 2,815
ALFRED NZO 1 471
CHRIS HANI 4 3,727
DISTRICTNAME
# OF OVCSERVED
# OFSITES
IPHC-SUPPORTED SITES OFFERING OVC SERVICES IN SOUTH AFRICASeptember 2008
Five Provinces, Eight Districts,23 Locations, and 19,240 OVC Served
BACKGROUND & METHODS
1 To maximize the impact of funding on the people it should serve, MSH uses performance-based grants to link a CBO’s financingwith its achievement of set targets.

3
• GENERAL HEALTHCARE services suchas referrals and linkages to child health care,immunization, growth monitoring, malaria pre-vention, and, when appropriate, HIV testing
• HEALTHCARE SUPPORT, specifically forantiretroviral therapy (ART).This service in-cludes prevention of mother-to-child trans-mission (PMTCT) or specialized paediatricART. Skin conditions, weight, and vital signs arealso monitored. Periodic CD4 and HIV testingfor all children and youth and paediatric ARTand ART-adherence interventions for HIV-positive OVC are also provided.
• HIV PREVENTION EDUCATION forbehaviour change using HIV preventionmessages
• PSYCHOSOCIALCARE to provide bothchildren and their caregivers with emotionalsupport
• GENERAL EDUCATION to ensure thatOVC stay in school over the short term. Di-rect assistance is provided to subsidizeschool-related costs such as fees, books, anduniforms.
• VOCATIONAL TRAINING that encour-ages access for OVC to learn a trade, such ascarpentry, welding, sewing, or agriculture
• ECONOMICOPPORTUNITY or eco-nomic strengthening that includes access tosocial grants, livelihood opportunities (e.g., in-come-generating activities, links with the pri-vate sector), small-business development, andactivities to create entrepreneurs from amongolder HIV & AIDS OVC and caregivers
In addition to funding, MSH has provided these 23organisations with both formal and informal technical
support.Through workshops and on-site coachingand mentoring during field visits, MSH has offeredtraining in project monitoring and management. MSHhas designed data collection and reporting tools andhas set up a reporting and documentation systemthat is used by the organisations.
This report focuses on the impact of work done inthree of the OVC projects supported by MSH:Inkwanca Home-Based Care (HBC) in Chris HaniDistrict, and Khanyiselani DevelopmentTrust(KDT) and Masakhane Women’s Organisation inSisonke District. More information about eachproject can be found beginning on page 14.
By eliciting first-hand experiences ofthese children, we can help assess theimpact of services provided toOVC.
PHO
TOBY
MSH
STA
FF
4
Interviewing Children
WHYCOLLECTCHILDREN’S VOICES?MSH commissioned Glynis Clacherty and Associ-ates for their expertise in participatory work withchildren. Glynis Clacherty and Associates talked toyoung people who are benefiting from three ofthe OVC programmes supported by USAID andPEPFAR through MSH’s IPHC Project. Reportsoften focus on the quantitative aspects of pro-grammes, but quantitative analysis is not the wholestory. Guided conversations with the beneficiariesof the OVC programmes help to demonstratequalitatively the programmes’ positive impact.
By eliciting the firsthand experiences of these chil-dren and their caregivers, we can help assess theimpact of services provided to OVC and identifysuccessful approaches to share with other stake-holders and partners, including community-basedorganisations (CBOs) that work with children.
METHODSUSED BYGLYNISCLACHERTY ANDASSOCIATESGlynis Clacherty and Associates used a combina-tion of activity-based focus group discussions andinterviews to gather information.This flexibilityworked well because it accommodated differentcontexts in different communities.
• At the Masakhane Women’s Organisation, theconsultants conducted two focus groups ofeight children, each for two different age groups(6- to 8-year-olds and 9- to 12-year-olds).
• At KDT, the consultants interviewed sevenchildren in the 6–10 age group in the juniorprimary school, four children in the 11–12 agegroup in the senior primary, and a 15-year-oldgirl and 16-year-old boy together from a localhigh school. (The girl started crèche at KDT,and the boy is a head of a household.)
• At Inkwanca HBC in the Eastern Cape, theconsultants conducted two focus groups ofnine children in the 6- to 8-year-old groupand eight children in the 9- to 12-year-oldgroup.
In all, 46 children (16 at Masakhane Women’sOrganisation, 13 at KDT, and 17 at Inkwanca HBC)participated in this exercise.
Glynis Clacherty and Associates designed activitiesto be simple and friendly and to allow even theyoungest children to participate.The instrumentcan be used either outdoors or indoors—under-neath a tree or in any available space. In two cases,the consultants spoke with children in an outdoorspace.The consultants also used “icebreaker”games at the beginning of the exercise and at in-tervals to create a relaxed environment.
The instrument is open-ended and allowed chil-dren to come up with their own opinions. Picturecodes, relevant scenarios, and third-person meth-ods were used to help the interviewers introducesensitive issues in a nonconfrontational manner. In-terviewers created a safe space for children to par-ticipate openly and talk about their experienceswithout necessarily revealing their identity. Childrenneeded to be relaxed and comfortable when theytalked about these issues.
ETHICALCONSIDERATIONS• Explaining clearly the purpose of the discus-
sion and how the information was going to beused
• Reinforcing to the children that it was okayfor them not to talk when they felt uncom-fortable or when they did not want to sharesomething and that declining to talk was notgoing to be used against them at any stage
• Explaining to children that the discussion wasconfidential and that their identity would notbe used
• Asking permission from the children to usethe tape recorder

5
Activity 2The interviewer sought to learn about the practicalhelp that the children get from the centre by ask-ing the children,“How does the centre help you?”The interviewer asked the children to respondusing art:
Draw all the things that the centre helpsyou with.
The interviewer then delved into the activities byrequesting that the children:
Draw the different things that you do at thecentre here.
Next the interviewer elicited discussion about thetwo drawings:
Let’s talk about them.
Activity 3The interviewer wanted to find out what childrenfelt were the positive and negative aspects of theirexperience at the centre, so he or she gave themthe following instructions:
Divide your paper into two parts.
On the left-hand side of the paper, draw all thethings that you like about the centre.
On the right-hand side of the paper, draw thethings you do not like about the centre.
Activity 4In talking with the first two groups, the interviewernoted that the children frequently referred to theirlives before coming to the centre.To capture thisinformation, the interviewer added this activitywhile speaking with children in the last group only.
The interviewer told the children to draw twopictures entitled:
Me—before I started coming to the centreMe—after I came to the centre
The interviewer then asked:How is your life different from what it was beforeyou came to the centre?
The interviewer asked the children torespond using art: “Draw all the thingsthat the centre helps youwith.”
THE ACTIVITIES USED TO ELICIT THECHILDREN’S OPINIONSThe children enjoyed the many icebreakers usedto help them relax.
Activity 1Silhouette figures helped to create a safe space forchildren to talk about their situations without feel-ing that they were giving away too much informa-tion about themselves.
When the interviewer brought out a silhouettefigure, he or she would say,
This boy/girl comes to the centre.
The interviewer would then ask the children,Who does he/she stay with at home?
What are his/her problems at home?
What does he/she need?

