ORMONI E FERTILITA’ - bollettino-emiliaromagna.it · Traditionally, hormone replacement therapy...
49
ORMONI E ORMONI E FERTILITA’ “L’evoluzione dell’ HRT” Cesare Battaglia, Arianna Cianciosi
-
Upload
doankhuong -
Category
Documents
-
view
216 -
download
0
Transcript of ORMONI E FERTILITA’ - bollettino-emiliaromagna.it · Traditionally, hormone replacement therapy...

ORMONI E ORMONI E FERTILITA’
“L’evoluzione dell’ HRT”
Cesare Battaglia, Arianna Cianciosi

The Menopausal Transition begins at age 47 and takes about 4 yrs. It is unchanged during the centuries, but enviromental factors (i.e.
smoking) may alter the ovarian aging process
~ 51 yrs
~ 4 yrs
Premenopause

Progressive loss of functional follicles pool
The perimenopausal transition begins in the mid- late thirties and is related to a
granulosa cells compromise(Barri, 2000)
The granulosa cells have a reduced function indicated by decreased mitosis and increased
apoptosis(Seifer and Naftolin, 1996)
(spontaneous ovulation <5% and pregnancies ~ 0%)

Menopause occurs when the ovarian follicular pool is functionally
exhausted(Age/POF) or by surgical removal of both ovaries
The hypoestrogenic state may affect estrogen target tissues
adverselyincluding the brain, adverselyincluding the brain, skeleton, and skin as well as
the cardiovascular and genitourinary systems
The concentrations and functions of hormone receptors vary in these organs
and systems
Differences in genetics, BMI, and body habitus may influence the estrogen and androgen levels in post-menopause

Menopause occurs when the ovarian follicular pool is functionally exhausted (Age/POF) or by surgical
removal of both ovaries
The frequency and severityof menopausal
symptoms and the
Differences in genetics, BMI, and body habitus may influence the estrogen and androgen levels in post-menopause
symptoms and the reaction of target tissues
to estrogen deficiency significantly vary among
women

Hot flushes
Sweat (nocturnal)
Anxiety
Sleep disturbances (chronic or transient):
Anxiety
Panic attack
Fatigue
Irritability
Inability to concentrate
Difficulty falling asleep
Early awakening
Trouble to resume sleep
Irregular sleep schedule

Libido
Vaginal lubrication
Premenstrual syndrome
Dispareunia
Vaginism
Genitourinary effects:
Incontinence
Nocturia
Vulvovaginal atrophy

After LMP there is a worsening of the premenopausal
symptomsFrontal cortex:
Cognition, Memory, Planning behavioral
Parietal cortex: Perception, Attention
Occipital cortex: visionTemporal cortex: Recognition, Memory
Cerebellum: motor coordination
Hypothalamus: Reproduction, Sexual
behavior, Thermoregulation, Feeding behavior
Hippocampus: short term memory
Amigdala: Emotion

After LMP there is a worsening of the premenopausal
symptoms
Thermoregulation
Serotonine
Feeding behavioir
Serotonine
Depressed mood
Serotonine
Noradrenaline
DOPA
β-endorphin
Noradrenaline
DOPA
β-endorphin
NPY
Noradrenaline
DOPA
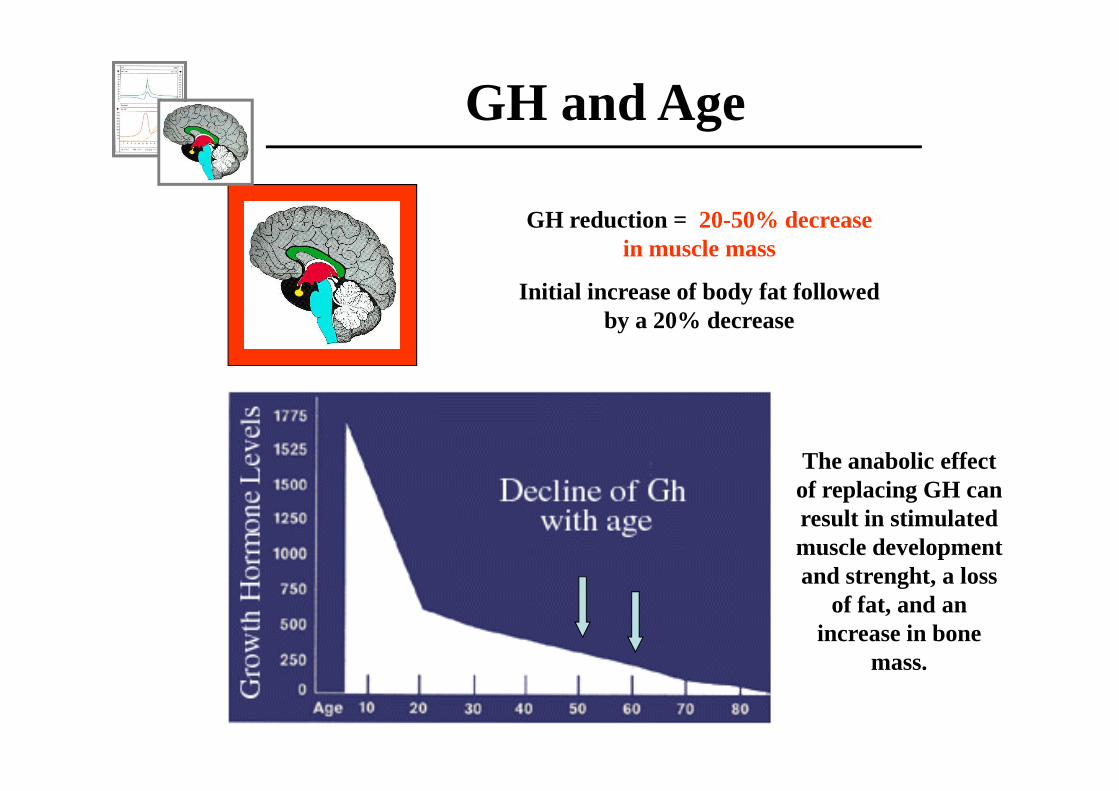
GH reduction = 20-50% decrease in muscle mass
Initial increase of body fat followed by a 20% decrease
GH and Age
The anabolic effect of replacing GH can result in stimulated muscle development and strenght, a loss
of fat, and an increase in bone
mass.

