
ORIGINAL COMMUNICATIONS Triangular fibrocartilage...
13
COMMUNICATIONS ORIGINAL Triangular fibrocartilage complex lesions: A classification Based on anatomic andbiomechanical studies andreviewof our clinical experience of the past 10 years, a classificationof injuries to the triangular fibrocartilage complex is p~-esented. This classification is based on the clinical examination, routine x-rayfilms, wrist arthrograms, wrist arthroscopy, and wrist arthrotomy. The classification recognizes both traumatic and degenerative lesions. Traumatic lesions are classified according to their location. Degenerative lesions are classified by the location and severity of degeneralive changes of the triangular fibrocartilage complex~ ulnar head, Ulnocarpal bones andlunotriquetral ligament.(J HAND SURG 1989;14A:594" 606.) Andrew K. Palmer, MD, Syracuse, N.Y. 198 .One of the most common wrist problems seen by practicing hand surgeons is a patient with ulnar wrist painl At times, there is a clearcut history of trauma, the examination reveals definitive pathologic conditions, the radiographic or other ancillary studies performed (such as bone scan, tomogram, computed tomogr~aphy (CT) scan, or arthrogram) are confirmatory of the presumed diagnosis and treatment is quite straightforward.l -n Unfortunately, however,the oppo- site mrre~often is true, i.e., the pain is chronic, is not associated with a clearcut history of trauma, the ex- amination is relatively normal, and the plain x-ray films, or ancillary studies reveal "no significant abnor- mality." These latter patients, more often than not, have enough symptoms to limit employment and demand treatment.. There are presently more than three dozenrecognized causes of acute and chronic ulnar wrist pain including fractures, dislocations, ligament injuries, avascularne- crosis and degenerativechangesof the distal radioulnar From the Department of Orthopaedic Surgery, SUNY Health Science Center, Syracusg, N.Y. Received for p~biication April 28, 1988; accepted in revised form Sept. 29, 1988. ¯ - " from Nobenefits in any form have been recetved or wdl be received a commercial party relatrd directly Or indirectly to the subject of this article. : . Reprint requests: Andrew K. Palmer, MD, Director of Hand Surgery, SUNY Health Science Center, 500 Harrison Center, Syracuse, NY 13202. 594 THE JOURNAL OF HAND sURGERY joint artd ulnar carpu s.~’ 2, ~, 9-22In addition, the triangular fibrocartilage complex (TFCC) been, and are, a recognized cause of ulnar pain)’ :" 9, to, is, ~-3~ Unfortunately, usually been thought of in terms of "tears" of the izontal portion of this complex only) 3’ :~" 33 A review of published anatomic, biomechanical, graphic, and clinical data, as well as a retros review of the patients we have treated with pain, have revealed that manyabnormalities of TFCC. other than tears of the horizontal ist)’ 14, ~6, 29, 34-46 This article will introduce cation of traumatic and degenerative lesions TFCC that we have noted. Anatomic review ~ The TFCC is a complex anatomic and ical structure about which much is known.l, a, 36, 38-42.47-53 It is a cartilaginous, structure interposed between the ulna and the carpus that ari;es from the radius and inserts into’~l. dis~l ulna and ulnar carpus (Fig. 1). ; the trian~ cartilaginous portion, often referred to as fibro-cartilage (TFC)proper, is relatively avas~fi[1 whereas its peripheral-ligamentous portion is h.i~ / vascularizedd 2 The TFCCis composed of a numbS/ anatomic componentsthat are more easily as separate anatomicentities in some persons others. 4~, 51 The horizontal portion of the TFCC TFC) is bordered both dorsally and palmarly by ligamentousportions that have previously Fig. ! carlila ~crtinl Scaph the d to in the 1~ the ~ .,~ ,., app¢ diffi tx~n~ whe lion the T prc~
Transcript of ORIGINAL COMMUNICATIONS Triangular fibrocartilage...

COMMUNICATIONSORIGINAL
Triangular fibrocartilage complex lesions:
A classificationBased on anatomic and biomechanical studies and review of our clinical experience of the past10 years, a classification of injuries to the triangular fibrocartilage complex is p~-esented. Thisclassification is based on the clinical examination, routine x-ray films, wrist arthrograms, wristarthroscopy, and wrist arthrotomy. The classification recognizes both traumatic and degenerativelesions. Traumatic lesions are classified according to their location. Degenerative lesions areclassified by the location and severity of degeneralive changes of the triangular fibrocartilagecomplex~ ulnar head, Ulnocarpal bones and lunotriquetral ligament. (J HAND SURG 1989;14A:594"
606.)
Andrew K. Palmer, MD, Syracuse, N.Y.
198
.One of the most common wrist problems
seen by practicing hand surgeons is a patient with ulnarwrist painl At times, there is a clearcut history oftrauma, the examination reveals definitive pathologicconditions, the radiographic or other ancillary studiesperformed (such as bone scan, tomogram, computedtomogr~aphy (CT) scan, or arthrogram) are confirmatoryof the presumed diagnosis and treatment is quitestraightforward.l-n Unfortunately, however, the oppo-site mrre~often is true, i.e., the pain is chronic, is notassociated with a clearcut history of trauma, the ex-amination is relatively normal, and the plain x-rayfilms, or ancillary studies reveal "no significant abnor-mality." These latter patients, more often than not, haveenough symptoms to limit employment and demand
treatment..There are presently more than three dozen recognized
causes of acute and chronic ulnar wrist pain includingfractures, dislocations, ligament injuries, avascular ne-crosis and degenerative changes of the distal radioulnar
From the Department of Orthopaedic Surgery, SUNY Health ScienceCenter, Syracusg, N.Y.
Received for p~biication April 28, 1988; accepted in revised formSept. 29, 1988. ¯ - " from
No benefits in any form have been recetved or wdl be receiveda commercial party relatrd directly Or indirectly to the subject of
this article. : .Reprint requests: Andrew K. Palmer, MD, Director of Hand Surgery,
SUNY Health Science Center, 500 Harrison Center, Syracuse, NY
13202.
