Organization: Anne Arundel Medical · PDF fileOrganization: Anne Arundel Medical Center...
12
Organization: Anne Arundel Medical Center Solution Title: Driving Quality and Change through Implementation of Leadership Standard Work Program/Project Description, including Goals: Executive leadership at Anne Arundel Medical Center (AAMC) identified that leaders in the organization were reactive in the management of their business units. Leaders spent a large portion of their day problem solving and taking on the problems of the front line staff. Leaders at AAMC did not have standard work nor the tools necessary to proactively run their units. Executive leadership engaged the performance improvement department to organize at team to create a proactive approach to continuous daily improvements and implement sustainable standard work. Goals of this program: Shift leaders from reactive to proactive Facilitate problem solving at the staff/frontline level Increase staff engagement and development Increase coaching and mentoring at all levels of leadership Data driven process improvement via metrics Process: The team used Lean methodology and started with a weeklong Rapid Improvement Event (RIE). The solutions and subsequent projects were created and implemented using A3 thinking. A3 is a tool named for the size of the paper that becomes a communication tool. A3 thinking is a methodology for working through a problem that forces consensus building, unifies culture, and promotes unit and organizational learning. The clinical nursing directors from the Heart and Vascular Unit (HVU) and Neonatal Intensive Care Unit (NICU) implemented the solutions identified during the RIE on their respective units, refined the process using A3 thinking, and continued to implement additional solutions over subsequent months. Solution: The RIE team identified three key aspects of Leadership Standard Work (LSW) to initially implement. LSW is standard work that directs leaders to know what to do throughout the day, incorporates teaching, coaching, and mentoring, uses metrics to drive change and improve quality, and requires leaders to create and deploy counter measures (Barnas, 2011). The three initial solutions were Daily Prep, Huddle including Huddle Board with daily metrics, and walking the gemba. Daily Prep sheets are a template used to capture the metrics data and identify trends in defects, quality outcomes, productivity, processes and systems that impact change. This template drives the business operations and key areas of work (Barnas, 2014). Huddle is a gathering of unit leaders and staff to review the status of departmental metrics to target for root cause, institute countermeasures at the process level in promoting and prioritizing
Transcript of Organization: Anne Arundel Medical · PDF fileOrganization: Anne Arundel Medical Center...

Organization: Anne Arundel Medical Center
Solution Title: Driving Quality and Change through Implementation of Leadership Standard
Work
Program/Project Description, including Goals: Executive leadership at Anne Arundel
Medical Center (AAMC) identified that leaders in the organization were reactive in the
management of their business units. Leaders spent a large portion of their day problem solving
and taking on the problems of the front line staff. Leaders at AAMC did not have standard work
nor the tools necessary to proactively run their units. Executive leadership engaged the
performance improvement department to organize at team to create a proactive approach to
continuous daily improvements and implement sustainable standard work.
Goals of this program:
Shift leaders from reactive to proactive
Facilitate problem solving at the staff/frontline level
Increase staff engagement and development
Increase coaching and mentoring at all levels of leadership
Data driven process improvement via metrics
Process: The team used Lean methodology and started with a weeklong Rapid Improvement
Event (RIE). The solutions and subsequent projects were created and implemented using A3
thinking. A3 is a tool named for the size of the paper that becomes a communication tool. A3
thinking is a methodology for working through a problem that forces consensus building, unifies
culture, and promotes unit and organizational learning. The clinical nursing directors from the
Heart and Vascular Unit (HVU) and Neonatal Intensive Care Unit (NICU) implemented the
solutions identified during the RIE on their respective units, refined the process using A3
thinking, and continued to implement additional solutions over subsequent months.
Solution: The RIE team identified three key aspects of Leadership Standard Work (LSW) to
initially implement. LSW is standard work that directs leaders to know what to do throughout
the day, incorporates teaching, coaching, and mentoring, uses metrics to drive change and
improve quality, and requires leaders to create and deploy counter measures (Barnas, 2011). The
three initial solutions were Daily Prep, Huddle including Huddle Board with daily metrics, and
walking the gemba. Daily Prep sheets are a template used to capture the metrics data and
identify trends in defects, quality outcomes, productivity, processes and systems that impact
change. This template drives the business operations and key areas of work (Barnas, 2014).
