
Oregon Health Net PPO Comparison Plans · Health Net PPO Comparison of Plans Eff ective January 1,...
24
Large Group Karen Boyd, Health Net We translate expertise into innovation. Commercial Health Net PPO Comparison of Plans Effective January 1, 2014 Oregon
Transcript of Oregon Health Net PPO Comparison Plans · Health Net PPO Comparison of Plans Eff ective January 1,...
Large Group
Karen Boyd,Health NetWe translate expertise into innovation.
Commercial
Health Net PPOComparison of Plans
Eff ective January 1, 2014Eff ective January 1, 2014
Karen Boyd,Health NetWe translate expertise into innovation.
Oregon

ContentsPlan family descriptions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1Plans at-a-glance
PPO Advantage LX . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2PPO HDHP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4PPO Advantage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6PPO Fifty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8PPO Essentials . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Pharmacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Ancillary programs
Well Net benefits and buy-up plan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Optional Dental. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Optional Vision . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Power Wellness! . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Online tools
Employers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Members . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20

Guide for Health Net Plan Families 2014
This guide outlines our most popular large group plans. Other plans
are available for sale to both size groups. Contact your Health Net
representative for a complete list of plans available.
PPO Advantage plans and Advantage LX• Advantage plans waive the deductible for
ER, urgent care, routine lab, and X-rays. They also have more items accumulating to OOPM.
• PPO Advantage LX waives the deductible for all diagnostic labs and imaging.
• Naming examples: A20-500-2-3500 or LX20-500-2-3500.
PPO HDHP plans• Suitable for Health Savings Accounts.
• Pharmacy benefit built in with deductible shared with the medical plan.
• No Well Net Alternative Care benefit included with these plans.
• Separate plan for individuals versus families.
• Naming examples: HD25008060w/HD80 or HD50008060w/HD80.
PPO Fifty plans• Two versions have zero deductible; member
pays 50% coinsurance up to OOPM.
• Two versions have a front-end deductible, then 50% member share on most services.
• Naming examples: 50/50-2500 or 1000-50/50-3500.
PPO Essentials• Two versions of each deductible plan:
1. Office visit copay version has OV copay and 80% coinsurance for most services after the deductible.
2. Most services apply toward deductible and coinsurance version – coinsurance applies to all services, 70% for most services, higher OOPM.
• Office visit copay version has higher copays for specialists.
• All diagnostic labs and imaging are subject to the plan deductible and coinsurance.
• Naming examples: E25-1000-2-5000 or E1000-3-6000.
For calendar year 2014, pharmacy benefits will not be included in the total out-of-pocket maximums under the Safe Harbor provision of the ACA.
All medical plans (except HDHP) include Well Net Alternative Care benefit $15 OV copayment ($25 for massage therapy; $1,000 annual max, all services combined).
1
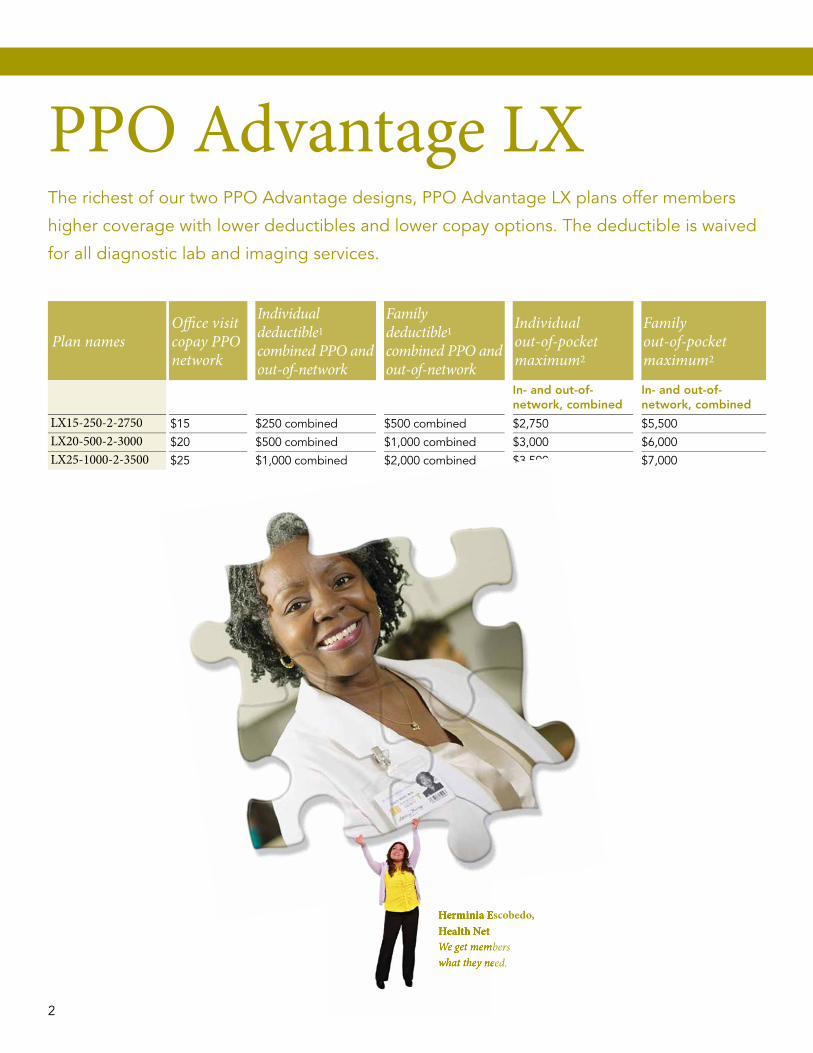
PPO Advantage LXThe richest of our two ppO Advantage designs, ppO Advantage LX plans offer members
higher coverage with lower deductibles and lower copay options. The deductible is waived
for all diagnostic lab and imaging services.