594 THE JOURNAL OF HAND sURGERY
joint artd ulnar carpus.~’ 2, ~, 9-22 In addition,the triangular fibrocartilage complex (TFCC)been, and are, a recognized cause of ulnarpain)’ :" 9, to, is, ~-3~ Unfortunately,usually been thought of in terms of "tears" of theizontal portion of this complex only)3’ :~" 33 Areview of published anatomic, biomechanical,graphic, and clinical data, as well as a retrosreview of the patients we have treated withpain, have revealed that many abnormalities of
TFCC. other than tears of the horizontalist)’ 14, ~6, 29, 34-46 This article will introduce cation of traumatic and degenerative lesions
TFCC that we have noted.
Anatomic review~ The TFCC is a complex anatomic and
ical structure about which much isknown.l, a, 36, 38-42.47-53 It is a cartilaginous,structure interposed between the ulna and the
carpus that ari;es from the radius and inserts into’~l.dis~l ulna and ulnar carpus (Fig. 1). ; the trian~cartilaginous portion, often referred to asfibro-cartilage (TFC)proper, is relatively avas~fi[1whereas its peripheral-ligamentous portion is h.i~/vascularizedd 2 The TFCC is composed of a numbS/anatomic components that are more easilyas separate anatomic entities in some personsothers.4~, 51 The horizontal portion of the TFCCTFC) is bordered both dorsally and palmarly by
ligamentous portions that have previously
Fig. !carlila~crtinlScaph
the d
to inthe 1~the ~.,~ ,.,
app¢diffitx~n~whelionthe
T
prc~

Vol. 14A, No. 4July 1989 Classification of TFCC lesions 595
Fig. 1. An anatomic specimen showing the triangular fibro-cartilage complex (TFCC) arising from the radius and in-,:-~iag into the ulnar styloid base and ulnar carpal bones. S,
i~.,,id; L, lunate; T, triquetrum. (Reprinted with permis-~ t?om Palmer AK, Werner FW. The triangular fibrocar-triage complex of the wrist: anatomy and function. J HANDStJRG 1981;6:153).
the dorsal and palmar radioulnar ligaments. These, inturn, are further strengthened and their fibers orientedto insert into the ulnar head at the ulnar styloid base,~!-:~: lunate as the ulnolunate ligament, the triquetrum as~i~e uinotriquetral ligament, and the hamate and base ofthe fifth metacarpal as th~ ulnocollateral ligament( Fig. 2). When the wrist is viewed externally, the TFCCappears as a homogeneous ligamentous structure withdiffuse attachments to the radius, ulna, and ulnocarpalbones. The individual components of the complex,when recognizable, are best seen with internal inspec-tion of the wrist, either with an arthrotomy or throughtt~e arthroscope.
Fhe horizontal portion of the TFCC is not normallyperforated. Mikic,~ in a now classic study, evaluatedthe TFCC of 180 cadaver wrists ranging in age frompremature infants to 97 years. There was no evidence
Fig. 2. Dorsal exposure of a cadaver wrist .with the wristacutely flexed showing the triangular fibrocartilage (TFC)arising from the radius and flowing ulnarly and distally. Othercomponents of the triangular fibrocartilage complex picturedare the dorsal radial-ulnar ligaments (~), the palmarradial-ulnar ligament (~ ~), the ulnolunate ligament (ULL),and the ulnotriquetral ligament (UTL). S, Scaphoid~ L, lunate;T, triquetrum. .
of degenerative change of any part of the disc in fetuses,the first or second decade. He found no perforationsbefore the age of 30. He further noted a relative linearprogression of perforations with age so that over theage of 50, all specimens showed degenerative Changes,many with a perforation of the horizontal portion of theTFCC. -.
Biomechanical review ..~ :
~The TFCC has been shown to have three major func-tions: (1) it functions as a cushion for the ulnar carpus,carrying approximately 20% of the axial load of theforearm in a cadaver specimen; (2) it is the major sta-bilizer of the distal radioulnar joint, and (3) it is stabiliizer of the ulnar carpus.*
