Original Article Successful repair of delayed esophageal ... · Successful repair of delayed...
9
Int J Clin Exp Med 2016;9(6):9143-9151 www.ijcem.com /ISSN:1940-5901/IJCEM0016542 Original Article Successful repair of delayed esophageal perforation with sternocleidomastoid muscle flap after anterior cervical spinal surgery Beier Luo 1* , Jinghui Huang 2* , Huiren Tao 2* , Mo Li 2 , Xianming Pan 3 , Ming Li 1 , Zhuojing Luo 2 1 Department of Orthopaedics, Changhai Hospital, No. 168, Changhai Road, Yangpu District, Shanghai 200433, China; 2 Department of Orthopaedics, Xijing Hospital, The Fourth Military Medical University, Xi’an 710032, Shanxi, China; 3 Department of Orhopaedics, Chengdu Military General Hospital, Chengdu 610083, Sichuan, China. * Equal contributors. Received July 19, 2015; Accepted March 24, 2016; Epub June 15, 2016; Published June 30, 2016 Abstract: No consensus has been available to optimize the treatment of delayed esophageal perforation. The pres- ent study was to investigate the surgical treatment for delayed esophageal perforation with sternocleidomastoid muscle (SCM) flap after anterior cervical spine surgeries. The diagnosis and treatment of 5 esophageal perforations (May 2004 to January 2013) that occurred in a delayed fashion were retrospectively reviewed. The five patients re- ceived uniform repair surgery strategy. Cervical spine was accessed through the fistula tract. The esophageal lesion was recognized by the preoperatively swallowed methylene blue. A nasogastric tube was positioned through the rupture to help locate and assess the size and shape of the lesion. The esophageal lesion was primarily closed with interrupted sutures. The ipsilateral SCM was exposed, dissected at the distal end, elevated, medially rotated, and then interposed between the cervical vertebrae and the esophagus. The caudal free end of SCM flap was sutured to contralateral longuscolli muscle. Post-operatively, supportive treatments including adequate drainage, appropriate antibiotics and cessation swallowing were provided for at least 2 weeks to facilitate healing of esophageal perfora- tion. All esophageal perforation healed without further complications. In conclusion, surgical repair strategy includ- ing esophageal suture and a local SCM flap is capable of achieving satisfactory clinical outcome, especially in those with a large or chronic perforation. Keywords: Esophageal perforation, anterior cervical surgery, revision spinal surgery, sternocleidomastoid muscle flap, complications Introduction Anterior cervical spine surgery is one of the most commonly performed techniques for degenerative disc disease or trauma around the world. However, esophageal perforation is a rare yet challenging complication associated with anterior cervical spine surgery [1]. It has been reported that the incidence of esopha- geal perforation is around 0.02-1.14%, and its mortality was in 6~34% of cases and varies according to the patient’s general status, perfo- rating site, underlying comorbidities and the time duration from perforation to proper management. Esophageal perforation can be result of spine trauma or, in iatrogenic cases, induced by retractor, operations or by foreign bodies includ- ing surgical implants and bone graft [2-4]. Patients may present with only subtle physical findings and nonspecific complaints in the early stage, and diagnosis of esophagus perforation is therefore difficult to establish and lead to, as exemplified by many cases, delayed treatment. This could result in cervical abscess, mediasti- nitis, or life-threatening events like septic shock and death [5-8]. It has been reported that the mortality rate is around 50% in delayed esopha- geal perforation (after 24 h) in contrast to 20% in early diagnosed and treated cases (within 24 h) [9-11]. Early diagnosis and treatment has been the common belief to ensure good outcome for esophageal perforation [12]. However, due to
Transcript of Original Article Successful repair of delayed esophageal ... · Successful repair of delayed...