Prl: no significant variations. Sometimes it is possible to observe a slight decrease
Thyroid: no significant variations in TSH values. With age there is an increase of thyroid disorders related to autoimmune diseases

Variable findings have been reported in regard the changes in circulating
androgens in relation to the FMP. However, the possible hirsutism may related to the
increased FAI

Adrenal gland and age
Cortisol unchange until advanced age. Then, because a higher nocturnal rhytmcity, there is a progressive increase with a further increase of sleep
disturbance and hypertension
DHEA
The data on enhancing insulin sensitivity and immune function, as well as quality of life, sex, mood and cognition are inconsistent. In addition, the correlation between elevated DHEA-S levels and better cardiovascular
survival, observed in men, was not found in women.


After 40ty % of women with coronary occlusions
% of plaque index of >3
C
V% of plaque index of >3
% of the intima media thickness (IMT)
V
D

HDL-C
LDL
Dyslipidemia
Triglycerides
HDL/triglycerides
3-7-fold Increased relative risk of CAD
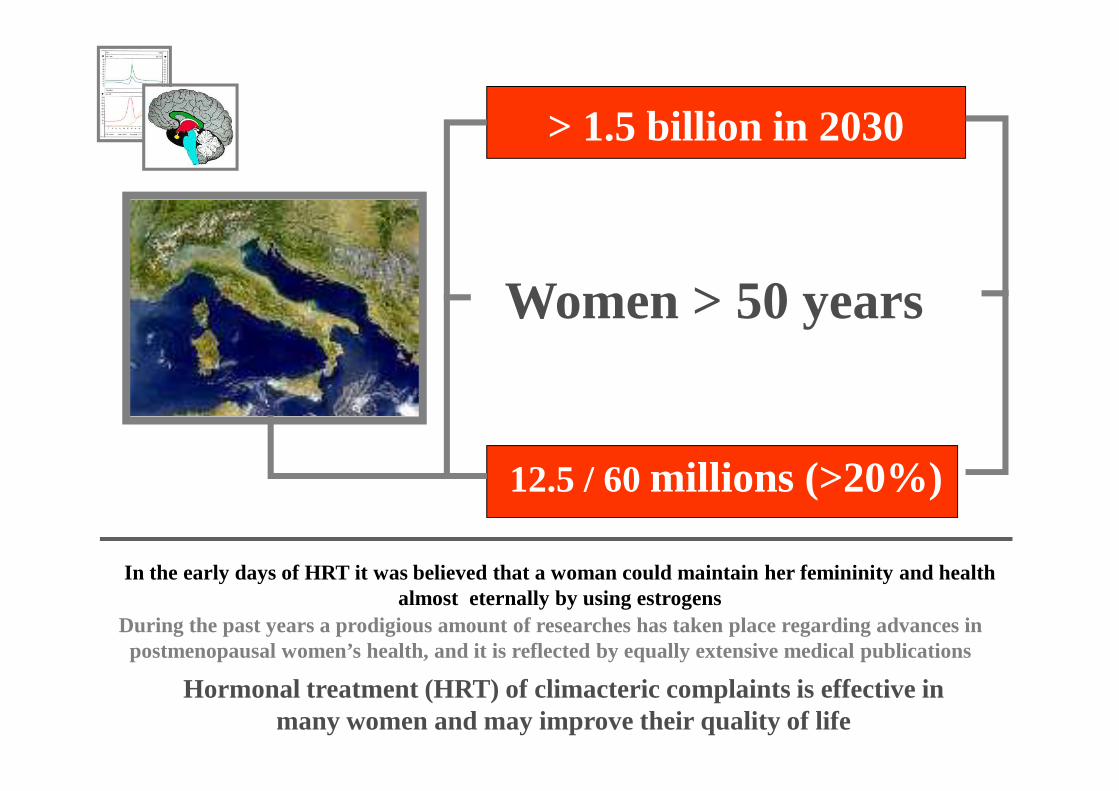
Women > 50 years
> 1.5 billion in 2030
12.5 / 60 millions (>20%)
Hormonal treatment (HRT) of climacteric complaints is effective in many women and may improve their quality of life
During the past years a prodigious amount of researches has taken place regarding advances in postmenopausal women’s health, and it is reflected by equally extensive medical publications