Variable loads are borne on the ulnar aspect of thewrist by the TFCC as the forearm moves thro~ugh pro-nation and supination.9’ ~0, 35, a~, 49, ~3-~6 Supinati0n resultsin a relative negative ulnar variance and pronation, amore relative positive ulnar variance), 57-6o Thesechanges in ulnar variance result in relatively small butpotentially significant changes in load borne by selectedportions of the TFCC as the ulnar head becomes un-
*Refe~rences 1, 2, 9, i0, 41, 42, 53, 54
596 Palmer
The JournalHAND
2
Table I. TFCC abnormalities
Class 1: TraumaticA Central perforationB Ulnar avulsion
With distal ulnar fractureWithout distal ulnar fracture
C Distal avulsionD Radial avulsion
With sigmoid notch fractureWithout sigmoid notch fracture
Class 2: Degenerative (ulnocarpal abutment syndrome)Stage:A TFCC wear ". ¯B TFCC wear .~!+ Lunate and/or ulnar chondromalaciaC TFCC perforation ̄
+ Lunate and/or ulnar chondromalaciaD TFCC perforation
+ Lunate and/or ulnar chondromalacia+ L-T ligament perforation
E TFCC perforation+ Lunate and/or ulnar chondromalacia+ L-T ligament perforation ..+ Ulnocarpal arthritis
A classification of triangular fibrocartilage complex injuries¯
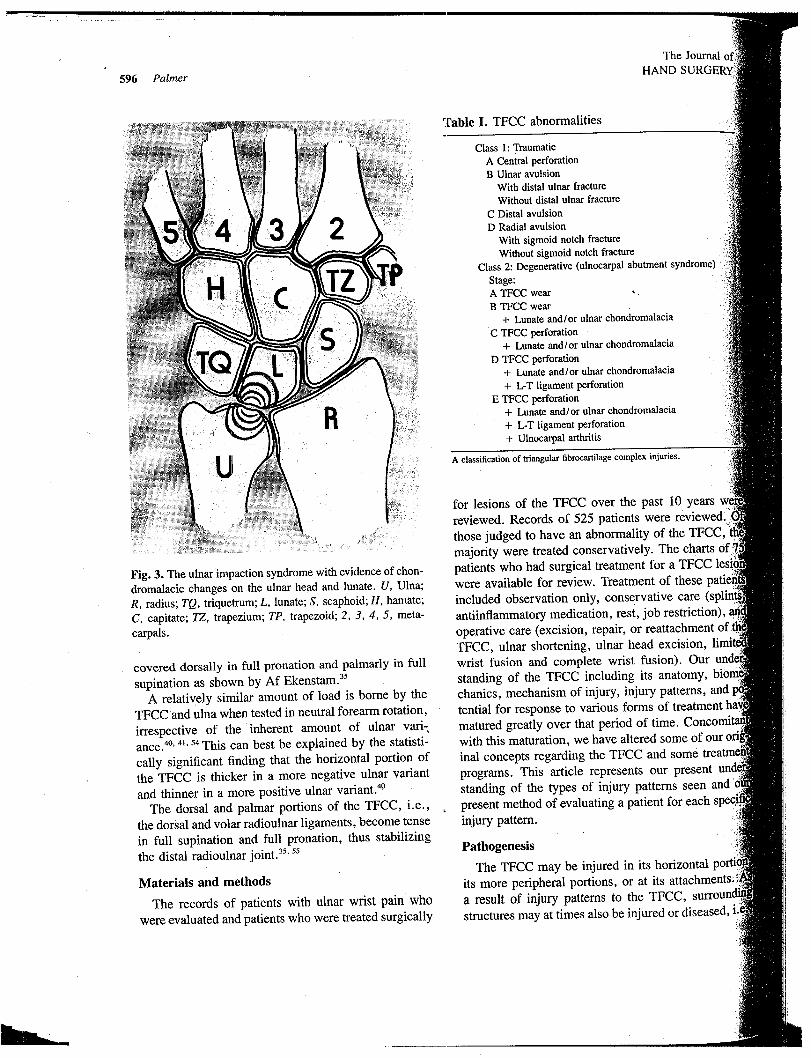
Fig. 3. The ulnar impaction syndrome with evidence of chon-dromalacic changes on the ulnar head and lunate. U, Ulna;R, radius; TQ, triquetrum; L, lunate; S, scaphoid; H, hatnate;C, capitate; TZ, trapezium; TP, trapezoid; 2, 3, 4, 5, meta-carpals.
covered dorsally in full pronation and palmarly in fullsupination as shown by Af Ekenstam.35
A relatix~ely similar amount of load is borne by theTFCC and ulna when tested in neutral forearm rotation,irrespective of the inherent amount of ulnar vari-,ance.4O. 4~. 54 This can best be explained by the statisti-cally significant finding that the horizontal portion of
¯ the TFCC is thicker in a more negative ulnar variantand thinner in a more positive ulnar variant.~°
The dorsal and palmar portions of the TFCC,. i.e.,the dorsal and volar radioulnar ligaments, become tensein full supination and full pronation, thus stabilizingthe distal radioulnar joint.3~" 5s
Materials and methods
The records of patients with ulnar wrist pain̄ whowere evaluated and patients who were treated surgically
for lesions of the TFCC over the past 10 yearsreviewed. Records of 525 patients werethose judged to have an abnormality of the TFCCmajority were treated conservatively. The charts ofpatients who had surgical treatment for a TFCCwere available for review. Treatment of theseincluded observation only, conservative careantiinflammatory medication, rest, joboperative care (excision, repair, or reattachment of TFCC, ulnar shortening, ulnar head excision,wrist fusion and complete wrist fusion). Ourstanding of the TFCC including its anatomy,chanics, mechanism of injury, injury patterns, andtential for response to various forms of tmatured greatly over that period of time.with this maturation, we have altered someinal concepts regarding the TFCC and someprograms. This article represents our presentstanding of the types of injury patterns seen andpresent method of evaluating ainjury pattern. ¯ ~
Pathogenesis
The TFCC may be injured in its horizontal
its more peripheral portions, or at its attachments.a result of injury patterns to the TFCC,structures may at times also be injured or diseased, i.
¯ Voi. |4A, No. 4July 19~9 Classification of TFCC lesions 597
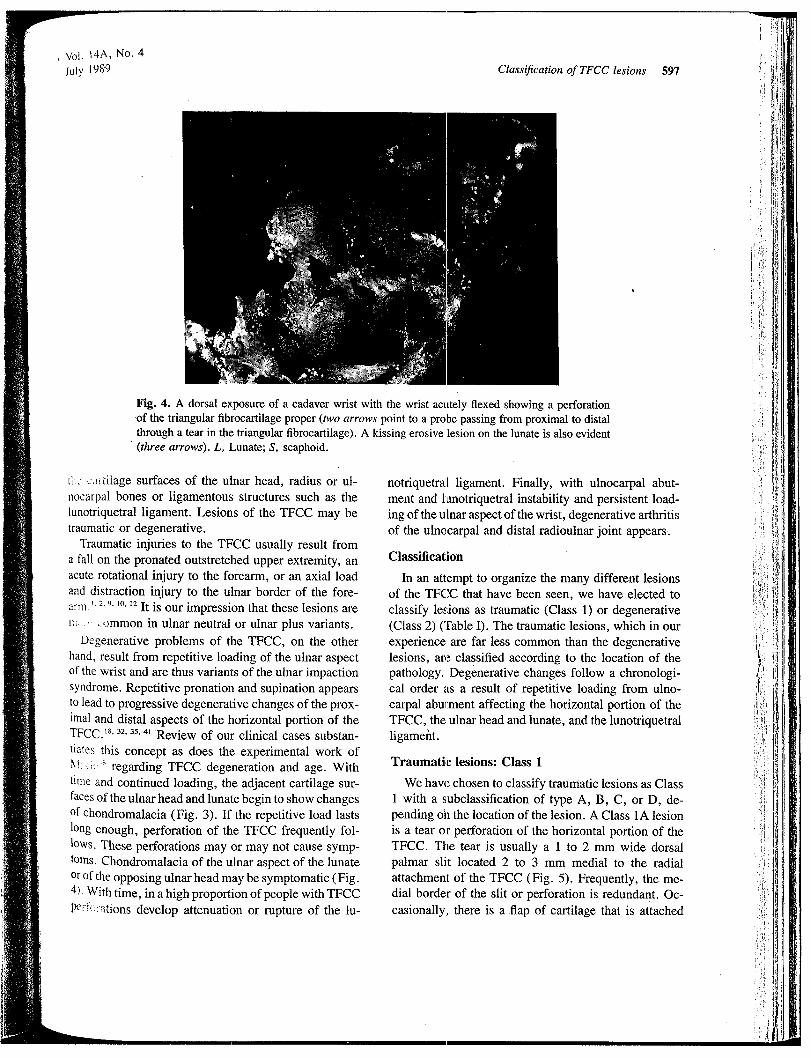
Fig. 4. A dorsal exposure of a cadaver wrist with the wrist acutely flexed showing a perforation.of the triangular fibrocartilage proper (two arrows point to a probe passing from proximal to distalthrough a tear in the triangular fibrocartilage). A kissing erosive lesion on the lunate is also evident(three arrows). L, Lunate; S, scaphoid.
ti:.’ c:~,.-tilage surfaces of the ulnar head, radius or ul-nocarpal bones or ligamentous structures such as thelunotriquetral ligament. Lesions of the TFCC may betraumatic or degenerative.
