Original Pediatric
14
ORIGINAL RESEARCH Indicators of pain in neonates at risk for neurological impairment Bonnie Stevens, Patrick McGrath, Annie Dupuis, Sharyn Gibbins, Joseph Beyene, Lynn Breau, Carol Camfield, Gordon Allen Finley, Linda S. Franck, Alexandra Howlett, Celeste Johnston, Patricia McKeever, Karel O’Brien, Arne Ohlsson & Janet Yamada Accepted for publication 22 August 2008 Correspondence to B. Stevens: e-mail: [email protected] Bonnie Stevens PhD RN Signy Hildur Eaton Chair in Paediatric Nursing Research Associate Chief Nursing Research The Hospital for Sick Children, Toronto, Ontario, Canada Patrick McGrath PhD OC FRSC Vice President, Research IWK Health Centre, Dalhousie University, Halifax, Nova Scotia, Canada Annie Dupuis PhD Biostatistician Child Health Evaluative Sciences, Research Institute, The Hospital for Sick Children, Toronto, Ontario, Canada Sharyn Gibbins PhD RN Director of Interdisciplinary Research Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada Joseph Beyene PhD Scientist Child Health Evaluative Sciences, Research Institute, The Hospital for Sick Children, Toronto, Ontario, Canada Lynn Breau PhD Registered Psychologist School of Nursing, Dalhousie University, Halifax, Nova Scotia, Canada Carol Camfield MD FRCPC Professor of Pediatrics Department of Pediatric Neurology, IWK Health Centre Halifax, Nova Scotia, Canada STEVENS B., MCGRATH P., DUPUIS A., GIBBINS S., BEYENE J., BREAU L., STEVENS B., MCGRATH P., DUPUIS A., GIBBINS S., BEYENE J., BREAU L., CAMFIELD C., ALLEN FINLEY G., FRANCK L.S., HOWLETT A., JOHNSTON C., CAMFIELD C., ALLEN FINLEY G., FRANCK L.S., HOWLETT A., JOHNSTON C., MCKEEVER P., O’BRIEN K., OHLSSON A. & YAMADA J. (2009) MCKEEVER P., O’BRIEN K., OHLSSON A. & YAMADA J. (2009) Indicators of pain in neonates at risk for neurological impairment. Journal of Advanced Nursing 65(2), 285–296 doi: 10.1111/j.1365-2648.2008.04854.x Abstract Title. Indicators of pain in neonates at risk for neurological impairment. Aim. This paper is a report of a study to compare the importance and usefulness ratings of physiological and behavioural indicators of pain in neonates at risk for neurological impairment by nurse clinicians and pain researchers. Background. Neonates at risk for neurological impairment have not been system- atically included in neonatal pain measure development and how clinicians and researchers view pain indicators in these infants is unknown. Methods. Data triangulation was undertaken in three Canadian Neonatal Intensive Care Units using data from: (a) 149 neonates at high, moderate and low risk for neurological impairment, (b) 95 nurse clinicians from the three units where infant data were collected and (c) 14 international pain researchers. Thirteen indicators were assessed following heel lance in neonates and 39 indicators generated from nurse clinicians and pain researchers were assessed for importance and accuracy. Data were collected between 2004 and 2005. Results. Across risk groups, indicators with the highest accuracy for discriminating ‘pain’ among neonates were: brow bulge (77–83%), eye squeeze (75–84%), naso- labial furrow (79–81%), and total facial expression (78–83%). Correlations between nurse ratings and neonatal accuracy scores ranged from moderate to none (mild risk r = 0 52, P = 0 07; moderate r = 0 43, P = 0 15; high r = 0 12, P = 0 69). Researchers demonstrated a better understanding of the importance of pain indicators (mild risk, r = 0 91, P < 0 001; moderate 0 85, P < 0 001; 0 0002; high r = 0 64, P = 0 019) than nurse clinicians. Conclusion/Discussion. Facial actions were rated as the most important indicators of neonatal pain. However, as neurological impairment risk increased, physiological indicators were rated more important by nurse clinicians and pain researchers, opposite to pain indicators demonstrated by neonates. Keywords: neonates, neurological impairment, nurses, pain indicators, researchers continued on page 286 Ó 2008 The Authors. Journal compilation Ó 2008 Blackwell Publishing Ltd 285 JAN JOURNAL OF ADVANCED NURSING
-
Upload
bayu-purnomo -
Category
Documents
-
view
213 -
download
1
description
anak
Transcript of Original Pediatric
-
ORIGINAL RESEARCH
Indicators of pain in neonates at risk for neurological impairment
Bonnie Stevens, Patrick McGrath, Annie Dupuis, Sharyn Gibbins, Joseph Beyene, Lynn Breau,
Carol Camfield, Gordon Allen Finley, Linda S. Franck, Alexandra Howlett, Celeste Johnston,
Patricia McKeever, Karel OBrien, Arne Ohlsson & Janet Yamada
Accepted for publication 22 August 2008
Correspondence to B. Stevens:
e-mail: [email protected]
Bonnie Stevens PhD RN
Signy Hildur Eaton Chair in Paediatric
Nursing Research
Associate Chief Nursing Research
The Hospital for Sick Children,
Toronto, Ontario, Canada
Patrick McGrath PhD OC FRSC
Vice President, Research
IWK Health Centre, Dalhousie University,
Halifax, Nova Scotia, Canada
Annie Dupuis PhD
Biostatistician
Child Health Evaluative Sciences,
Research Institute, The Hospital for
Sick Children, Toronto, Ontario, Canada
Sharyn Gibbins PhD RN
Director of Interdisciplinary Research
Sunnybrook Health Sciences Centre,
Toronto, Ontario, Canada
Joseph Beyene PhD
Scientist
Child Health Evaluative Sciences, Research
Institute, The Hospital for Sick Children,
Toronto, Ontario, Canada
Lynn Breau PhD
Registered Psychologist
School of Nursing, Dalhousie University,
Halifax, Nova Scotia, Canada
Carol Camfield MD FRCPC
Professor of Pediatrics
Department of Pediatric Neurology,
IWK Health Centre
Halifax, Nova Scotia, Canada
STEVENS B. , MCGRATH P. , DUPUIS A. , GIBBINS S. , BEYENE J. , BREAU L. ,STEVENS B. , MCGRATH P. , DUPUIS A. , GIBBINS S. , BEYENE J. , BREAU L. ,
CAMFIELD C. , ALLEN FINLEY G., FRANCK L.S . , HOWLETT A., JOHNSTON C.,CAMFIELD C., ALLEN FINLEY G., FRANCK L.S. , HOWLETT A., JOHNSTON C. ,
MCKEEVER P. , OBRIEN K. , OHLSSON A. & YAMADA J. (2009)MCKEEVER P. , OBRIEN K., OHLSSON A. & YAMADA J. (2009) Indicators of
pain in neonates at risk for neurological impairment. Journal of Advanced Nursing
65(2), 285296
doi: 10.1111/j.1365-2648.2008.04854.x
AbstractTitle. Indicators of pain in neonates at risk for neurological impairment.
