Orf: A Case Report
3
Henry Ford Hospital Medical Journal Henry Ford Hospital Medical Journal Volume 37 Number 2 Article 8 6-1989 Orf: A Case Report Orf: A Case Report Brent W. Mohr David Katz Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal Part of the Life Sciences Commons, Medical Specialties Commons, and the Public Health Commons Recommended Citation Recommended Citation Mohr, Brent W. and Katz, David (1989) "Orf: A Case Report," Henry Ford Hospital Medical Journal : Vol. 37 : No. 2 , 79-80. Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol37/iss2/8 This Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Henry Ford Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons.
Transcript of Orf: A Case Report
Henry Ford Hospital Medical Journal Henry Ford Hospital Medical Journal
Volume 37 Number 2 Article 8
6-1989
Orf: A Case Report Orf: A Case Report
Brent W. Mohr
David Katz
Follow this and additional works at: https://scholarlycommons.henryford.com/hfhmedjournal
Part of the Life Sciences Commons, Medical Specialties Commons, and the Public Health Commons
Recommended Citation Recommended Citation Mohr, Brent W. and Katz, David (1989) "Orf: A Case Report," Henry Ford Hospital Medical Journal : Vol. 37 : No. 2 , 79-80. Available at: https://scholarlycommons.henryford.com/hfhmedjournal/vol37/iss2/8
This Article is brought to you for free and open access by Henry Ford Health System Scholarly Commons. It has been accepted for inclusion in Henry Ford Hospital Medical Journal by an authorized editor of Henry Ford Health System Scholarly Commons.

Orf: A Case Report
Brent W. Mohr, MD,* and David Katz, MD+
Ecthyma contagiosum (orf), a viral disease endemic to sheep and goats, can be zoonotically transmitted to humans through contact with infected animals. While the disease is common among sheep and goat herders worldwide, it comes to medical attention infrequently since it is generally a mild self-limited illness. We recently treated a healthy 36-year-old female who presented with bullous lesions on her fingers and a diffuse macular rash which had developed after antibiotic therapy for her bullae. She had been caring for her neighbor's goats which had recently been ill with "sore mouth." We discuss this case of orf and review the medical literature on this self-limited illness uncommon to the midwestem UnitedStates. (Henry Ford Hosp Med J 1989:37:79-80)
Case Report
Apreviously healthy 36-year-old female presented with bullous lesions on her fingers and a widespread maculopapular rash.
Approximately four weeks prior to admission she noted blisters (up to 1 cm in diameter) on her fingers that had developed rapidly over 24 hours. The lesions were neither painful nor pruritic. Her private physician prescribed dicloxacillin therapy four days later On the fourth day of her antibiosis she developed an extensive generalized maculopapular rash on her hands, feet, trunk, and arms with sparing of her palms and soles. The antibiotic was di.scondnued.
The patient lived on a farm in southeastem Michigan and raised goats and horses. About one month prior to her illness she was caring for young goats with "sore mouth" and was feeding these animals by hand, coming in contact with fluid from their oral lesions.
The patient's medical history was remarkable for a traumatic amputation of the distal left thumb and peptic ulcer disease. Her only medication was cimetidine. There were no known allergies.
On physical examination vital signs and temperature were normal. Bullous lesions up to 1 cm in diameter with purplish discoloration were noted on her fingers. Some lesions had ruptured and were in various stages of healing (Fig 1). In addition, there was a diffuse erythematous maculopapular rash with areas of confluence on the hands, wrist, forearms, trunk, and perioral region (Figs 2 and 3).
Serum electrolytes, renal function, and complete blood count were normal.
Discussion Ecthyma contagiosum (orf, sore mouth, or contagious pos-
tular stomatitis) is a viral cutaneous disease endemic in sheep and goat herds worldwide. It may be transmitted to humans and generally manifests as nodules on exposed areas.
The disease is common among sheepherders around the world; however, the majority of cases are not reported, and no accurate figures regarding incidence are known (1,2). Sheep and goat herders, veterinarians, and immunosuppressed individuals are at particular risk for this disease.
The orf virus is a member of the poxvirus group and is quite hardy, surviving the winter months on barn doors, feeding troughs, fences, and shearing equipment (2,3). Susceptible ovine species become infected through contact with contaminated objects. Humans become infected by direct contact with contaminated animals and less frequently through contact with fences, shearing equipment, etc (2,4). Human-to-human transmission rarely, if ever, occurs (3,5,6).
Fig 1—Bullous lesions typical of orf.