Int J Clin Exp Med 2016;9(6):9143-9151www.ijcem.com /ISSN:1940-5901/IJCEM0016542
Original ArticleSuccessful repair of delayed esophageal perforation with sternocleidomastoid muscle flap after anterior cervical spinal surgery
Beier Luo1*, Jinghui Huang2*, Huiren Tao2*, Mo Li2, Xianming Pan3, Ming Li1, Zhuojing Luo2
1Department of Orthopaedics, Changhai Hospital, No. 168, Changhai Road, Yangpu District, Shanghai 200433, China; 2Department of Orthopaedics, Xijing Hospital, The Fourth Military Medical University, Xi’an 710032, Shanxi, China; 3Department of Orhopaedics, Chengdu Military General Hospital, Chengdu 610083, Sichuan, China. *Equal contributors.
Received July 19, 2015; Accepted March 24, 2016; Epub June 15, 2016; Published June 30, 2016
Abstract: No consensus has been available to optimize the treatment of delayed esophageal perforation. The pres-ent study was to investigate the surgical treatment for delayed esophageal perforation with sternocleidomastoid muscle (SCM) flap after anterior cervical spine surgeries. The diagnosis and treatment of 5 esophageal perforations (May 2004 to January 2013) that occurred in a delayed fashion were retrospectively reviewed. The five patients re-ceived uniform repair surgery strategy. Cervical spine was accessed through the fistula tract. The esophageal lesion was recognized by the preoperatively swallowed methylene blue. A nasogastric tube was positioned through the rupture to help locate and assess the size and shape of the lesion. The esophageal lesion was primarily closed with interrupted sutures. The ipsilateral SCM was exposed, dissected at the distal end, elevated, medially rotated, and then interposed between the cervical vertebrae and the esophagus. The caudal free end of SCM flap was sutured to contralateral longuscolli muscle. Post-operatively, supportive treatments including adequate drainage, appropriate antibiotics and cessation swallowing were provided for at least 2 weeks to facilitate healing of esophageal perfora-tion. All esophageal perforation healed without further complications. In conclusion, surgical repair strategy includ-ing esophageal suture and a local SCM flap is capable of achieving satisfactory clinical outcome, especially in those with a large or chronic perforation.
Keywords: Esophageal perforation, anterior cervical surgery, revision spinal surgery, sternocleidomastoid muscle flap, complications
Introduction
Anterior cervical spine surgery is one of the most commonly performed techniques for degenerative disc disease or trauma around the world. However, esophageal perforation is a rare yet challenging complication associated with anterior cervical spine surgery [1]. It has been reported that the incidence of esopha-geal perforation is around 0.02-1.14%, and its mortality was in 6~34% of cases and varies according to the patient’s general status, perfo-rating site, underlying comorbidities and the time duration from perforation to proper management.
Esophageal perforation can be result of spine trauma or, in iatrogenic cases, induced by
retractor, operations or by foreign bodies includ-ing surgical implants and bone graft [2-4]. Patients may present with only subtle physical findings and nonspecific complaints in the early stage, and diagnosis of esophagus perforation is therefore difficult to establish and lead to, as exemplified by many cases, delayed treatment. This could result in cervical abscess, mediasti-nitis, or life-threatening events like septic shock and death [5-8]. It has been reported that the mortality rate is around 50% in delayed esopha-geal perforation (after 24 h) in contrast to 20% in early diagnosed and treated cases (within 24 h) [9-11].
Early diagnosis and treatment has been the common belief to ensure good outcome for esophageal perforation [12]. However, due to

Muscle flap for esophageal perforation
9144 Int J Clin Exp Med 2016;9(6):9143-9151
Table 1. General information of patients
No. Gender Age (year)
Primary pathology Primary surgery Fixation
failure Clinical presentation Time to 1st repair surgery
Strategy for esophageal repair
Repair surgery times
Time to recovery
1 Female 20 Trauma C5 corpectomy C4-C6 ACDF No neck swelling with palpable mass, difficult breathing, wound dehiscence and alimentary fluid leakage
14 months Removal of implant; esophageal repair; SCM flap
1 3 weeks
2 Female 28 Trauma C5/C6 ACDF No fever, neck pain, local abscess, wound dehiscence with mucopurulent discharge and alimentary fluid.