Plan namesOffi ce visitcopay PPO network
Individual deductible1
combined PPO and out-of-network
Family deductible1
combined PPO and out-of-network
Individualout-of-pocketmaximum2
Familyout-of-pocketmaximum2
In- and out-of-network, combined
In- and out-of-network, combined
LX15-250-2-2750 $15 $250 combined $500 combined $2,750 $5,500LX20-500-2-3000 $20 $500 combined $1,000 combined $3,000 $6,000LX25-1000-2-3500 $25 $1,000 combined $2,000 combined $3,500 $7,000
Herminia Escobedo,Health NetWe get members what they need.
$3,500
Herminia Escobedo,Health NetWe get members what they need.
2 3
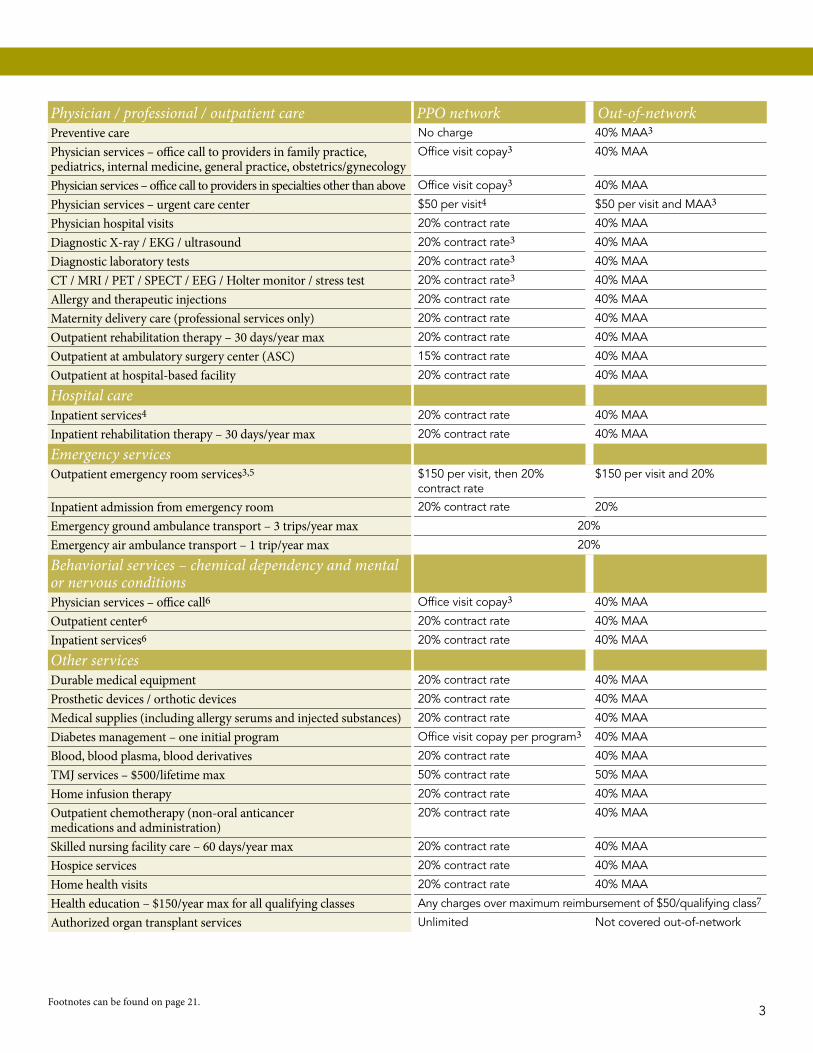
Physician / professional / outpatient care PPO network Out-of-networkPreventive care No charge 40% MAA3
Physician services – office call to providers in family practice, pediatrics, internal medicine, general practice, obstetrics/gynecology
Office visit copay3 40% MAA
Physician services – office call to providers in specialties other than above Office visit copay3 40% MAA
Physician services – urgent care center $50 per visit4 $50 per visit and MAA3
Physician hospital visits 20% contract rate 40% MAA
Diagnostic X-ray / EKG / ultrasound 20% contract rate3 40% MAA
Diagnostic laboratory tests 20% contract rate3 40% MAA
CT / MRI / PET / SPECT / EEG / Holter monitor / stress test 20% contract rate3 40% MAA
Allergy and therapeutic injections 20% contract rate 40% MAA
Maternity delivery care (professional services only) 20% contract rate 40% MAA
Outpatient rehabilitation therapy – 30 days/year max 20% contract rate 40% MAA
Outpatient at ambulatory surgery center (ASC) 15% contract rate 40% MAA
Outpatient at hospital-based facility 20% contract rate 40% MAA
Hospital careInpatient services4 20% contract rate 40% MAA
Inpatient rehabilitation therapy – 30 days/year max 20% contract rate 40% MAA
Emergency servicesOutpatient emergency room services3,5 $150 per visit, then 20%
contract rate$150 per visit and 20%
Inpatient admission from emergency room 20% contract rate 20%
Emergency ground ambulance transport – 3 trips/year max 20%
Emergency air ambulance transport – 1 trip/year max 20%
Behaviorial services – chemical dependency and mental or nervous conditionsPhysician services – office call6 Office visit copay3 40% MAA
Outpatient center6 20% contract rate 40% MAA
Inpatient services6 20% contract rate 40% MAA
Other servicesDurable medical equipment 20% contract rate 40% MAA
Prosthetic devices / orthotic devices 20% contract rate 40% MAA
Medical supplies (including allergy serums and injected substances) 20% contract rate 40% MAA
Diabetes management – one initial program Office visit copay per program3 40% MAA
Blood, blood plasma, blood derivatives 20% contract rate 40% MAA
TMJ services – $500/lifetime max 50% contract rate 50% MAA
Home infusion therapy 20% contract rate 40% MAA
Outpatient chemotherapy (non-oral anticancer medications and administration)
20% contract rate 40% MAA
Skilled nursing facility care – 60 days/year max 20% contract rate 40% MAA
Hospice services 20% contract rate 40% MAA
Home health visits 20% contract rate 40% MAA
Health education – $150/year max for all qualifying classes Any charges over maximum reimbursement of $50/qualifying class7
Authorized organ transplant services Unlimited Not covered out-of-network
Footnotes can be found on page 21.2 3

Plan namesOffice visit copay PPO network
Individual deductible1
Family deductible1
Individual out-of-pocket maximum2
Family out-of-pocket maximum2
PPO network
Out-of-network
PPO network
Out-of-network
PPO network
Out-of-network
PPO network
Out-of-network
HD15008060w/HD80 20% $1,500 $3,000 $3,000 $6,000 $3,000 $9,000 $6,000 $18,000 HD20008060w/HD80 20% $2,000 $4,000 $4,000 $8,000 $4,000 $12,000 $8,000 $24,000 HD25008060w/HD80 20% $2,500 $5,000 $5,000 $10,000 $5,000 $15,000 $10,000 $30,000 HD50008060w/HD80 20% $5,000 $10,000 $10,000 $20,000 $6,000 $18,000 $12,000 $36,000
Prescription benefits – NMSAHD80
Supplemental prescription benefit schedule for High Deductible Health Plans. This pharmacy rider is included with all HDHP medical plans. Medical plan deductible applies. Once the deductible has been met, prescription benefits are covered with a 20% coinsurance for all tiers.