Aim. This paper is a report of a study to compare the importance and usefulness
ratings of physiological and behavioural indicators of pain in neonates at risk for
neurological impairment by nurse clinicians and pain researchers.
Background. Neonates at risk for neurological impairment have not been system-
atically included in neonatal pain measure development and how clinicians and
researchers view pain indicators in these infants is unknown.
Methods. Data triangulation was undertaken in three Canadian Neonatal Intensive
Care Units using data from: (a) 149 neonates at high, moderate and low risk for
neurological impairment, (b) 95 nurse clinicians from the three units where infant
data were collected and (c) 14 international pain researchers. Thirteen indicators
were assessed following heel lance in neonates and 39 indicators generated from
nurse clinicians and pain researchers were assessed for importance and accuracy.
Data were collected between 2004 and 2005.
Results. Across risk groups, indicators with the highest accuracy for discriminating
pain among neonates were: brow bulge (7783%), eye squeeze (7584%), naso-
labial furrow (7981%), and total facial expression (7883%). Correlations
between nurse ratings and neonatal accuracy scores ranged from moderate to none
(mild risk r = 052, P = 007; moderate r = 043, P = 015; high r = 012,P = 069). Researchers demonstrated a better understanding of the importance of
pain indicators (mild risk, r = 091, P < 0001; moderate 085, P < 0001; 00002;
high r = 064, P = 0019) than nurse clinicians.
Conclusion/Discussion. Facial actions were rated as the most important indicators
of neonatal pain. However, as neurological impairment risk increased, physiological
indicators were rated more important by nurse clinicians and pain researchers,
opposite to pain indicators demonstrated by neonates.
Keywords: neonates, neurological impairment, nurses, pain indicators, researcherscontinued on page 286
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 285
JAN JOURNAL OF ADVANCED NURSING
-
Gordon Allen Finley MD FRCPC FAAP
Medical Director
Pediatric Pain Management, Centre for
Pediatric Pain Research, IWK Health Centre
Halifax, Nova Scotia, Canada
Linda S. Franck PhD RN RSCN
Professor of Childrens Nursing Research
Institute of Child Health, Centre for Nursing
and Allied Health Professions Research,
Great Ormond Street Hospital for Children,
London, UK
Alexandra Howlett MD FRCPC
Neonatologist
Department of Pediatrics,
IWK Health Centre,
Halifax, Nova Scotia, Canada
Celeste Johnston DEd RN
James McGill Professor
School of Nursing, McGill University,
Montreal, Quebec, Canada
Patricia McKeever PhD RN
Senior Scientist
Bloorview Kids Foundation Chair in
Childhood Disability Studies,
and Professor
Lawrence S. Bloomberg Faculty of Nursing,
University of Toronto,
Ontario, Canada
Karel OBrien MD FRCPC
Interim Pediatrican-in Chief
Department of Pediatrics, Mount Sinai
Hospital Toronto, Ontario, Canada
Arne Ohlsson MD FRCPC
Professor
Departments of Paediatrics, Obstetrics and
Gynaecology, and Health Policy,
Management and Evaluation, University of
Toronto,
and Director
Evidence Based Neonatal Care and
Outcomes Research,
Department of Pediatrics,
Mount Sinai Hospital,
Ontario, Canada
Janet Yamada MSc, RN
Research Associate
Child Health Evaluative Sciences,
Research Institute, Hospital for Sick
Children, Toronto, Ontario, Canada
Introduction
Responses of healthy term and preterm neonates to painful
procedures have been well documented (Johnston et al.
1997, Stevens et al. 1999, Thase et al. 2000, Craig et al.
2002). These behavioural and physiological responses have
been established as the basis for the development and
validation of multiple neonatal pain assessment measures by
researchers worldwide (See summary of neonatal pain
measures in Duhn & Medves 2004, Stevens et al. 2007a).
However, risk for neurological impairment (NI) has not
been adequately considered in pain assessment in neonates
by either clinicians or researchers. Risk for NI is determined
by a multiplicity of factors, including congenital syndrome/
chromosomal abnormalities (e.g. congenital trisomies), birth
trauma (e.g. fractures, nerve injuries), extreme preterm birth
[e.g. intraventricular haemorrhage (IVH); necrotising entero-
colitis (NEC)], and acquired illnesses with central nervous
system involvement (Robertson et al. 1998). Risk for NI is
an important consideration for pain assessment by clinicians
and researchers as infants at the highest risk for NI have
been reported to undergo statistically significantly more
painful procedures (e.g. heel lances) and to receive less
analgesia than infants at minimal or no risk for NI (Stevens
et al. 2003). Although physiological and behavioural pain
indicators in infants at risk for NI have been described
(Stevens et al. 2003, 2007b), little is known about how
these indicators are interpreted by the nurses who care for
these neonates in the clinical setting or by neonatal pain
researchers who generate knowledge to promote evidence-
based pain assessment and management. Pain may be
inaccurately assessed and managed in neonates at risk for
NI when reciprocal interaction between infant and care
provider is not adequately considered and when measures
that were not validated for neonatal and infant populations
at risk for NI are used. Therefore, triangulation of data
from multiple sources that is guided through a conceptual
framework will enhance our understanding and enhance-
ment of pain in this population.
Background
Two studies have been undertaken to explore healthcare
professionals pain perceptions. In the first study, 99 health-
care professionals completed the Pain Opinion Questionnaire
aimed at understanding beliefs and attitudes about pain
assessment and management in neonates at risk for NI. They
believed that these neonates have less pain than those who are
not at risk for NI, and that neonates at higher levels of NI are
likely to have less pain (Breau et al. 2006). In the second
B. Stevens et al.
286 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd
-
study, 95 healthcare professionals reviewed nine video clips
depicting preterm and term neonates having a heel lance
(Breau et al. 2004). Prior to the video, the level of NI was
provided. Ratings of pain, distress, and time to calm did not
vary statistically significantly with level of NI risk, but ratings
of the effectiveness of a non-pharmacological intervention
were statistically significantly lower as risk increased. Neither
study included an assessment of how healthcare professionals
rated the importance and/or usefulness of individual pain
indicators. No research to our knowledge has examined these
ratings in neonatal/infant pain researchers.