Traumatic injuries to the TFCC usually result froma fall on the pronated outstretched upper extremity, anacute rotational injury to the forearm, or an axial loadand distraction injury to the ulnar border of the fore-arm." ~-’ 9, 10. t2 It is our impression that these lesions aren~ .. common in ulnar neutral or ulnar plus variants.
Degenerative problems of the TFCC, on the otherhand, result from repetitive loading of the ulnar aspectof the wrist and are thus variants of the ulnar impactionsyndrome. Repetitive pronation and supination appearsto lead to progressive degenerative changes of the prox-imal and distal aspects of the horizontal portion of theTFCC.18.32. 35, 41 Review of our clinical cases substan-
tiates this concept as does the experimental work of~! i~i’. ~ regarding TFCC degeneration and age. Withtime and continued loading, the adjacent cartilage sur-faces of the ulnar head and lunate begin to show changesof chondromalacia (Fig. 3). If the repetitive load lastslong enough, perforation of the TFCC frequently fol-lows. These perforations may or may not cause symp-toms. Chondromalacia of the ulnar aspect of the lunateor of the opposing ulnar head may be symptomatic (Fig.4). With time, in a high proportion of people with TFCC
P~erf,:::ations develop attenuation or rupture of the lu-
notriquetral ligament. Finally, with ulnocarpal abut-ment and lanotriquetral instability and persistent load-ing of the ulnar aspect of the wrist, degenerative arthritisof the uln~carpal and distal radioulnar joint appears.
Classification
In an attempt to organize the many different lesionsof the TFCC that have been seen, we have elected toclassify lesions as traumatic (Class 1) or degenerative(Class 2) (’fable I). The traumatic lesions, which in experience are far less common than the degenerativelesions, are classified according to the location of thepathology. Degenerative changes follow a chronologi-cal order as a result of repetitive loading from ulno-carpal abu~ment affecting the horizontal portion of theTFCC, the ulnar head and lunate, and the lunotriquetralligamefit.
Traumatic lesions: Class 1
We haw~ chosen to classify traumatic lesions as Class1 with a subclassification of type A, B, C, or D, de-pending oh the location of the lesion. A Class 1A lesionis a tear or perforation of the horizontal portion of theTFCC. The tear is usually a 1 to 2 mm wide dorsalpalmar slit located 2 to 3 mm medial to the radialattachment of the TFCC (Fig. 5). Frequently, the me-dial border of the slit or perforation is redundant. Oc-casionally, there is a .flap of cartilage that is attached

598 Palmer
The J~HAND
Fig. 5.-The ligamentous supports of the ulnar aspect of thewrist (the triangular fibrocartilage complex) illustrating Class 1A perforation. The perforation is a dorsal palmar tear(arrow) just medial to the radial origin of the TFCC. R,Radius; U, ulna; L, lunate; T, triquetrum.
only at the palmar aspect of the slit. A triple injectionwrist arthrogram using either a radiocarpal or distalradioulnar joint injection technique performed on sucha wrist will reveal a perforation of the TFCC near itsattachment to the radius (Fig. 6). 34, 46, 61-66
Class 1B lesions represent traumatic avulsions of theTFCC from its insertion into the distal ulna (Figs.7, A and B). These may or may not be accompaniedby a fracture of the ulnar styloid at its base. As theTFCC represents the major stabilizer of the distal ra-dioulnar joint, these lesions are usually associated withdistal radioulnar joint instability. An arthrogram per-formed on such a wrist will reveal no abnormality witha radiocarpal injection. An arthrogram done on such awrist via a distal radioulnar joint injection may revealdye leakage out ulnarly from beneath the TFCC(Fig. 8).
Class 1C lesions represent tears of the TFCC in itsperiphery, i.e., avulsion of the TFCC from its distalattachment to the lunate (the ulnolunate ligament) the triquetrum (the ulnotriquetral ligament) (Fig. As the TFCC is a major stabilizer of the ulnar carpus,these lesions frequently result in ulnar carpal instabilitymanifested by palmar translocation of the ulnar carpusin reference to the radius and/or ulnar head. An ar-throgram done on such a wrist will show no perforationof the horizontal portion of the TFCC but may verypossibly reveal a capsular leak with either a radiocarpal
Fig. 6. A, The PA radi ~ograph of a wrist with a 0.5 mm~ulnar variance and B, an arthrogram ofta perforation between the radiocarpal and distaljoints after a radiocarpal injection of contrast media
or midcarpal injection, depending on’thethe tear (Fig. 10).
Class 1D lesions are traumatic avulsfrom its attachment to the radius at the distalthe sigmoid notch (Fig. 1 1). wrist can be expected to show a~ween the radiocarpal and distal radioulnar joint ~itocation of the TFCC disruption with ~,or distal radioulnar injection, unlessload at time of the study obscures the
Degenerative lesions: Class 2 ~i
Degenerative lesions of the TFCC are, as hasviously been mentioned, a result of chronic loadulnar wrist, i.e., the ulnar impaction3). We have chosen to categorize these lesionsB, C, D, or E, depending on the extent andof degenerative changes present.

V~I. 14A, No. 4July 1989 Classification of TFCC lesions 599
ClasFig. 7. A, The ligamentous supports of the ulnar aspect of the wrist (the triangular fibrocartilagecomplex) illustrating a Class 1B lesion. In this instance, the TFCC is avulsed from the distal ulnawith an associated fragment of bone, i.e., the distal ulna. R, Radius; U, ulna; L, lunate; T, triquetrum.B,.The ligamentous supports of the ulnar aspect of the wrist (the triangular fibrocartilage complex)illustrating a Class 1B lesion. In this case, the triangular fibrocartilage complex is torn free fromthe base of the ulnar styloid without an associated fracture (arrow). R, Radius; U, ulna; L, lunate;T, triquetrum.