3 months Removal of implant; esophageal repair; SCM flap
2 8 months
3 Male 61 Myelopathy C5, C6 corpectomy; C4-C7 fixation with titanium mesh
No fever, wound dehiscence, dysphagia, alimentary fluid leakage, purulent secretion; neck swelling
6 days Removal of implant; esophageal repair; SCM flap
2 9 months
4 Female 57 Myelopathy C5 corpectomy; C4-C6 fixation with titanium mesh
No fever, neck pain, wound dehiscence, difficulty breathing, mucopurulent discharge
1 month Removal of implant; esophageal repair; SCM flap
1 2 months
5 Male 41 Trauma C3/C4 ACDF No fever, wound dehiscence, alimentary fluid leakage; dysphagia, neck swelling
3 months Removal of implant; esophageal repair; SCM flap
1 3 months

Muscle flap for esophageal perforation
9145 Int J Clin Exp Med 2016;9(6):9143-9151
the variable and nonspecific clinical presenta-tions, early identification of esophageal perfo-ration is difficult, which usually lead to delayed diagnosis and treatment. For those with delayed esophageal perforation, no consensus has been available to optimize their treatment. In the present study, we described the diagno-sis and management of 5 patients with large chronic esophageal perforation that occurred in a delayed fashion after cervical spine sur-gery, aiming to provide information for improv-ing clinical outcome of delayed esophageal perforation.
Methods and results
From May 5th 2004 to January 16th 2013, five patients (2 male and 3 females) who had received anterior cervical spine surgery by our team (2 of 5 cases) or other centers (3 of 5 cases) were treated in our department for delayed esophagus perforations. We retrospec-tively reviewed the medical records and imag-ing of the 5 patients. Clinical characteristics and conditions of all 5 patients were assessed and summarized in Table 1.
The surgical revision focused mainly on esoph-agus repair techniques, which was illustrated in
Figure 1. In brief, the procedure of repair begins with an incision along the anterior border of the SCM muscle on the side of the lesion. The supraomohyoid muscle and the middle thyroid vein were dissected. Thyroid gland and the carotid sheath were retracted to both sides for better exposure of the perforation lesion. Methylene blue was injected via nasogastric tube to identify the location and morphology of the perforation (Figure 1A). Plate, mesh, cage, screws or any implants could be removed depending on the specific case. After debride-ment of granulation tissue and repeated rinsing with metronidazole solution, the perforation was sutured with absorbable interrupted stitch-es (Figure 1B). Since complete closure of the perforation might be compromised in delayed cases where edema or chronic inflammation was present on the esophagus wall, a SCM flap was used to promote the healing of esophageal lesion.
The entire lateral and medial surface of the SCM muscle was exposed. The SCM muscle was incised at the distal sternal end while pre-serving the accessory nerve, forming a free end to the caudal direction and a pedicle to the cephalic direction. The SCM muscle flap was
Figure 1. Repair procedures for esophageal perforation. A. Cervical spine was accessed through the fistula tract. The esophageal lesion was recognized by the preoperatively swallowed Methylene blue and then further explored. A nasogastric tube could be positioned through the rupture to help locating and assessing the size and shape of the lesion. B. After debridement of granulation tissue and repeated rinsing of the wound, the esophageal lesion was primarily closed with interrupted sutures. C. The ipsilateral sternocleidomastoid muscle was exposed, dissected and incised according to the location and size of the lesion. The pedicled SCM flap was then elevated and tract toward the esophageal defect. D. The elevated SCM flap was interposed between the cervical vertebrae and the esopha-gus, and then sutured with contralateral longuscolli muscle. Suture of the esophageal wall was therefore reinforced.