In the early days of HRT it was believed that a woman could maintain her femininity and health almost eternally by using estrogens
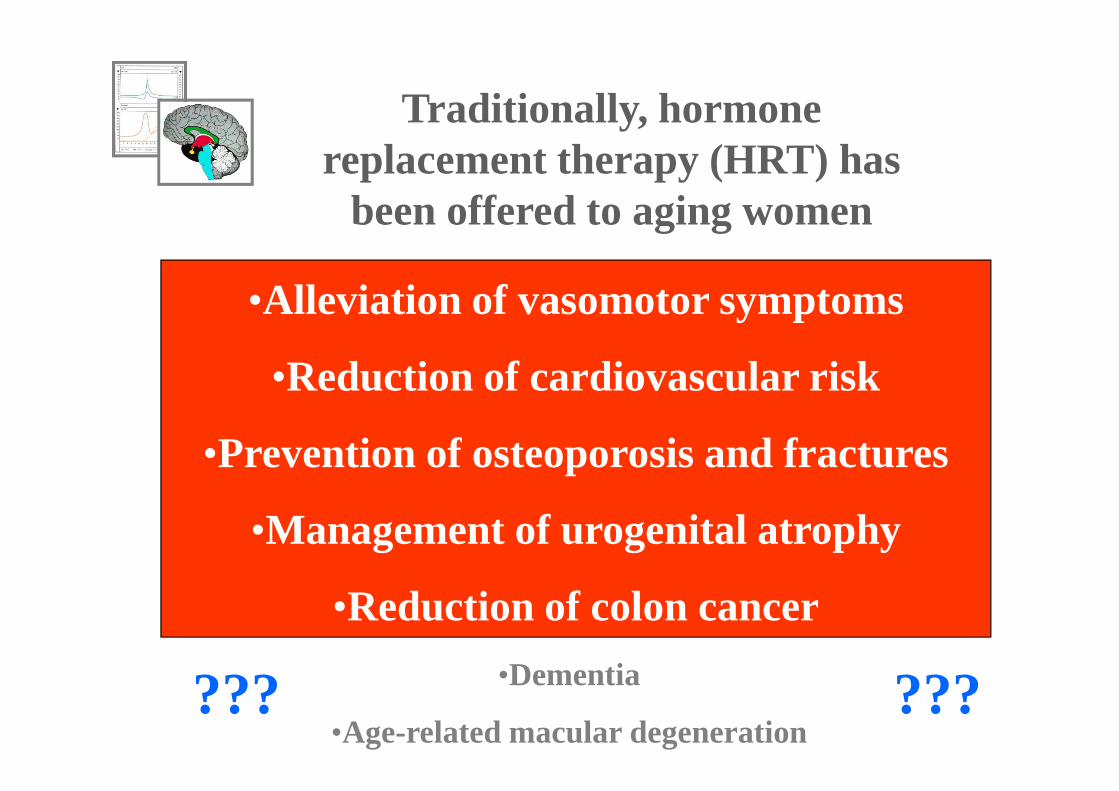
Traditionally, hormone replacement therapy (HRT) has
been offered to aging women
•Alleviation of vasomotor symptoms
•Reduction of cardiovascular risk•Reduction of cardiovascular risk
•Prevention of osteoporosis and fractures
•Management of urogenital atrophy
•Reduction of colon cancer
•Dementia
•Age-related macular degeneration??? ???

% HRT users
4825
<15 % in 1990
41
28
USA UK Italy Thai
15
Women Health Initiative (JAMA, 2002)
Million Women Study (Lancet, 2003)
The picture of omnipotent and safe HRT was tarnished among physicians and mass media

RISCHI E BENEFICI DELL’HRT
• PATOLOGIE CARDIOVASCOLARI ( RR= 1.29)
•ICTUS (RR = 1.41)
•EMBOLIE POLMONARI ( RR = 2.13)
MAGGIORE INCIDENZA DI
•CANCRO DELLA MAMMELLA ( RR = 1.26)
MINORE INCIDENZA DI
•CANCRO DEL COLON -RETTO ( RR = 0.63)
•CANCRO DELL’ENDOMETRIO ( RR = 0.83)
•FRATTURE DA OSTEOPOROSI (RR = 0.66)

MA…IN QUESTO STUDIO CI SONO STATI
SOSTANZIALI ERRORI METODOLOGICI :
WHI
Età media 63.2 aaEtà media 63.2 aa
89% ha iniziato HRT dopo i 55 aa
BMI medio 28.5 (34% >30)
7% affetta da patologie cardiovascolari
37.5 % in terapia antipertensiva
19% usava aspirina come antiaggregante

41
25
48 15
Italy USA UK Thai
Pre WHI (1990-1995)
40
60
80
100
Mean duration of the continous use of HRT (%)
369
Post WHI~ - 40%
0
20
<6 mths 6-12mths
12-18mths
18-24mths
>24 mths
25
15
36