Conceptual model
The Socio Communication Model of Infant Pain (Craig &
Pillai Riddell 2003) provided the conceptual framework for
this study. This model asserts that infant pain should be
viewed as a dynamic, interactive process between infant and
caregiver. Two stages of inquiry (Pain Expression; Pain
Experience) are central to this model. Pain expression is
operationalized as the response of infants to a painful (tissue-
damaging) procedure. As pain is subjective (International
Association for the Study of Pain, 2003) and, given the
infants incapacity of verbal report, behavioural and physi-
ological indicators are accepted as proxies for self-report
(Anand & Craig 1996). Furthermore, due to the infants
vulnerable nature and their dependency on caregivers, their
pain is intrinsically linked to the caregiver. Pain Experience is
determined by how: (a) clinicians who care for these infants
and (b) researchers who develop infant pain measures
interpret the pain expression of infants at risk for NI, in
either clinical practice or the development of neonatal pain
measures. To link the stages of inquiry proposed in the
conceptual framework with our data collection methods, we
elicited the perspectives of clinicians and researchers on the
importance and usefulness of potential pain indicators,
observed the behavioural and physiological indicators of
pain in infants undergoing a painful event, and through the
process of data triangulation, determined how pain expres-
sion and pain experience were influenced by NI risk status in
infants.
The study
Aim
The aim of this study was to compare the importance and
usefulness ratings of physiological and behavioural indicators
of pain in neonates at risk for NI by nurse clinicians and pain
researchers.
Design
Three sets of data were obtained from three sources and
integrated through a process of triangulation. Triangulation
involves using multiple sources, methods and investigators to
corroborate evidence to shed light on a theme or perspective
(Creswell 1998). Nurses in clinical practice and pain
researchers opinions on the importance and usefulness of
these indicators of pain were compared to the neonates
expressions of pain during a painful procedure. This study
was one of five investigations in a programme of research on
Pain in Infants at risk for Neurological Impairment (PINI)
supported by a grant from the Canadian Institutes of Health
Research (MCT 63143).
Participants
Neonates
The first set of data was collected from a prospective obser-
vational cohort study of 149 neonates at three tertiary level
neonatal intensive care units (NICUs) in central and eastern
Canada (Stevens et al. 2007b). Eligible neonates were hos-
pitalized in the NICU,>25 weeks gestational age,
-
Pain researchers
The third set of data was collected from 14 international,
multidisciplinary pain researchers as part of a Delphi consen-
sus exercise (Stevens et al. 2006). These experts were identified
by the 13 PINI study investigators and from the International
Association for the Study of Pain Directory ofMembers, 2004.
Eligible participants had at least 2 years of research experience
related to the assessment andmanagement of pain in neonates,
infants and young children, had published in peer-reviewed
pain journals, had presented at major paediatric pain meetings
or were known to be involved in current research in neonatal/
infant pain. Co-investigators in the PINI programme of
research were excluded.
Data collection
Neonatal physiological data were collected using a comput-
erized multi-channel data collection system (Compumedics
USA Ltd., El Paso, TX, USA) coordinated with behavioural
data collected by audiotaping and videotaping infants during
baseline, procedure, and return to baseline phases of a routine
heel lance procedure. Data collection procedures/protocols
that have been validated in multiple studies by Stevens and
Johnston are described elsewhere (Johnston et al. 1996,
Stevens et al. 1999, 2003, 2007b). All data were collected for
the three studies between 2004 and 2005. Demographic data
were abstracted from neonates medical records.
Physiological pain indicators
Changes from baseline in heart rate, heart rate variability and
oxygen saturation were assessed. In previous research on
healthy term and preterm neonates, heart rate and oxygen
saturation have been the most prevalent physiological indi-
cators of pain and have been included in several composite
neonatal pain measures (van Dijk et al. 2000, Debillon et al.
2001), including the Premature Infant Pain Profile (Stevens
et al. 1996).
All physiological and behavioural data were collected using
the Compumedics E-Series ProFusion PSG documentation
software (Compumedics USA Ltd.). Disposable ECG elec-
trodes and pulse oximetry probes were placed on the
neonates and ECG, respiratory rate and oxygen saturation
were continuously recorded using a cardiorespiratory mon-
itor and personal computer (1000 HZ sampling rate). An
electronic event marker was used to mark each phase of the
heel lance procedure.
Behavioural pain indicators
Facial actions were collected by videotaping the neonates
pain response on an 8 mm camcorder (Sharp, Panasonic or
Sony) and audiotaping through all phases of the heel lance
procedure. Facial actions were independently coded second-
to-second according to a reliable and valid measure of facial
expression, the Neonatal Facial Coding System (NFCS)
(Grunau & Craig 1990, Stevens et al. 2007a) by two trained
coders with established inter- and intra-rater reliability
(>95%). A final score based on percentage of time the action
was present was calculated for each individual indicator. A
total facial action score was calculated by summing the
individual scores.
Procedure for nurse and researcher data collection
A 39- item self-administered questionnaire was developed by
the investigators to include indicators representing neonatal
physiological, behavioural and contextual pain responses as
well as pain indicators identified by parents and healthcare
professionals (Stevens et al. 2006). Face and content validity
were established with the 13 study investigators and with 10
advanced practice nurses with expertise in pain assessment
and management from three local neonatal and paediatric
intensive care units. As a result of this validation, only minor
changes were made to the formatting and wording of the
questionnaires.
The questionnaire was organized to assess four domains: (a)
physical indicators (11 items); (b) facial actions (ten items); (c)
vocal behaviour/cry indicators (nine items); (d) neonatal
activity (nine items). Each participant was asked to give
opinions on the importance and usefulness of the pain
indicators for neonates at high, moderate, and low risk for
NI. Importance and usefulness were each rated on a Ten-point
analogue scale, where a score of 1 = not important/useful at
all and 10 = extremely important/useful. Importance referred
to how crucial the pain indicator was in accurately and
consistently identifying pain following a painful tissue dam-
aging procedure. Usefulness referred to the feasibility (i.e.
how easily the pain indicator was to observe and score) and
clinical utility (i.e. how useful the pain indicator was for
making decisions about individualized pain management
(Stevens & Gibbins 2002). An indicator could be important
for accurately measuring pain but not useful because of the
difficulties in using it to assess pain in clinical practice.