Muscle flap for esophageal perforation
9146 Int J Clin Exp Med 2016;9(6):9143-9151
Figure 2. Surgical repair of a female patient with delayed esophageal perforation. The anteroposterior (A, B) and lat-eral (C, D) views of the cervical spine before (A, C) and after repair surgery (B, D) were shown. The patients showed a complete paraplegia at C5 and wound dehiscence with viscous secretion on admission (E) and the wound healed at the latest follow-up (F). The cervical spine was approached through the original incision and the implants were removed (G). A nasogastric tube was positioned through the perforation site to locate and assess the size and shape of the lesion (H). The esophageal perforation was then sutured (I) and a SCM flap was sutured with contralateral longuscolli muscle to protect the esophageal from the vertebrae (J).
Muscle flap for esophageal perforation
9147 Int J Clin Exp Med 2016;9(6):9143-9151
elevated until a sufficient length of SCM flap (8 cm to 10 cm) was available. The SCM flap was then medially rotated, crossed over the verte-brae, interposed between vertebrae and the posterior wall of esophagus, and then sutured to contralateral longuscolli muscle (Figure 1D). The SCM flap forms a soft tissue barrier be- tween the esophageal lesion and cervical ver-tebrae as to reinforce the primary repair, pro-tect the esophageal wall and provide with abun-dant blood supply for the healing of perfora- tion.
Direct suture of the SCM flap to the margins of the perforation as a patch was not used in our cases since the anticipated scar tissue might
contract the esophageal wall and contribute to discomfort. Fistula tract and accompanying scar tissue were also resected when exist since their presence could interfere with normal clo-sure and adherence of local tissue. Surgical operations should be performed with caution when the fistula tract was anatomically close to vascular structures. The incision is then closed with a drainage retained for 72 hours.
Postoperative management strategies were planned accordingly to the condition in each case. All patients were asked not to intake food orally unless the esophagographic result at 14 days postoperatively was negative. Follow-up
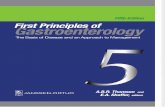
Figure 3. The anteroposterior (A, B) and lateral (C, D) views of the cervical spine before (A, C) and after repair surgery (B, D) were shown. The patients showed a wound dehiscence on admission (E) and the wound healed at the latest follow-up (F).
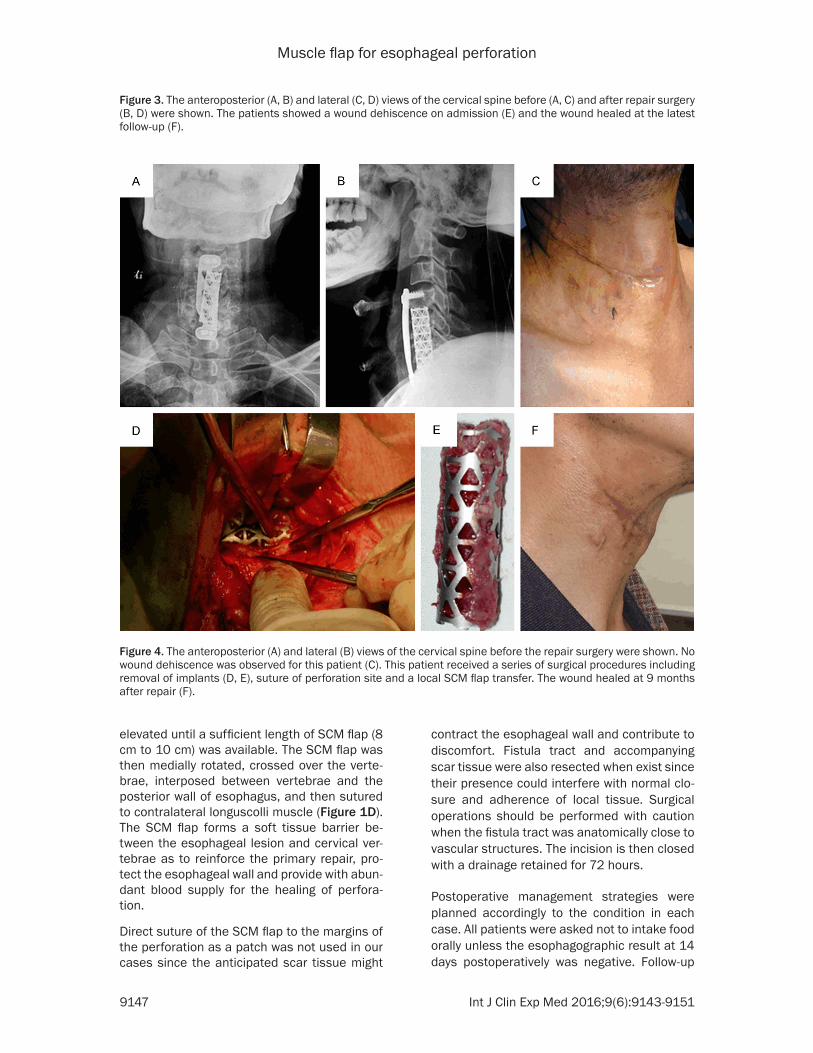
Figure 4. The anteroposterior (A) and lateral (B) views of the cervical spine before the repair surgery were shown. No wound dehiscence was observed for this patient (C). This patient received a series of surgical procedures including removal of implants (D, E), suture of perforation site and a local SCM flap transfer. The wound healed at 9 months after repair (F).