Submitted for publication: August 8. 1989. Accepted for publication: October 17. 1989. *Departmenl of Intemal Medicine, St Joseph Mercy Hospital. Ann Arbor tDepartment of Infectious Diseases, St Joseph Mercy Hospital, Ann Arbor Address correspondence lo Dr Mohr. Department of Intemal Medicine. St Joseph Mercy
Hospital. 5301 East Huron River Dr. Ann Arbor. Ml 48106.
Henry Ford Hosp Med J—Vol 37. No 2. 1989 Orf—Mohr & Katz 79
HI' \
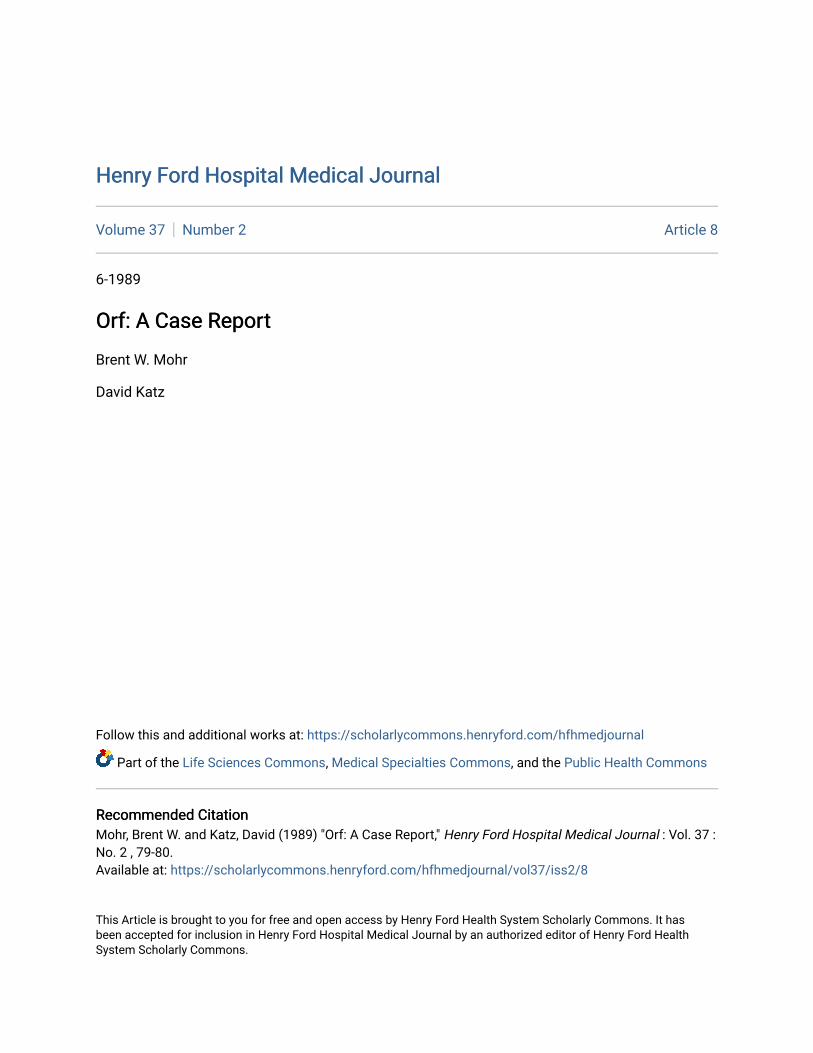
Fig 2—Oral vesicular lesions in our patient likely attributable to the orf virus.