An explanation of the purpose and description of the
research was given to participants, with opportunities for
clarification of questions prior to completion of the ques-
tionnaire. Definitions of pain indicators were provided and
respondents were asked to add any additional indicators they
felt were important or useful. Demographic information and
years of experience with neonates at risk for NI data were
also obtained from each participant. The questionnaire took
approximately 2030 minutes to complete.
B. Stevens et al.
288 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd
-
Questionnaires were distributed to eligible researchers
electronically (e-mail) by a research administrative assistant
who was not familiar with the study or participants and who
could not link the participants identity with any response.
Reminder emails were sent to individuals 2 weeks after the
initial email, and after the questionnaires were returned the
indicators were ordered by importance and usefulness ratings
and returned to the participants for a second round of
consensus rating. The ratings from the second round were
considered final and were used for the analysis.
Questionnaires were distributed to eligible nurse clinicians
in paper and pencil form in each clinical setting by a research
nurse. They were completed individually during break
periods or at educational sessions and were returned in
unmarked envelopes in a central collection designation to
ensure confidentiality and anonymity.
Ethical considerations
All included studies in this program of research were
approved by the Research Ethics Boards at the universities
and university-affiliated participating paediatric hospitals.
Written consent was obtained from parents for the cohort
study of neonates. Participation in the surveys was voluntary
and return of completed questionnaires by nurse clinicians
and pain research implied consent to participate.
Data analysis
The neonatal behavioural and physiological pain indicators
constituted the gold standard for acute procedural pain.
These indicators were compared to the nurse and researcher
ratings in terms of importance and usefulness. Cutoff values
for each indicator were established to classify infants as
being in pain or not in pain. These estimates of pain
accuracy gave a good indication of which variables were
important in identifying pain vs. which variables provided
little or no information. This information served as the basis
for comparing nurse and researcher assessments to the
information gained from the neonates at different levels of
NI risk.
Baseline data served as the no pain state which was
compared to the pain state (defined as the most invasive
stick phase of the heel lance procedure) so that each neonate
served as their own control. For each variable, all possible
cutoffs were evaluated for their ability to classify infants as
being in no pain or pain. All values below the given cutoff
were classified as no pain and all values above the cutoff
were classified as pain. Each variables accuracy was
calculated as 1 (the total misclassification rate) and was
expressed as a percent value. The cutoff that maximized
accuracy was chosen as the best cutoff for that variable.
Preliminary analyses showed similar optimum cutoffs and no
differences in patterns across the three NI risk groups so that,
in subsequent analyses, a single cutoff was selected for all
neonates.
Changes from baseline values were also examined, with
change from baseline to the warming phase of the heel lance
representing no pain and change from baseline to stick phase
of the heel lance representing pain. Data from the warming
phase suggested that warming itself was an intervention that
decreased heart rate. Consequently, the direction of change
from baseline to warming or warming to baseline was
randomly assigned for each neonate to obtain an estimate of
the variability of change between two no pain states.
Estimates of accuracy based on the same sample used to
derive the best cutoff values were considered optimistic.
Unbiased estimates were obtained using bootstrapping to
create replicate datasets of the pain indicator data. To create
each replicate, a neonate was randomly selected from the
pool of subjects. After each draw, the selected neonate was
replaced in the same pool and the draw was repeated until the
sample size was equal to that of the original sample. The best
cutoff value was estimated for each of 1000 bootstrap
samples created to establish a reference distribution for the
sample of 149 neonates. This cutoff was applied to the data
on neonates that were not selected for the given sample.
Analysis of data from neonates not included in the bootstrap
sample provided an estimate of the optimism that could be
used to correct estimates of accuracy, sensitivity and speci-
ficity derived from the original data.
Estimates of accuracy based on the neonatal data were
compared to the importance of the pain indicators, rather
than their usefulness, as rated in the researchers opinion
surveys. Evaluating the usefulness of pain indicators would
require information on how difficult it would be to measure
these pain variables and the neonatal data could not provide
this information. Accuracy is expressed was a percentage
whereas nurse and researcher ratings were expressed on a
scale from 0 to 10. To compare the gold standard pain
indicators (i.e. neonatal data) to nurse and researcher ratings,
a linear relationship between accuracy and importance rating
was assumed. An accuracy of 50% for discriminating the
pain and no pain states is no better than chance, and thus
corresponds to a rating of 0. Conversely, 100% accuracy
corresponds to a rating of 10. Figures were created to
compare the accuracy of each pain indicator to the nurse and
researcher ratings, and the correlation coefficient for each
comparison was calculated. Results were reported using 95%
confidence intervals. SAS statistical software, version 9.1
JAN: ORIGINAL RESEARCH Indicators of pain in neonates
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 289
-
(SAS Institute Inc., Carey, NC, USA) was used to analyze the
data.
Results
The number of pain indicators that were common to all three
data sets (i.e. neonates, nurses and pain researchers) reduced
the number of variables from 39 to 13; these indicators
formed the basis for the analysis and included 10 facial
expression variables: brow bulge, eye squeeze, nasolabial
furrow, open lips, chin quiver, lip purse, taut tongue,
horizontal stretch mouth, vertical stretch mouth, total facial
expression and three physiologic variables: increase or
decrease in heart rate and decrease in oxygen saturation.
Table 1 Neonatal characteristics of study sample by group*
High risk for NI Moderate risk for NI Low risk for NI F, P-value
GA at birth (weeks) 3400(527)n = 54
3111(534)n = 45
3142(393)n = 50
F(2,146) = 541, P = 0005
Birth weight (grams) 222774(113444)n = 54
78473(109709)n = 45
165688(73569)n = 50
F(2,146) = 462, P = 0011
Apgar score (5 minutes) 723(214)n = 53
769(134)n = 45
826(127)n = 50
F(2,145) = 503, P = 0008
SNAPP: PE score 2085 (2165)n = 53
2424(2120)n = 45
1314(1666)n = 50
F(2,145) = 392 P = 0022
NTISS score 1558(882)n = 53
1667(770)n = 45
1444(521)n = 50
F(2,145) = 107, P = 0346
GA, gestational age; SNAPP: PE, score for neonatal acute physiology-perinatal extension; NTISS, neonatal therapeutic intervention scoring
system; NI, neurological impairment.