6
The consultants taped and transcribed thediscussions with the children, and thensorted the quotes into themes (e.g.,“I get
help with my education”).Voices of children fromthe three projects are combined here.To preservethe children’s words, we edited the quotations forpunctuation and spelling only; each child’s genderand age range follow the quote in parentheses.
Hardships I Faced BeforeFinding the Centre
Some children were comfortable discussing theirown struggles; others talked about likely situationsfaced by silhouette figures representing childrenlike them.
She gets to school late and they laugh at her.There is no electricity at her home and she hasto wash with cold water. (Boy, 9–12)
I don’t like it when other children play rough. Idon’t like smoking. I don’t like being a street kid.(Boy, 9–12)
Maybe she stays with her grandfather, and her grand-father does not take care of her and he hits herwith a stick when she comes home late. (Boy, 9–12)
I don’t like being hit with claps at home. (Boy, 9–12)
I felt sorry for myself and thought it would havebeen nice if I had parents. (Girl, 6–10)
There is no food at home….They do not buyfood; they spend money on alcohol….They treather badly at home…. No one cares for her….They hit her….They do not want her to go toschool….They do not want to give her food. (Boysand girls, 6–8)
I Get Help withMy Education
Children talked about how the drop-in centreshelped them access schooling by helping themwith uniforms and school supplies.
At Khanyiselani, we are given uniform when wedo not have. Food we are given and books whenwe don’t have. (Boy, teenager)
When you come here and lay your problembefore them—tell them that you do not haveclothes, you do not have school uniform, you donot have shoes, you do not have a trouser—theygive you. It can be a pen, pritt [glue stick],anything that you need for school you get here.(Boy, 9–12)
It helped me with school uniform and with foodevery day after school. (Girl, 6–8)
They buy you the uniform.They also pay for yourschool fees. (Girl, 9–12)
THE CHILDREN SPEAK
PHOTO BY MSH STAFF

7
I Get Help withMyHomework
Children mentioned homework as one greatsupport that they received from the centres.Homework included other projects, such as bak-ing, that they were expected to do at school. Inone group, children talked about basic literacy assomething that they really appreciated. Home-work is an important factor because one princi-pal was sceptical about the help the centre wasgiving children; he mentioned that teachersthemselves often struggled with the curriculum.
Some days we do homework, but if you have aproblem with your work regardless of the day youcan bring it and someone will help you with it.Wemostly do homework when Love Life people arearound. (Girl, 9–12)
I like the fact that what they give us is valuable[izinto ezine nqondo], things like helping you withyour homework. (Boy, 6–8)
What I like about Pink Huis [drop-in centre] isthat when you struggle at school with yourwork—when you fail and always get thingswrong at school and you do not have all yourschool things—they help you.They help you withyour homework, they explain things, and they giveyou things that you need for the school.Youbecome clever at school, and you pass. (Boy, 9–12)
The other day, we had a project at school. Sissuggested that we should bake for the project.They bought us the ingredients here at thecentre, and Sis baked with us. She taught us tomake a banana bread.We used the stove in thekitchen. Our choice of the project was the best,
and we felt proud. Other children liked thebanana bread, too. (Girl, 9–12)
The experience of working with children hasshown that school is the most important part ofthe lives of vulnerable children. For most children,when the researchers asked about their needs,school uniforms, school fees, and books took toppriority above everything else, including food.Thissignificance is not surprising because the childrenspend most of their time at school, and school isprobably the only place where the OVC feel thesame as other children.
“They help youwith your homework,they explain things, and they give youthings that you need for the school.”(Boy, 9–12)

8
The Food Is Good Here
Food has always been a challenge for children toaccept as an intervention both in public and atschool because of the stigma attached to it.Whystigma is attached to food remains unclear, butnevertheless, the children feel differently about ac-cepting the food from the drop-in centres.
Judging from what the children say, the food thatthey get from the centres is of good quality, wellbalanced, and nutritious, and it is prepared carefullyand very nicely.They are given the food with dig-nity, the preparation is good, and children feel val-ued. In some cases, it was also mentioned thatchildren who go to these centres do not eat in thefeeding schemes in schools; they wait until lunch atthe centre, especially the children who get break-fast as well at the centre.
I like fruit. I like the food. I like the fact that welaugh a lot when we are here. I like playing withthe bicycle, and I like it when we sing. (Boy, 9–12)
What I like here is the way they cook the food.The food is nice. (Boy, 9–12)
In the morning I wake up, make the fire, warmthe water, wash and put on uniform, and go to
school. I come here to eat porridge. I go to school.During break time, I play, and after school, Icome here and eat and go home. (Boy, 6–8)
I like the food here.They cook it nicely. I like myfriends. I like listening to music. I like netball.(Girl, 9–12)
When we get to Khanyiselani we eat, we get full.We have a snack or juice. (A teenager)
In isolated cases, children who were not part ofthe centre would sneak in for the food.Althoughthis practice was, of course, not encouraged be-cause food is prepared according to the numbersregistered at the centre, the centres did their bestto care for these other vulnerable children.The factthat it happens shows how the centres have man-aged to feed the children with dignity.
“I like the fact thatwe laugh a lotwhenwe are here.” (Boy, 9–12)
PHO
TOBY
MSH
STA
FF

