ORIGINAL RESEARCH INJURY RISK IS ALTERED BY PREVIOUS ...
13
The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 583 ORIGINAL RESEARCH INJURY RISK IS ALTERED BY PREVIOUS INJURY: A SYSTEMATIC REVIEW OF THE LITERATURE AND PRESENTATION OF CAUSATIVE NEUROMUSCULAR FACTORS Jessica Fulton, PT, DPT, HFS 1 Kathryn Wright, PT, DPT 1 Margaret Kelly, PT, DPT, CSCS 1 Britanee Zebrosky, PT, DPT, CSCS 1 Matthew Zanis, PT, DPT, ATC, CSCS 1 Corey Drvol, PT, DPT 1 Robert Butler, PT, PhD 1 ABSTRACT Background: Active adults commonly present with lower extremity (LE) injuries from a variety of professional and amateur sports activities. Decreased LE function significantly alters daily life and subsequent injuries increase this impact. The purpose of this systematic review was to examine the association between previous injury and the risk of re-injury, and to describe the changes in kinematics and motor programming that may contribute to this relationship. Methods: A preliminary search was conducted to determine the four most common LE injuries on PubMed, CINAHL and Web of Science. These injuries, in a healthy active adult population, were hamstring strain (HS), anterior cruciate ligament injury (ACL), achilles tendon pathology, and ankle sprain. After these injuries were established, the search for this systematic review found evidence relating these injuries to re-injury. Articles related to degenerative changes were excluded. Twenty-six articles were included in the systematic review detailing the risk of re-injury from a previ- ous injury and were graded for quality. Results: ACL injury was linked to a successive injury of the same ACL, and other injuries in the LE. HS was associ- ated with subsequent ipsilateral HS and knee injuries. Previous achilles tendon rupture increased the risk of an analo- gous injury on the contralateral side. An ankle sprain was associated with a re-injury of either the ipsilateral or the contralateral ankle. Post-injury changes were present in strength, proprioception, and kinematics, which may have led to overall changes in motor control and function. Conclusion: This review provides insight into the changes occurring following common LE injuries, how these changes potentially affect risk for future injury, and address the needs of the active adult population in rehabilitation. Clinical Relevance: Current research on previous injury and re-injury is of high quality, but scarce quantity. Deficits following an injury are known, but how these deficits correlate or lead to re-injury requires further exploration. Keywords: Injury, motor programming, re-injury Level of Evidence: 1 1 Duke University, Durham, NC, USA CORRESPONDING AUTHOR Robert J. Butler, PT, PhD Doctor of Physical Therapy Division Duke University DUMC 104002 Durham, NC 27705 Phone: 919.681.7225 Fax: 919.684.1846 E-mail: [email protected] IJSPT
Transcript of ORIGINAL RESEARCH INJURY RISK IS ALTERED BY PREVIOUS ...

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 583
ORIGINAL RESEARCH
INJURY RISK IS ALTERED BY PREVIOUS INJURY:
A SYSTEMATIC REVIEW OF THE LITERATURE AND
PRESENTATION OF CAUSATIVE NEUROMUSCULAR
FACTORS
Jessica Fulton, PT, DPT, HFS1
Kathryn Wright, PT, DPT1
Margaret Kelly, PT, DPT, CSCS1
Britanee Zebrosky, PT, DPT, CSCS1
Matthew Zanis, PT, DPT, ATC, CSCS1
Corey Drvol, PT, DPT1
Robert Butler, PT, PhD1
ABSTRACTBackground: Active adults commonly present with lower extremity (LE) injuries from a variety of professional and amateur sports activities. Decreased LE function significantly alters daily life and subsequent injuries increase this impact. The purpose of this systematic review was to examine the association between previous injury and the risk of re-injury, and to describe the changes in kinematics and motor programming that may contribute to this relationship.
Methods: A preliminary search was conducted to determine the four most common LE injuries on PubMed, CINAHL and Web of Science. These injuries, in a healthy active adult population, were hamstring strain (HS), anterior cruciate ligament injury (ACL), achilles tendon pathology, and ankle sprain. After these injuries were established, the search for this systematic review found evidence relating these injuries to re-injury. Articles related to degenerative changes were excluded. Twenty-six articles were included in the systematic review detailing the risk of re-injury from a previ-ous injury and were graded for quality.
Results: ACL injury was linked to a successive injury of the same ACL, and other injuries in the LE. HS was associ-ated with subsequent ipsilateral HS and knee injuries. Previous achilles tendon rupture increased the risk of an analo-gous injury on the contralateral side. An ankle sprain was associated with a re-injury of either the ipsilateral or the contralateral ankle. Post-injury changes were present in strength, proprioception, and kinematics, which may have led to overall changes in motor control and function.
Conclusion: This review provides insight into the changes occurring following common LE injuries, how these changes potentially affect risk for future injury, and address the needs of the active adult population in rehabilitation.
Clinical Relevance: Current research on previous injury and re-injury is of high quality, but scarce quantity. Deficits following an injury are known, but how these deficits correlate or lead to re-injury requires further exploration.
Keywords: Injury, motor programming, re-injury
Level of Evidence: 1
1 Duke University, Durham, NC, USA
CORRESPONDING AUTHORRobert J. Butler, PT, PhDDoctor of Physical Therapy DivisionDuke UniversityDUMC 104002Durham, NC 27705Phone: 919.681.7225Fax: 919.684.1846E-mail: [email protected]
IJSP
T

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 584
INTRODUCTIONAttempts at healthy living spur an increase in activ-ity in the adult population and consequently, also in the risk for injury. Traumatic and atraumatic inju-ries are a common consequence of new or increased activity. Following injury, patients often experience decreased functional capacity. Several authors have described previous injury as the greatest risk fac-tor for future injury secondary to changes along the kinematic chain, i.e. proprioceptive deficits, reduced range of motion, excessive flexibility, and scar tis-sue accumulation.1-3 Knowledge of these intrinsic changes may benefit rehabilitation models for active adults with the potential of reducing re-injury rates and improving quality of life, while also helping to lower overall medical costs.
A recent systematic review of the literature (SR) determined that the most common lower extremity injuries in a healthy active adult population were, in no specific order, hamstring strain (HS), ante-rior cruciate ligament (ACL) injury, achilles tendon pathology, and ankle sprain. Due to the intricate relationships between joints during movement of the lower extremity, changes often occur at sites other than the initial point of injury.4 Regional inter-dependence is an important key to understanding how anatomic variables occurring within the kinetic chain may contribute to re-injury.5 Previously, researchers have examined these common inju-ries and the subsequent changes in kinematics and motor programming.2,6-9 However, the connection of these changes to subsequent lower extremity inju-ries has not been examined.
The purpose of this systematic review is to establish the most common lower extremity injuries and the risk of re-injury or subsequent injury as it relates to alterations in kinematics and motor programing. This review combines an analysis of established data on the risk of re-injury following a lower extremity injury with a qualitative discussion on the factors that contribute to this relationship. By developing a greater understanding of the kinematic and motor programming changes following injury, the authors hope to illuminate how one injury to the lower extremity may increase the risk for re-injury or sub-sequent injury. By integrating information on the relationship between injury and subsequent injury,
rehabilitation could focus on not only the immediate injury, but also potentially reducing future injury.
METHODSA five-stage process was used to select studies. The first stage involved a search on PubMed, CINAHL, and Web of Science using the search terms “injuries AND lower extremity AND prevalence AND adults”. This search provided data that was utilized to select the four most common injuries that occur in the lower extremities. This search yielded 158 articles of which 17 were ruled in based on a title and abstract screen. From here the articles were read for full text and six articles were chosen for their specific research on injury prevalence according to these search terms. From the information presented in these articles, the four most common musculoskele-tal injuries were determined to be ankle sprain, ACL injury, HS, and achilles injury.