All values expressed as means (standard deviation).
*Adapted from Stevens et al. 2007b.
Table 2 Nurse and pain researcher charac-
teristics*Nurses
N = 95
Pain researchers
N = 14
Respondents professional
role
General duty nurse = 75
CNS-NNP = 8
Nurse educator = 6
Other = 2
N = 91
Nurse scientists = 9
Psychologist = 4
Physical Therapist = 1
N = 14
Mean number of years in
current position
984 (790) (minimum 79 years;maximum 30 years)
N = 88
1339 (656) (minimum5 years; maximum 24 years)
N = 13
Professional contact with
infants who have or
at risk for neurological
impairment
None = 2
Very little = 9
Moderate amount = 27
Great deal = 52
N = 90
None = 4
Very little = 2
Moderate amount = 3
Great deal = 5
N = 14
Non-professional contact
with infants who have or
are at risk for neurological
impairment
None = 20
Very little = 45
Moderate amount = 17
Great deal = 9
N = 91
None = 2
Very little = 8
Moderate amount = 3
Great deal = 1
N = 14
Academic or school-based
learning about infants at
risk for neurological
impairment
None = 10
Very little = 29
Moderate amount = 38
Great deal = 14
N = 91
None = 2
Very Little = 3
Moderate amount = 3
Great deal = 6
N = 14
*Adapted from Stevens et al. 2006.
CNS-NNP, clinical nurse specialist-neonatal nurse practitioner.
B. Stevens et al.
290 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd
-
Additional variables that were suggested by the nurses and
pain researchers (e.g., body movements, consolability, finger
splay) were not observed in neonates in the existing data and
therefore were not included in these analyses.
The characteristics of the neonates, nurses and pain
researchers are summarized in Tables 1 and 2. As reported
previously (Stevens et al. 2007b), neonates at the highest risk
for NI had higher birth weights, increased maturity, higher
NBRS (Neonatal Neurobiologic Risk Score) and lower Apgar
scores than the other two groups. Neonates at moderate risk
for NI had statistically significantly higher severity of illness
scores, spent more days on the ventilator in low flow oxygen/
air. The number of days until no further apnea, bradycardia
and/or desaturation spells occurred was the highest in the
moderate NI risk group.
Estimates of accuracy for each of the infant pain
indicators across NI risk groups revealed that the four
variables with the highest accuracy for discriminating pain
and no pain in infants were: brow bulge (7783% within
the three risk groups), eye squeeze (7584%), nasolabial
Table 3 Optimal cutpoints* for the variables with highest accuracy
for discriminating between pain and no pain states
Variables Cutpoint (95% CI)
Total facial 1085 (99; 120)Brow bulge 125 (6; 24)Eye squeeze 105 (3; 12)Naso-labial furrow 95 (7; 18)
*Cutpoints were selected to maximize accuracy; all observations
below the cutpoint are classified as no pain and all observations
above the cutpoint are classified as pain states.
Table 4 Mild risk group
Infants Nurses Researchers
Sensitivity Specificity Accuracy Mean ratings Mean ratings
Total facial 71 (51; 87) 93 (77; 99) 83 (70; 91) 86 93Brow bulge 69 (49; 85) 91 (73; 98) 80 (67; 90) 81 91Eye squeeze 64 (43; 81) 94 (78; 99) 79 (66; 89) 82 86Naso-labial furrow 70 (49; 86) 89 (71; 97) 79 (66; 86) 75 79Horizontal stretch mouth 43 (24;63) 97 (81; 100) 70 (56; 82) 61 59Increase in mean heart rate 78 (59; 91) 56 (35; 75) 67 (53; 80) 86 73Open lips 71 (51; 86) 57 (37; 75) 64 (50; 77) 62 62Vertical stretch mouth 29 (13; 50) 97 (82; 100) 63 (49; 76) 63 52Taut tongue 23 (10; 44) 98 (83; 100) 61 (47; 75) 58 59Decrease in oxygen saturation 47 (28; 67) 72 (50; 87) 59 (44; 72) 82 71Chin quiver 3 (0; 19) 100 (86; 100) 52 (38; 66) 67 41Decrease in mean heart rate 96 (81; 99) 5 (1; 22) 52 (38; 66) 76 38Lip purse 1 (0; 15) 99 (85; 100) 51 (37; 65) 59 24
Table 5 Moderate risk group
Infants Nurses Researchers
Sensitivity Specificity Accuracy Mean ratings Mean ratings
Total facial 69 (45; 86) 89 (67; 97) 78 (63; 89) 84 91Brow bulge 62 (40; 81) 92 (72; 99) 77 (62; 88) 79 90Eye squeeze 58 (36; 78) 92 (73; 99) 75 (59; 57) 81 84Naso-labial furrow 65 (43; 84) 93 (74; 99) 79 (64; 90) 73 78Horizontal stretch mouth 44 (23; 66) 100 (83; 100) 72 (56; 84) 59 56Increase in mean heart rate 75 (53; 90) 43 (23; 65) 59 (43; 73) 88 72Open lips 67 (44; 84) 58 (36; 78) 62 (46; 77) 60 61Vertical stretch mouth 21 (7; 44) 89 (68; 98) 55 (38; 70) 60 51Taut tongue 17 (5; 41) 97 (78; 100) 57 (40; 73) 57 61Decrease in oxygen saturation 62 (39; 81) 78 (55; 92) 70 (54; 83) 86 74Chin quiver 5 (0; 24) 100 (83; 100) 52 (36; 67) 65 39Decrease in mean heart rate 98 (81; 100) 4 (1; 22) 51 (35; 66) 81 51Lip purse 1 (0; 18) 100 (83; 100) 50 (34; 66) 58 21
JAN: ORIGINAL RESEARCH Indicators of pain in neonates
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 291
-
furrow (7981%), and total facial expression (7883%).
The cut-off values for these variables are presented in
Table 3. No statistically significant differences were
observed in the neonatal data between accuracy estimates
among the three risk groups. However, there was a non-
statistically significant but consistent trend towards higher
indicator accuracy in the most severe NI risk group
compared to the mild group. The physiological variables
used in the analysis (i.e. increase and decrease in mean heart
rate and decrease in oxygen saturation) demonstrated poor
accuracy (Tables 46).