I Go onOutings and Picnics
Children mentioned food during outings and pic-nics as one of the things that they enjoyed:
I enjoyed food and swimming when we went toEast London. (Boy, 9–12)
Food was very nice.We had a braai [barbeque]at the beach. (Boy, 6–12)
Some days we just play and play at the centre.On some special days we are taken out, and weeat out at Nando’s in town. (Girl, 6–10)
We went to a dam, we played games, we danced,they braaied for us and we had fun. (Girl, 11–12)
It is not hard to see how the centres have tried tocreate a homey atmosphere around the outings.They have gone out of their way to make the pic-nics family outings, and the children have loved it. Insome centres, children are taken out to restaurants.
I Take Trips
Many children in poor environments do not travelfar from their homes. In actual fact they have neverbeen beyond their hometowns.They lack expo-sure.This does not happen just to vulnerable chil-dren; it happens to most people in thesecommunities.
We travel to places for games and trials.We aretaken out to faraway places like Port Edward. It islike a treat being taken out to natural settings tothink and talk about our troubles.We come backlight, hopeful about our future and looking for-ward to living our lives.You cry when you want tocry; you pray when you want to pray. (Girl, 11–12)
In East London, we went to the MhloboWenene [aradio station], to the museum, to the zoo, and tothe beach. It was so much fun.We enjoyed it [besionwabile—“with smiles on our faces”]. (Boy, 9–12)
We have outings.We braai.We dance.We haveChristmas parties, and they buy us presents.(Girl, 6–10)
9
We feel free and happy at these outings. (Girl, 6–8)
Most of us went to East London for the first timeand now we are going to Ebhayi [Port Elizabeth].(Boy, 9–12)
I Enjoy Different, FunActivities
Activities varied from sports activities to culturalactivities.The centres seem to have filled a gap oforganised activities in their communities.This com-ponent is quite important and has been found tobe lacking nationally in all the municipalities andleads to many of the social problems experiencedby youth and children in the communities. Childrenhave neither play spaces nor well-maintainedsports facilities in these communities.
We do marjorettes here at school and at thecentre.We have a beautiful uniform here at thecentre; we perform in some of the dos in thetownship as a centre. I love it. (Girl, 11–12)
There are cultural activities, art activities, and allsorts of activities that start at four. Everyone iswelcome. Many children love coming. (Boy, 11–12)
We have a park with swings, with abojingo.…Weplay where it is safe. (Girl 11–12)
Some days we eat, do hand work like sewing andcrocheting. Only older children like us do these. Ican put on back a seam on my uniform dresswhen it’s undone. [says it proudly] (Girl, 11–12)
I Learn Important Life Skills
Some of the life skills topics that the children men-tioned help to instil in them the values of Ubuntu,a philosophy that focuses on people’s allegiances toand relationships with one another—values thatsome South Africans feel are disappearing with thedisintegration of society.The centres seem to becentral in restoring and reinforcing the role that

10
the functional society and its institutions such asthe church and units such as families should play inraising the children.
We come here after school.We eat.We play.Weare taught about HIV. Sometimes they wash ouruniform on Saturdays. (Girl, 9–12)
They teach you things that you do not know.(Girl, 9–12)
There are older children who are taught to sew.They work with their hands, and they are taughtmany things. (Girl, 9–12)
I like the care centre because it teaches youabout the things that you didn’t know.They teachus that we should not sleep with boys before it isyour time, and that those who are doing it shoulduse a condom. (Girl, 9–12)
I like the care centre.They found most of ussmoking on the streets.They took us in and tookcare of us.They taught us about drugs in ourgroups, and they sent us back to school. Now weeat here after school. It is like home. (Boy, 9–12)
At the centre, we are taught how we shouldbehave, that we should obey adults when theytalk to us. (Boy, 9–12)
I like it when they teach us about different drugs.I used to smoke glue and they taught us how itharms us.They showed us pictures of whatdifferent substances did to our different bodyparts. (Boy, 9–12)
Loving one another was a life skill that children hadsaid they had learned.
We are taught that we should be peaceful withother children when we play.We should not fightwith them, and we should not swear at them.(Boy, 6–10)
We are taught to take care of the youngerchildren who also come to Khanyiselani; forexample, we should help them to cross the roadsafely when we go home. (Girl, 11–12)
We are also responsible for walking home withour younger siblings who are at the crèche aftereating. (Girl, 6–10)
I Found a Place to Call Home
Many children who go to the centres feel as thoughthey are home. For some children, the centres arethe homes they never had and for some they arethe homes that they once had and lost. It is clearfrom some children’s comments that the centresprovide for them much more than they could hopefor in a home, and they appreciate that.
Pink Huis [drop-in centre] is like your mother orfather.They do for you all the things they do notdo for you at home—they give you food andschool things that you do not have, and you cancome and talk to someone when you have aproblem, and they help you. (Girl, 9–12)
I know what I go to Khanyiselani for. It is ahome…. [T]here are people we can talk to aboutour problems. It is just an amazing place. I feelthat when I grow up I want to contribute to anenvironment like that. I wasn’t this big when I firstcame here.They brought me up. (A teenager)
“It is like in the centrewe have ourmothers even thoughwe are orphans.”(Girl, 9–12)
PHOTO COURTESY OF WINTERVELDT HIV/AIDS PROJECT