The second search for the topic of the current review utilized the terms “ankle sprain OR ACL injury OR Achilles injury OR hamstring strain AND previous injury” in PubMed and CINAHL (Figure 1). A filter of “ages 19-44” was applied to this search. Next, two independent reviewers performed an initial assess-ment of the identified papers based on title. For all assessments, inclusion criteria included articles dealing with an active, healthy, athletic population (including military personnel); directly related to one of the four selected injuries; concerned with motor control or kinematics; as well as describing injury as a result of re-injury. Articles dealing with osteoarthritis or degenerative injury were excluded. Articles writ-ten in languages other than English were excluded, unless a translated version was available. These crite-ria were chosen based on the immense return utiliz-ing the selected search terms and the need to specify the population most likely at risk for re-injury. Sec-ond, two independent reviewers performed an assess-ment based on the articles’ abstract. For both the title and abstract assessments, all articles that received a “Yes” rating by one reviewer were kept. Finally, a full text review was performed, dividing articles equally among three teams of reviewers. Each team of two independent reviewers assessed each set. Any arti-cles published before the year 2000 were excluded. Articles that received a split rating (one “Yes” and

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 585
one “No”) were reviewed by another independent reviewer who made the final decision.
Four independent reviewers using the Quality Assessment of Diagnostic Accuracy Studies (QUA-DAS) tool completed grading of the articles regard-ing injury as a risk of re-injury.10 The QUADAS is a 14-question tool to determine the internal and exter-nal validity of a study. The questions are answered “yes, no, N/A or unclear”, for which one point is awarded for every “yes” answer. The QUADAS exam-ines such biases as spectrum, selection, disease progression, and verification bias. Two reviewers graded articles related to ACL injuries and HS, while two other reviewers graded articles regarding Achil-les and ankle injuries. After independently grading these articles, each pair came to a consensus on scor-ing criteria for each article. A score of 10 or more was considered “high quality, low risk of bias” and a score below 10 was considered “low quality, high risk of bias”.11 Cook states, “systematic reviews that use the QUADAS instrument provide a qualitative assessment of design with recognition that weak-nesses in selected regions may alter some test find-ings more than others.”10(p. 98) Thus, with this grading
system it can be stated that despite possible bias(es) existing within an article, overall quality could still be considered to be good. One of the articles, Friel et al,12 was not evaluated using the QUADAS due to the study design being Ex-post Facto. Therefore, two independent reviewers individually graded this article as “poor”, “fair”, or “good” and came to a con-sensus on the grading of the article.
All five articles for ACL injury relating to subsequent injury were of high quality and low risk of bias, with scores ranging from 10 to 12 based on the QUADAS criteria. Of the seven HS related studies; only one was graded to be of low quality and high risk of bias, with a score of 8. The other articles ranged from a score of 10 to 13, indicating high quality and low risk of bias. Similarly, high quality and low risk of bias was evident in the three articles for the Achil-les group, with scores ranging from 11 to 12, and the ankle injury group where the ten studies scores ranged from 11 to 13. With these findings and analy-ses, the authors concluded that appropriate designs have been formulated and implemented resulting in outcomes that could be used for evidence-based practice.
Figure 1. Flow of literature search and review of studies

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 586
RESULTS
Hamstring StrainFive articles were found correlating HS with subse-quent strains of the same muscle group (Appendix 1). In a study analyzing elite level Australian foot-ball players, the authors concluded that a HS strain within the previous 12 months was a strong predic-tor of future HS.3 The football players were 4.3 times more likely to incur another HS as opposed to players without history of previous HS.3 In a similar popula-tion of Australian football players and track and field athletes, 34% of HS were recurrences and previous strain was the most common reason for subsequent HS.13 In addition, 27% of all HS in the Australian Foot-ball League (AFL) were caused by previous HS, which increased the risk of recurrence by 11.6. It is unclear, however, if the cause of increased recurrence is due to accumulated microscopic muscle damage or the presence of a single injurious event.16 No matter the cause of HS, the research clearly indicates that previ-ous HS is an important risk factor for future HS.14,15
Anterior Cruciate Ligament InjuryACL injury has been linked to a successive injury of the same ACL and other impairments or injuries in the lower extremity (Appendix 2). In one study, ACL graft ruptures occurred in 6.4% of subjects and a contralateral ACL rupture followed at a frequency of 5.7%.17 In addition to a previous injury of the ACL, activity level after the injury was indicated to predict another injury of the same or contralateral ACL.17 In elite footballers, 70% of current ACL injuries occurred on the same leg as a previous ACL injury.2 Ten per-cent of subjects in another study reported traumati-cally reinjuring their knee, resulting in disruption of the graft, between four and twelve months after ACL reconstruction.18 Research indicates that re-injury can occur to the same or contralateral ACL following an initial ACL injury, when that injury was treated conservatively or surgically. Inadequate landing force attenuation was identified as imposing abnor-mal forces after reconstruction on the musculoskele-tal components, thus increasing the risk of re-injury.19
Achilles Tendon Injury There is little research exploring achilles tendon injury and its effect on re-injury or subsequent injury (Appendix 3). However, one article discussed that
following an Achilles tendon injury among the adult population, risk of re-injury is greater in individuals 30 years or younger.20 Another study linked previ-ous Achilles tendon rupture to a risk of an analogous injury on the contralateral side, stating that an indi-vidual is 176 times more likely to injure the opposite side approximately 3.1 years later compared to an individual without a previous Achilles tendon pathol-ogy. The authors proposed a multifactorial explana-tion to this connection suggesting an increased risk due to degenerative changes, a genetic predisposition for tendon ruptures, or disuse atrophy of the contra-lateral tendon from overall decreased physical activ-ity due to immobilization of the injured leg.21
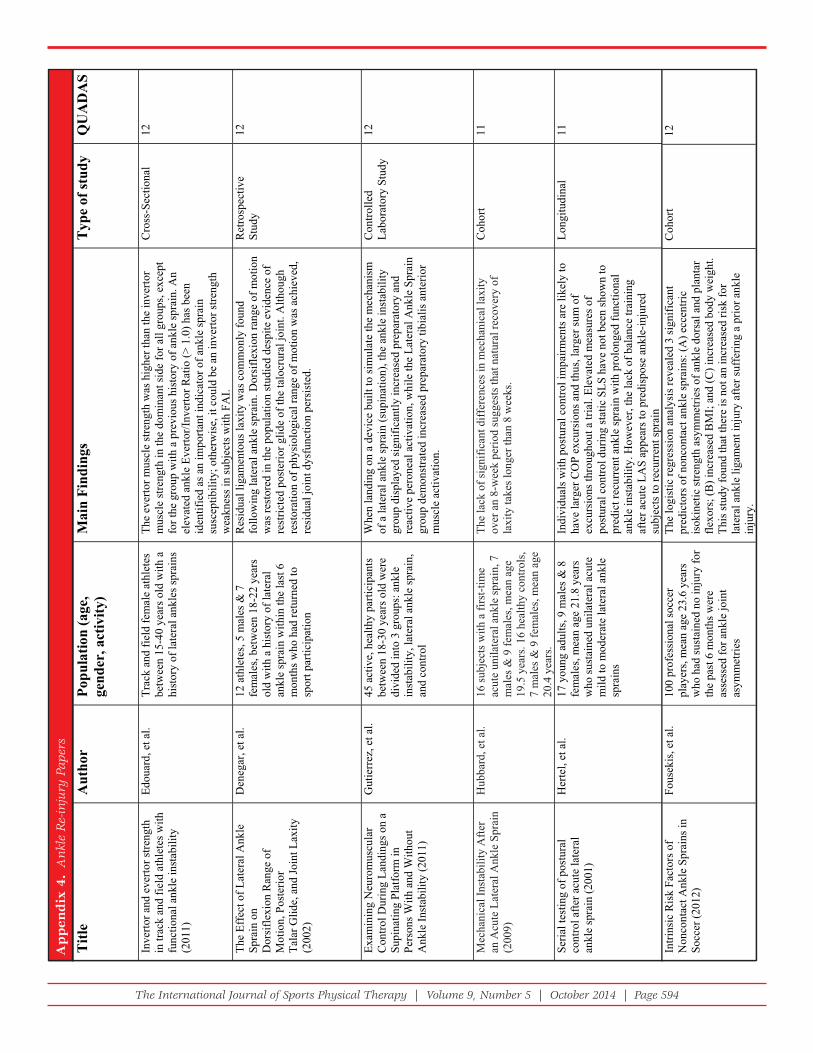
Ankle SprainIn accordance with the research, a single ankle sprain is the most common injury resulting in a secondary sprain of the ipsilateral or contralateral ankle among the active adult population (Appendix 4). In a study investigating the effect of ankle sprain on recurrent ankle sprains in 202 elite Greek track athletes, there was a higher risk of re-injury for low-grade ankle sprains as opposed to high-grade ankle sprains.22 The authors discovered that 17.8 percent of their athletes suffered a second lateral ankle sprain by the end of the follow-up period.22 In another study involving 65 professional male football play-ers, the recurrence of a secondary ankle sprain fol-lowing the same initial injury was 50 percent higher than those without a previous ankle sprain. The authors also found that 75.38 percent of these ath-letes had sustained multiple ankle sprains (63.27 percent in bilateral ankles; 24.49 percent in the dominant ankle only) during their entire career up until the point at which the study was concluded.23 Pefanis et al found that a previous ankle sprain was the most important statistical factor leading to a subsequent ankle sprain, increasing the occurrence by 21 percent.24 Additional research in this area has suggested that leg dominance may be a factor lead-ing to injury. Williams and colleagues reported that in college freshman physical education students 59 percent of recurrent ankle sprains occurred in the dominant foot among 44 of the 241 participants.25 In conclusion, the results of this SR indicate that an ankle sprain is linked to both re-injury and subse-quent injury to the contralateral side.