Specialty Pharmacy
Certain drugs identified on the PDL with the designation “SP” are classified as Specialty Pharmacy drugs. Specialty Pharmacy drugs are high-cost biologic, injectable and oral drugs typically dispensed through a limited network of pharmacies and have significantly higher cost than traditional pharmacy benefit drugs. Specialty Pharmacy medications are shipped to the member or their provider from an approved Specialty Pharmacy vendor.
4 5
High Deductible Health PlansOur HSA-qualified High Deductible Health plans allow your clients or their employees to
open a tax-deferred Health Savings Account that employees can use to pay for medical
expenses not covered by the health plan. HDHps may encourage employees to better
understand health care costs and to make cost-effective medical choices, reducing overall
medical costs.
All High Deductible Health plans include coverage for prescription drugs. prescription drug
costs are subject to the plan deductible and apply to the out-of-pocket maximum. Well Net
benefits are not included in High Deductible Health plans.

Physician / professional / outpatient care PPO network Out-of-networkPreventive care No charge 40% MAA3
Physician services – office call to providers in family practice, pediatrics, internal medicine, general practice, obstetrics/gynecology
20% contract rate 40% MAA
Physician services – office call to providers in specialties other than above 20% contract rate 40% MAA
Physician services – urgent care center 20% contract rate 20% MAA
Physician hospital visits 20% contract rate 40% MAA
Diagnostic X-ray / EKG / ultrasound 20% contract rate 40% MAA
Diagnostic laboratory tests 20% contract rate 40% MAA
CT / MRI / PET / SPECT / EEG / Holter monitor / stress test 20% contract rate 40% MAA
Allergy and therapeutic injections 20% contract rate 40% MAA
Maternity delivery care (professional services only) 20% contract rate 40% MAA
Outpatient rehabilitation therapy – 30 days/year max 20% contract rate 40% MAA
Outpatient at ambulatory surgery center (ASC) 15% contract rate 40% MAA
Outpatient at hospital-based facility 20% contract rate 40% MAA
Hospital careInpatient services4 20% contract rate 40% MAA
Inpatient rehabilitation therapy – 30 days/year max 20% contract rate 40% MAA
Emergency servicesOutpatient emergency room services 20% contract rate 20%
Inpatient admission from emergency room 20% contract rate 20%
Emergency ground ambulance transport – 3 trips/year max 20%
Emergency air ambulance transport – 1 trip/year max 20%
Behaviorial services – chemical dependency and mental or nervous conditionsPhysician services – office call5 20% contract rate 40% MAA
Outpatient center5 20% contract rate 40% MAA
Inpatient services5 20% contract rate 40% MAA
Other servicesDurable medical equipment 20% contract rate 40% MAA
Prosthetic devices / orthotic devices 20% contract rate 40% MAA
Medical supplies (including allergy serums and injected substances) 20% contract rate 40% MAA
Diabetes management – one initial program 20% contract rate 40% MAA
Blood, blood plasma, blood derivatives 20% contract rate 40% MAA
TMJ services – $500/lifetime max 50% contract rate 50% MAA
Home infusion therapy 20% contract rate 40% MAA
Outpatient chemotherapy (non-oral anticancer medications and administration)
20% contract rate 40% MAA
Skilled nursing facility care – 60 days/year max 20% contract rate 40% MAA
Hospice services 20% contract rate 40% MAA
Home health visits 20% contract rate 40% MAA
Health education – $150/year max for all qualifying classes Not covered Not covered out-of-network
Authorized organ transplant services Unlimited Not covered out-of-network
Footnotes can be found on page 21.4 5

PPO AdvantageppO Advantage, our most popular plan design, balances strong member coverage with
lower employer costs than ppO Advantage LX. The deductible is waived for routine
diagnostic lab and imaging services while there is a higher member cost-share on other
imaging categories such as MRIs, CT scans and EEGs. ppO Advantage has our widest range
of deductible options.