I Have the Company of OtherChildren fromMyCommunity
Children have formed their own network of sup-port with other children.At the centres, they feellike other children, and they can relax and laughabout things.
I like being with other children. (Boy, 6–8)
When we are here at Inkwanca, we are likeapples—like other children—because they makeme laugh. [I like] playing soccer with other teams,riding a bicycle, and [going to] school. (Boy, 6–8)
MyHealth Is Important Here
Most centres have clinic records of their children.They also follow up on children’s health, send themfor screening, and keep their medical histories.Theymake sure that children have access to medicaltreatment when they need it.This attention makeschildren feel special and cared for.The centres aremore organised than some parents in this regard.
Before we came to the centre, we sometimes(most of the time) did not eat in the morningbefore we came to school.After school you wouldfind that you eat only pap, and at school, wewould eat starch only with gravy. Now that weare in the centre, we eat nutritious, balancedfood, and we no longer get sick. (Girl, 6–10)
I used to have stomach aches. I was thin.(Girl, 11–12)
We used to have sores on our body. Now theyare gone. (Boy, 6–10)
It is like home because they give us stationery,they give us food, and they help us; now I am well.They first took care of me when my mother died.(Girl, 9–12)
It is like in the centre we have our mothers eventhough we are orphans.There is that love that weget from our caregivers, when we have problemswe can talk to our caregivers. (Girl, 9–12)
It has been 8 years since I started eating atKhanyiselani, and I am still eating there now,because Khanyiselani is a place that I can call myhome. (Girl, 15)
When I walk into the centre after school, I feellike I am walking into my home which is well builtand beautiful. (Girl, 11–12)
I Have Someone to Talk to
Many children in general find it difficult to talk toan adult about their problems. Children in the cen-tres felt protected and listened to.This feeling givesthe children the message that they are valued andthat they are important.
There is always someone to talk to at the centre.They listen to you, and they help. (Girl, 9–12)
When you do not feel right—when there issomething bothering you at home, when they donot treat you well—you come and talk to a socialworker about it here at the centre. (Girl, 11–12)
When you have a problem at home, they solve itfor you, they talk to the person who bothers youat home. (Boy, 6–10)
When you have a problem of children whobother you here at school, you can tell them atKhanyiselani, and someone will come to talkabout your problem here at school. (Girl, 11–12)
11
“There is always someone to talk to usat the centre. They listen to you, andthey help.” (Girl, 9–12)
12
Sometimes I used to sleep in class. I don’tanymore. It was hunger. (Girl, 11–12)
I also want to thank Khanyiselani because I amalways well since I started in Khanyiselani. I usedto be sickly. (Girl, 11–12)
Since I joined the centre, I am well.At first I usedto be sickly, and I slept in hospital a lot. When Iwas in hospital, they made sure I had nutritiousfood with nutrients like proteins and vitamins, andthey brought me fresh food. (Girl, 11–12)
When we are sick—
When you are sick, your parent or guardian hasto report here at Khanyiselani that you are inhospital or so that they take you to hospital. Thenpeople here at Khanyiselani go and see you inthe hospital and they bring you healthy food thatyou should eat—food that is safe; food thatbuilds your body. (Boy, 6–10)
I was once in hospital after I had an accident andmy grandmother came to report here at thecentre. I slept there for a day, but they came onthe first day to see me, and they brought me foodand snacks (peanuts and raisins). (Girl, 11–12)
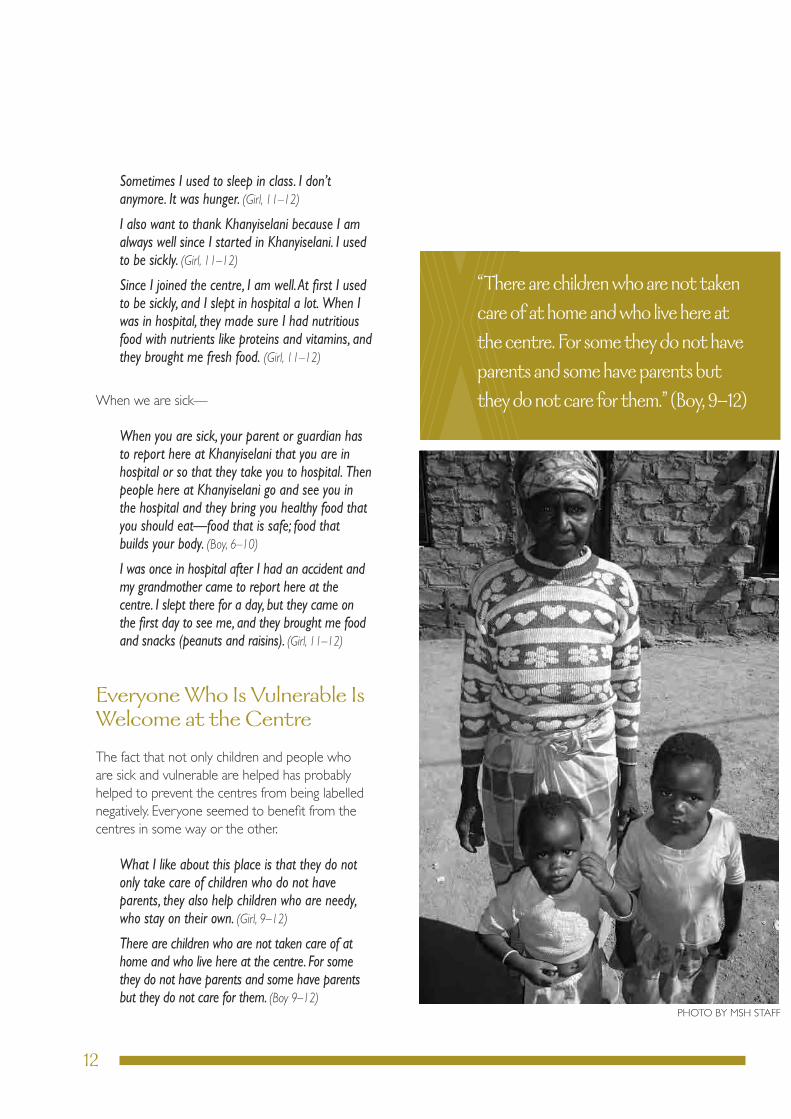
EveryoneWho Is Vulnerable IsWelcome at the Centre
The fact that not only children and people whoare sick and vulnerable are helped has probablyhelped to prevent the centres from being labellednegatively. Everyone seemed to benefit from thecentres in some way or the other.
What I like about this place is that they do notonly take care of children who do not haveparents, they also help children who are needy,who stay on their own. (Girl, 9–12)
There are children who are not taken care of athome and who live here at the centre. For somethey do not have parents and some have parentsbut they do not care for them. (Boy 9–12)
“There are childrenwho are not takencare of at home andwho live here atthe centre. For some they do not haveparents and some have parents butthey do not care for them.” (Boy, 9–12)
PHOTO BY MSH STAFF

13
Some people who are poor and some who aresick get groceries here. (Boy, 6–8)
If she [a girl represented by the silhouette figure]comes to the Care Centre, she will be cared forby the women at the Care Centre.They will talkto her, and they will protect her from being astreet kid. (Boy, 9–12)
I AmCared For and Protected
Centres provide a haven for children who mayhave no other refuge.
I feel like there is someone who knows you andcares.When you come to the centre, they want toknow everything about you—they want to knowwho you are staying with and what are yourproblems so that they can help you.They can talkon your behalf. (Girl, 11–12)
It has kept us safe [Isilondolozile]. It hasprotected us by taking care of us at our homesand at school. (Boy, 6–10)
She [a girl represented by the silhouette figure]will feel better and she will get help [from thecentre] and will realize she is not alone. (Girl, 9–12)
I used to worry about myself. Now I don’t—boAuntie [aunties] at Khanyiselani help us whenwe have a problem.They help by listening, and ifyou need something they make sure that they getit for you. (Girl, 6–10)
I Feel Good aboutMyself
The centres affirm the children.They boost theirconfidence.
I feel good about myself because of what thecentre helps me with. I feel like other children. Iused to feel bad about my situation at home.(Boy, 6–10)
Since I have been at Khanyiselani, I feel free. Ifeel much better. (Girl, 6–10)
I am right now. I used to feel worried and I gothelp. (Boy, 6–10)
“I feel like there is someonewho knowsyou and cares.” (Girl, 11–12)