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 587
DISCUSSIONThe results of this systematic review revealed a relationship between previous injury and re-injury in each lower extremity injury that was studied. Overall, the vast majority of articles reviewed dis-cussed this relationship in detail and suggested many possibilities for why this trend exists. Re-injury was suggested to be associated with deficits in neuromuscular factors that are present following injuries.2,3,18,21,26 The goal of this discussion will be to qualitatively examine the changes that were iden-tified in papers examined that occurred post-injury and how they were proposed to link injury to re-injury. Following injury, researchers have identified alterations occurring in strength, proprioception, and kinematics, which have led to overall changes in motor control and function.2,13,15,25,27-35 This combi-nation of insight may offer valuable information to clinicians for reduction of re-injury.
Strength deficits between affected and unaffected limbs as well as imbalances between muscle groups have been documented post hamstring strain, post ACL rupture, and post Achilles tendon rup-ture.7,9,15,27-29,33,36,37 Without recovering muscle strength of involved muscles following an initial injury, the stability of joints, biomechanics of motion, and the ability to safely participate in activity are likely com-promised. Several authors suggested that incorpo-rating strength training and standards for strength following injury is necessary in order to decrease long-term muscular deficits that could go on to affect kinematics and motor control both proximal and dis-tal to the injury, further increasing the risk of subse-quent injury.7,9,15,27-29,33,36,37
Proprioceptive deficits, altered muscular recruit-ment patterns, and changes in static and dynamic stability occur from altered neuronal firing and decreased sensory awareness within joint and mus-cle tissue following ACL rupture, Achilles tendon injury, and ankle sprains.9,19,31,38-52 Authors of papers reviewed described variations in postural sway, gait mechanics, and decreased dynamic stability within functional activities that might place individuals at higher risk for re-injury.39,40,42,48,50
Changes in strength and proprioception, which very likely occur together, contribute to the next factor
to be addressed: changes in lower extremity bio-mechanics following injury. The observed biome-chanical changes that have been documented are changes in peak torque, altered gait mechanics, and intra-articular and intra-muscular forces (including, compressive, tensile, and shear forces) in the ham-string, ACL, and ankle.13,30,47,48,53-58 Comprehensive biomechanical evaluation of the patient is pertinent in order to correctly develop treatment strategies that positively affect vectors of force displacement within the body, with the aim of normalizing joint mechanics. Suboptimal mechanics during high-level functional tasks have at times been associated with risk of future sports injuries.59-61 The authors of this systematic review believe that by examining and addressing joint kinematics post injury, patients may have the potential to return to functional activ-ity at a greater rate and avoid potential re-injury.
This systematic review adequately describes the major risk of re-injury post initial injury in the adult population. The high risk of re-injury described, stresses the importance of comprehensive rehabili-tation that uses the theory of regional interdepen-dence to adequately mitigate local, proximal, and distal deficits in strength, proprioception, and lower extremity mechanics.5 Future research establishing standards for the aforementioned deficits and devel-oping rehabilitation programming that addresses these limitations is important, and it may be possible to remove the previous injury risk factor component with regard to risk of future injury. In addition to the health benefits of preventing re-injury, medical costs may also be reduced which would lower the economic burden of the initial injury.
Limitations to the study are typical of those attrib-uted to systematic reviews. This paper focused on the four most common lower extremity injuries; however, the breadth of injuries incurred in the adult population extends beyond those examined in this research. Additionally, this research cannot be expanded beyond the active adult population. While the relationship between injury and re-injury was described, the ability to generalize the qualitatively identified variables including kinematic alterations, motor control deficits, and musculoskeletal changes to other injuries requires further exploration. To maintain the focus of this SR, the authors did not

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 588
attempt to discuss a standardized way to examine a patient for these changes, nor was it appropriate to discuss specific interventions to treat these impair-ments as these components were beyond the scope of this systematic review. Although there were stan-dardized criteria for inclusion and exclusion of arti-cles, the selection process has inherent inter-rater reliability concerns, such that a third party reviewer was utilized if raters could not agree.
Future StudiesFuture research should be performed in order to determine standardized outcome tools that could be used to objectively identify changes that occur following injury that relate to the risk for future injury. Based on the current research, it appears that it would be beneficial to include outcome tools that assess a patient’s movement patterns following injury in order to optimize function from a regional interdependence approach prior to returning the patient to his/her previous level of activity. These tests may be beneficial in examining patients post-treatment to assess for functional return to activity. Furthermore, research should be performed in order to identify the most beneficial interventions and strategies used to address changes following injury and to develop protocols to reduce risk of re-injury.
CONCLUSIONIn conclusion, this systematic review of the literature identified and reviewed 26 articles, which describe a relationship between injury and re-injury for the four most common lower extremity injuries. Overall, the studies on re-injury were of moderate to high qual-ity, but the quantity of research was scarce. Evidence regarding the hamstring strain, ACL rupture, achil-les tendon injury, and ankle sprain are of moderate to high quality in relation to this topic, aside from one article with a low quality rating.3 More analysis on the relationship between injury and re-injury is needed. Motor control and kinematic deficits follow-ing injury have been suggested, but their direct rela-tion to re-injury requires further exploration.
REFERENCES 1. Hagglund M, Walden M, Ekstrand J. Previous injury
as a risk factor for injury in elite football: A prospective study over two consecutive seasons. Br J Sports Med. 2006;40(9):767-772.
2. Walden M, Hagglund M, Ekstrand J. High risk of new knee injury in elite footballers with previous anterior cruciate ligament injury. Br J Sports Med. 2006;40(2):158-62; discussion 158-62.
3. Gabbe BJ, Bennell KL, Finch CF, Wajswelner H, Orchard JW. Predictors of hamstring injury at the elite level of australian football. Scand J Med Sci Sports. 2006;16(1):7-13.
4. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Defi cits in neuromuscular control of the trunk predict knee injury risk: A prospective biomechanical-epidemiologic study. Am J Sports Med. 2007;35(7):1123-1130.
5. Wainner RS, Whitman JM, Cleland JA, Flynn TW. Regional interdependence: A musculoskeletal examination model whose time has come. J Orthop Sports Phys Ther. 2007;37(11):658-660.
6. Brown C, N., Padua D, A., Marshall S, W., Guskiewicz K, M., Gribble P, A. [Commentary on] hip kinematics during a stop-jump task in patients with chronic ankle instability. J Athletic Train. 2011;46(5):461-470.
7. Ageberg E, Pettersson A, Fridén T. 15-year follow-up of neuromuscular function in patients with unilateral nonreconstructed anterior cruciate ligament injury initially treated with rehabilitation and activity modifi cation: A longitudinal prospective study. Am J Sports Med. 2007;35(12):2109-2117.
8. Silder A, Thelen DG, Heiderscheit BC. Effects of prior hamstring strain injury on strength, fl exibility, and running mechanics. Clin Biomech (Bristol, Avon). 2010;25(7):681-686.