Huddle is a gathering of unit leaders and staff to review the status of departmental metrics to
target for root cause, institute countermeasures at the process level in promoting and prioritizing

ideas at staff level. An evaluation of updated improvements from the previous day and how we
can do it better using the daily prep sheet (Barnas, 2014). Gemba means the “real place”; the
place where work is done, walking in the place to ask right questions, actively listening to
responses, following through on improvements and opportunities that is sustainable (Barnas,
2014). The clinical nursing director from HVU implemented these three aspects of LSW in
January 2014 after the RIE. The clinical nursing director from NICU was the next department
and implemented LSW in March 2014. Each director worked with the performance
improvement office to choose daily metrics. The daily metrics needed to be proactive measures,
easily obtained, that drove quality indicators, standard work, or processes. The directors worked
with their leadership teams to implement the Daily Prep and Huddle. Gemba by the directors
helped create engagement with staff for the huddle and daily metrics. Through Gemba, the
directors and staff, together, looked at processes and standard work.
Measurable Outcomes:
HVU implemented huddles, gemba, and daily metrics in January 2014. We chose quality
indicators, created action plans, and used daily metrics to drive improvement. We worked on
reducing the number of falls and number of injury falls and reducing catheter associated urinary
tract infections (CAUTI). For falls our daily metric was the percentage of patients that had all
aspects of fall prevention in place. Baseline data for HVU falls:
Total Patient Falls Per 1,000 Patient Days
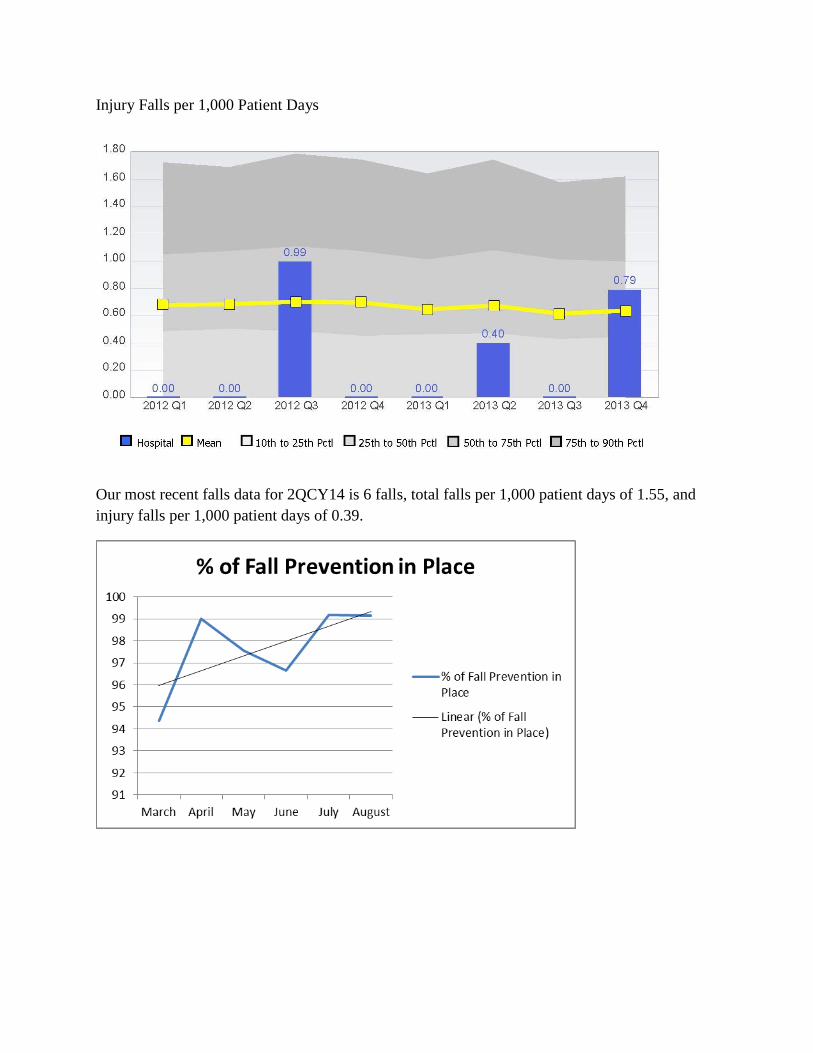
Injury Falls per 1,000 Patient Days
Our most recent falls data for 2QCY14 is 6 falls, total falls per 1,000 patient days of 1.55, and
injury falls per 1,000 patient days of 0.39.

For CAUTI, our daily metric was the percentage of the foleys that meet criteria for continued
use. The criteria for continued use are strict output measurement, <24 hours postop, bladder
outlet obstruction, neurogenic bladder, prolonged immobilization, open sacral or perineal
wounds, alteration of perineum post procedure, epidural use, or comfort/end of life care.