14
MasakhaneWomen’sOrganisation
Masakhane Women’s Organisation (MWO), acommunity-based initiative that was established in2003, is located in Hlokozi village, a rural area situ-ated in High Flats, in the Sisonke District ofKwaZulu Natal Province.The project is under theUbuhlebezwe local municipality in the subdistrict ofIxopo.The municipality has a total population of122,860 people and a high unemployment rate: 82percent.The major economic activity is sugar canefarming and forestry, but estimates indicate that 83percent of the households have no monthly in-come. Projected estimates show that 20 percentof the population is HIV positive.
Masakhane Women’s Organisation has a staff of 25consisting of a project manager, a project adminis-trator, 18 caregivers, and 3 professional nurses. Inaddition to the funding from IPHC, the MasakhaneWomen’s Organisation also receives funding fromthe South African Department of Health.
The organisation supports 367 OVC, the majorityof whom (53 percent) are male (Table 1). These aresome of the activities being undertaken byMasakhane Women’s Organisation to support OVC:
•Supporting an early learning centre for28 OVC
•Facilitating access to health care through amobile clinic once a month
•Assisting OVC to obtain identity documentsand birth certificates
•Providing counselling services and protectionto abused and neglected OVC
MASAKHANEWOMEN’S ORGANISATION MALE FEMALE TOTAL
Clinical nutrition interventions 5 5 10
Food and/or food parcels 190 170 360
Shelter interventions 2 0 2
Child protection interventions 192 167 359
general health care services 59 50 109
Health care support specifically for antiretrovirals (arVs) 61 50 111
HIV prevention education or interventions 59 52 111
Psychosocial care 0 1 1
general education 60 51 111
Vocational training 1 0 1
economic opportunity or economic strengthening 1 1 2
Total number of OVC supported at MWO 195 172 367
note: Each orphan or vulnerable child may receive several services. Source: IPHC Semi-Annual Report (2008)
THEORGANISATIONS & THE CENTRES
Table 1. A Summary of Services Provided to OVC by MWO
15
•Providing care and support for HIV-positiveOVC at the drop-in centre
•Networking with government departments inaddressing the needs of OVC
•Conducting awareness campaigns to advocatefor child protection needs
Inkwanca Home-Based Care
Established in 2001, Inkwanca HBC operates inChris Hani District of Eastern Cape Province.Inkwanca local municipality has a small populationof 14,000 people, of whom 5,000 are children.Theaim of the Inkwanca HBC is to provide holistic,community-based care to vulnerable children, theirfamilies, and the larger community in the town ofMolteno. Inkwanca HBC also hopes to establish asecond community centre in the nearby town ofSterkstroom.
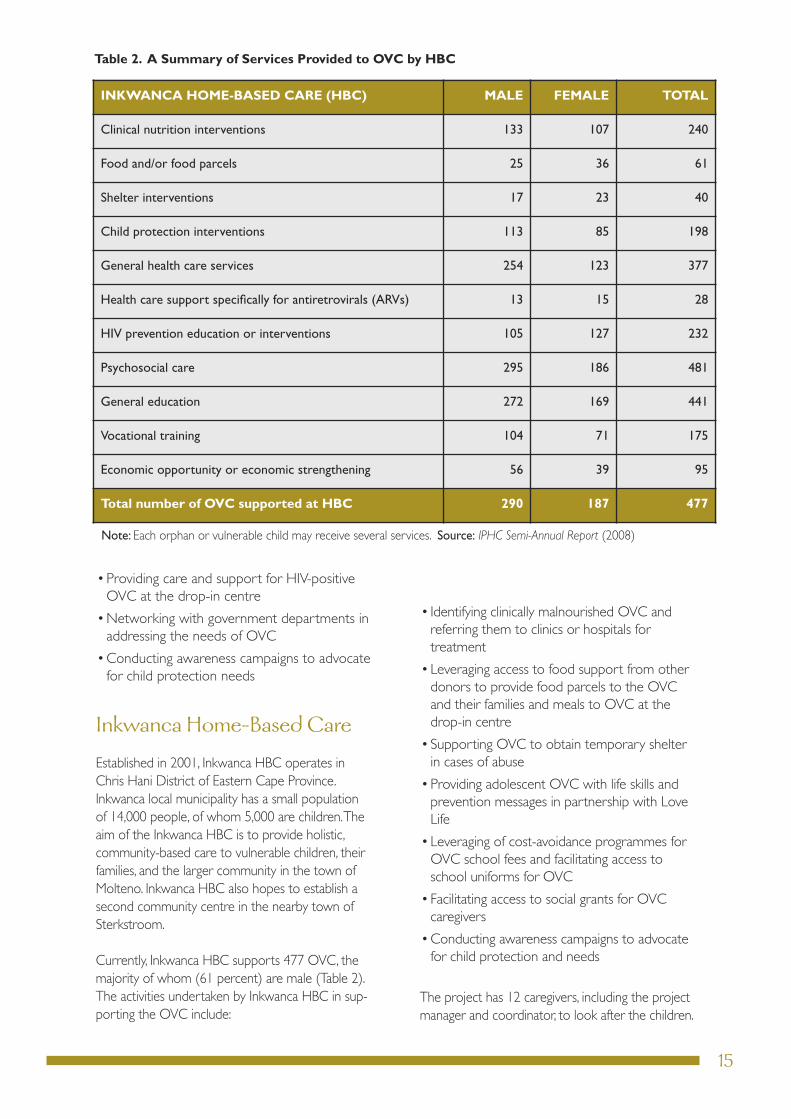
Currently, Inkwanca HBC supports 477 OVC, themajority of whom (61 percent) are male (Table 2).The activities undertaken by Inkwanca HBC in sup-porting the OVC include:
• Identifying clinically malnourished OVC andreferring them to clinics or hospitals fortreatment
•Leveraging access to food support from otherdonors to provide food parcels to the OVCand their families and meals to OVC at thedrop-in centre
•Supporting OVC to obtain temporary shelterin cases of abuse
•Providing adolescent OVC with life skills andprevention messages in partnership with LoveLife
•Leveraging of cost-avoidance programmes forOVC school fees and facilitating access toschool uniforms for OVC
•Facilitating access to social grants for OVCcaregivers
•Conducting awareness campaigns to advocatefor child protection and needs
The project has 12 caregivers, including the projectmanager and coordinator, to look after the children.
INKWANCA HOME-BASED CARE (HBC) MALE FEMALE TOTAL
Clinical nutrition interventions 133 107 240
Food and/or food parcels 25 36 61
Shelter interventions 17 23 40
Child protection interventions 113 85 198
general health care services 254 123 377
Health care support specifically for antiretrovirals (arVs) 13 15 28
HIV prevention education or interventions 105 127 232
Psychosocial care 295 186 481
general education 272 169 441
Vocational training 104 71 175
economic opportunity or economic strengthening 56 39 95
Total number of OVC supported at HBC 290 187 477
note: Each orphan or vulnerable child may receive several services. Source: IPHC Semi-Annual Report (2008)
Table 2. A Summary of Services Provided to OVC by HBC