9. Bressel E, Larsen BT, McNair PJ, Cronin J. Ankle joint proprioception and passive mechanical properties of the calf muscles after an achilles tendon rupture: A comparison with matched controls. Clin Biomech (Bristol, Avon). 2004;19(3):284-291.
10. Cook C, Cleland J, Huijbregts P. Creation and critique of studies of diagnostic accuracy: Use of the STARD and QUADAS methodological quality assessment tools. J Man Manip Ther. 2007;15(2):93-102.
11. Reiman MP, Goode AP, Hegedus EJ, Cook CE, Wright AA. Diagnostic accuracy of clinical tests of the hip: A systematic review with meta-analysis. Br J Sports Med. 2013;47(14):893-902.
12. Friel K, McLean N, Myers C, Caceres M. Ipsilateral hip abductor weakness after inversion ankle sprain. J Athletic Train. 2006;41(1):74-78.
13. Brockett CL, Morgan DL, Proske U. Predicting hamstring strain injury in elite athletes. Med Sci Sports Exerc. 2004;36(3):379-387.

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 589
14. Warren P, Gabbe BJ, Schneider-Kolsky M, Bennell KL. Clinical predictors of time to return to competition and of recurrence following hamstring strain in elite australian footballers. Br J Sports Med. 2010;44(6):415-419. d
15. Fousekis K, Tsepis E, Poulmedis P, Athanasopoulos S, Vagenas G. Intrinsic risk factors of non-contact quadriceps and hamstring strains in soccer: A prospective study of 100 professional players. Br J Sports Med. 2011;45(9):709-714.
16. Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: Factors that lead to injury and re-injury. Sports Med. 2012;42(3):209-226.
17. Salmon L, Russell V, Musgrove T, Pinczewski L, Refshauge K. Incidence and risk factors for graft rupture and contralateral rupture after anterior cruciate ligament reconstruction. Arthroscopy. 2005;21(8):948-957.
18. Gerber JP, Marcus RL, Dibble LE, Greis PE, Burks RT, LaStayo PC. Effects of early progressive eccentric exercise on muscle size and function after anterior cruciate ligament reconstruction: A 1-year follow-up study of a randomized clinical trial. Phys Ther. 2009;89(1):51-59.
19. Ernst GP, Saliba E, Diduch DR, Hurwitz SR, Ball DW. Lower-extremity compensations following anterior cruciate ligament reconstruction. Phys Ther. 2000;80(3):251-260.
20. Rettig AC, Liotta FJ, Klootwyk TE, Porter DA, Mieling P. Potential risk of rerupture in primary achilles tendon repair in athletes younger than 30 years of age. Am J Sports Med. 2005;33(1):119-123.
21. Aroen A, Helgo D, Granlund OG, Bahr R. Contralateral tendon rupture risk is increased in individuals with a previous achilles tendon rupture. Scand J Med Sci Sports. 2004;14(1):30-33.
22. Malliaropoulos N, Ntessalen M, Papacostas E, Longo UG, Maffulli N. Reinjury after acute lateral ankle sprains in elite track and fi eld athletes. Am J Sports Med. 2009;37(9):1755-1761.
23. Baroni BM, Generosi RA, Junior E. Incidence and factors related to ankle sprains in athletes of futsal national teams [portuguese]. FISIOTER MOVIMENTO. 2008;21(4):79-88.
24. Pefanis N, Karagounis P, Tsiganos G, Armenis E, Baltopoulos P. Tibiofemoral angle and its relation to ankle sprain occurrence. Foot Ankle Spec. 2009;2(6):271-276.
25. Willems TM, Witvrouw E, Delbaere K, Mahieu N, Bourdeaudhuij I, De Clercq D. Intrinsic risk factors for inversion ankle sprains in male subjects: A prospective study. Am J Sports Med. 2005;33(3):415-423.
26. Denegar CR, Hertel J, Fonseca J. The effect of lateral ankle sprain on dorsifl exion range of motion,
posterior talar glide, and joint laxity. J Orthop Sports Phys Ther. 2002;32(4):166-173.
27. O’Sullivan K, O’Ceallaigh B, O’Connell K, Shafat A. The relationship between previous hamstring injury and the concentric isokinetic knee muscle strength of irish gaelic footballers. BMC Musculoskelet Disord. 2008;9:30.
28. Ageberg E, Fridén T. Normalized motor function but impaired sensory function after unilateral non-reconstructed ACL injury: Patients compared with uninjured controls. Knee Surg Sports Traumatol Arthrosc. 2008;16(5):449-456.
29. Andrade MS, Cohen M, Picarro IC, Silva AC. Knee performance after anterior cruciate ligament reconstruction. Isokinetics Exerc Sci. 2002;10(2):81-86..
30. Button K, van Deursen R, Price P. Recovery in functional non-copers following anterior cruciate ligament rupture as detected by gait kinematics. PHYS THER SPORT. 2008;9(2):97-104.
31. St Clair Gibson A, Lambert MI, Durandt JJ, Scales N, Noakes TD. Quadriceps and hamstrings peak torque ratio changes in persons with chronic anterior cruciate ligament defi ciency. J Orthop Sports Phys Ther. 2000;30(7):418-427. d
32. Bressel E, McNair PJ. Biomechanical behavior of the plantar fl exor muscle-tendon unit after an achilles tendon rupture. Am J Sports Med. 2001;29(3):321-326.
33. Mahieu NN, Witvrouw E, Stevens V, Van Tiggelen D, Roget P. Intrinsic risk factors for the development of achilles tendon overuse injury: A prospective study. Am J Sports Med. 2006;34(2):226-235.
34. Edouard P, Chatard J, Fourchet F, et al. Invertor and evertor strength in track and fi eld athletes with functional ankle instability. Isokinetics Exerc Sci. 2011;19(2):91-96.
35. Hertel J, Buckley WE, Denegar CR. Serial testing of postural control after acute lateral ankle sprain. J Athletic Train. 2001;36(4):363-368.
36. Bonfi m TR, Paccola C, Barela JA. Proprioceptive and behavior impairments in individuals with anterior cruciate ligament reconstructed knees. Arch Phys Med Rehabil. 2003;84(8):1217-1223.
37. Benjuya N, Plotqin D, Melzer I. Isokinetic profi le of patient with anterior cruciate ligament tear. Isokinetics Exerc Sci. 2000;8(4):229-232.
38. Roberts D, Andersson G, Friden T. Knee joint proprioception in ACL-defi cient knees is related to cartilage injury, laxity and age: A retrospective study of 54 patients. Acta Orthop Scand. 2004;75(1):78-83.
39. Courtney C, Rine RM, Kroll P. Central somatosensory changes and altered muscle synergies in subjects with anterior cruciate ligament defi ciency. Gait Posture. 2005;22(1):69-74.

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 590
40. Fonseca ST, Ócarino J, Silva P, Guimarães R, Oliveira M, Lage CA. Proprioception in individuals with ACL-defi cient knee and good muscular and functional performance. Res Sports Med. 2005;13(1):47-61.
41. Heroux ME, Tremblay F. Corticomotor excitability associated with unilateral knee dysfunction secondary to anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc. 2006;14(9):823-833.
42. Williams GN, Barrance PJ, Snyder-Mackler L, Buchanan TS. Altered quadriceps control in people with anterior cruciate ligament defi ciency. Med Sci Sports Exerc. 2004;36(7):1089-1097.
43. Brown C, Padua D, Marshall SW, Guskiewicz K. Individuals with mechanical ankle instability exhibit different motion patterns than those with functional ankle instability and ankle sprain copers. Clin Biomech. 2008;23(6):822-831.
44. Palmieri-Smith R, McLean SG, Ashton-Miller J, Wojtys EM. Association of quadriceps and hamstrings cocontraction patterns with knee joint loading. J ATHLETIC TRAIN. 2009;44(3):256-263.
45. Palmieri-Smith R, Hopkins JT, Brown TN. Peroneal activation defi cits in persons with functional ankle instability. Am J Sports Med. 2009;37(5):982-988.
46. Santilli V, Frascarelli MA, Paoloni M, et al. Peroneus longus muscle activation pattern during gait cycle in athletes affected by functional ankle instability: A surface electromyographic study. Am J Sports Med. 2005;33(8):1183-1187.