Ciass 2A represents wear of the horizontal portionof the TFCC distally, proximally, or both, without per-foration (Fig. 12). Mikic38 elegantly describes this formof TFCC abnormality anatomically and histologically.The neutral forearm rotation PA x-ray films of such awrist will usually, as with all Class 2 lesions, reveal aneutral or positive ulnar variant.57’ 58, ~o The arthrogramin such a case is usually normal. However, with careful
s~:r~.~tiny one may see raggedness of the horizontal por-tiov. of the TFCC on its proximal aspect with a distal
radioulnar joint injection or on its distal aspect with aradic,carpal injection (Fig. 13). The pathology, as witha Cl~tss 2B lesion, can best been seen with arthroscopyand ].ess easily with an arthrotomy.4~’ 67.68
Class 2B lesions represent wear of the horizontalportion of the TFCC and additional wear or chondro-malacia of the ulnar aspect of the lunate or the radialaspect of the ulnar head or both (Fig. 14). Again, theneut~:al forearm rotation PA x-ray film of such a wristwill usually show an ulnar neutral or positive variant.

600 Palmer
TheHAND
Fig. 8. (Left) PA x-ray film of a wrist after trauma with a small avulsed fragment of bone adjacentto the ulnar styloid (arrow). (Center) A radiocarpal injection arthrogram showing a midcarpalcommunication but no abnormality of the TFCC. (.Right) A distal radioulnar joint injection showinga tear of the TFCC from its insertion onto the dii;tal ulnar allowing contrast leakage out into the
ulnar soft tissues (arrows).
Clas¯ Fig. 9. The ligamentous supports of the ulnar aspect of thewrist (the triangular fibrocartilage complex) illustrating Class 1C lesion. The triangular fibrocartilage complex isavulsed distally from its bony insertion to the lunate by theulnolunate ligament and/or the triquetrum by the ulnotrique-tral ligament (arrows). R, Radius; U, ulna; L, lunate; T;triquetrum.
Occasionally, subchondral erosive changes of the lunateor ulnar head may be seen (Fig. 15). The arthrogramis usually normal except for subtle changes on the hor-
izontal portion of the TFCC.Class 2C lesions represent further progression or de-
generative change to the point that the horizontal por-tion of the TFCC becomes perforated (Fig. 16). This
perforation tends to be ovoid, whereas a traumatic per-foration tends to be a dorsal.palmar slit. Degenerativeperforations are located in the thin avascular portion of
the TFCC, i.e., ulnar to the location of aperforation. Wrist arthrograms with eitheror distal radioulnar joint injections usuallya perforation of the horizontal portion ofconfirms the anatomic location and shape offora~ion as just described (Fig. 17).
Class 2D lesions represent even further
of the degenerative process where there isdegenerative changes of the articularnate and ulnar head, the horizontal portion
is perforated, and the lunotriquetral ligamentrupted (Fig. 18). We postulate that chronicthe ulnar aspect of the lunate leads to
and eventual attenuation of the interosseousthe lunotriquetral ligament. An arthrogram ofwrist with a midcarpal, radiocarpal, or C
.joi~nt injection will usually show the TFCCand lunotriquetral ligament disruption (Fig. 19).
Class 2E lesions represent theimpaction syndrome, i.e., degenerativeultnocarpal and occasionallY, distal radioulnarthese cases, the horizontal portion of the TFCCally completely absent and the lunotriquetralseous ligament is completely disrupted.
Discussion
’ We believe that classification of lesions of theis helpful as a plethora of TFCC problemsbeen seen, the pathogenesis of thesenized, and the treatment for each frequently
dividualization. Differentiation ofhas been difficult in the past. A careful
amination including palpation for locderness, stress testing for. detection

Vol. I4A, No. 4July 1989 Classification of TFCC lesions 601
Fig. 10. A-B. A, A radiocarpal injection arthrogram showing dye leakage out ulnarly (two arrows)and B, palmarly (one arrow).
T
Class 1D V / I ClassFig. 11. The ligamentous supports.of the ulnar aspect of thewrist (the triangular fibrocartilage complex) illustrating Class 1D lesion. Arrows indicate an avulsion of the TFCCfrom its radial origin. The avulsion can be with or without afragment of bone. R, Radius; U, ulna; L, lunate; T, tri-quetmm.
Fig. 12. The ligamentous supports of the ulnar aspect of thewrist (the triangular fibrocartilage complex) illustrating Class 2A lesion. Both the proximal and distal aspects of theTFCC histologically and at times, grossly, evidence degen7erative changes as illustrated by the stippling on this illustra-tion (arrow). R, Radius; U, ulna; L, lunate; T, triquetrum.
~’5:~tal radioulnar joint instability, and observation forswelling or deformity are frequently helpful in local-izing the lesion; The presence or absence of an avulsionfracture or positive ulnar variance as determined byneutral forearm rotation PA x-ray films are helpful inclassifying lesions. Arthrographic studies, until late,have been used to demonstrate a "tear" of the TFCC.It is now recognized, however, that triple injection ar-thrography of the wrist, including injections into thera,~.ii,.~carpal, distal radioulnar, and midcarpal joints al-lows better delineation of the complex abnormalities of
the TFCC and by localization of the tear, differentiationbetween a traumatic tear and the degenerative perfo-ration, An injection into the radiocarpal joint may reveala perfi3ration through the central portion of the TFCC,peripheral partial tears of the TFCC, peripheral disrup-tions of the TFCC, and in a high percentage of patientswith a perforated horizontal portion of the TFCC, leak-age of dye across the lunotriquetral perforation, indi-cating: a lunotriquetral ligament abnormality.61 Dye in-jection into the distal radioulnar joint can reveal a per-foration of the horizontal portion of the TFCC, tears of

602 PalmerThe Journal
HAND SU
L
R
Fig. 13. A distal radial-ulnar joint injection arthrogram witha partial tear of the TFCC (arrow po!nting to a tear of theproximal aspect of the TFCC).
the peripheral aspect of the TFCC (either partial ortotal), and complete disruption of the TFCC from thedistal ulna. ̄
Recently, Roth and Haddada6 showed that wrist ar-throscopy is more accurate in evaluating perforationsof the TFCC than is arthrography. In this well-controlled study, arthrograms were done with a singlecompartment injection. Perhaps with the triple injectiontechnique, more accurate information could have beengained.62. 66 Arthroscopy is, in some hands, replacingarthrography for the evaluation of chronic ulnar wristpain, for arthroscopy allows one to evaluate the sizeand shape of a TFCC perforation, the presence or ab-sence of chondromalacial changes on the carpal bonesand/or ulnar head, and the integrity and strength of theintrinsic wrist ligaments,u" 68 Of most importance, how-ever, a torn TFCC can be debrided or an area of chon-dromalacia abraded at the time of the arthroscopy.