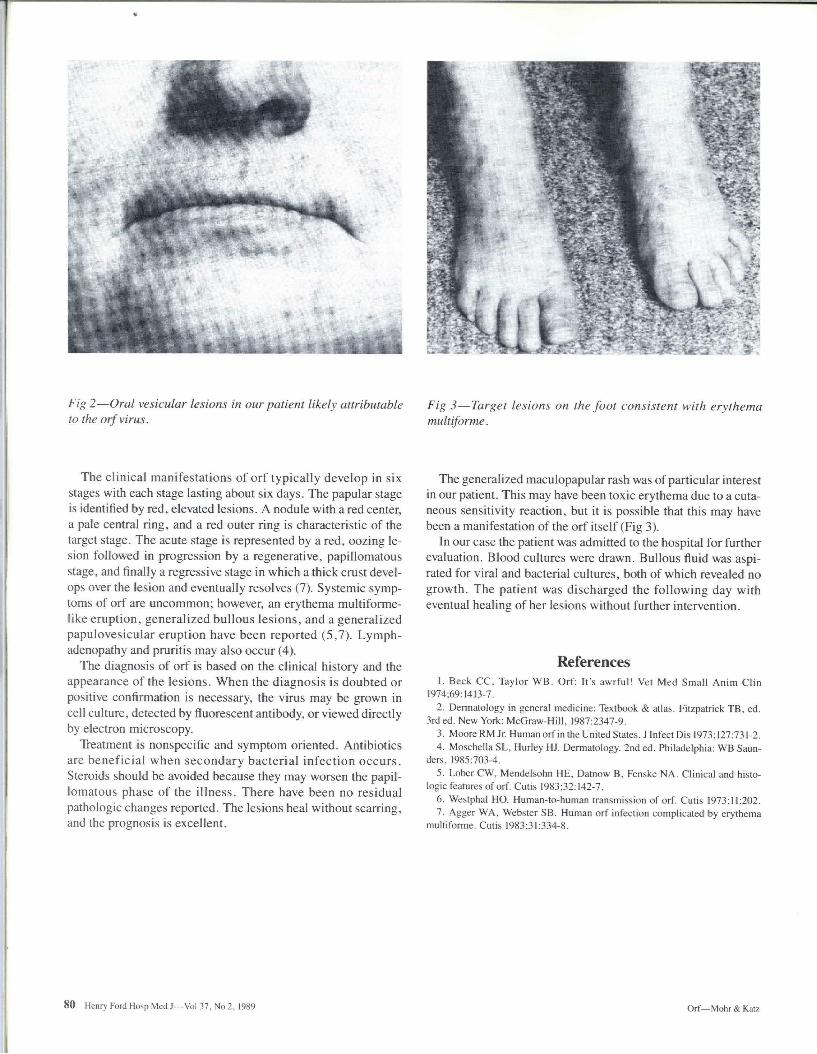
Fig 3—Target lesions on the foot consistent with erythema multiforme.
The clinical manifestations of orf typically develop in six stages with each stage lasting about six days. The papular stage is identified by red, elevated lesions. A nodule with a red center, a pale central ring, and a red outer ring is characteristic of the target stage. The acute stage is represented by a red, oozing lesion followed in progression by a regenerative, papillomatous stage, and finally a regressive stage in which a thick crust develops over the lesion and eventually resolves (7). Systemic symptoms of orf are uncommon; however, an erythema multiforme-like eruption, generalized bullous lesions, and a generalized papulovesicular eruption have been reported (5,7). Lymphadenopathy and pruritis may also occur (4).
The diagnosis of orf is based on the clinical history and the appearance of the lesions. When the diagnosis is doubted or positive confirmation is necessary, the virus may be grown in cell culture, detected by fluorescent antibody, or viewed directly by electron microscopy.
Treatment is nonspecific and symptom oriented. Antibiotics are beneficial when secondary bacterial infection occurs. Steroids should be avoided because they may worsen the papillomatous phase of the illness. There have been no residual pathologic changes reported. The lesions heal without scarring, and the prognosis is excellent.
The generalized maculopapular rash was of particular interest in our patient. This may have been toxic erythema due to a cutaneous sensitivity reaction, but it is possible that this may have been a manifestadon of the orf itself (Fig 3).
In our case the patient was admitted to the hospital for further evaluadon. Blood cultures were drawn. Bullous fluid was aspirated for viral and bacterial cultures, both of which revealed no growth. The patient was discharged the following day with eventual healing of her lesions without further intervention.
References 1. Beck CC, Taylor WB. Orf: It's awrful! Vet Med Small Anim Clm
1974;69:1413-7. 2. Dermatology in general medicine: Textbook & atlas. Fitzpatrick TB. ed.
3rded. New York: McGraw-Hill, 1987:2347-9. 3. Moore RM Jr Human ort'in the United States. J Infect Dis 1973; 127:731-2. 4. MoschellaSL, Hurley HJ. Dermatology. 2nded. Philadelphia: WB Saun
ders, 1985:703-4. 5. Lober CW, Mendelsohn HE, Datnow B, Fenske NA. Clinical and histo
logic features of orf. Cufis 1983;32:142-7. 6. Westphal HO. Human-to-human transmission of orf. Cutis 1973:11:202. 7. Agger WA. Webster SB. Human orf infection complicated by erythema
muldforme. Cutis 1983:31:334-8.
80 Henry Ford Hosp Med J—Vol 37, No 2, 1989 Orf—Mohr & Katz