1. Menopausal symptoms are now tolerable
2. I don’t like taking medication
1. Weight gain
2. Breast tenderness or enlargement
3. Water retention/puffiness
Patients convincements
Fear/side effects
3. Water retention/puffiness
4. Decrease in sex drive
5. Fear of developing endometrial/breast cancer becauseMedia
1. Physician didn’t think I needed them
2. Physician never brought this up
Physician’s suggestions
Although HT may improve a woman’s quality of life, each woman has a unique risk profile that might lead to more, or less, benefit
from HT.
Patient preferencesas well as evidence from medical research may influence management decisions
As a result
A standard treatment applied to all A standard treatment applied to all menopausal women will not necessarily meet
the needs of many individual women.
Health-care providers should, therefore, consider the balance between the benefits and risks of treatmentfor individual patient
and likelihood of adherence to the prescribed regimenbefore drawing conclusions or recommending HT


Progesterone or a progestin prevents the overproliferation of the endometrial tissue, but the degree of this effect depends upon its antiestrogenic properties and the dose and duration of treatment
In the last decades many speculations were provided on the role of ESTROGENS in HRT. As regards PROGESTINS, there was a general consensus that they are more or less similar and play a minor role in HRT. This oversimplification could
not have been further from the truth.
Proliferative
Secretive
Administration of progesterone/progestin for 12-14 dys/mth induces secretory/atrophic transformation of the endometrium

The effects of progestins are related to interaction not only with
Progesterone Receptors (PR) Estrogen Receptors (ER)
but also with:
Androgen receptors (AR)Glucocort Receptors (GR)Minercort Receptors (MR)

Which Progestins are New?By convention the older progestins are divided into three generations:
•Ist: Noretynodrel, Nortestosterone, 17-Hydroxyprogesterone derivatives
•IInd : Norgestrel and Levonorgestrel
•IIIrd : Levonorgestrel derivatives (Desogestrel, Gestodene, Norgestimate)
Most of the progestins in these 3 generations were derived from testosterone
Several New Progestins have been synthesized in the last decade for use in HRTs
The new progestins may be defined as a 4th generation: they were designed to bind very specifically to PR, and to exert no androgenic, estrogenic, or glucocorticoid adverse effects
• Pregnanes:Nestorone Progestational and antigonadotropinic
Nomegestrol AcetateAntigonadotropinic
Trimegestone Progestational
•Estranes: Dienogest Antiandrogenic
Drospirenone Antimineralcorticoid/Antiandrogenic

DROSPIRENONE
Is derived from spironolactone and is, essentially, an
antimineralcorticoid progestin. In addition, it has some
antiandrogenic actions.
Estranes:
antiandrogenic actions.
In rats, the antimineralcorticoid activity was associated with reduction in sodium and water retentiondue to partial suppression of the renin-
angiotensin-aldosterone system
Drospirenone has been associated with weight lossrather than weight gain as observed in other HRT.
In a small randomised study in postmenopausal women with hypertension treated with enalapril, Drospirenone produced an additive antihypertensive
effect.
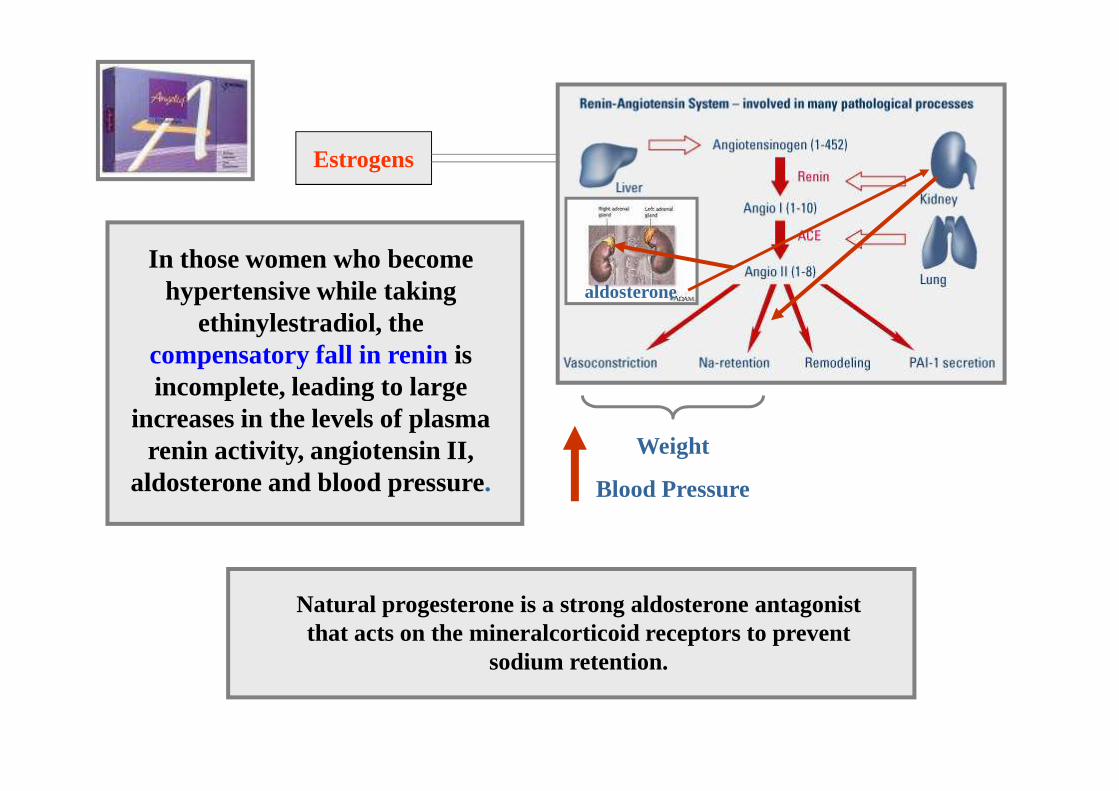
Estrogens
In those women who become hypertensive while taking
ethinylestradiol, thecompensatory fall in reninis incomplete, leading to large
aldosterone
Weight
Blood Pressure
incomplete, leading to large increases in the levels of plasma
renin activity, angiotensin II, aldosterone and blood pressure.
Natural progesterone is a strong aldosterone antagonist that acts on the mineralcorticoid receptors to prevent
sodium retention.