Muscle flap for esophageal perforation
9148 Int J Clin Exp Med 2016;9(6):9143-9151
was carried out to ensure solid food intake (generally 2 to 3 weeks after surgical repair) and spinal stability in all cases.
Case 1
A 20-year-old female with C5 burst fracture underwent C5 corpectomy and C4-C6 anterior fixation at another hospital (Figure 2A-D). Six days after the surgery, the patient presented with neck swelling with a palpable mass, diffi-cult breathing, wound dehiscence and alimen-tary fluid leakage (Figure 2E). The symptoms were not effectively controlled for over 14 months after the index surgery, and she was then transferred to our hospital with long-term artificial ventilation over tracheostoma. On admission, the patient showed complete para-plegia below C5 and wound dehiscence with viscous secretion. Diagnosis of esophageal perforation was confirmed by dye leakage through the cervical wound after swallowing methylene blue. The revision surgery was then planned on December 2nd, 2008. Repair sur-gery was performed as described above (Figure 2G-J). The patient resumed eating liquid food 3 weeks after the revision surgery. No sign of recurred perforation was noticed since then and all symptoms were relieved up to the latest follow-up (Figure 2F).
Case 2
A 28-year-old female underwent anterior cervi-cal discectomy and fusion at C5/C6 ACDF in October 2011(Figure 3A-D). One month later, the patient presented with fever, neck pain and local abscess. A 2cm wound dehiscence with mucopurulent discharge was seen (Figure 3E). Esophagoscopy demonstrated anesophageal perforation at the level of C6, which was con-firmed by a barium swallow test. Nasogastric nutrition, local wound irrigation and drainage were then given for 3 months, but salivary liq-uid and food pieces could still be seen on the wound dressing. On May 28th, 2012, we per-formed the first repair surgery and found a 1cm longitudinal esophagus rupture with bulging mucosa at the site adjacent to the implanted plate. We then sutured the esophageal rupture and closed the wound with drainage. Daily dressing change, intravenous antibiotics, naso-gastric nutrition were maintained. Ten months later, visible dehiscence could still be observed with liquid discharge on the wound dressing. A second repair surgery was performed in April 2013.
After exposure of the cervical esophagus, the esophageal perforation sutured 10 months ago was found unhealed and a 1.8 cm longitudinal esophagus rupture was detected. Infection was found in the tissue around the cage, so the interbody cage was removed since the C5/6 was confirmed to be stable. We firstly repaired the ruptured esophagus with absorbable inter-rupted stitches. Then the SCM muscle flap was sutured to the contralateral longuscolli muscle to promote healing of esophageal perforation. The patient was encouraged to take liquid food at the 2nd postoperative week and all symptoms were relieved up to the last follow-up (Figure 3F).