Plan namesOffice visit copay PPO network
Individual deductible1
Family deductible1 Coinsurance
Individual out-of-pocket maximum2
Family out-of-pocket maximum2
PPO network (ASC/all other)
Out-of-network coinsurance
In- and out-of- network, combined
In- and out-of- network, combined
A15-250-2-2750 $15$250 combined
$500 combined
15% / 20% 40% $2,750 $5,500
A20-500-2-3000 $20 $500 combined
$1,000 combined
15% / 20% 40% $3,000 $6,000
A20-750-2-3750 $20 $750 combined
$1,500 combined
15% / 20% 40% $3,750 $7,500
A20-1000-2-4000 $20 $1,000 combined
$2,000 combined
15% / 20% 40% $4,000 $8,000
A25-1500-2-4500 $25 $1,500 combined
$3,000 combined
15% / 20% 40% $4,500 $9,000
A20-2000-2-5000 $20 $2,000 combined
$4,000 combined
15% / 20% 40% $5,000 $10,000
A30-3000-2-6000 $30 $3,000 combined
$6,000 combined
15% / 20% 40% $6,000 $12,000
A35-5000-2-6350 $35 $5,000 combined
$10,000 combined
15% / 20% 40% $6,350 $12,700
A30-1500-3-4500 $30 $1,500 combined
$3,000 combined
25% / 30% 50% $4,500 $9,000
A30-2500-3-6350 $30 $2,500 combined
$5,000 combined
25% / 30% 50% $6,350 $12,700
6 7
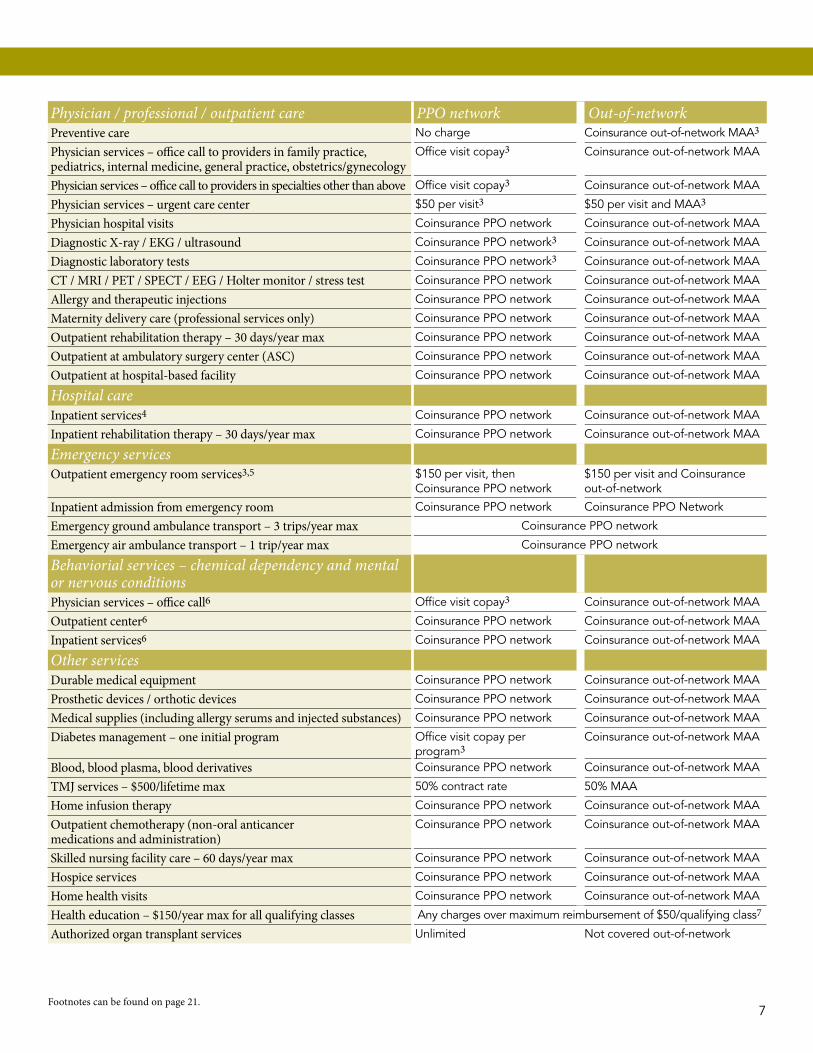
Physician / professional / outpatient care PPO network Out-of-networkPreventive care No charge Coinsurance out-of-network MAA3
Physician services – office call to providers in family practice, pediatrics, internal medicine, general practice, obstetrics/gynecology
Office visit copay3 Coinsurance out-of-network MAA
Physician services – office call to providers in specialties other than above Office visit copay3 Coinsurance out-of-network MAA
Physician services – urgent care center $50 per visit3 $50 per visit and MAA3
Physician hospital visits Coinsurance ppO network Coinsurance out-of-network MAA
Diagnostic X-ray / EKG / ultrasound Coinsurance ppO network3 Coinsurance out-of-network MAA
Diagnostic laboratory tests Coinsurance ppO network3 Coinsurance out-of-network MAA
CT / MRI / PET / SPECT / EEG / Holter monitor / stress test Coinsurance ppO network Coinsurance out-of-network MAA
Allergy and therapeutic injections Coinsurance ppO network Coinsurance out-of-network MAA
Maternity delivery care (professional services only) Coinsurance ppO network Coinsurance out-of-network MAA
Outpatient rehabilitation therapy – 30 days/year max Coinsurance ppO network Coinsurance out-of-network MAA
Outpatient at ambulatory surgery center (ASC) Coinsurance ppO network Coinsurance out-of-network MAA
Outpatient at hospital-based facility Coinsurance ppO network Coinsurance out-of-network MAA