-1,6
-1,2
-0,8
-0,4
0
0,4
0,8
1,2
Estradiol Angeliq
KgWeight modifications
Estradiol Angeliq
1 3 6 12 Mths
0
25
50
75
100
Abdom bloating Breast tendern Swelling of extrem
Improvement in severity of somatic symptoms 6 mths after a HRT
switch

Drospirenonedoes not antagonize the benificial effect of estradiol on lipids. Angeliq® is
associated with favorable effects associated with favorable effects on total-cholesterol and LDL and has neutral effects with respect to
HDL-cholesterol

A dose-dependent effect in hypertensive w
omen
dependent effect in hypertensive wom
en

40
60
80
HOT FLASHES AND THERAPY
n°
0
20
40
Pre 8 12 16 Wks
Placebo EE+DRSP 1mgEE+DRSP 2 mg EE+DRSP 3 mg

80
100
%
Clinical efficacy for induction of complete amenorrhea/absence of spotting
60
3 6 12 wks
EE+DRSP 1mg EE+DRSP 2 mg EE+DRSP 3 mg
%
No cases of endometrial hyperplasia or carcinoma. 85-92% of women had an inactive/atrophic endoemtrium

Age >50 (51-56)
BMI <30 (22.5-27.5)
Multiparae (2-3)
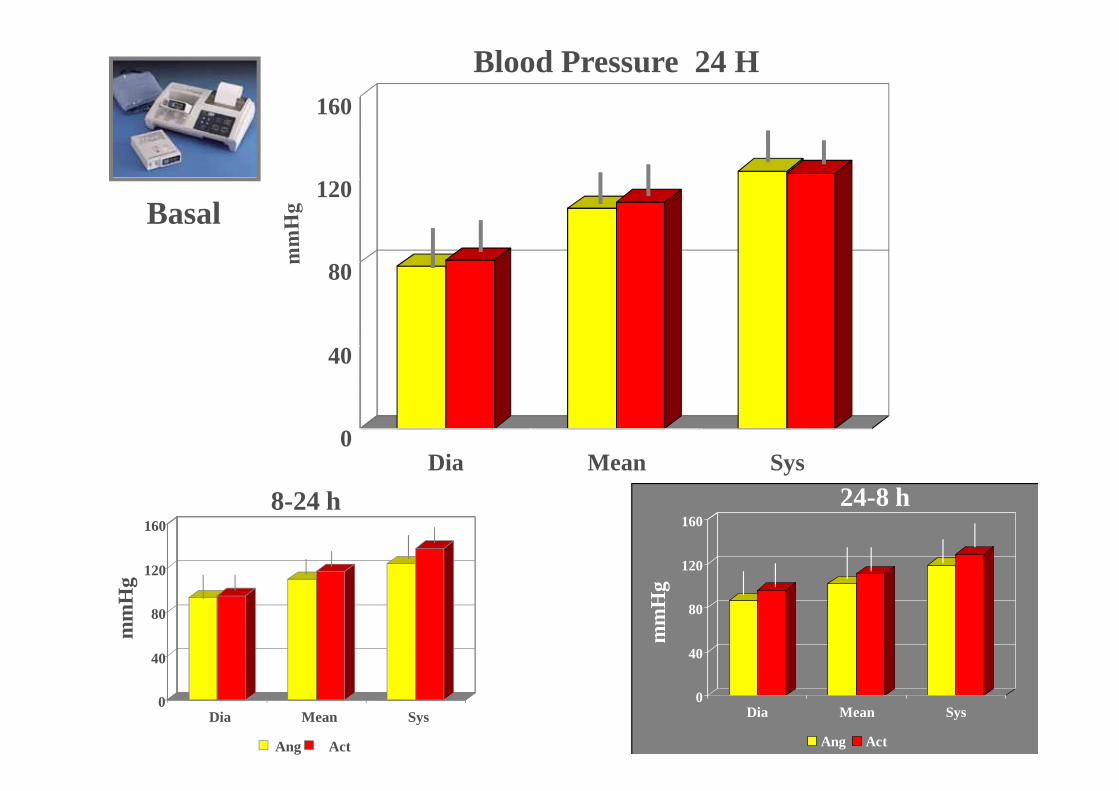
Basal: before therapy
N=15 N=15No: dyslipidemia/diabetes/hypertension/
gynecological disorders
Drosp 2 mg + estr 1 mgNoretist Ac 0.5+ estr 1 mg
After 6 mths
Drosp 2 mg + estr 1 mgNoretist Ac 0.5+ estr 1 mg
40
80
120
160
Blood Pressure 24 H
Basal
0Dia Mean Sys
0
40
80
120
160
Dia Mean Sys
Ang Act
24-8 h
0
40
80
120
160
Dia Mean Sys
Ang Act
8-24 h
mm
Hg
mm
Hg