Baseline HVU CAUTI data:
Catheter Associated Urinary Tract Infections per 1000 Catheter Days

HVU looked at this metric daily from January through April 2014. Once our compliance was
close to 100% for greater than a month, we moved this measure to the kamishibai board where
we randomly audited compliance once a month. A kamishibai board is a lean tool for visual
management of audits that promote sustainability and continuous process improvements (Barnas,
2014). HVU had three CAUTI in 1QCY14 for a rate of 9.35 total CAUTI per 1,000 catheter
day. HVU did not have any CAUTI for 2QCY14, 1 CAUTI in July 2014, and zero for August
and September.
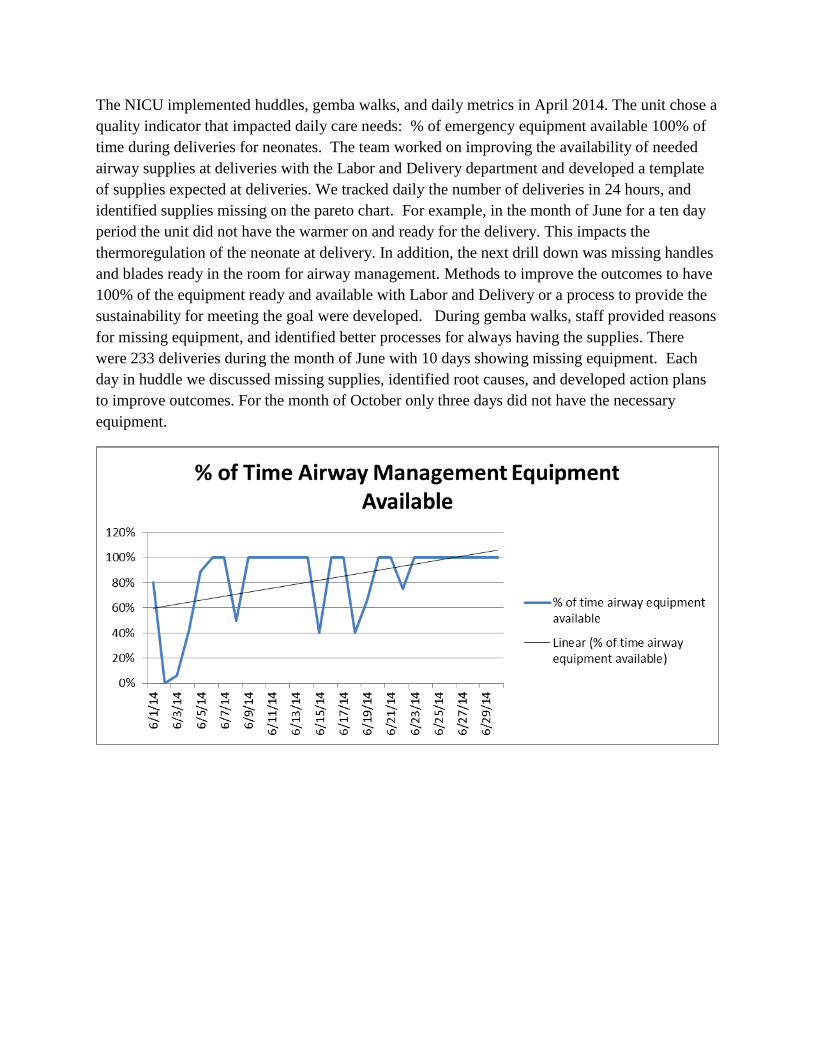
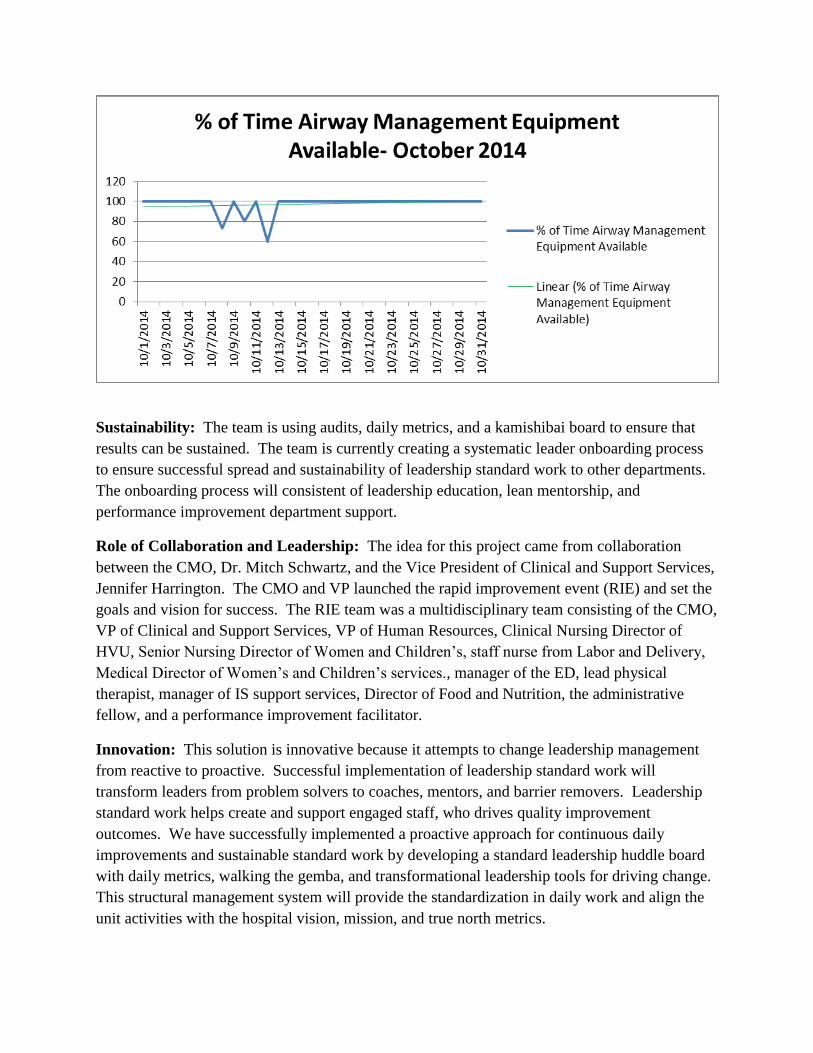
The NICU implemented huddles, gemba walks, and daily metrics in April 2014. The unit chose a
quality indicator that impacted daily care needs: % of emergency equipment available 100% of
time during deliveries for neonates. The team worked on improving the availability of needed
airway supplies at deliveries with the Labor and Delivery department and developed a template
of supplies expected at deliveries. We tracked daily the number of deliveries in 24 hours, and
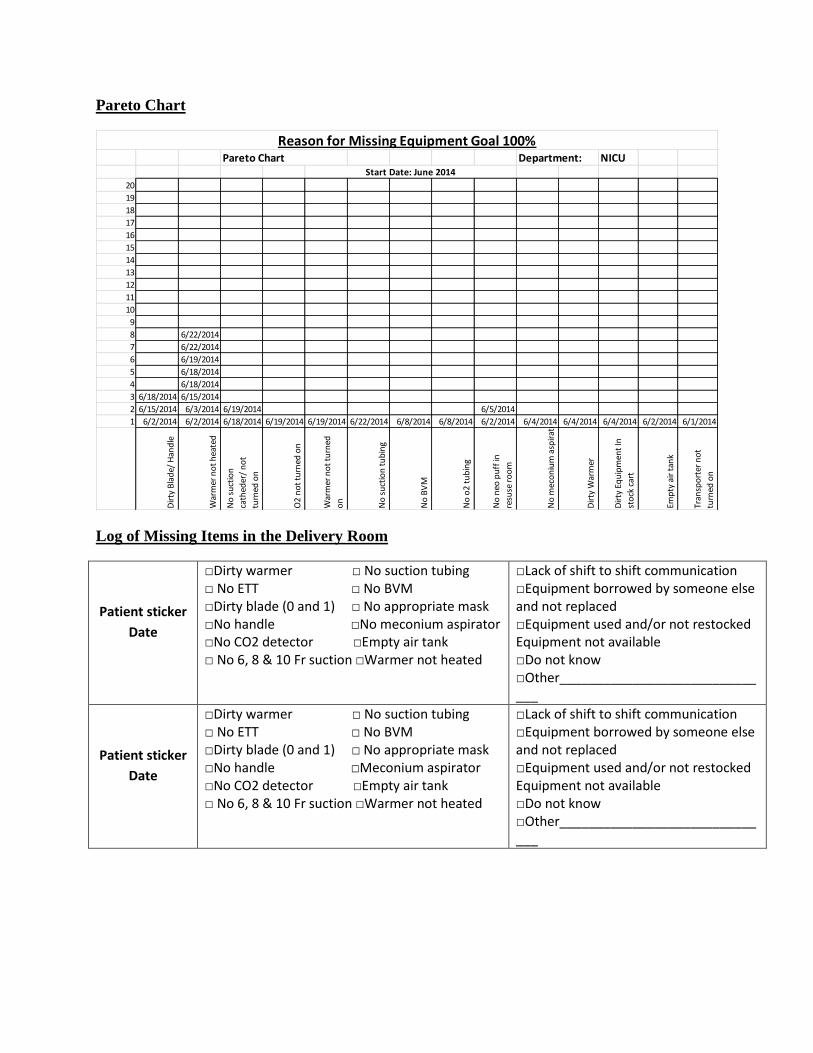
identified supplies missing on the pareto chart. For example, in the month of June for a ten day
period the unit did not have the warmer on and ready for the delivery. This impacts the
thermoregulation of the neonate at delivery. In addition, the next drill down was missing handles