Hospital careInpatient services4 Coinsurance ppO network Coinsurance out-of-network MAA
Inpatient rehabilitation therapy – 30 days/year max Coinsurance ppO network Coinsurance out-of-network MAA
Emergency servicesOutpatient emergency room services3,5 $150 per visit, then
Coinsurance ppO network$150 per visit and Coinsurance out-of-network
Inpatient admission from emergency room Coinsurance ppO network Coinsurance ppO Network
Emergency ground ambulance transport – 3 trips/year max Coinsurance ppO network
Emergency air ambulance transport – 1 trip/year max Coinsurance ppO network
Behaviorial services – chemical dependency and mental or nervous conditionsPhysician services – office call6 Office visit copay3 Coinsurance out-of-network MAA
Outpatient center6 Coinsurance ppO network Coinsurance out-of-network MAA
Inpatient services6 Coinsurance ppO network Coinsurance out-of-network MAA
Other servicesDurable medical equipment Coinsurance ppO network Coinsurance out-of-network MAA
Prosthetic devices / orthotic devices Coinsurance ppO network Coinsurance out-of-network MAA
Medical supplies (including allergy serums and injected substances) Coinsurance ppO network Coinsurance out-of-network MAA
Diabetes management – one initial program Office visit copay per program3
Coinsurance out-of-network MAA
Blood, blood plasma, blood derivatives Coinsurance ppO network Coinsurance out-of-network MAA
TMJ services – $500/lifetime max 50% contract rate 50% MAA
Home infusion therapy Coinsurance ppO network Coinsurance out-of-network MAA
Outpatient chemotherapy (non-oral anticancer medications and administration)
Coinsurance ppO network Coinsurance out-of-network MAA
Skilled nursing facility care – 60 days/year max Coinsurance ppO network Coinsurance out-of-network MAA
Hospice services Coinsurance ppO network Coinsurance out-of-network MAA
Home health visits Coinsurance ppO network Coinsurance out-of-network MAA
Health education – $150/year max for all qualifying classes Any charges over maximum reimbursement of $50/qualifying class7
Authorized organ transplant services Unlimited Not covered out-of-network
Footnotes can be found on page 21.6 7

PPO FiftyOur ppO Fifty plans offer a more affordable option for employers while still offering
employees coverage from the start. We now offer ppO Fifty plans with and without a
deductible. Covered employees simply pay 50 percent coinsurance. Then, if an employee
has high medical expenses during the year, Health Net pays 100 percent for covered
expenses once the out-of-pocket maximum is met (ppO network only, MAA applies
out-of-network).