47. Mitchell A, Dyson R, Hale T, Abraham C. Biomechanics of ankle instability. part 1: Reaction time to simulated ankle sprain. Med Sci Sports Exerc. 2008;40(8):1515-
48. Mitchell A, Dyson R, Hale T, Abraham C. Biomechanics of ankle instability. part 2: Postural sway-reaction time relationship. Med Sci Sports Exerc. 2008;40(8):1522-1528.
49. Ross SE, Guskiewicz KM. Examination of static and dynamic postural stability in individuals with functionally stable and unstable ankles. Clin J Sport Med. 2004;14(6):332-338.
50. McKeon PO, Hertel J. Spatiotemporal postural control defi cits are present in those with chronic ankle instability. BMC Musculoskelet Disord. 2008;9:76.
51. Refshauge KM, Kilbreath SL, Raymond J. Defi cits in detection of inversion and eversion movements among subjects with recurrent ankle sprains... including commentary by vandervoort AA with authors’ response. J Orthop Sports Phys Ther. 2003;33(4):166-176.
52. Sefton JM, Hicks-Little C, Hubbard TJ, et al. Sensorimotor function as a predictor of chronic ankle instability. Clin Biomech. 2009;24(5):451-458.
53. DeVita P, Hortobagyi T. Functional knee brace alters predicted knee muscle and joint forces in people with ACL reconstruction during walking. J APPL BIOMECH. 2001;17(4):297-311.
54. Tecco S, Salini V, Calvisi V, et al. Effects of anterior cruciate ligament (ACL) injury on postural control and muscle activity of head, neck and trunk muscles. J Oral Rehabil. 2006;33(8):576-587.
55. Binder-Macleod B, Buchanan TS. Tibialis anterior volumes and areas in ACL-injured limbs compared with unimpaired. Med Sci Sports Exerc. 2006;38(9):1553-1557.
56. Rudolph KS, Axe MJ, Snyder-Mackler L. Dynamic stability after ACL injury: Who can hop? Knee Surg Sports Traumatol Arthrosc. 2000;8(5):262-269.
57. Paterno MV, Ford KR, Myer GD, Heyl R, Hewett TE. Limb asymmetries in landing and jumping 2 years following anterior cruciate ligament reconstruction. Clin J Sport Med. 2007;17(4):258-262.
58. Nakasa T, Fukuhara K, Adachi N, Ochi M. The defi cit of joint position sense in the chronic unstable ankle as measured by inversion angle replication error. Arch Orthop Trauma Surg. 2008;128(5):445-449.
59. Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: Lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43(6):417-422.
60. Boling MC, Padua DA, Alexander Creighton R. Concentric and eccentric torque of the hip musculature in individuals with and without patellofemoral pain. J Athl Train. 2009;44(1):7-13.
61. Ferber R, Noehren B, Hamill J, Davis IS. Competitive female runners with a history of iliotibial band syndrome demonstrate atypical hip and knee kinematics. J Orthop Sports Phys Ther. 2010;40(2):52-58.
62. Kiesel KB, Butler RJ, Plisky PJ. Prediction of injury by limited and asymmetrical fundamental movement patterns in american football players. J Sport Rehabil. 2014;23(2):88-94. doi:
63. Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. 2006;36(12):911-919.
64. Plisky PJ, Gorman PP, Butler RJ, Kiesel KB, Underwood FB, Elkins B. The reliability of an instrumented device for measuring components of the star excursion balance test. N Am J Sports Phys Ther. 2009;4(2):92-99.

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 591
Titl
e A
utho
r Po
pula
tion
(age
, ge
nder
, act
ivity
) S
AD
AU
Qydut sfo
e pyT
sgnidni Fni a
M
Pred
icto
rs o
f ham
strin
g in
jury
at t
he e
lite
leve
l of
Aus
tralia
n fo
otba
ll (2
006)
Gab
be,B
.J., e
t al.
22
2 el
ite m
ale
Aus
tralia
n fo
otba
ll pl
ayer
s, be
twee
n 17
-37
yea
rs o
ld fr
om 6
M
elbo
urne
AFL
clu
bs d
urin
g pr
e-se
ason
of 2
002
"A p
ositi
ve h
amst
ring
inju
ry h
isto
ry (s
usta
ined
dur
ing
the
prev
ious
12
mon
ths)
was
iden
tifie
d as
the
stro
nges
t pre
dict
or o
f su
bseq
uent
ham
strin
g in
jury
and
supp
orts
the
findi
ngs o
f sev
eral
st
udie
s.”
8troho
C
Intri
nsic
risk
fact
ors o
f no
n-co
ntac
t qua
dric
eps
and
ham
strin
g st
rain
s in
socc
er: a
pro
spec
tive
stud
y of
100
pr
ofes
sion
al p
laye
rs
(201
0)
Fous
ekis
,K.,
et a
l. 10
0 pr
ofes
sion
al so
ccer
pl
ayer
s, be
twee
n 19
-28
year
s ol
d, fr
ee o
f inj
ury
for a
t lea
st
6 m
onth
s prio
r to
test
ing
“For
the
deve
lopm
ent o
f ham
strin
g st
rain
s in
socc
er p
laye
rs, t
wo
func
tiona
l asy
mm
etrie
s of t
he lo
wer
lim
bs (i
soki
netic
stre
ngth
an
d le
g le
ngth
) are
acc
ount
able
, with
pre
viou
s his
tory
of s
train
s in
the
sam
e m
uscl
e gr
oup
bein
g ra
ther
redu
ctiv
e of
the
odds
of
this
inju
ry.”
31tr oho
C
Pred
ictin
g ha
mst
ring
stra
in in
jury
in e
lite
athl
etes
(200
4)
Bro
cket
t,C.L
, et a
l. 27
ath
lete
s, 26
mal
es &
1
fem
ale,
23
AFL
pla
yers
& 4
tra
ck-a
nd-f
ield
ath
lete
s, be
twee
n 19
-33
year
s old
.
“If t
he o
ptim
um le
ngth
for a
ctiv
e te
nsio
n is
rath
er sh
ort,
in te
rms
of th
e m
uscl
e’s w
orki
ng ra
nge,
it fo
llow
s tha
t mor
e of
the
desc
endi
ng li
mb
will
be
incl
uded
with
in th
e w
orki
ng ra
nge.
Tha
t, in
turn
, inc
reas
es th
e ris
k of
dam
age.
"
Con
trolle
d La
bora
tory
Stu
dy
11
Clin
ical
risk
fact
ors f
or
ham
strin
g m
uscl
e st
rain
(200
1)
Ver
rall,
et a
l.
114
mal
es fr
om tw
o pr
ofes
sion
al A
ustra
lian
Foot
ball
Leag
ues,
mea
n ag
e 21
.6 y
ears
.
“The
re w
as a
sign
ifica
ntly
incr
ease
d ris
k of
inju
ry w
ith o
lder
ag
e, b
eing
of a
borig
inal
des
cent
, a p
ast h
isto
ry o
f pos
terio
r thi
gh
inju
ry, a
pas
t his
tory
of k
nee
inju
ry, a
nd a
pas
t his
tory
of o
stei
tis
pubi
s.”
Pros
pect
ive
Coh
ort
12
Clin
ical
pre
dict
ors o
f tim
e to
retu
rn to
co
mpe
titio
n an
d of
re
curr
ence
follo
win
g ha
mst
ring
stra
in in
el
ite A
ustra
lian
foot
balle
rs (2
008)
War
ren,
et a
l.
59 e
lite
mal
e A
ustra
lian
foot
ball
play
ers,
mea
n ag
e 24
ye
ars,
who
mis
sed
at le
ast o
ne
gam
e du
e to
inju
ry.
“Nin
e pl
ayer
s (15
%) e
xper
ienc
ed a
recu
rren
ce o
f the
ir ha
mst
ring
inju
ry w
ithin
the
first
3 w
eeks
of r
etur
ning
to p
lay”
Pr
ospe
ctiv
e O
bser
vatio
nal
13
The
rela
tions
hip
betw
een
prev
ious
ha
mst
ring
inju
ry a
nd
the
conc
entri
c is
okin
etic
kne
e m
uscl
e st
reng
th o
f iris
h ga
elic
fo
otba
llers
(200
8)
O'S
ulliv
an, e
t al.