40
80
120
160Blood Pressure 24 H
6 Mths
0Dia Mean Sys
0
40
80
120
160
Dia Mean Sys
Angt Act
8-24 h
mm
Hg
0
40
80
120
160
Dia Mean Sys
Ang Act
24-8 h
mm
Hg

2
4
%
Basal Blood Pressure
0
2
>140 >90 >140 >90 >120 >8024 h 8-24 h 24-8 h
mmHg
Wake-up: 118±4 mmHg vs 121±4 mmHg; p=0.058
Ang
Act

2
4
%
6 Mths Blood Pressure
0
2
>140 >90 >140 >90 >120 >8024 h 8-24 h 24-8 h
mmHg
Wake-up: 116±2 mmHg vs 120±3 mmHg; p=0.067
Ang
Act
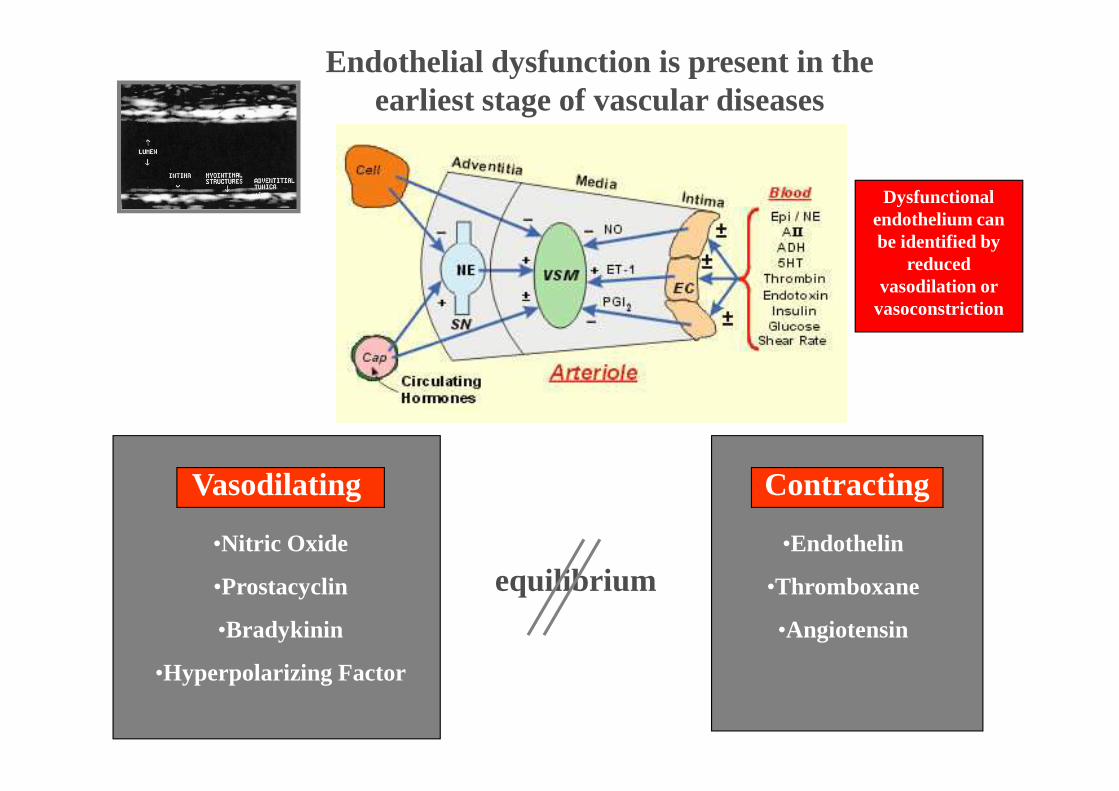
Endothelial dysfunction is present in the earliest stage of vascular diseases
Dysfunctional endothelium can be identified by
reduced vasodilation or
vasoconstriction
Vasodilating
•Nitric Oxide
•Prostacyclin
•Bradykinin
•Hyperpolarizing Factor
Contracting
•Endothelin
•Thromboxane
•Angiotensin
equilibrium