Plan namesOffice visit cost-share PPO network
Individual deductible1
Family deductible1
Individual out-of-pocket maximum2
Family out-of-pocket maximum2
PPO network
Out-of-network
PPO network
Out-of-network
PPO network
Out-of-network
PPO network
Out-of-network
1000-50/50-3500 50% $1,000 $3,000 $2,000 $6,000 $3,500 $10,500 $7,000 $21,000
2000-50/50-4500 50% $2,000 $6,000 $4,000 $12,000 $4,500 $13,500 $9,000 $27,000
50/50-2500 50% No deductible No deductible $2,500 $7,500 $5,000 $15,000
50/50-5000 50% No deductible No deductible $5,000 $15,000 $10,000 $30,000
40-50/50-3000 40% No deductible No deductible $3,000 $9,000 $6,000 $18,000
8 9

Physician / professional / outpatient care PPO network Out-of-networkPreventive care No charge 50% MAA
Physician services – office call to providers in family practice, pediatrics, internal medicine, general practice, obstetrics/gynecology
Office visit cost-share 50% MAA
Physician services – office call to providers in specialties other than above Office visit cost-share 50% MAA
Physician services – urgent care center 50% contract rate 50% MAA
Physician hospital visits 50% contract rate 50% MAA
Diagnostic X-ray / EKG / ultrasound 50% contract rate 50% MAA
Diagnostic laboratory tests 50% contract rate 50% MAA
CT / MRI / PET / SPECT / EEG / Holter monitor / stress test 50% contract rate 50% MAA
Allergy and therapeutic injections 50% contract rate 50% MAA
Maternity delivery care (professional services only) 50% contract rate 50% MAA
Outpatient rehabilitation therapy – 30 days/year max 50% contract rate 50% MAA
Outpatient at ambulatory surgery center (ASC) 45% contract rate 50% MAA
Outpatient at hospital-based facility 50% contract rate 50% MAA
Hospital careInpatient services3 50% contract rate 50%
Inpatient rehabilitation therapy – 30 days/year max 50% contract rate 50%
Emergency servicesOutpatient emergency room services 50% contract rate 50%
Inpatient admission from emergency room 50% contract rate 50%
Emergency ground ambulance transport – 3 trips/year max 50%
Emergency air ambulance transport – 1 trip/year max 50%
Behaviorial services – chemical dependency and mental or nervous conditionsPhysician services – office call4 Office visit cost-share 50% MAA
Outpatient center4 50% contract rate 50% MAA
Inpatient services4 50% contract rate 50% MAA
Other servicesDurable medical equipment 50% contract rate 50% MAA
Prosthetic devices / orthotic devices 50% contract rate 50% MAA
Medical supplies (including allergy serums and injected substances) 50% contract rate 50% MAA
Diabetes management – one initial program Office visit cost-share per program 50% MAA
Blood, blood plasma, blood derivatives 50% contract rate 50% MAA
TMJ services – $500/lifetime max 50% contract rate 50% MAA
Home infusion therapy 50% contract rate 50% MAA
Outpatient chemotherapy (non-oral anticancer medications and administration)
50% contract rate 50% MAA
Skilled nursing facility care – 60 days/year max 50% contract rate 50% MAA
Hospice services 50% contract rate 50% MAA
Home health visits 50% contract rate 50% MAA
Health education – $150/year max for all qualifying classes Any charges over maximum reimbursement of $50/qualifying class5
Authorized organ transplant services Unlimited Not covered out-of-network
Footnotes can be found on page 21.8 9
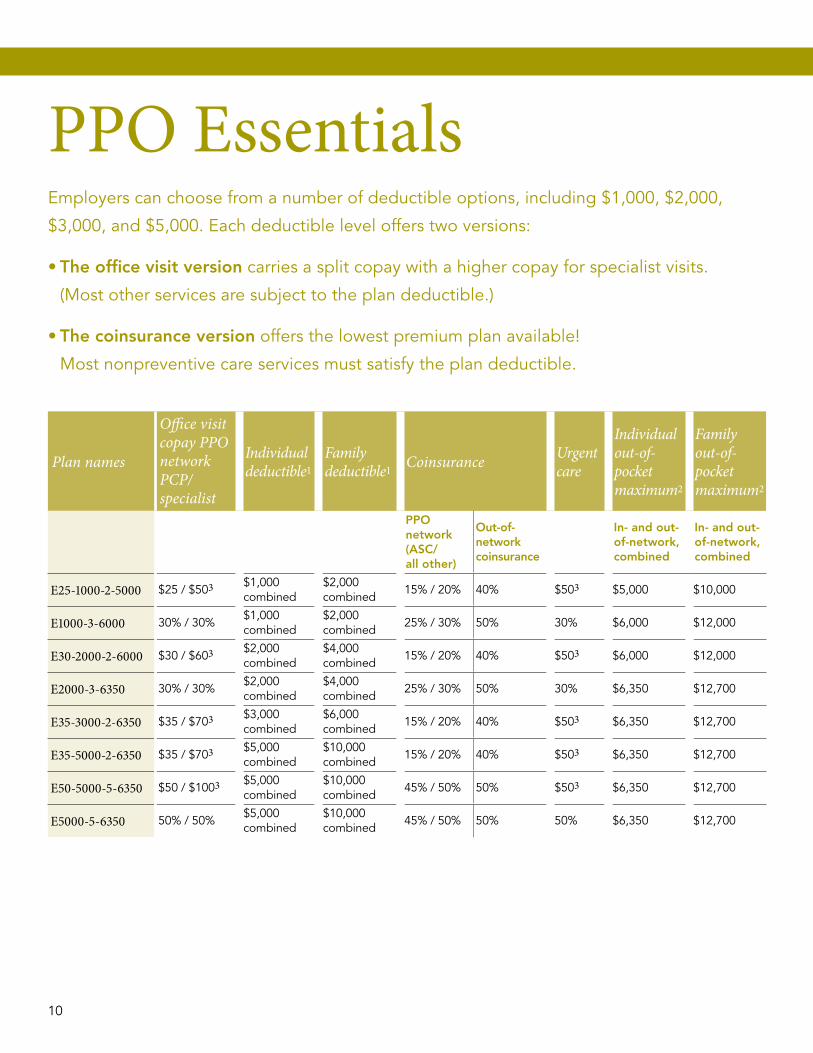
PPO EssentialsEmployers can choose from a number of deductible options, including $1,000, $2,000,
$3,000, and $5,000. Each deductible level offers two versions:
• The office visit version carries a split copay with a higher copay for specialist visits.