The nurse-neonate correlations were lower than
researcher-neonate correlations. The level of statistical sig-
nificance for the high NI group was P = 0014, for the
moderate NI group was P = 015 and for the mild NI group
was P = 0025. Nurse-infant correlations ranged from 052,
P = 007 for the mild NI risk group, 043, P = 015 for
moderate NI risk and zero correlation, 012, P = 069 forthe high NI risk group. Nurses said that physiological
variables were more important for assessing pain in the high
NI risk group compared to the mild NI risk group (paired t-
test, P = 009). However, when the mild and high risk groups
were compared, there was an increase in accuracy for the
behavioural variables and a decrease in accuracy for the
physiological variables. With increases in risk for NI,
variables were ranked as less important by the nurses,
whereas a trend towards increased accuracy with increasing
severity existed. There was little variability in nurses ratings,
with average mean ratings ranging from 55 to 88/10 across
all NI risk groups (Figure 1).
Pain researchers showed very good understanding of the
relative importance of the different pain variables, as dem-
onstrated by the high correlation between their ratings and
accuracy scores of the neonates. The correlation between
neonate and researcher data was very high for mild 091,
P < 00001 and moderate NI risk groups (085, P = 00002),
but lower for the high NI risk group (064, P = 0019). These
researchers ranked variables as less important for the high NI
risk infants; however, they assigned a greater range of mean
ratings to the variables (2093) (Figure 1).
When infants in each NI risk group were compared against
each other, they were highly correlated in how they expressed
pain: mild compared to moderate risk group correlation =
091; mild compared to high risk group correlation = 092;
moderate compared to high risk group correlation = 079.
Discussion
Study limitations
Although this study illustrates the importance of taking the
perspectives of nurse clinicians and pain researchers into
consideration, several limitations merit discussion. First, only
a limited number of pain indicators could be included in the
study specifically those that were available across the
neonate, nurse and pain researcher data sets. Although it is
unreasonable to consider evaluating a much broader scope of
neonatal pain variables, there is the possibility of including
frequently-emerging indicators such as gross and fine body
movements and indicators of cortical involvement in future
studies of this nature.
Second, only attributes of importance and feasibility were
investigated for nurses and pain researchers. As it is essential
to establish validity of pain assessment indicators further
across a wide spectrum of neonates with varying levels of risk
for NI, our aim was to focus on and maximize the construct
Table 6 Severe risk group
Infants Nurses Researchers
Sensitivity Specificity Accuracy Mean ratings Mean ratings
Total facial 82 (59; 94) 83 (62; 94) 82 (68; 92) 79 89Brow bulge 82 (61; 94) 84 (64; 95) 83 (69; 92) 75 87Eye squeeze 81 (60; 94) 86 (66; 96) 84 (70; 93) 76 81Naso-labial furrow 85 (64; 96) 78 (57; 91) 81 (68; 91) 69 76Horizontal stretch mouth 61 (38; 81) 93 (74; 99) 78 (63; 89) 57 54Increase in mean heart rate 76 (55; 90) 50 (30; 70) 63 (48; 76) 88 74Open lips 76 (54; 90) 57 (37; 75) 66 (50; 79) 57 57Vertical stretch mouth 59 (37; 80) 86 (66; 96) 73 (58; 85) 57 48Taut tongue 47 (25; 71) 92 (73; 99) 72 (57; 85) 55 59Decrease in oxygen saturation 51 (30; 71) 59 (38; 78) 55 (40; 69) 88 74Chin quiver 4 (0; 22) 98 (82; 100) 54 (39; 69) 61 36Decrease in mean heart rate 93 (76; 98) 2 (0; 18) 48 (33; 63) 85 54Lip purse 4 (0; 23) 96 (79; 100) 53 (38; 68) 57 20
B. Stevens et al.
292 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd
-
Mean nurse ratings vs. accuracy Mild
50 60 70 80 90 100
108
64
20
BBESNF
OLCQ
LP TT HMVM
TF
DH
IHDO
R = 052
Mean expert ratings vs. accuracy
50 60 70 80 90 100
108
64
20
BBESNF
OL
CQ
LP
TTHMVM
TF
DH
IHDO
R = 091
Moderate
50 60 70 80 90 100
018
64
20
BBES
NF
OLCQ
LP TT HMVM
TFDHIH DO
R = 043
50 60 70 80 90 100
108
64
20
BBES
NF
OL
CQ
LP
TTHM
VM
TF
DH
IH DO
R = 085
Severe
50 60 70 80 90 100Accuracy
108
64
20
BBESNF
OLCQ
LP TT HMVM
TFDH
IHDO
R = 012
50 60 70 80 90 100Accuracy
108
64
20
BBES
NF
OL
CQ
LP
TTHM
VM
TF
DH
IHDO
R = 064
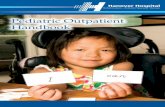
Figure 1 Accuracy Ratings of Nurses and Researchers for Pain Indicators by NI risk group. Mean nurse and researcher ratings are plotted
against estimated accuracy for each physiological and behaviour variable. TF, total facial; BB, brow bulge; ES, eye squeeze; NF, naso-labial
furrow; HM, horizontal stretch mouth; IH, increase in mean HR; OL, open lips; VM, vertical stretch mouth; TT, taut tongue; DO, decrease in
O2sat; CQ, chin quiver ; DH, decrease in mean HR and LP, lip purse. The dashed line represents perfect agreement, assuming that 50% accuracy
(random chance) is equivalent to a rating of 0 and 100% accuracy represents a rating of 10. The solid line is a least squares fit of the data.
JAN: ORIGINAL RESEARCH Indicators of pain in neonates
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 293
-
of accuracy. Therefore, sensitivity and specificity, although
reported, were not of primary concern in this study. Future
research with a control situation will be required to establish
the optimum cut-offs for pain to maximize sensitivity and
specificity.
Comparison with previous research
In this study, the accuracy of pain assessment in neonates at
varying levels of risk for NI was determined from the
perspectives of practising neonatal nurses and neonatal/infant
pain research experts compared to data generated by the
neonates during a painful procedure. Ultimately, it is impor-
tant to determine whether existing pain measures are valid
and reliable for assessing pain in newborn infants across the
broad spectrum of risk for NI and consistent with the
conceptualization for this study, understanding the percep-
tions of healthcare providers about pain is crucial.