44
mal
e ga
elic
foot
ball
play
ers,
mea
n ag
e 21
.2 y
ears
. "E
vide
nce
of h
amst
ring
mus
cle
wea
knes
s and
mus
cle
stre
ngth
im
bala
nce
in g
aelic
foot
balle
rs a
fter p
revi
ous h
amst
ring
inju
ry"
Pros
pect
ive
Obs
erva
tiona
l 10
Effe
cts o
f Prio
r H
amst
ring
Stra
in
Inju
ry o
n St
reng
th,
Flex
ibili
ty, a
nd
Run
ning
Mec
hani
cs
(201
0)
Sild
er, e
t al.
18 in
divi
dual
s inv
olve
d in
ru
nnin
g-re
late
d sp
orts
with
a
prev
ious
ham
strin
g in
jury
, be
twee
n 18
-45
year
s old
.
"Our
resu
lts su
gges
t tha
t, w
hile
scar
tiss
ue m
ay b
e pr
esen
t in
subj
ects
with
a p
rior h
amst
ring
inju
ry, t
hese
und
erly
ing
mor
phol
ogic
al c
hang
es d
o no
t app
ear t
o be
dis
cern
able
in te
rms
of fu
nctio
nal s
treng
th m
easu
res,
or m
uscu
lote
ndon
stre
tch
and
neur
omus
cula
r pat
tern
s dur
ing
sprin
ting.
"
Pros
pect
ive
Coh
ort
11
Appen
dix
1.
Ham
stri
ng S
trai
n R
e-in
jury
Pap
ers

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 592
Titl
e A
utho
r Po
pula
tion
(age
, ge
nder
, act
ivity
) M
ain
Find
ings
T
ype
of
stud
y Q
UA
DA
S
Hig
h ris
k of
new
kne
e in
jury
in
elite
foot
balle
rs w
ith p
revi
ous
ante
rior c
ruci
ate
ligam
ent i
njur
y (2
006)
Wal
de ́n
, M.,
et
al.
310
Mal
e Sw
edis
h Le
ague
pla
yers
, m
ean
age
25 y
ears
. 24
AC
L in
jure
d, 2
86 A
CL
heal
thy.
“Tot
al, 7
15 in
jurie
s wer
e re
cord
ed, a
nd 6
25 (8
7%)
wer
e lo
cate
d to
the
low
er li
mbs
. Of t
he in
jurie
s to
the
low
er e
xtre
miti
es in
the
AC
L in
jure
d gr
oup,
70%
(3
8/54
) aff
ecte
d a
limb
with
a p
revi
ous A
CL
inju
ry.”
Pros
pect
ive
Coh
ort
12
Fact
ors a
ffec
ting
retu
rn to
spor
ts
afte
r ant
erio
r cru
ciat
e lig
amen
t re
cons
truct
ion
with
pat
ella
r ten
don
and
ham
strin
g gr
aft:
a pr
ospe
ctiv
e cl
inic
al in
vest
igat
ion
(200
6)
Gob
bi,A
., et
al.
10
0 at
hlet
es, 6
7 m
ales
& 3
3 fe
mal
es,
mea
n ag
e 28
yea
rs. A
thle
tes p
layi
ng in
sp
orts
at r
egio
nal/n
atio
nal l
evel
s/re
c sp
orts
at l
east
3x/
wee
k, w
ith n
orm
al
cont
rala
tera
l kne
e, th
ose
w/ p
art.
men
isce
ctom
ies
“Tw
o pa
tient
s pre
sent
ed w
ith p
ersi
sten
t clic
king
and
ca
tchi
ng d
urin
g th
e fir
st y
ear p
ost-A
CL…
In a
noth
er
case
(HT
graf
t), re
-inju
ry to
the
oper
ated
kne
e w
as
docu
men
ted”
Long
itudi
nal
10
Nor
mal
ized
mot
or fu
nctio
n bu
t im
paire
d se
nsor
y fu
nctio
n af
ter
unila
tera
l non
-rec
onst
ruct
ed A
CL
inju
ry: p
atie
nts c
ompa
red
with
un
inju
red
cont
rols
(200
8)
Age
berg
, et a
l. 56
indi
vidu
als,
36 m
ales
& 2
0 fe
mal
es, b
etw
een
15-4
5 ye
ars o
ld w
ho
wer
e A
CL
defic
ient
with
an
unin
jure
d co
ntra
late
ral e
xtre
mity
.
“The
impa
ct o
f the
se fi
ndin
gs o
n th
e ris
k of
su
stai
ning
re-in
jurie
s req
uire
s fur
ther
stud
ies,
and
ther
e m
ay b
e a
brea
kpoi
nt a
t whi
ch th
e di
scre
panc
y be
twee
n m
otor
and
sens
ory
func
tion
beco
mes
a ri
sk
fact
or d
urin
g m
ore
stre
nuou
s act
ivity
.”
Cro
ss-s
ectio
nal
12
Effe
cts o
f ear
ly p
rogr
essi
ve
ecce
ntric
exe
rcis
e on
mus
cle
size
an
d fu
nctio
n af
ter a
nter
ior c
ruci
ate
ligam
ent r
econ
stru
ctio
n: a
1-y
ear
follo
w-u
p st
udy
of a
rand
omiz
ed
clin
ical
tria
l (20
09)
Ger
ber,J
.P.,
et
al.
40 p
atie
nts w
ith A
CL-
R, b
etw
een
18-
50 y
ears
old
, who
wer
e m
oder
atel
y ac
tive
prio
r to
inju
ry. R
ando
mly
as
sign
ed: G
roup
1 re
ceiv
ing
early
pr
ogre
ssiv
e ec
cent
ric e
xerc
ise
and
Gro
up 2
rece
ivin
g st
anda
rd re
hab.
“Of t
hose
not
retu
rnin
g fo
r 1-y
ear f
ollo
w-u
p,
4 pa
rtici
pant
s tra
umat
ical
ly re
inju
red
thei
r inv
olve
d kn
ee b
etw
een
4 an
d 12
mon
ths f
ollo
win
g in
itial
AC
L-R
, cau
sing
gra
ft di
srup
tion.
”
Ran
dom
ized
C
ontro
l Tria
l 11
Clo
sed
kine
tic c
hain
alo
ne
com
pare
d to
com
bine
d op
en a
nd
clos
ed k
inet
ic c
hain
exe
rcis
es fo
r qu
adric
eps s
treng
then
ing
afte
r an
terio
r cru
ciat
e lig
amen
t re
cons
truct
ion
with
resp
ect t
o re
turn
to
spor
ts: a
pro
spec
tive
mat
ched
fo
llow
-up
stud
y (2
000)
Mik
kels
en,C
., et
al.
44 in
divi
dual
s, be
twee
n 18
–40
year
s ol
d w
ith a
firs
t-eve
r uni
late
ral A
CL
inju
ry a
nd a
hea
lthy
cont
rala
tera
l leg
. R
ando
mly
ass
igne
d: G
roup
1 tr
aine
d w
ith C
KC
and
Gro
up 2
trai
ned
with
C
KC
for f
irst 6
wee
ks, t
hen
OK
C fo
r qu
adric
eps m
uscl
e.
Of t
he 2
2 pa
tient
s in
grou
p 2,
“12
retu
rned
to sp
ort a
t th
e sa
me
leve
l as b
efor
e th
e in
jury
, eig
ht p
atie
nts h
ad
redu
ced
thei
r act
ivity
leve
l and
/or c
hang
ed to
a le
ss
knee
dem
andi
ng sp
ort d
ue to
impa
ired
knee
func
tion
in th
ree
patie
nts,
soci
al a
nd fa
mily
reas
ons i
n th
ree,
an
d th
e fe
ar o
f rei
njur
ing
the
knee
in tw
o. O
ne p
atie
nt
did
not r
etur
n to
any
type
of s
port
due
to a
new
kne
e in
jury
of t
he c
ontra
late
ral l
eg. O
ne p
atie
nt w
as n
ot
phys
ical
ly a
ctiv
e ei
ther
bef
ore
or a
fter A
CL
reco
nstru
ctio
n.”
Ran
dom
ized
C
ontro
l Tria
l 11
Appen
dix
2.