16
The Inkwanca DirectorSpeaks
While I was working at the hospital I realized thateverybody was sent to the hospital for differentproblems—even for the ones where the hospitalcouldn’t help. I felt that some people suffered justbecause of social problems, and they did not needhospitalization but just counselling. Some of theproblems were because of communicable diseaseslike diarrhoea and many other diseases that couldbe prevented. Hunger [malnutrition] was the mainissue for children.
We started as a soup kitchen—cooking soup froma small room, and I went around the communityasking for spoons, plates, and whatever peoplecould give me to feed the vulnerable children andalso the orphans. Fortunately, the community ofMolteno responded, giving us clothes as well.Agroup of ladies from different churches startedtaking interest, and they ended up giving us foodevery Friday to cook for the children. I could thenafford to feed continuously.
We realized that a lot of street children were eat-ing from the dustbins. I then initiated this as a mul-tipurpose centre, to address other social problemslike alcoholism and HIV & AIDS, and to help every-one who was needy in Molteno. I recruited thevolunteers to visit the people and find out moreabout what was wrong within this community.
IN-HOUSE SERVICESNow we are fortunate to get funding from differ-ent donors like the Department of Health, SocialDevelopment, the European Union, and MSH-USAID that have enabled us to render our serv-ices more efficiently.
THEDAYCARECENTREThis centre started after we went door-to-doorand found that some of the orphans were left withsick old ladies and so were not growing up in anormal healthy environment—and the old ladieswere struggling with them. Some of the childrenwere left with alcoholic foster parents. So wethought the day care centre would be the bestway to protect the children and to take care ofthem.We took the children in, observed them, andreferred them to different institutions for differentassessments.We now have children from ages 2 to5 years.They come in the morning until 13:00.Some are HIV positive and on treatment. Becauseof this, the diet is very healthy and takes into con-sideration their specific needs.We have a well-equipped playground for them and experiencedearly-childhood development practitioners.
LUNCHANDTRANSPORTARE FREEThe parents do not pay anything toward the cen-tre. Children get all their meals here, and they havefree transport that fetches them from home toschool and back again.
ACTIVITIES FORSCHOOL-AGECHILDRENANDANONGOINGLIFE SKILLS PROGRAMMESchoolgoing children come to the centre everyday after school for their lunch.They have activitiesin the afternoons, and there are life skills pro-grammes that are offered on an ongoing basis.
HOMEWORKChildren get support with their homework andprojects here at the centre.
MS. SOPHIEMANXALA
IN HERWORDS

17
OUTREACH PROGRAMMESWe went from strength to strength, and wereached out to the community by providing thefollowing additional services.
MEALSONWHEELSIn this project, we take meals to the community.We cook for them, and a group of volunteers of-fered their cars to deliver the meals in the homesof vulnerable people on Mondays,Wednesdays,and Fridays.
EDUCATION FORCAREGIVERSOFCHILDRENAND SICK PEOPLEWe go out to the community to train caregiverson how to take care of people who are sick andvulnerable.We also recruited volunteers andtaught them the same skills and further skills onhow to identify people and children who areneedy in the community up until they acceptedand owned the project.
LIFE SKILLS PROGRAMMEThis programme has been extended to localschools. So we do not only reach children whocome to the centre, we also reach other childrenas well.
RELATIONSHIPWITHMSHMSH started supporting us in 2006 regarding theOVC.They fund us [through USAID], and theystarted with R300,000, and in 2007 they increasedit to R350,000 because of the other branch atSterkstroom where we have extended our serv-ices. They give us this money in tranches; we firstgive them a quarterly report, and they give us thetranche.We use the money and write them a re-port. One of the reasons that we have been cho-sen for the MSH funding is that we do care andprovide support for the OVC. �
PHOTO COURTESY OF WINTERVELDT HIV/AIDS PROJECT

18
Khanyiselani DevelopmentTrust
Established in 2001, the Khanyiselani DevelopmentTrust (KDT) operates in the Sisonke District ofKwaZulu Natal Province. Its aim is to provide holis-tic, community-based care to vulnerable children,their families, and their communities in the greaterKokstad local municipality. Kokstad has a populationof more than 46,000 people, and approximately9,000 are children.
In 2002, the National Peace Accord Trust (NPAT)established a formal partnership with KDT to buildthe capacity of the organisation and help it to ex-pand into surrounding areas. NPAT has experiencein trauma counselling, so the partnership has en-abled KDT to offer counselling services to OVCtraumatized by abuse or bereavement.
Since 2002, the main activities of NPAT have re-lated to capacity-building of KDT and provision ofsupport services.The executive director of NPAT,
who is based in the organisation’s Gauteng head-quarters, visits KDT approximately once a month.NPAT has satellite offices in Margate and Kokstadin KwaZulu Natal—hence the easy access toKhanyiselani. NPAT has also helped Khanyiselani todevelop into a National Integrated Programme.The support of NPAT to KDT includes provisionof salaries to six KDT staff members.
KDT is currently providing support to 1,594 OVC,the majority of whom (59 percent) are female(Table 3).These are some of the activities under-taken by KDT:
•Helping OVC obtain ART
•Leveraging access to food support to providemeals to OVC at drop-in centres
•Supporting OVC through vocational trainingin beadwork, sewing, and painting
•Providing OVC with psychosocial carethrough performance arts, including dance,poetry, and music
The partnership with NPAT has enhanced the per-formance of KDT in management of its financialresources. NPAT provides financial oversight of allKDT expenditures for its OVC activities, including amonthly review of all expenditures and accountingthrough receipts.
KDT is currently providing support to1,594 orphans and vulnerable children.
PHO
TOBY
MSH
STA
FF

19
KHANYISELANI DEVELOPMENTTRUST MALE FEMALE TOTAL
Clinical nutrition interventions 32 33 65
Food and/or food parcels 290 357 647
Shelter interventions 0 0 0
Child protection interventions 308 340 648
general health care services 263 238 501
Health care support specifically for antiretrovirals (arVs) 107 139 246
HIV prevention education or interventions 307 341 648
Psychosocial care 215 231 446
general education 264 275 539
Vocational training 200 228 428
economic opportunity or economic strengthening 0 0 0
Total number of OVC supported at KDT 647 947 1,594
note: Each orphan or vulnerable child may receive several services. Source: IPHC Semi-Annual Report (2008)
“We have seen children whowereshy, whowere not confident, andwho couldn’t open up beingtransformed... they are nowconfident, and they talk more.”
Table 3. A Summary of Services Provided to OVC by KDT