Case 3
A 61-year-old male patient had suffered quad-riplegia after a motor vehicle accident on May 15th, 2004. X-ray and MRI showed severe spon-dylotic myelopathy and spinal canal stenosis from C4 to C7, ruptured C4/C5 intervertebral disc and protruded intervertebral disc (C5/6 and C6/7). Anterior corpectomy of C5 and C6, and fixation with an anterior plate from C4 to C7 were performed (Figure 4A, 4B).
The patient complained of neck swelling and short of breath by the second postoperative day, and his condition had worsened by the tenth day with fever (39.0°C), difficult and pain-ful swallowing, alimentary fluid leakage and purulent secretion.No wound dehiscence was observed for this patient (Figure 4C). Suspecting esophageal injury, we exposed the esophagus through the original incision site on June 3rd.Purulent material in the parapharyngeal space was observed and a 8 cm esophageal perfora-tion was seen in the posterolateral wall of esophagus at the level of C3 to C6. The perfora-tion was repaired with simple interrupted su- tures. The SCM flap was prepared and sutured to the contralateral longuscolli muscle by cross-ing underneath the esophagus (Figure 4E). Drainage, intravenous antibiotics, nasogastric nutrition were maintained. Three weeks later, the patient was encouraged to orally take liquid food. However, symptoms including fever, neck swelling, wound dehiscence and mucopurulent discharge recurred up to nine months. We per-formed another surgery on March 8th, 2005. It was observed that the esophageal perforation had healed, and no significant mucopurulent discharge or inflammation was seen around esophagus. Infection in the bone graft and tita-

Muscle flap for esophageal perforation
9149 Int J Clin Exp Med 2016;9(6):9143-9151
nium mesh was found by further exploration. We then removed the bone graft together with the titanium mesh and no further fixation was performed since the segments were confirmed to be stable (Figure 4D). The patient resumed eating liquid food 3 weeks later. Up to latest follow-up, all symptoms were relieved without complications (Figure 4F). The neurological condition continued to improve without any sign of cervical spine instability.
Case 4
A 57-year-old female underwent C5 corpectomy and C4-C6 fixation with titanium mesh for spon-dylotic myelopathy. Two weeks postoperatively, she developed fever, neck pain, difficult breath-ing, wound dehiscence and mucopurulent dis-charge. Surgical intervention was performed by 1 month after the index surgery since all symp-toms were not relived with treatments including nasogastric feeding, intravenous antibiotic, drainage, local irrigation and dressing change. By a lateral cervical approach, we found a 3 cm esophageal perforation and closed it with inter-rupted suture. The SCM flap was prepared and sutured to the contralateral longuscolli muscle as described above. Drainage was placed and the incision was closed. All nonsurgical man-agements were continued. The patient started oral intake of liquid food 2 weeks later, and all symptoms were relieved at 3 months after the revision surgery.
Case 5
A 41-year-old male underwent C3/C4 ACDF on July 18th, 2009. Two weeks after surgery, the patient presented with fever, wound dehis-cence, alimentary fluid leakage, dysphagia and neck swelling. He was given nasogastric nutri-tion, intravenous antibiotics, local wound irriga-tion and drainage for three months, but salivary liquid and food pieces could still be seen on the wound dressing. On October 28th, 2009, we performed a repair surgery and found a 2 cm longitudinal esophageal perforation at the level of C3/C4. The ruptured esophagus was repaired with absorbable interrupted stitches. The SCM muscle flap was subsequently sutured to the contralateral longuscolli muscle to promote healing of esophageal perforation. After sur-gery, he was given nasogastric nutrition, intra-venous antibiotics, local drainage, and wound dressing change. The patient was encouraged to take liquid food at the 14th postoperative
day. The wound healed well and the patient returned to normal diet at 3 months postopera-tively with all symptoms relieved.
Discussion
Current management strategy for esophageal perforations remains conventional and nonsur-gical, such as nasogastric drainage, antibiotics, intravenous alimentation and other treatments. In cases with large perforation, poor systemic condition or delayed management, the consen-suses for ideal treatment have not yet been reached [13, 14]. Nevertheless, a multidisci-plinary approach that includes surgical inter-vention and supporting managements is war-ranted to ensure the successful repair of eso- phageal perforation [15, 16].