AC
L R
e-In
jury
Pap
ers

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 593
Titl
e A
utho
r Po
pula
tion
(a
ge,
gend
er, a
ctiv
ity)
Mai
nfin
ding
sT
ype
of st
udy
QU
AD
AS
Bio
mec
hani
cal
Beh
avio
r of t
he
Plan
tar
Flex
or M
uscl
e-Te
ndon
U
nit a
fter a
n A
chill
es T
endo
n R
uptu
re (2
001)
Bre
ssel
, et a
l. 40
indi
vidu
als,
26 m
ales
& 1
4 fe
mal
es, m
ean
age
51.4
yea
rs,
volu
ntee
red
for t
he st
udy.
All
subj
ects
wer
e in
volv
ed in
at l
east
lig
ht/ r
ecre
atio
nal a
ctiv
ity a
nd h
ad
rupt
ured
thei
r Ach
illes
tend
on m
ore
than
1 y
ear b
efor
e th
e st
udy.
Stiff
ness
and
vis
coel
astic
pro
perti
es, s
uch
as to
rque
re
laxa
tion,
wer
e si
mila
r bet
wee
n th
e in
volv
ed a
nd
unin
volv
ed li
mbs
. How
ever
, oth
er m
easu
rem
ents
, suc
h as
pe
ak p
assi
ve to
rque
, cal
f circ
umfe
renc
e, a
nd m
axim
al
isom
etric
pla
ntar
flex
or to
rque
, wer
e gr
eate
r in
the
unin
volv
ed li
mb.
Incr
ease
d va
lues
for s
tiffn
ess m
ay
pred
ispo
se th
e m
uscl
e-te
ndon
uni
t to
furth
er d
amag
e.
Expe
rimen
tal
12
Con
trala
tera
l ten
don
rupt
ure
risk
is
incr
ease
d in
in
divi
dual
s with
a
prev
ious
Ach
illes
te
ndon
rupt
ure
(200
4)
Aro
en, e
t al.
168
patie
nts,
142
mal
es &
26
fem
ales
, med
ian
age
38.5
yea
rs a
t tim
e of
inju
ry, w
ho h
ad A
chill
es
rupt
ure
betw
een
1990
and
199
7 at
a
Nor
way
hos
pita
l.
Gre
atly
incr
ease
d ris
k of
rupt
ure
of c
ontra
late
ral A
chill
es
tend
on in
thos
e w
ho h
ad a
pre
viou
s rup
ture
on
one
side
. Th
e au
thor
s pro
pose
d th
at th
is c
ould
be
due
to a
gen
etic
pr
edis
posi
tion
for t
endo
n ru
ptur
es, t
hat t
he in
jury
is c
ause
d by
deg
ener
ativ
e ch
ange
s, or
that
dis
use
atro
phy
of th
e co
ntra
late
ral t
endo
n du
e to
imm
obili
zatio
n of
the
inju
red
leg
cont
ribut
ed to
the
inju
ry.
Ret
rosp
ectiv
e Se
lf-R
epor
t Q
uest
ionn
aire
11
Intri
nsic
Ris
k Fa
ctor
s fo
r the
Dev
elop
men
t of
Ach
illes
Ten
don
Ove
ruse
Inju
ry (2
006)
Mah
ieu,
et a
l. 69
mal
e of
ficer
cad
ets a
t the
Bel
gian
R
oyal
Mili
tary
aca
dem
y, m
ean
age
18 y
ears
.
10/6
9 ha
d A
chill
es o
veru
se in
jurie
s dur
ing
the
6 w
eeks
of
basi
c tra
inin
g. T
hose
with
low
e r p
lant
ar fl
exor
stre
ngth
and
in
crea
sed
dors
iflex
ion
RO
M w
ere
at g
reat
er ri
sk o
f thi
s in
jury
. Aut
hors
hyp
othe
size
d th
at st
rong
er m
uscl
e st
reng
th
prod
uces
stro
nger
tend
ons t
hat c
ould
bet
ter d
eal w
ith
exce
ssiv
e fo
rce.
Coh
ort (
Pros
pect
ive)
11
Appen
dix
3.
Ach
illes
Ten
don
Re-
inju
ry P
aper
s
The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 594
Titl
e A
utho
r Po
pula
tion
(age
, ge
nder
, act
ivity
) S
AD
AU
Qydutsfo
epyT
sgnidn iFnia
M
Inve
rtor a
nd e
verto
r stre
ngth
in
trac
k an
d fie
ld a
thle
tes w
ith
func
tiona
l ank
le in
stab
ility
(2
011)
Edou
ard,
et a
l. Tr
ack
and
field
fem
ale
athl
etes
be
twee
n 15
-40
year
s old
with
a
hist
ory
of la
tera
l ank
les s
prai
ns
The
ever
tor m
uscl
e st
reng
th w
as h
ighe
r tha
n th
e in
verto
r m
uscl
e st
reng
th in
the
dom
inan
t sid
e fo
r all
grou
ps, e
xcep
t fo
r the
gro
up w
ith a
pre
viou
s his
tory
of a
nkle
spra
in. A
n el
evat
ed a
nkle
Eve
rtor/I
nver
tor R
atio
(> 1
.0) h
as b
een
iden
tifie
d as
an
impo
rtant
indi
cato
r of a
nkle
spra
in
susc
eptib
ility
; oth
erw
ise,
it c
ould
be
an in
verto
r stre
ngth
w
eakn
ess i
n su
bjec
ts w
ith F
AI.
Cro
ss-S
ectio
nal
12
The
Effe
ct o
f Lat
eral
Ank
le
Spra
in o
n D
orsi
flexi
on R
ange
of
Mot
ion,
Pos
terio
r Ta
lar G
lide,
and
Join
t Lax
ity
(200
2)
Den
egar
, et a
l.
12 a
thle
tes,
5 m
ales
& 7
fe
mal
es, b
etw
een
18-2
2 ye
ars
old
with
a h
isto
ry o
f lat
eral
an
kle
spra
in w
ithin
the
last
6
mon
ths w
ho h
ad re
turn
ed to
sp
ort p
artic
ipat
ion
Res
idua
l lig
amen
tous
laxi
ty w
as c
omm
only
foun
d fo
llow
ing
late
ral a
nkle
spra
in. D
orsi
flexi
on ra
nge
of m
otio
n w
as re
stor
ed in
the
popu
latio
n st
udie
d de
spite
evi
denc
e of
re
stric
ted
post
erio
r glid
e of
the
talo
crur
al jo
int.
Alth
ough
re
stor
atio
n of
phy
siol
ogic
al ra
nge
of m
otio
n w
as a
chie
ved,
re
sidu
al jo
int d
ysfu
nctio
n pe
rsis
ted.
Ret
rosp
ectiv
e St
udy
12
Exam
inin
g N
euro
mus
cula
r C
ontro
l Dur
ing
Land
ings
on
a Su
pina
ting
Plat
form
in
Pers
ons W
ith a
nd W
ithou
t A
nkle
Inst
abili
ty (2
011)
Gut
ierr
ez, e
t al.
45 a
ctiv
e, h
ealth
y pa
rtici
pant
s be
twee
n 18
-30
year
s old
wer
e di
vide
d in
to 3
gro
ups:
ank
le
inst
abili
ty, l
ater
al a
nkle
spra
in,
and
cont
rol
Whe
n la
ndin
g on
a d
evic
e bu
ilt to
sim
ulat
e th
e m
echa
nism
of
a la
tera
l ank
le sp
rain
(sup
inat
ion)
, the
ank
le in
stab
ility
gr
oup
disp
laye
d si
gnifi
cant
ly in
crea
sed
prep
arat
ory
and
reac
tive
pero
neal
act
ivat
ion,
whi
le th
e La
tera
l Ank
le S
prai
n gr
oup
dem
onst
rate
d in
crea
sed
prep
arat
ory
tibia
lis a
nter
ior
mus
cle
activ
atio
n.
Con
trolle
d La
bora
tory
Stu
dy
12
Mec
hani
cal I
nsta
bilit
y A
fter
an A
cute
Lat
eral
Ank
le S
prai
n (2
009)
Hub
bard
, et a
l. 16
subj
ects
with
a fi
rst-t
ime
acut
e un
ilate
ral a
nkle
spra
in, 7
m
ales
& 9
fem
ales
, mea
n ag
e 19
.5 y
ears
. 16
heal
thy
cont
rols
, 7
mal
es &
9 fe
mal
es, m
ean
age
20.4
yea
rs.