The association between ulnar variance, as obtainedin a neutral forearm rotation film and TFCC abnor-malities is now well-recognized.1’ 2, 9-12 Positive andneutral ulnar variance is more commonly associated’with abnormalities of the TFCC. It is uncommon to seean individual with a TFCC abnormality with negative "ulnar variance. We believe that positive ulnar varianceis an etiologic factor in the production of Class 2 lesionsof the TFCC and ulnocarpal complex.
The classification of TFCC lesions presented here isbased on our anatomical dissection, biomechanicalstudies, review of the work of others who have studiedTFCC problems, and review of the patients we haveseen and treated with these lesions for more than 10
U
Class 2BFig. 14. The ligamentous supports of the ulnar aspectwrist (the triangular fibrocartilage complex)Class 2B lesion. In addition to the degenerativethe TFCC seen in a Class 2A lesion (stippling),erosion of the ulnar head beneath the TFCC is seenor of the kissing area of the medial border of the lunateto the TFCC (arrow). R, Radius; U, ulna; L, lunate;quetrum.
years. During that period of time, many treatmentgrams have been tried for different TFCC lesions.have learned to never excise the TFCC completely.TFCC is not the appendix of the wrist joint. Wediscarded some procedures that we originallywould be successful in the treatment of problemsTFCC such as repair of tears of the horizontalof the complex. The treatment program that weently use has been in place for the past 2 yearsappears to offer promise. As our classificationnine different lesions, almost all patients areconservatively originally and the operativefor each lesion varies depending on theamination, plain films, arthrographic studies, anderative findings; large groups of patients inment group are not presently available for lonfollow-up. Many TFCC lesions respond totire measures and never come to surgicaltion.!" 2, 9-12 Traumatic tears of the horizontalthe TFCC that do not respondbest treated with limited TFCC debridement,words, enlargement of the size of theTFCC avulsions or midsubstance tears,
*References 7, 24, 25, 27-29, 31-33, 44, 45, 68, 69

Vol. 14A, No. 4July 1989 Classification of TFCC lesions 603
Fig. 15. (Left) PA radiograph of a wrist with subchondral bony erosion of the lunate as a result ofan ulnar impaction syndrome (arrow). (Right) A radiocmpal injection arthrogram of the same patientevidencing a tear of the distal aspect of the horizontal p~rtion of the TFCC (arrow) without throughand through perforation and dye leakage into the distal radioulnar joint.
Class 2CFig. 16. The ligamentous supports of the ulnar aspect of the~r’.~ ,~he triangular fibrocartilage complex) illustrating Ch~.~ 2C lesion. Further progression of the Class 2 degen-erative lesions of the TFCC evidences now a large centralperforation of the TFC (proximal arrow), as well as the un-derlying cartilage abnormality of the ulnar head and distally,the medial aspect of the lunate. R, Radius; U, ulna; L, lunate;T. triquetrum.
either through positioning or immobilization or open
ret~:’.i’: followed by immobilization is recommended.9
Degenerative perforations that do not respond to con-servative measures are best treated with ulnar short-ening.~8. 29. 70 Associated lunotriquetral ligament insta-bility is treated with ulnar shortening and rarely requires
addition of a limited intercarpal arthrodesis. Ulnocarpalarthritis, the final stage of degenerative perforation, istreated with a salvage procedure such as an ulnar head
resection. 7~ We have treated very few patients withCl.-.~s~; 1B, C and D lesions. Therefore, although the
Fig:. 17. PA arthrogram of the wrist after a radiocarpal injec-tion illustrating a large perforation of the TFCC with dye,communication between the radiocarpal and distal radioulnarjoints (arrows).
treatment plan outlined above for the treatment of dif-ferent TFCC lesions has, to date, given good results inour hands and parts of the treatment plan, good resultsin the hands of others, our recommendations for treat-ment must be viewed as preliminary.29, ,3, **
Summary
A classificationof traumatic and degenerative lesionsof the TFCC has been presented. The clinical, radio-

604 PalmerThe
HAND
Class 2D \Fig. 18. The ligamentous supports of the ulnar aspect ofthe wrist (the triangular fibrocartilage complex) illustrat-ing a Class 2D lesion. Further progression of the degenera-tive TFCC abnormalities reveals a through- and through-perforation of the horizontal portion of the TFC (proximalarrow), cartilage abnormalities of the ulnar head and of anadjacent area of the medial border of the lunate (distal radialarrow), and a disruption of the lunotriquetral ligament (distalulna arrow). R, Radius; U, ulna; L, lunate; T, triquetrum.
graphic, and arthrographic findings associated with eachlesion lias been specifically outlined. Our experience intreating patients with lesions of the TFCC, as well asthe accumulated knowledge of the last few years re-garding the anatomy, biomechanics and pathogenesisof TFCC lesions, has helped us develop this classifi-cation. It has also shown us the need for a classificationon which to base treatment for the myriad of lesionsthat are seen in patients with injuries to the TFCC.Patients do not suffer from "just a torn TFCC" but havea distinct lesion that is ciassifiable. It is our hope thatothers will; using this classification schema as a frame-work, be able to develop appropriate treatment pro-grams or test previously developed treatment programsfor the treatment of specific TFCC lesions. Patients withulnar wrist pain need no longer be considered the lowback pain of the wrist.
REFERENCES
1. Bowers WH. Problems of the distal radioulnar joint. In:Advances in orthopaedic surgery. Baltimore: Williams& Wilkins, 1984:289-303.