and blades ready in the room for airway management. Methods to improve the outcomes to have
100% of the equipment ready and available with Labor and Delivery or a process to provide the
sustainability for meeting the goal were developed. During gemba walks, staff provided reasons
for missing equipment, and identified better processes for always having the supplies. There
were 233 deliveries during the month of June with 10 days showing missing equipment. Each
day in huddle we discussed missing supplies, identified root causes, and developed action plans
to improve outcomes. For the month of October only three days did not have the necessary
equipment.
Sustainability: The team is using audits, daily metrics, and a kamishibai board to ensure that
results can be sustained. The team is currently creating a systematic leader onboarding process
to ensure successful spread and sustainability of leadership standard work to other departments.
The onboarding process will consistent of leadership education, lean mentorship, and
performance improvement department support.
Role of Collaboration and Leadership: The idea for this project came from collaboration
between the CMO, Dr. Mitch Schwartz, and the Vice President of Clinical and Support Services,
Jennifer Harrington. The CMO and VP launched the rapid improvement event (RIE) and set the
goals and vision for success. The RIE team was a multidisciplinary team consisting of the CMO,
VP of Clinical and Support Services, VP of Human Resources, Clinical Nursing Director of
HVU, Senior Nursing Director of Women and Children’s, staff nurse from Labor and Delivery,
Medical Director of Women’s and Children’s services., manager of the ED, lead physical
therapist, manager of IS support services, Director of Food and Nutrition, the administrative
fellow, and a performance improvement facilitator.
Innovation: This solution is innovative because it attempts to change leadership management
from reactive to proactive. Successful implementation of leadership standard work will
transform leaders from problem solvers to coaches, mentors, and barrier removers. Leadership
standard work helps create and support engaged staff, who drives quality improvement
outcomes. We have successfully implemented a proactive approach for continuous daily
improvements and sustainable standard work by developing a standard leadership huddle board
with daily metrics, walking the gemba, and transformational leadership tools for driving change.
This structural management system will provide the standardization in daily work and align the
unit activities with the hospital vision, mission, and true north metrics.

Related Tools and Resources
The Daily Prep - NICU
6/16 6/17 6/18 6/19 6/20 6/21 6/22 Notes
Date Mon Tue Wed Thu Fri Sat Sun Monday Tuesday Wednesday Thursday Friday Fri/Sat Additional Notes
Qu
alit
y
#of Pts discharge on time/# of patients for discharge each day.