(Most other services are subject to the plan deductible.)
• The coinsurance version offers the lowest premium plan available!
Most nonpreventive care services must satisfy the plan deductible.
Plan names
Office visit copay PPO network PCP/specialist
Individual deductible1
Family deductible1 Coinsurance Urgent
care
Individual out-of-pocket maximum2
Family out-of-pocket maximum2
PPO network (ASC/ all other)
Out-of-network coinsurance
In- and out-of-network, combined
In- and out-of-network, combined
E25-1000-2-5000 $25 / $503 $1,000 combined
$2,000 combined
15% / 20% 40% $503 $5,000 $10,000
E1000-3-6000 30% / 30%$1,000 combined
$2,000 combined
25% / 30% 50% 30% $6,000 $12,000
E30-2000-2-6000 $30 / $603 $2,000 combined
$4,000 combined
15% / 20% 40% $503 $6,000 $12,000
E2000-3-6350 30% / 30%$2,000 combined
$4,000 combined
25% / 30% 50% 30% $6,350 $12,700
E35-3000-2-6350 $35 / $703 $3,000 combined
$6,000 combined
15% / 20% 40% $503 $6,350 $12,700
E35-5000-2-6350 $35 / $703 $5,000 combined
$10,000 combined
15% / 20% 40% $503 $6,350 $12,700
E50-5000-5-6350 $50 / $1003 $5,000 combined
$10,000 combined
45% / 50% 50% $503 $6,350 $12,700
E5000-5-6350 50% / 50%$5,000 combined
$10,000 combined
45% / 50% 50% 50% $6,350 $12,700
10 11
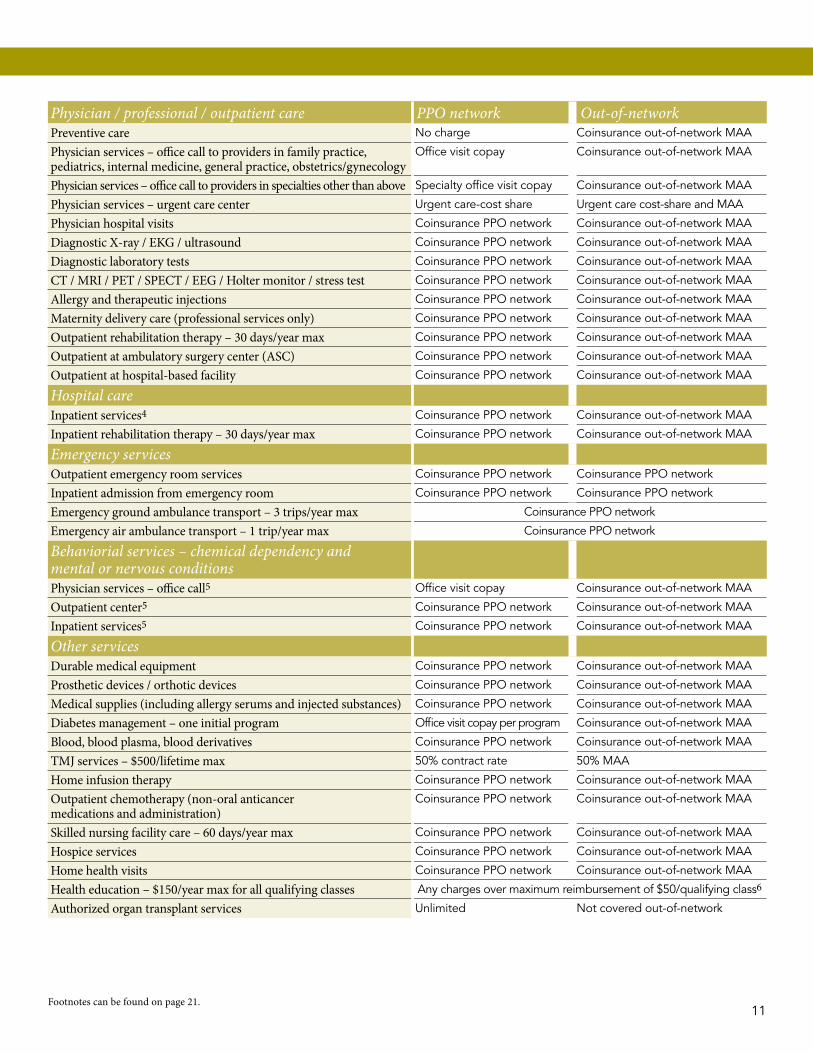
Physician / professional / outpatient care PPO network Out-of-networkPreventive care No charge Coinsurance out-of-network MAA
Physician services – office call to providers in family practice, pediatrics, internal medicine, general practice, obstetrics/gynecology
Office visit copay Coinsurance out-of-network MAA
Physician services – office call to providers in specialties other than above Specialty office visit copay Coinsurance out-of-network MAA
Physician services – urgent care center Urgent care-cost share Urgent care cost-share and MAA
Physician hospital visits Coinsurance ppO network Coinsurance out-of-network MAA
Diagnostic X-ray / EKG / ultrasound Coinsurance ppO network Coinsurance out-of-network MAA
Diagnostic laboratory tests Coinsurance ppO network Coinsurance out-of-network MAA
CT / MRI / PET / SPECT / EEG / Holter monitor / stress test Coinsurance ppO network Coinsurance out-of-network MAA
Allergy and therapeutic injections Coinsurance ppO network Coinsurance out-of-network MAA
Maternity delivery care (professional services only) Coinsurance ppO network Coinsurance out-of-network MAA
Outpatient rehabilitation therapy – 30 days/year max Coinsurance ppO network Coinsurance out-of-network MAA
Outpatient at ambulatory surgery center (ASC) Coinsurance ppO network Coinsurance out-of-network MAA
Outpatient at hospital-based facility Coinsurance ppO network Coinsurance out-of-network MAA
Hospital careInpatient services4 Coinsurance ppO network Coinsurance out-of-network MAA
Inpatient rehabilitation therapy – 30 days/year max Coinsurance ppO network Coinsurance out-of-network MAA
Emergency servicesOutpatient emergency room services Coinsurance ppO network Coinsurance ppO network
Inpatient admission from emergency room Coinsurance ppO network Coinsurance ppO network
Emergency ground ambulance transport – 3 trips/year max Coinsurance ppO network
Emergency air ambulance transport – 1 trip/year max Coinsurance ppO network
Behaviorial services – chemical dependency and mental or nervous conditionsPhysician services – office call5 Office visit copay Coinsurance out-of-network MAA