2. Bowers WH. The distal radioulnar joint. In Green DP,ed. Operative hand surgery. Vol II. New York: ChurchillLivingstone, 1988:939-89.
Fig. 19. A midcarpal injection arthrogram showingage from the midcarpal jperforation into the midcarpal joint (single arrow)from the radiocarpal joint through a TFCCthe distal radioulnar joint (two arrows).
3. Bunnell S. Surgery of the hand. 3rd ed.Lippincott, 1956.
4. Cone RO, Szabo R, Resnick D, et al.mography Of the normal radioulnar joints. Invest1983;18:541-5.
5. Dameron TB. Traumatic dislocation of the distalulnar joint. Clin Orthop 1972;83:55-63.
6. Destot E. Injuries of the wrist: a radiologiclated by FRB Atkinson. New York: Paul B.1926.
7. Geisl H, Spritzendorfer E. Der fib des discuslaris als ursache des posttraumatischenschmerzes. Unfallheilkunde 1984;84:55-9.
8. Mino DE, Palmer AK, Levinsohn EM. Thediography and computerized tomography insubluxation and dislocation of the distal radioulnarJ HAND Surt6 1983;8:23-31.
9. Palmer AK. The distal radioulnar joint. In:DM, ed. The wrist and its disorders. Philadelphia:Saunders, 1988:220-31.
10. Palmer AK. The distal radioulnar joint. In:ed. Hand clinics--management of wrist problems.adelphia: WB Saunders, 1987:31-40.
11. Palmer AK. The distal radioulnar joint. OrthopNorth Am 1984;15:321-35.
12. Palmer AK. Symposium on distal ulnar injuries.temp Orthop 1983;7:81.
13. Albert WM, Wohl MA, Reihtman AM. Treatment ofi

V~I. 14A, No. 4July 1989
disrupted radioulnar joint. J Bone Surg 1963;45A: 1373-81.
14. Bell MJ, Hill RJ, McMurty RY. Ulnar impingement syn-drome.. J Bone Joint Surg 1985;67B:126-9.
15.~’hun S, Palmer AK. Chronic ulnar wrist pain secondaryto partial rupture of the extensor carpi ulnaris tendon.J HAND St~RG 1987;12A:1032-5.
16. Darrach N. Arterior dislocation of the head of the ulna.Ann Surg 1912;56:802-3.
17. Darrach W. Partial excision of lower shaft of ulna fordeformity following Colles’ fracture. Ann Surg 1913;57:764-5.
18. Darrow JC, Linscheid RL, Dobyns JH, Mann JM, WoodMB, Beckenbaugh RD. Distal ulnar recession for dis-:~.rders of the distal radioulnar joint. J HAND SURG! 985; 10A:482-91.
19. Eckhardt WA, Palmer AK. Recurrent dislocation of theextensor carpi ulnaris tendon. J HAND StJRG 1981 ;6:629-31.
20. Goncalves D. Correction of disorders of the distal radio-ulnar joint by artificial pseudarthrosis of the ulna. J BoneJoint Surg 1974;56B:462-4.
21. Hagert CG. Functional aspects on the distal radio-ulnarioint. J HAND SURG 1979;4:585.
2. : ~nner M, Kaplan EB. Extensor carpi ulnaris. Its re-lationship to stability of the distal radioulnar joint. ClinOrthop 1970;68:124-9.
23. Coleman HM. Injuries of the articular disc at the wrist.J Bone Joint Surg 1960;42B:522-9.
24. Imbriglia JE, Boland DS. Tears of the articular disc ofthe triangular fibrocartilage complex and results of ex-cision of the articular disc [Abstract]. J HAND SURG1983;8:620.
25. Martinek H. Zur traumatologie des discus triangulafis.:"~rch Orthop 1977;87:285-97.
2~. Mohanti RC, Kar N. Study of triangular fibrocartilageof the wrist joint in Colles’ fracture. Br J Ace Surg1979;11:321-4.
27. Mossing N. Isolated lesions of the radio-ulnar disk treatedwith excision. Scand J Plast Reeonstr Surg 1975;9:231-3.
28. Neviaser RJ, Palmer AK. Traumatic perforation of thea~ticular disc of the triangular fibrocartilage complex ofthe wrist. Bull Hosp J Dis Orthop Inst 1984;44:376.
?"~ i~terman AL, Bora FW, Martin E. Arthroscopic excisionof flap tears of the triangular fibroeartilage. Presented atthe 42nd Annual Meeting of the ASSH. San Antonio,Texas: September 1987.
30. Redler I. Meniscoid of the wrist. Clin Orthop 1972;88:138-41.
31. van der Linden AJ. Disk lesion of the wrist joint. J HAND
StJRG 1986;11A:490-7.32. Weigl K, Spira E. The triangular fibrocartilage of the
wrist joint. Reconstr Surg Traumatol 1969;11:139-53.? 3. ?’-~enon J, Wood VE, Schoene HR, Frykman GK, Hohl
Classification of TFCC lesions 605
JC, Bestard EA. Isolated tears of the triangular fibro-cartilage of the wrist: results of partial excision. J HANDSt~RG 1984;9A:527-30.
34. Blair WF, Berger RA, El-Khoury GY. Arthrotomographyof the wrist: an experimental and preliminary, clinicalstody. J HAND SVR6 1985;10A:350-9.
35. Af Ekenstam F. The distal radioulnarjoint--an anatom-ical, experimental, and clinical study [Dissertion]. Upp-sala: Acta Univ Abstr Uppsala, 1984;505:1-55.
36. ~,wis OJ. Evolutionary change in the palmate wrist andinferior radio-ulnar joints. Anat Ree 1965;151:275-85.
37. I~=wis OJ. The hominoid wrist joint. Am J Phys An-thropol 1969;30:251-67.
38. I~iikic ZD. Age changes in the triangular fibroeartilageof the wrist joint. J Anat 1978;126:367-84.
39. l~[ohiuddin A, Janjua MZ. Form and function of radioul-nar articular disc. Hand 1982;14:61-6.
40. Palmer AK, Glisson RR, Werner FW. Relationship be-tween ulnar variance and triangular fibrocartilage com-plex thickness. J HAND SOR~ 1984;9A:681-3.