A favorable environment of soft tissue is required for wound healing and tissue regener-ation. The musculature of the cervical spine offers the possibility for surgeons to repair the perforated esophagus with a muscle flap, and such reinforcement has therefore been atte- mpted in surgical treatment of esophageal per-foration. To our knowledge, the use of a SCM flap for treatment of esophageal perforation fol-lowing a repairing suture has been described and established, and promising outcomes have been seen in several publications with limited number of cases [17-21]. Therefore, more stud-ies are encouraged to report the results of SCM flap in the repair of esophageal perforation. In the present study, the SCM flap was sutured only on the caudal end to the contralateral lon-guscolli muscle, but not directly on the esopha-geal defect margin nor the platysmamuscle. Satisfying results were obtained in all 5 cases, providing more evidence for the reliability of SCM flap repair.
Alternative techniques of soft tissue coverage to close a esophageal perforation include free jejunal graft [22], longuscollimuslce flap [23] and pectoralis major flap [24]. We prefer SCM flap since it is close to the perforation site and does not cost another surgical incision to har-vest. Occasionally, owing to either the delayed recognition or severe inflammation, the closure of perforation may fail even with SCM flap repairing. In such a situation, a pectoralis major flap may be more appropriate because of its large size [25]. Meanwhile, adequate drainage, cessation swallowing and antibiotic therapy should also be relied on. Direct repair was indi-

Muscle flap for esophageal perforation
9150 Int J Clin Exp Med 2016;9(6):9143-9151
cated only when patient’s systemic condition was stable.
Conclusions
The management of esophageal perforation following anterior cervical spine fusion has been considered as a significant surgical chal-lenge. Although conservative management remains irreplaceable, we suggest in the pres-ent study that surgical repair strategy including removal of implants, esophageal suture, and a local SCM flap is capable of achieving satisfac-tory clinical outcome, especially in those with a large chronic perforation site.
Disclosure of conflict of interest
None.
Address correspondence to: Zhuojing Luo, Depart- ment of Orthopaedics, Xijing Hospital, The Fourth Military Medical University, Xi’an 710032, China. Tel: 86-29-84775285; Fax: 86-29-84775285; E-mail: [email protected]; [email protected]
References
[1] Konstantakos AK, Temes RT. Delayed esopha-geal perforation: a complication of anterior cervical spine fixation. Ann Thorac Surg 2005; 80: 349.
[2] Sahjpaul RL. Esophageal perforation from an-terior cervical screw migration. Surg Neurol 2007; 68: 205-209.
[3] Fountas KN, Kapsalaki EZ, Machinis T, Robin-son JS. Extrusion of a screw into the gastroin-testinal tract after anterior cervical spine plat-ing. J Spinal Disord Tech 2006; 19: 199-203.
[4] Pompili A, Canitano S, Caroli F, Caterino M, Crecco M, Raus L, Occhipinti E. A symptomatic esophageal perforation caused by late screw migration after anterior cervical plating: report of a case and review of relevant literature. Spine (Phila Pa 1976) 2002; 27: E499-E502.
[5] Gupta NM, Kaman L. Personal management of 57 consecutive patients with esophageal per-foration. Am J Surg 2004; 187: 58-63.
[6] Newhouse KE, Lindsey RW, Clark CR, Lieponis J, Murphy MJ. Esophageal perforation follow-ing anterior cervical spine surgery. Spine (Phila Pa 1976) 1989; 14: 1051-1053.
[7] Skinner DB, Little AG, DeMeester TR. Manage-ment of esophageal perforation. Am J Surg 1980; 139: 760-764.
[8] Smith MD, Bolesta MJ. Esophageal perforation after anterior cervical plate fixation: a report of two cases. J Spinal Disord 1992; 5: 357-362.
[9] Jones WG, Ginsberg RJ. Esophageal perfora-tion: a continuing challenge. Ann Thorac Surg 1992; 53: 534-543.