The
lack
of s
igni
fican
t diff
eren
ces i
n m
echa
nica
l lax
ity
over
an
8-w
eek
perio
d su
gges
ts th
at n
atur
al re
cove
ry o
f la
xity
take
s lon
ger t
han
8 w
eeks
.
Coh
ort
11
Seria
l tes
ting
of p
ostu
ral
cont
rol a
fter a
cute
late
ral
ankl
e sp
rain
(200
1)
Her
tel,
et a
l. 17
you
ng a
dults
, 9 m
ales
& 8
fe
mal
es, m
ean
age
21.8
yea
rs
who
sust
aine
d un
ilate
ral a
cute
m
ild to
mod
erat
e la
tera
l ank
le
spra
ins
Indi
vidu
als w
ith p
ostu
ral c
ontro
l im
pairm
ents
are
like
ly to
ha
ve la
rger
CO
P ex
curs
ions
and
thus
, lar
ger s
um o
f ex
curs
ions
thro
ugho
ut a
tria
l. El
evat
ed m
easu
res o
f po
stur
al c
ontro
l dur
ing
stat
ic S
LS h
ave
not b
een
show
n to
pr
edic
t rec
urre
nt a
nkle
spra
in w
ith p
rolo
nged
func
tiona
l an
kle
inst
abili
ty. H
owev
er, t
he la
ck o
f bal
ance
trai
ning
af
ter a
cute
LA
S ap
pear
s to
pred
ispo
se a
nkle
-inju
red
subj
ects
to re
curr
ent s
prai
n
Long
itudi
nal
11
Intri
nsic
Ris
k Fa
ctor
s of
Non
cont
act A
nkle
Spr
ains
in
Socc
er (2
012)
Fous
ekis
, et a
l.
100
prof
essi
onal
socc
er
play
ers,
mea
n ag
e 23
.6 y
ears
w
ho h
ad su
stai
ned
no in
jury
for
the
past
6 m
onth
s wer
e as
sess
ed fo
r ank
le jo
int
asym
met
ries
The
logi
stic
regr
essi
on a
naly
sis r
evea
led
3 si
gnifi
cant
pr
edic
tors
of n
onco
ntac
t ank
le sp
rain
s: (A
) ecc
entri
c is
okin
etic
stre
ngth
asy
mm
etrie
s of a
nkle
dor
sal a
nd p
lant
ar
flexo
rs; (
B) i
ncre
ased
BM
I; an
d (C
) inc
reas
ed b
ody
wei
ght.
This
stud
y fo
und
that
ther
e is
not
an
incr
ease
d ris
k fo
r la
tera
l ank
le li
gam
ent i
njur
y af
ter s
uffe
ring
a pr
ior a
nkle
in
jury
.
Coh
ort
12
Appen
dix
4.
Ank
le R
e-in
jury
Pap
ers

The International Journal of Sports Physical Therapy | Volume 9, Number 5 | October 2014 | Page 595
Titl
e A
utho
r Po
pula
tion
(age
, ge
nder
, act
ivity
) S
AD
AU
Qydutsfo
epyT
sgnidn iFnia
M
Ipsi
late
ral H
ip A
bduc
tor
Wea
knes
s Afte
r Inv
ersi
on
Ank
le S
prai
n (2
006)
Frie
l, et
al.
C
onve
nien
ce sa
mpl
e of
23
indi
vidu
als,
betw
een
18-5
2 ye
ars o
ld w
ith a
his
tory
of a
t le
ast 2
ank
le sp
rain
s to
the
sam
e si
de
Sign
ifica
nt w
eakn
ess i
n th
e hi
p ab
duct
or m
uscl
es o
n th
e in
volv
ed si
de a
s com
pare
d w
ith th
e un
invo
lved
lim
b of
su
bjec
ts w
as fo
und
with
chr
onic
ank
le sp
rain
, whi
ch c
an
cont
ribut
e to
incr
ease
d ris
k fo
r re-
inju
ry.
Ex-P
ost F
acto
D
esig
n N
/A
Rei
njur
y A
fter A
cute
Lat
eral
A
nkle
Spr
ains
in E
lite
Trac
k an
d Fi
eld
Ath
lete
s (20
09)
Mal
liaro
poul
os,
et a
l. 20
2 el
ite m
ale
and
fem
ale
Gre
ek tr
ack
athl
etes
with
acu
te
late
ral a
nkle
spra
ins
Low
-gra
de a
nkle
spra
ins r
esul
t in
a hi
gher
risk
of r
e-in
jury
th
an h
igh-
grad
e an
kle
spra
ins a
t a 2
4-m
onth
follo
w-u
p.
Gra
de II
inju
ries s
how
ed a
sign
ifica
ntly
hig
her r
ate
of re
-in
jury
than
gra
des I
and
III A
. The
re w
as n
o si
gnifi
cant
di
ffer
ence
in ti
me
betw
een
orig
inal
inju
ry a
nd re
-inju
ry
base
d on
gra
de o
f inj
ury.
Coh
ort (
Prog
nosi
s)
12
Tibi
ofem
oral
ang
le a
nd it
s re
latio
n to
ank
le sp
rain
oc
curr
ence
(200
9)
Pefa
nis,
et a
l. 45
hig
h-le
vel b
aske
tbal
l, so
ccer
, and
vol
leyb
all m
ale
athl
etes
, mea
n ag
e 23
yea
rs.
The
fact
ors c
ontri
butin
g m
ore
to a
n an
kle
spra
in w
ere
prev
ious
sim
ilar i
njur
y, fo
llow
ed b
y B
MI,
and
age.
TFA
w
as p
rove
n to
be
stat
istic
ally
non
-sig
nific
ant a
nd d
oes n
ot
seem
to b
e a
fact
or th
at c
ould
incr
ease
the
prob
abili
ty o
f sp
rain
ing
an a
nkle
.
Pros
pect
ive
11
The
effe
ct o
f Q-a
ngle
on
ankl
e sp
rain
occ
urre
nce
(200
9)
Pefa
nis,
et a
l. 45
hig
h-le
vel b
aske
tbal
l, so
ccer
, and
vol
leyb
all m
ale
athl
etes
, mea
n ag
e 23
yea
rs.
The
fact
ors c
ontri
butin
g m
ore
to a
n an
kle
spra
in w
ere
prev
ious
sim
ilar i
njur
y, fo
llow
ed b
y B
MI a
nd a
ge. Q
-ang
le
was
show
n to
be
stat
istic
ally
non
-sig
nific
ant a
nd d
oes n
ot
seem
to b
e a
fact
or th
at c
ould
incr
ease
the
chan
ces o
f sp
rain
ing
an a
nkle
.
Pros
pect
ive
11
Intri
nsic
risk
fact
ors f
or
inve
rsio
n an
kle
spra
ins i
n m
ale
subj
ects
(200
5)
Will
ems,
et a
l. 24
1 m
ale
Phys
. Ed.
stud
ents
, m
ean
age
18.3
yea
rs w
ho w
ere
fres
hman
at t
he G
hent
U
nive
rsity
.
44 o
f the
241
sust
aine
d an
inve
rsio
n sp
rain
with
in th
e 1-
3 ye
ar fo
llow
-up,
4 sp
rain
ed b
oth
ankl
es.
Thos
e w
ith sl
ower
ru
nnin
g sp
eed,
less
car
dior
espi
rato
ry e
ndur
ance
, les
s ba
lanc
e, d
ecre
ased
dor
sifle
xion
mus
cle
stre
ngth
, dec
reas
ed
dors
iflex
ion
RO
M, l
ess c
oord
inat
ion,
and
fast
er re
actio
n of
th
e tib
ialis
ant
erio
r and
gas
trocn
emiu
s mus
cles
are
at a
gr
eate
r ris
k of
ank
le sp
rain
s.
Pros
pect
ive
Coh
ort S
tudy
13
Appen
dix
4.
Ank
le R
e-in
jury
Pap
ers
(con
tinue
d)