As corroborated by other research (Stevens et al. 2007c),
behavioural indicators were more consistently accurate and
representative of the neonates response to pain. Nurses and
researchers considered these indicators important. This find-
ing continues to support the external validity of multidimen-
sional behavioural measures such as the NFCS (Grunau &
Craig 1990), yet fuels the discussion on whether composite
pain measures such as the PIPP (Premature Infant Pain
Profile; Stevens et al. 1996) and DAN (Douleur Aigue du
Nouveau-ne; Carbajal et al.1997) have construct validity and
clinical utility. Recent findings in an in-depth series of factor
analyses indicate that physiological indicators (e.g. heart rate,
heart rate variability, oxygen saturation), although contrib-
uting less to the total pain response, still give important
information on the level of pain intensity for infants across
NI groups undergoing painful procedures (Stevens et al.
2007c).
Of particular interest in the present study was the high pain
researcher-neonate pain indicator correlations compared to
moderate nurse clinician-neonate correlations. This finding
could be attributed to our enhanced knowledge about
neonatal pain indicators, much of which may have been
directly contributed by researchers through the development
of pain assessment measures or evaluation of pain-relieving
strategies in neonates and infants. They may have also
benefited from the two rounds of the Delphi study, where
they received feedback in the initial round which may have
led to more precise identification of indicator importance in
the second round. However, it is reasonable to expect that
NICU nurses would have more practical expertise with
neonates undergoing painful procedures and familiarity with
neonates of all levels of NI risk; thus, would be able to
discriminate more accurately between pain indicators
amongst NI risk groups, should they exist. Yet, increased
risk for NI was rated as less important by nurses even though
the results showed a trend towards increased accuracy of pain
indicators with increasing risk of NI. Further exploration of
the meaning of this finding in terms of nursing assessment of
neonatal pain is required to better understand this result.
There was little variability in nurses ratings of pain
indicators; they considered that most indicators were of
moderate to high importance for discriminating pain in
neonates. Although there is no obvious reason for this
finding, nurses may have difficulty discriminating important
from unimportant indicators, or they may not believe that
these indicators represent pain or that pain is important in
these neonates. Conversely, one might wonder why the pain
researcher-neonate correlations were so high, yet were lower
(similar to nurses) for the most at-risk NI neonates. Does this
suggest that both research and clinical experts are consistent
What is already known about this topic
Neonates at risk for neurological impairment have notbeen systematically included in the development of
neonatal pain measures.
The validity of existing pain measures is unknown forthis population of vulnerable infants.
What this paper adds
Behavioural indicators were rated as the most impor-tant indicators in the neonates response to pain by
both nurse clinicians and pain researchers.
Pain researchers ratings of pain indicators showedhigher correlations with neonatal physiological and
behavioural pain indicators compared to nurses clini-
cians ratings.
Ratings of both pain researchers and nurse clinicianson the importance of behavioural and physiological
indicators were opposite to the actual pain responses
demonstrated by infants.
Implications for practice and/or policy
The influence of context on process and outcomesneeds to be unravelled if we hope to improve clinical
outcomes, particularly decreased pain intensity, for
these vulnerable neonates.
Development of infant pain assessment policies shouldinclude input from both healthcare professionals and
pain researchers.
B. Stevens et al.
294 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd
-
in their thinking, namely that as NI risk status increases,
physiological variables become more important than
behavioural indicators, resulting in their assignment of lower
importance to behavioural indicators but higher importance
to physiological indicators? Pain researchers ratings sug-
gested a higher level of association with neonatal variables;
yet, both nurses and pain researchers opinions were oppo-
site to the pain indicators demonstrated by neonates. That is,
nurses and pain researchers thought behavioural indicators
were more important in the mild NI risk group than in the
severe NI risk group, and physiological indicators were more
important in the high NI risk group than in the low risk
group. Conversely, neonates demonstrated (by the accuracy
scores) that behavioural indicators were more important in
the high risk group compared to the low risk group, and
physiological indicators were more important in the low risk
group compared to the high risk group. These results are
puzzling and raise the question of whether the attributes of
importance and usefulness capture the essence of what is
crucial in pain assessment with neonates.
Conclusion
The clinical implications of these findings relate directly to
how nurses evaluate pain in hospitalized neonates. There are
clearly differences in the importance and validity of various
indicators from the perspectives of nurses and pain research-
ers that could influence the nature and frequency of pain
assessment and management in these vulnerable neonates.
These differences are not dissimilar to the quandaries of
knowledge translation, where we are unsure of the influence
of context (e.g. opinions and values of clinicians) on the
translation of evidence into practice. Unraveling the influence
of context on process and outcomes is important if we hope
to improve clinical outcomes, particularly decreased pain
intensity, for these vulnerable neonates.
Development of infant pain assessment policies should
include input from both healthcare professionals and pain
researchers. Further research is warranted on how nurse
clinicians conceptualize pain in infants and on the develop-
ment and evaluation of knowledge translation strategies that
will effectively translate infant pain research into practice.
Acknowledgements
We acknowledge the research nurses who participated in the
collection and management of study data including Marilyn
Ballantyne, Anne Jack, Marie Bagg, Mary Anne Fagan, Janet
Narciso, Kim Caddell, Janet Chee Salena Mohammed-
Breault, Sandy Lin and Karolina Kupczyk. Finally, we are
grateful for the willingness of the infants families who agreed
to participate in this study.
Funding
Funding is acknowledged from the Canadian Institutes of
Health Research (MOP-37884) and the Bloorview Childrens
Hospital Foundation. We would also like to acknowledge
financial support from the Ontario Ministry of Health for
the Career Scientist Award and the Signy Hildur Eaton Chair
in Paediatric Nursing Research at the Hospital for Sick
Children to B. Stevens, a Canada Research Chair Award to
P. McGrath, and a Canadian Institutes of Health Research
Fellowship to J. Yamada.
Author contributions
BJS, PM, SG, LB, CSC, GAF, LF, AH, CJ, PMcK & AO were
responsible for the study conception and design. CSC, AH &
JY performed the data collection. BJS, PM, AD, JB & CJ
performed the data analysis. BJS, PM, AD, SG, JB, LF & JY
were responsible for the drafting of the manuscript. BJS, PM,
SG, JB, CSC, GAF, LF, KOB, AO & JY made critical
revisions to the paper for important intellectual content. BJS,
AD & JB provided statistical expertise. BJS, PM, SG, JB, LB,
GAF, AH, CJ, PMcK, KOB & AO obtained funding. AH &
JY provided administrative, technical or material support.
BJS, CSC & AH supervised the study.
References
Anand K.J. & Craig K.D. (1996) New perspectives on the definition
of pain. Pain 67(1), 36.
Breau L.M., McGrath P.J., Stevens B., Beyene J., Camfield C.S.,
Finley G.A., Franck L., Howlett A., OBrien K. & Ohlsson A.