[10] Jougon J, Cantini O, Delcambre F, Minniti A, Velly JF. Esophageal perforation: life threaten-ing complication of endotracheal intubation. Eur J Cardiothorac Surg 2001; 20: 7-11.
[11] Brinster CJ, Singhal S, Lee L, Marshall MB, Kai-ser LR, Kucharczuk JC. Evolving options in the management of esophageal perforation. Ann Thorac Surg 2004; 77: 1475-1483.
[12] Orlando ER, Caroli E, Ferrante L. Management of the cervical esophagus and hypofarinx per-forations complicating anterior cervical spine surgery. Spine (Phila Pa 1976) 2003; 28: E290-E295.
[13] Lucas J, Smith E, Eskander M, McPhee J, Lap-insky A. Esophageal perforation more than 10 years after anterior cervical spine plating. Clin Neurol Neurosurg 2013; 115: 1842-1844.
[14] Lu X, Guo Q, Ni B. Esophagus perforation com-plicating anterior cervical spine surgery. Eur Spine J 2012; 21: 172-177.
[15] von Rahden BH, Stein HJ, Scherer MA. Late hypopharyngo-esophageal perforation after cervical spine surgery: proposal of a therapeu-tic strategy. Eur Spine J 2005; 14: 880-886.
[16] Dakwar E, Uribe JS, Padhya TA, Vale FL. Man-agement of delayed esophageal perforations after anterior cervical spinal surgery. J Neuro-surg Spine 2009; 11: 320-325.
[17] Navarro R, Javahery R, Eismont F, Arnold DJ, Bhatia NN, Vanni S, Levi AD. The role of the sternocleidomastoid muscle flap for esopha-geal fistula repair in anterior cervical spine sur-gery. Spine (Phila Pa 1976) 2005; 30: E617-E622.
[18] Benazzo M, Spasiano R, Bertino G, Occhini A, Gatti P. Sternocleidomastoid muscle flap in esophageal perforation repair after cervical spine surgery: concepts, techniques, and per-sonal experience. J Spinal Disord Tech 2008; 21: 597-605.
[19] Ahn SH, Lee SH, Kim ES, Eoh W. Successful repair of esophageal perforation after anterior cervical fusion for cervical spine fracture. J Clin Neurosci 2011; 18: 1374-1380.
[20] Iyoob VA. Postoperative pharyngocutaneous fistula: treated by sternocleidomastoid flap re-pair and cricopharyngeus myoyomy. Eur Spine J 2013; 22: 107-112
[21] Beasley N. Expert’s comment concerning grand rounds case entitled “Postoperative pharyngocutaneous fistula: treated with ster-nocleidomastoid flap repair and cricopharyn-geusmyotomy” (by V.A. Iyoob). Eur Spine J 2013; 22: 113-5.
[22] Küntscher MV, Erdmann D, Boltze WH, Ger-mann G. Use of a free jejunal graft for oesoph-

Muscle flap for esophageal perforation
9151 Int J Clin Exp Med 2016;9(6):9143-9151
ageal reconstruction following perforation af-ter cervical spine surgery: case report and review of the literature. Spinal Cord 2003; 41: 543-548.
[23] Haku T, Okuda Sy, Kanematsu F, Oda T, Miyau-chi A, Yamamoto T, Iwasaki M. Repair of cervi-cal esophageal perforation using longuscolli muscle flap: a case report of a patient with cervical spinal cord injury. Spine J 2008; 8:831-835.
[24] Reid RR, Dutra J, Conley DB, Ondra SL, Duma-nian GA. Improved repair of cervical esopha-geal fistula complicating anterior spinal fusion: free omental flap compared with pectoralis major flap. Report of four cases. J Neurosurg 2004; 100: 66-70.
[25] Liu HL, Chan JY, Wei WI. The changing role of pectoralismajor flap in head and neck recon-struction. Eur Arch Otorhinolaryngol 2010; 267: 1759-1763.