20
The Director Describes theKDT Project
We started as a small project in church.We gath-ered children who were eating from the dumpsiteand gave them food.We asked members of thechurch to donate food for cooking and secondhand clothing for the children.We invited the chil-dren to church on Sundays, and they would bebeautiful and clean.We went to town and askedfor food donations, and some would donate thingssuch as soup, and we cooked for the children.
Then came 2000, I decided to take early retire-ment because I started having a passion to workwith these children. I was working at the district of-fice, and all of a sudden I was inundated with callsfrom people who wanted funding towork with vulnerable children.When we took these reports tothe provincial level, they would sayif we had a nongovernmentalorganisation (NGO) inKokstad, it would take careof such things.When weadvised people to formNGOs, they abandonedtheir ideas until I decidedto leave work and do itmyself.We collated thestatistics of the vulnera-ble children.
After some time, I saw an advertisement in thenewspaper about the government’s National Inte-grated Programme for vulnerable children, forwhich they were inviting NGOs to apply. I applied,and we were selected as a pilot site for the project.We had nowhere to work from.As you know, thegovernment does not fund churches.We had tolook for a place as a result, but then in the mean-time, we were allowed to utilize the church as oursite, as it had space. But we had to be clear that wewere not a church organisation.We applied to themunicipality to give us a space.The Department ofHealth offered us a park home that had offices anda kitchen, and that is the one that is right there andworks as a crèche now.Then we found this house,and the municipality renovated it for us.There wasnow growth and development in the organisation.By now we had so many children who had suchharsh lives and so many traumatic life experiences.
IN HERWORDS
MS. THEODORANONDUMISOMAKALIMA
PHOTO BY MSH STAFF
21
We partnered with a number of groups:
NATIONAL PEACEACCORDTRUSTThrough this partnership, we were now able tohave a holistic intervention.We initially had thehealth, welfare, and education interventions, butthe component of psychosocial support was lack-ing, and the partnership with NPAT helped in thatregard. Its main mission is around trauma interven-tion strategies; therefore, it gave a huge boost toemotional wellness as part of our intervention.
Our caregivers were exposed to trauma manage-ment, which enabled them to deal with their owntraumas before they could deal with the children’straumas.They were also exposed to skills inecotherapy, which is a trauma intervention strategy.We now have ecotherapy facilitators who havebeen trained by the NPAT. It is a very powerfultool in addressing the traumas of the participants.It is such an eye opener, and it is unbelievable tolisten to small children—10- and 11-year-olds—sharing their experiences about the ecotherapyand their lives.
DEPARTMENTOFWELFAREThe Department of Social Welfare and Develop-ment identified us as a site that could benefit froman Association for NationalYouth and Caregivers.Our field workers could be trained and accreditedfor child and youth work.This training would en-able them to deal with issues that emanate fromdealing with OVC.
ART TEACHERS, WHOUSE ARTAS AFORMOF THERAPYTwo art teachers from the local schools offered tovolunteer their services to us after school.Art hasreally taken shape, and it has really helped our chil-dren. It has always been our dream to have art atthe centre, but we did not know where to start.The impact on the children has been unbelievable.
We have seen children who were shy, who werenot confident, and who couldn’t open up beingtransformed when they perform—they are nowconfident, and they talk more.They are assertive. Ithas boosted their morale. Both the performancearts (drama, music, poetry, and dance) and the vi-sual arts (sewing, drawing) are used.They havebeen exposed to workshops in art, and now wehave networked with people at the provincial levelon arts.
NFSASIn 2005 I saw an NFSAS [National Education Fi-nancial Scheme for South African Students] adver-tisement in a newspaper inviting NGOs to ameeting in Durban.They said when they madetheir survey on the beneficiaries of their services,they found that it was vulnerable children from thecities who benefited more from them and not chil-dren from the outskirts like us.They were lookingat ways of working closer with people from thesmall and marginalized communities.This presentedus with a real opportunity, so we applied asKhanyiselani to partner with them.They acceptedus. Because of this partnership, we are now able torefer students who are vulnerable to the nearesttertiary institutions.We have seven of our benefici-aries in tertiary at different levels—three at thirdyear, two at second year, and two at first year. Wehave since realized (now that we can interact withgovernment departments) that they have bursaries,so this year we have two children who are doingdegrees in agriculture, and they are now sponsoredby the Department of Agriculture in KwaZuluNatal.
One of our success stories is a girl who graduatedon April 21, 2008, with a social sciences degree.We sent her for her first-year studies with a dona-tion that we received from Standard Bank; that wasbefore we had NFSAS. She is now doing herhonours. �

22
Centre StaffDiscuss MSH Support
Researchers also talked to the staff about their ex-periences of working with OVC. For many, the ex-perience of watching children transform as a resultof their intervention was a key factor in why theyare committed to the work they do.
The work gives pleasure because you can actuallysee the children you have identified getting help.Some get food here in the mornings, some getfood parcels to cook at home, and some getuniforms from the centre.Through helping them,you feel you are making a difference. You seethem become children again.
As volunteers, we are paid by PEPFAR.Thestipend that we get makes a big difference in mylife. I am being paid to help my community, and Iam also being taught by attending workshops.I am grateful.
MSH bought the children soccer jerseys….Everyone in the villages cannot close theirmouths about it.They look like professionalplayers when they go to play.They are the envy ofthe village. (Note:This reduces stigma andenhances the children’s self-esteem.)
When it comes to children’s things, PEPFAR doesnot laugh.They support us, they make sure thatthe children are catered to. Look at theplayground things for the preschool children.Weare not found wanting in that division.Theyprovide.
PEPFAR helps us a lot in providing for thechildren. It helps us a lot on travel (petrol andlogistics), stationery for the children…generaleducation, play equipment for the early-childhooddevelopment centre.
HIV education and issues of child protection areimportant—like if a child has been raped, we canstart by reporting to the Induna [traditionalleader], then the police.They pay stipends for 10HBC people, training.
Their funding is not for food, but when they came,they saw that we had a day care centre and thatwe did not have food for the centre; they said wecan buy meat. So because of the day care centre,we do buy food because some of the children areinfected.
The big thing is that they are one of the fundingorganisations that you can access food as well,which the other funding organisations do notallow—they do it only with specific occasions.With MSH, you can access the groceries and thatsort of thing to feed the children. It is purely usedto feed the children. It is for the day care and theafter care.That has helped a lot.
I found people from MSH who have been here agreat help.Talking to them puts into perspectivewhat your actual job is. Speaking to project staffwhen they came down here almost told me whatmy job was.That was great support. I think theyare fantastic.They keep systems—you are able tokeep track. It helps—you know administrationoffices are not usually the best, but because oftheir intervention I can find you anything,anytime, I promise you.
“Through helping them, you feel youare making a difference. You seethem become children again.”