41. Palmer AK, Werner FW. Biomechanics of the distal ra-diioulnar joint. Clin Orthop 1984;187:26-34.
42. Palmer AK, Werner FW. The triangular fibrocartilagecomplex of the wrist--anatomy and function. J HANDSUR6 1981;6:153-62.
43. Poehling GG, Koman LA, Whipple TL, Roth JH, Kam-mire G. Diagnosis and management of articular cartilagele.sions of the wrist. Presented at the 42nd Annual Meet-ing of the ASSH. San Antonio, Texas, September 1987.
44. R~oth JH. A review of my first 150 cases of wrist arthros-copy. Wrist Investigators Workshop. Orlando, Florida,November 1987.
45. l~’,oth JH. Wrist arthroscopy. In: Lichtman DM, ed. Thewrist and its disorders. Philadelphia: WB Saunders,1988:220-31.
46. Roth JH, Haddad RG. A comparison of arthrography andarthroscopy in the diagnosis of chronic ulnar wrist pain.Presented at the 41st Annual Meeting of the ASSH.New Orleans, Louisiana, February 1986.
47. Johnson RK. Muscle-tendon transfer for stabilization ofthe distal radioulnar joint. J HAND SURG 1985;10A:437.
48. Johnson RK, Shrewsbury MM. The pronator quadratusin motions and in stabilization of the radius and ulna atthe distal radioulnar joint. J HAND SUR~ 1976;1:205-9.
49. Kauer JMG. The articular disc of the hand. Acta Anat]1975;93:590-605.
50. Kauer JMG. Functional anatomy of the wrist. Clin Or-thop 1980;149:9-20.
51. Taleisnik J. The ligaments of the wrist. J HAND SURG1976;1:110-18.
52. Thim-Pathi RG, Ferlic DC, Clayton ML, McClure DC.Arterial anatomy of the triangular fibrocartilage of thewrist and its surgical significance. J HAND SURG 1986;l 1A:258-63.
53. Werner FW, Glisson RR, Murphy D J, Palmer AK. Force

The Journal,606 Palmer HAND SURGE
transmission through the distal radioulnar carpal joint:effect of ulnar lengthening and shortening. Handchirurgie1986;18:304-8.
54. Ekenstam F, Palmer AK, Glisson RR. The load on the¯ radius and ulna in different position of the wrist and
forearm. Acta Ortho Scand 1984;55:363-5.55. Ekenstam FW, Hagert CG. Anatomical studies on the
geometry and stability of the distal radioulnar joint.Scand J Plast Reconstr Hand Surg 1985;19:17-25.
56. Kapandji IA. The inferior radioulnar joint and prono-supination. In: Tubiana R, ed. The Hand. Vol 1. Phila-delphia: WB Saunders, 1981:121-9.
57. Epner RA, Bowers WH, Guilford WB. Ulna variance:the effect of wrist positioning and roentgen filming tech-nique. J HAND SURG 1982;7:298-305.
58. Hardy DC, Totty WG, Reinas WR, Gilula LA. Postero-anterior wrist radiography: importance of arm position-ing. J HAND SURG 1987;12A:504-8.
59. Hulten O. Uber anatomische variationen der hand ge-lenknochen. Acta Radiol 1928;9:155-69.
60. Palmer AK,~ Glisson RR, Werner FW. Ulnar variancedetermination. J HAND SURG 1982;7:376.
61. Levinsohn EM, Palmer AK. Arthrography of the trau-matized wrist. Radiology 1983;146:647-51.
62. Levinsohn EM, Palmer AK, Coren AB, Zinberg E. Wristarthrography: the value of the three compartment injec-tion technique. Skeletal Radiology 1987;16:539-44.
63. Mikic ZD. Arthrography of the wrist joint. Anmental study. J Bone Joint Surg 1984;66A:371-8.
64. Palmer AK, Levinsohn EM, Kuzma GR.of the wrist. J HAND SURG 1983;8:15-23.
65. Reimas WR, Hardy DC, Totty WG, Gilula LA.scopic evaluation of the carpal triangularcomplex. J HAND StJRG 1987;12A:495-503.
66. Zinberg EM, Palmer AK, Coren AB, LevinsohnThe triple injection wrist arthrogram. J HA~D1988;13A:803-9.
67. Wehbe MA. Surgical approach to the ulnar wrist. JSURG 1986;11A:509-12.
68. Whipple TL. Clinical applicatiola of wristIn: Lichtman DM, ed. The wrist and its disorders.adelphia: WB Saunders, 1988:118-28.
69. Palmer AK, Werner FW, Glisson RRexcision of the triangular fibrocartilage complex:pefimental study. J HAND SURG 1988;13A:391-4.
70. Palmer AK. Wafer procedure. Presented at theRadioulnar Joint Course. Orlando, Florida,1987. ~i(
71. Bowers WH. Distal radioulnar jointhemiresection interposition technique. J. HAnD :~1985;10A:169-78.
Make researching easier with the Five-Year Cumulative Index (1984-1988) to THE JOURNALOF HAND SURGERY.
The Five-Year Cumulative Index is a complete guide to more than 5,000 pages of original articles,case reports, letters, and editorials published in Trn~ JOURNAL OF HAnD SUR6ER¥ from 1984 through1988 (volumes 9 to 13). The Cumulative Index, numbering approximately 150 pages, covers boththe American and the British volumes of the Journal. This hard-cover index includes both a subjectand an author index. Price, including shipping, i.s $42.00 U.S. ($45.00 international). Paymentmust accompany all orders and must be in U.S. funds, drawn on a U.S. bank.
Contact The C.V. Mosby Company, Circulation Department, 11830 Westline Industrial Drive,St. Louis, Missouri 63146-3318, U.S.A.; phone (314) 872-8370, ext. 394. In the U.S., call toll-free: 1-800-325-4177, ext. 394. Please allow six weeks for delivery.










![Well-founded practice or personal preference: a comparison ...sis of distal forearm fractures [5] and in diagnosis of condi-tions like ulnar impaction syndrome and triangular fibrocartilage](https://static.fdocuments.in/doc/165x107/5f1c1c8c4bf76178453659fa/well-founded-practice-or-personal-preference-a-comparison-sis-of-distal-forearm.jpg)