40
42
44
Brachial Artery Flow -mediated Vasodilation
Normal flow-mediated vasodilation is approximately >10% using the upper-arm occlusion technique
Basal
34
36
38
40
Pre 30" 60" 120"
Act Ang
mm
Time Cuff-release

40
42
44
Brachial Artery Flow -mediated Vasodilation
Normal flow-mediated vasodilation is approximately >10% using the upper-arm occlusion technique
6 Mths
34
36
38
40
Pre 30" 60" 120"
Act Ang
mm
Time Cuff-release
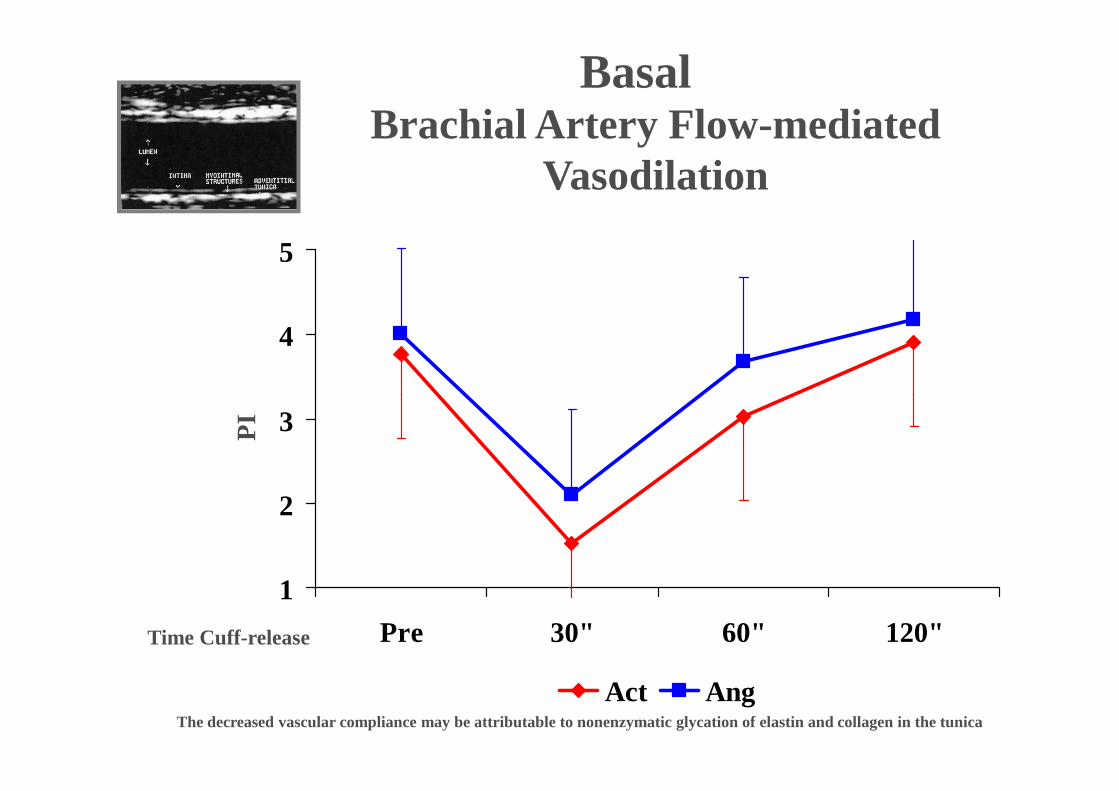
4
5
Brachial Artery Flow -mediated Vasodilation
Basal
1
2
3
Pre 30" 60" 120"
Act Ang
PI
Time Cuff-release
The decreased vascular compliance may be attributable to nonenzymatic glycation of elastin and collagen in the tunica