23
Much recent thinking around the best ap-proach to helping vulnerable children hasfocused on the theory of resilience. The
work of Julia Bala (1996) is an example of this the-ory. Bala identifies four levels at which resiliencecan be built in children:
REDUCING STRESSORS•Reducing the impact of present stressors
•Unloading accumulated problems
•Assisting in making peace with the past
•Minimizing anticipated stress that could inter-fere with daily life
STRENGTHENINGAND SUPPORTINGTHEUSEOF EXISTING PROTECTIVE FACTORS•Within the child
•Within the family
•Within the wider social environment (e.g.,friends and neighbours)
BROADENINGCOPINGALTERNATIVES•Facilitating the use of existing coping strategies
•Providing assistance in seeking new copingskills (including, for example, training, life skills,and beliefs)
STRENGTHENINGANDOPENING FUTUREPERSPECTIVES•Supporting the search for future possibilities
and visions
A complete impact study developed around spe-cific indicators would be required to measure theextent to which these factors are present in thelives of the children who attend the MSH-supportedcentres. It is possible, however, to look at the quo-tations collected from the children in this reportand see how the centres are building resilience inchildren.
It is clear that the drop-in centres play an impor-tant role in the children’s lives.They obviously pro-vide help at a physical level—children receive foodand help with school needs.What stands out fromwhat the children say, however, is the extent towhich this meeting of physical needs has an impacton their psychosocial well-being. Clearly reflectedin their comments is the fact that meeting theirphysical needs reduces their emotional stress (pre-sent stressors) and minimizes anticipated stress.Furthermore, this provision of physical needs alsoworks to build protective factors within the individ-ual child. Having everyday needs met creates asense of self-worth and locus of control—both im-portant components of resilience.
Additionally, the centres also make a big contribu-tion to children’s psychosocial well-being throughthe social interaction that the staff at the centreshave with children—the outings, the help withhomework—and the contact with other childrenin similar circumstances. Children feel loved whenthey go to the centres.This feeling of acceptancereduces emotional stress and helps children dealwith grief to some extent too (i.e., to unload accu-mulated problems).Additionally, the comments in-dicate that the centre staff and other children, insome cases, become an alternative family, providingthe protective role that family would play for chil-dren.The children also talk about how they havelearned new skills and problem-solving strategies(e.g., learning about rights) through the life skillseducation they receive.
Again, a more comprehensive study would beneeded to confirm this assertion, but this prelimi-nary work suggests that the drop-in centre model isan effective way of reaching vulnerable children.�
CONCLUSION

24
Bala, j. 1996. Strengthening the Protective Umbrella:The Refugee Child and the Family. Proceedings of theCongress on Children,War and Persecution – RebuildingHope. Maputo 1–4 Dec.
Integrated Primary Health Care Project, 2008. Semi-Annual Report to USAID. Pretoria, South Africa.
Khulisa management Services. 2008. Case Studies ofPEPFAR Funded OVC Program in South Africa.
REFERENCES
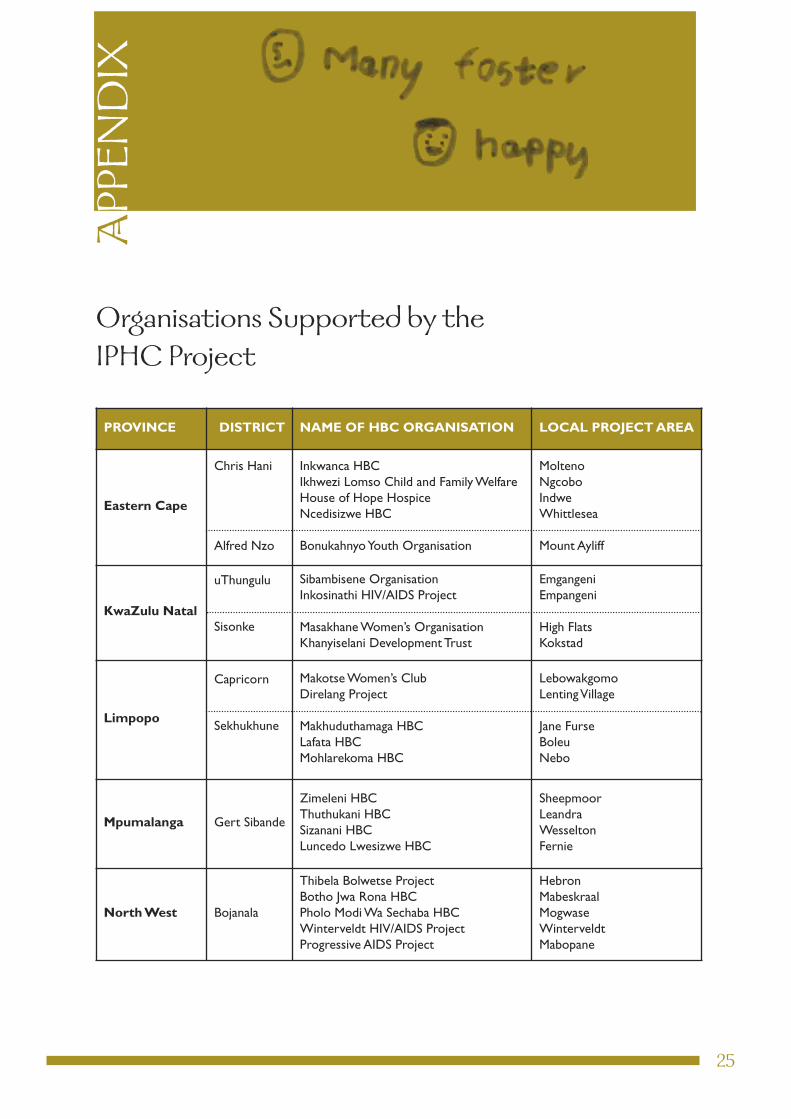
PROVINCE DISTRICT NAME OF HBC ORGANISATION LOCAL PROJECTAREA
Eastern Cape
Chris Hani
alfred nzo
Inkwanca HBCIkhwezi lomso Child and Family WelfareHouse of Hope Hospicencedisizwe HBC
Bonukahnyoyouth organisation
moltenongcoboIndweWhittlesea
mount ayliff
KwaZulu Natal
uthungulu
Sisonke
Sibambisene organisationInkosinathi HIV/aIdS Project
masakhane Women’s organisationKhanyiselani development trust
emgangeniempangeni
High FlatsKokstad
Limpopo
Capricorn
Sekhukhune
makotse Women’s Clubdirelang Project
makhuduthamaga HBClafata HBCmohlarekoma HBC
lebowakgomolentingVillage
jane FurseBoleunebo
Mpumalanga gert Sibande
Zimeleni HBCthuthukani HBCSizanani HBCluncedo lwesizwe HBC
SheepmoorleandraWesseltonFernie
NorthWest Bojanala
thibela Bolwetse ProjectBotho jwa rona HBCPholo modi Wa Sechaba HBCWinterveldt HIV/aIdS ProjectProgressive aIdS Project
HebronmabeskraalmogwaseWinterveldtmabopane
25
APPENDIX
Organisations Supported by theIPHC Project
this booklet is a project of the national department of Health and is made possibleby the support of the american people through the United States agency for
International development (USaId).the contents are the sole responsibility of theIntegrated Primary Health Care (IPHC) Project and do not necessarily reflect the
views of USaId or the United States government.
INTEGRATED PRIMARY HEALTH CARE (IPHC) PROJECTmanagement SCIenCeS For HealtH
Board Walk office ParkBlock 6
Haymeadow StreetFaerIe glen, 0048
South africa
Phone: 012 9913559Fax: 012 9912714
email: [email protected]
natIonal dePartment oFHealtH oF SoUtH aFrICa
SoUtH aFrICanS and amerICanSIn PartnerSHIP to FIgHt HIV/aIdS