(2004) Healthcare professionals perceptions of pain in infants at
risk for neurological impairment. BMC Pediatrics 4(1), 2331.
Breau L.M., McGrath P.J., Stevens B., Beyene J., Camfield C., Finley
G.A., Franck L., Gibbins S., Howlett A., McKeever P., OBrien K.
& Ohlsson A. (2006) Judgments of pain in the neonatal intensive
care setting: a survey of direct care staffs perceptions of pain in
infants at risk for neurological impairment. The Clinical Journal of
Pain 22(2), 122129.
Carbajal R., Paupe A., Hoenn E., Lenclen R. & Olivier-Martin M.
(1997) [APN: evaluation behavioral scale of acute pain in newborn
infants]. Archives de pediatrie 4(7), 623628.
Craig K.D. & Pillai Riddell R. (2003) Social influences, culture and
ethnicity. In Pediatric Pain: Biological and social context. Progress
in Pain Research and Management, Vol. 26 (McGrath P.J. &
Finley G.A., eds), IASP Press Seattle, Seattle, WA, pp. 159182.
Craig K.D., Korol C.T. & Pillai Riddell R. (2002) Challenges of
judging pain in vulnerable infants. Clinics in Perinatology, 29(3),
445457.
JAN: ORIGINAL RESEARCH Indicators of pain in neonates
2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd 295
-
Creswell J.W. (1998) Qualitative Inquiry and Research Design:
Choosing Among Five Traditions. Sage Publications Inc, Thousand
Oaks, CA.
Debillon T., Zupan V., Ravault N., Magny J.F. & Dehan M.
(2001) Development and initial validation of the EDIN scale, a
new tool for assessing prolonged pain in preterm infants.
Archives of disease in childhood. Fetal and Neonatal Edition
85(1), F36F41.
van Dijk M., de Boer J.B., Koot H.M., Tibboel D., Passchier J. &
Duivenvoorden H.J. (2000) The reliability and validity of the
COMFORT scale as a postoperative pain instrument in 0 to
3-year-old infants. Pain 84(23), 367377.
Duhn L.J. & Medves J.M. (2004) A systematic integrative review of
infant pain assessment tools. Advances in Neonatal Care 4(3),
126140.
Grunau R. & Craig K. (1990) Facial activity as a measure of neonatal
pain expression. In Advances in Pain Research and Therapy,
Pediatric Pain (Tyler D. & Krane E., eds), Raven Press Ltd,
New York, pp. 147153.
International Association for the Study of Pain (2003) IASP
Task Force on Taxonomy: IASP Pain Terminology. Retri-
eved from http://www.iasp-pain.org/AM/Template.cfm?Section=
Home&Template=/CM/HTMLDisplay.cfm&ContentID=6632 on
26 February 2008.
Johnston C.C., Stevens B., Yang F. & Horton L. (1996) Develop-
mental changes in response to heelstick in preterm infants:
a prospective cohort study. Developmental Medicine and Child
Neurology 38(5), 438445.
Johnston C.C., Stremler R.L., Stevens B.J. & Horton L.J. (1997)
Effectiveness of oral sucrose and simulated rocking on pain
response in preterm neonates. Pain 72(12), 193199.
Robertson C.M., Svenson L.W. & Joffres M.R. (1998) Prevalence of
cerebral palsy in Alberta. The Canadian Journal of Neurological
Sciences 25(2), 117122.
Stevens B. & Gibbins S. (2002) Clinical utility and clinical signifi-
cance in the assessment and management of pain in vulnerable
infants. Clinics in Perinatology 29(3), 459468.
Stevens B., Johnston C., Petryshen P. & Taddio A. (1996) Premature
infant pain profile: development and initial validation. The Clinical
Journal of Pain 12(1), 1322.
Stevens B., Johnston C., Franck L., Petryshen P., Jack A. & Foster G.
(1999) The efficacy of developmentally sensitive interventions and
sucrose for relieving procedural pain in very low birth weight
neonates. Nursing Research 48(1), 3543.
Stevens B., McGrath P., Gibbins S., Beyene J., Breau L., Camfield C.,
Finley A., Franck L., Howlett A., McKeever P., OBrien K.,
Ohlsson A. & Yamada J. (2003) Procedural pain in newborns at
risk for neurologic impairment. Pain 105(12), 2735.
Stevens B., McGrath P., Yamada J., Gibbins S., Beyene J., Breau L.,
Camfield C., Finley A., Franck L., Howlett A., Johnston C.,
McKeever P., OBrien K. & Ohlsson A. (2006) Identification of
pain indicators for infants at risk for neurological impairment: a
Delphi consensus study. BMC Pediatrics, 6, 1.
Stevens B., Pillai R.B., Oberlander T. & Gibbins S. (2007a) Assess-
ment of pain in neonates and infants. In Pain in Neonates and
Infants (Stevens B. & McGrath P., eds), Elsevier, Edinburgh, UK,
pp. 6790.
Stevens B., McGrath P., Gibbins S., Beyene J., Breau L., Camfield C.,
Finley A., Franck L., Howlett A., Johnston C., McKeever P.,
OBrien K., Ohlsson A. & Yamada J. (2007b) Determining
behavioural and physiological responses to pain in infants
at risk for neurological impairment. Pain 127(12), 94
102.
Stevens B., Franck L., Gibbins S., McGrath P.J., Dupuis A., Yamada
J., Beyene J., Camfield C., Finley G.A., Johnston C., OBrien K. &
Ohlsson A. (2007c) Determining the structure of acute pain
responses in vulnerable neonates. The Canadian Journal of Nurs-
ing Research 39(2), 3247.
Thase M.E., Friedman E.S., Berman S.R., Fasiczka A.L., Lis J.A.,
Howland R.H. & Simons A.D. (2000) Is cognitive behavior ther-
apy just a nonspecific intervention for depression? A retrospective
comparison of consecutive cohorts treated with cognitive behavior
therapy or supportive counseling and pill placebo. Journal of
Affective Disorders 57(13), 6371.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the
advancement of evidence-based nursing, midwifery and health care by disseminating high quality research and
scholarship of contemporary relevance and with potential to advance knowledge for practice, education, management
or policy. JAN publishes research reviews, original research reports and methodological and theoretical papers.
For further information, please visit the journal web-site: http://www.journalofadvancednursing.com
B. Stevens et al.
296 2008 The Authors. Journal compilation 2008 Blackwell Publishing Ltd