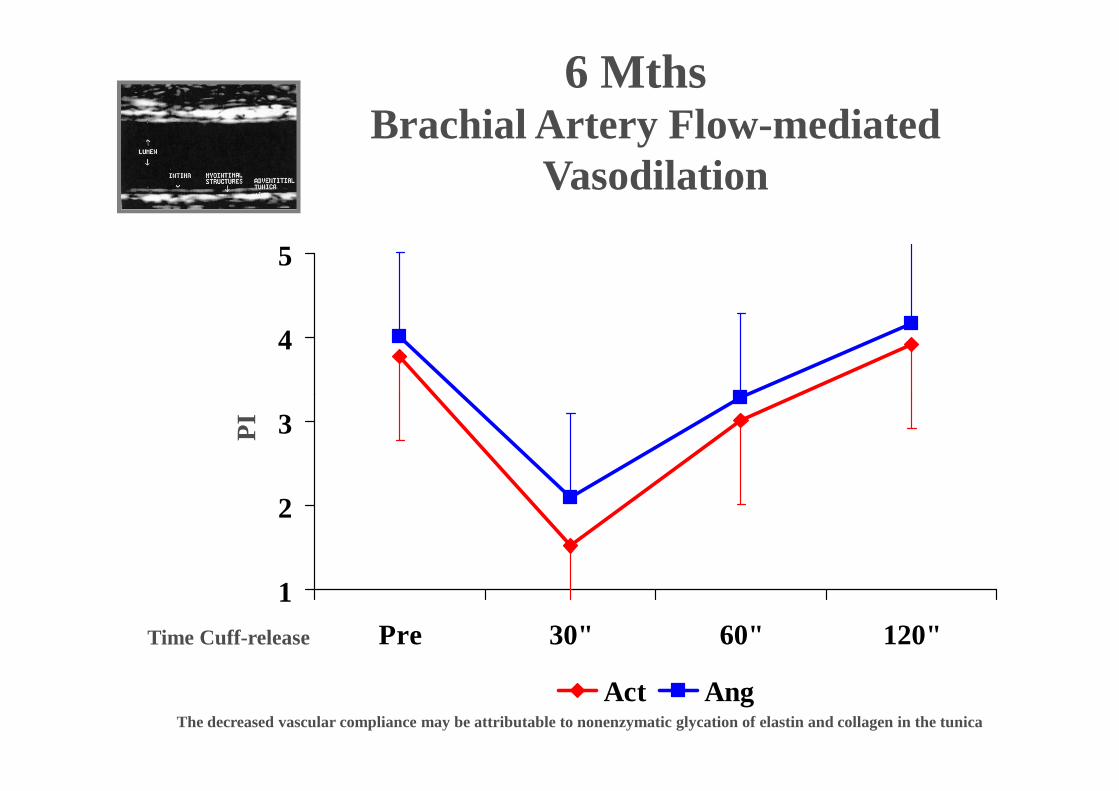
4
5
Brachial Artery Flow -mediated Vasodilation
6 Mths
1
2
3
Pre 30" 60" 120"
Act Ang
PI
Time Cuff-release
The decreased vascular compliance may be attributable to nonenzymatic glycation of elastin and collagen in the tunica
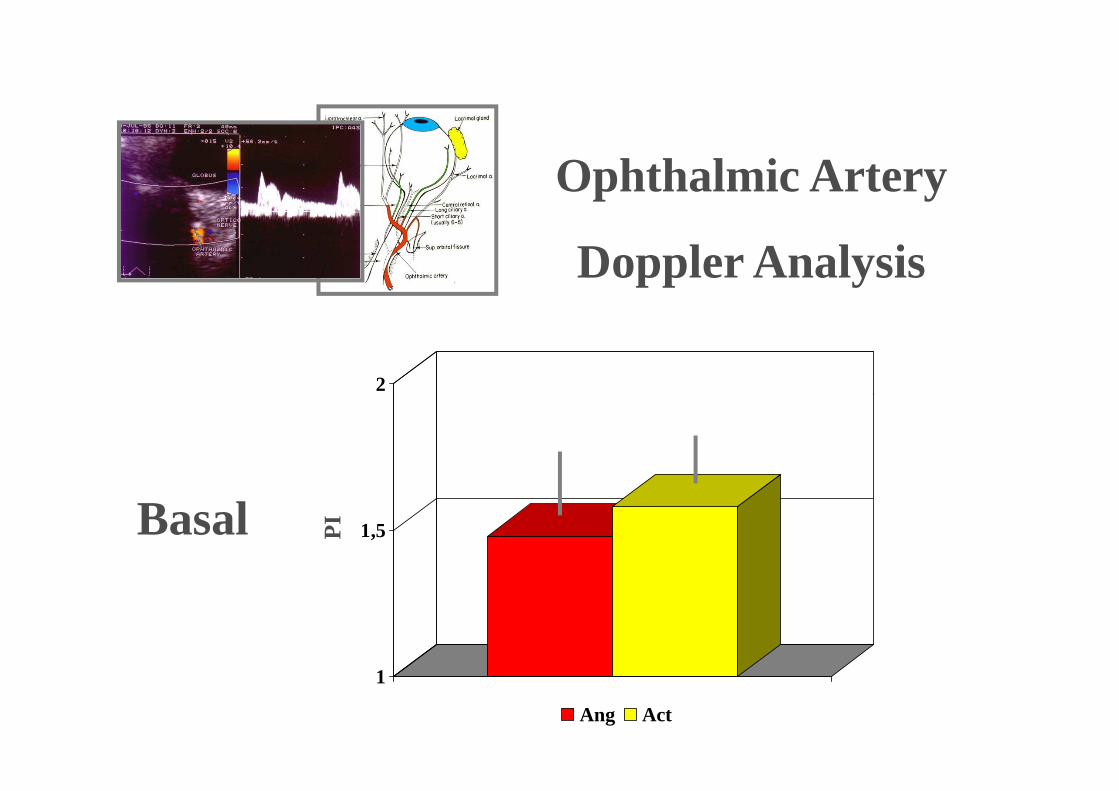
2
Ophthalmic Artery
Doppler Analysis
1
1,5
Ang Act
PIBasal

2
Ophthalmic Artery
Doppler Analysis
1
1,5
Ang Act
PI6 Mths

Although no differences were found in HRT users
it would seem prudent to
CONCLUSIONS
it would seem prudent to reccomend lifestyle modifications (i.e. smoking, physical inactivity,
salt loading, job or marital/familial stress), particularly for obese
women