0/0 0/1 5/5 2/2 N/A 1/1 2/4
% discharge time N/A 100% 100% 100% N/A 100% 50%
# of times airway management equipment not available (past 24hr)
0/3 0/11 4/10 4/6 0/5 0/4 3/4
% of airway equipment available 100% 100% 40% 66% 100% 100% 75%
# of pts/# of RN's staffing 17/7 22/8 20/8 18/8 18/7 16/7 18/7
Staffing metric of volume 2.43 2.75 2.5 2.25 2.57 2.29 2.57
% Productivity 97% 100% 100% 90% 100% 92% 100%
Co
mm
un
ity
Pt./ Family need extra support 2 2 2 2 3 1 1
Family concerns/complaints 0 1 0 0 0 0 0
Wo
rkfo
rce
Staff need extra support 0 0 1 0 0 0 0
Staff orientation 0 0 0 0 2 0 0
Staff floating in/staff floating out 0/0 0/0 1/0 0/0 0/0 0/0 0/0
Celebrations
Hot Cards
Mock
Survey
Inservices/competencies Magnet - - - - - >
Gro
wth
PT / RN 17/7 22/8 20/8 15/6 18/8 16/7 18/7
Staffing to Volume 2.42 2.75 2.5 2.5 2.25 2.29 2.57
Acuity (level 1/2 of care) 2/5 2/5 2/7 3/3 4/3 2/4 2/4
Transfers in / transfer out 0/0 1/0 0/0 0/0 0/0 0/0 0/0
Fin
ance
Staff callouts 0 0 0 0 0 0 0
Staff on call 0 0 0
2OC 1LC
2OC 0 0
Staff in overtime 0 0 0 0 0 0 0
Anticipated admissions 3 1 3 1 0 0 0
Anticipated discharges 1 3 5 2 1 0 2

Supply management needs
eye spec
00 Blades
00 Blades
Upcoming Week
KEY Staffing to Volume - Goal 2.4 PT/RN
current past 24 hours
The Huddle Board Standard Work
Frequency – Daily
5-7 minutes
Recognition - 1 minute
o Examples
Identify persons who have solved problems
Birthdays/anniversaries – let staff announce rather than the leader being
challenged to remember all
Review of Metrics – 3 minutes
Updates – 1 minute
o Examples
Flu shots due
Mandatory Education due
Evaluations due
Opportunities - 2 minutes
o Place on pick chart
o Team assigns priority
o Encourage staff member to take ownership
o Post completed items under success and leave for two weeks

Gemba
Monday:
• Is there Standard Work?
• Is Standard Work adhered to?
• Is it good Standard Work?
• Can it be improved?
Tuesday:
Wednesday: Thursday:
Friday: Saturday/Sunday:
Pareto Chart
Department: NICU
20
19
18
17
16
15
14
13
12
11
10
9
8 6/22/2014
7 6/22/2014
6 6/19/2014
5 6/18/2014
4 6/18/2014
3 6/18/2014 6/15/2014
2 6/15/2014 6/3/2014 6/19/2014 6/5/2014
1 6/2/2014 6/2/2014 6/18/2014 6/19/2014 6/19/2014 6/22/2014 6/8/2014 6/8/2014 6/2/2014 6/4/2014 6/4/2014 6/4/2014 6/2/2014 6/1/2014
Dir
ty B
lad
e/ H
and
le
War
mer
no
t h
eate
d
No
su
ctio
n
cath
eder
/ n
ot
turn
ed o
n
O2
no
t tu
rned
on
War
mer
no
t tu
rned
on
No
su
ctio
n t
ub
ing
No
BV
M
No
o2
tu
bin
g
No
neo
pu
ff in
resu
se r
oo
m
No
mec
on
ium
asp
irat
or
Dir
ty W
arm
er
Dir
ty E
qu
ipm
ent
In
sto
ck c
art
Emp
ty a
ir t
ank
Tran
spo
rter
no
t
turn
ed o
n
Start Date: June 2014
Reason for Missing Equipment Goal 100%Pareto Chart
Log of Missing Items in the Delivery Room
Patient sticker
Date
□Dirty warmer □ No suction tubing □ No ETT □ No BVM □Dirty blade (0 and 1) □ No appropriate mask □No handle □No meconium aspirator □No CO2 detector □Empty air tank □ No 6, 8 & 10 Fr suction □Warmer not heated
□Lack of shift to shift communication □Equipment borrowed by someone else and not replaced □Equipment used and/or not restocked Equipment not available □Do not know □Other______________________________
Patient sticker
Date
□Dirty warmer □ No suction tubing □ No ETT □ No BVM □Dirty blade (0 and 1) □ No appropriate mask □No handle □Meconium aspirator □No CO2 detector □Empty air tank □ No 6, 8 & 10 Fr suction □Warmer not heated
□Lack of shift to shift communication □Equipment borrowed by someone else and not replaced □Equipment used and/or not restocked Equipment not available □Do not know □Other______________________________
Contact Person
Title: Carol Lacher, Holly Sowko
Email: [email protected], [email protected]
Phone: 443-891-4331, 443-481-1523
References
Barnas, K. (2014) Beyond Heroes: A Lean Management System for Healthcare.
Appleton, WI: ThedaCare Center for Healthcare Value.
Barnas, K. (2011) ThedaCare’s business performance system: Sustaining continuous daily
improvement through hospital management in a Lean environment. The Joint
Commission Journal on Quality and Patient Safety, 37(9), 387-399.