Outpatient center5 Coinsurance ppO network Coinsurance out-of-network MAA
Inpatient services5 Coinsurance ppO network Coinsurance out-of-network MAA
Other servicesDurable medical equipment Coinsurance ppO network Coinsurance out-of-network MAA
Prosthetic devices / orthotic devices Coinsurance ppO network Coinsurance out-of-network MAA
Medical supplies (including allergy serums and injected substances) Coinsurance ppO network Coinsurance out-of-network MAA
Diabetes management – one initial program Office visit copay per program Coinsurance out-of-network MAA
Blood, blood plasma, blood derivatives Coinsurance ppO network Coinsurance out-of-network MAA
TMJ services – $500/lifetime max 50% contract rate 50% MAA
Home infusion therapy Coinsurance ppO network Coinsurance out-of-network MAA
Outpatient chemotherapy (non-oral anticancer medications and administration)
Coinsurance ppO network Coinsurance out-of-network MAA
Skilled nursing facility care – 60 days/year max Coinsurance ppO network Coinsurance out-of-network MAA
Hospice services Coinsurance ppO network Coinsurance out-of-network MAA
Home health visits Coinsurance ppO network Coinsurance out-of-network MAA
Health education – $150/year max for all qualifying classes Any charges over maximum reimbursement of $50/qualifying class6
Authorized organ transplant services Unlimited Not covered out-of-network
Footnotes can be found on page 21.10 11

Orally-administered anticancer medications and pharmacy-dispensed women’s contraceptive methods are covered at no charge to the member when dispensed at a retail pharmacy. Mail order may not be available; please check the pharmacy plan summary for details.
Specialty PharmacyCertain drugs identified on the PDL with the designation “SP” are classified as Specialty Pharmacy drugs. Specialty Pharmacy drugs are high-cost biologic, injectable and oral drugs typically dispensed through a limited network of pharmacies and have significantly higher cost than traditional pharmacy benefit drugs. Specialty Pharmacy medications are shipped to the member or their provider from an approved Specialty Pharmacy vendor. Unless otherwise indicated, the member share on Specialty Pharmacy drugs is:
Pay 10% to a maximum of $100 (per fill, up to a 30-day supply).
For calendar year 2014, pharmacy benefits will not be included in the total out-of-pocket maximums under the Safe Harbor provision of the ACA.
PharmacyHealth Net uses a prescription drug formulary called the preferred Drug List (pDL) for therapeutic drugs so our members receive quality at reasonable costs. A committee that includes pharmacists and providers from various medical specialities develops our pDL. To view the current pDL for your state, go to http://broker.healthnet.com > Pharmacy Plan Information (bottom left) > Drug Lists. Some drugs require prior authorization. A member may call our Customer Contact Center with any questions. If a member regularly takes prescription medications, we have a mail-order program that provides an easy way to order up to a 90-day supply.
Prescription benefit NMSS/L10–20–40 NMSS/L15–30–50 NMSS/L10-50-75
In pharmacy (30-day supply)
Mail order (90-day supply)
In pharmacy (30-day supply)
Mail order (90-day supply)
In pharmacy (30-day supply)
Mail order (90-day supply)
Tier 1 $10 $20 $15 $30 $10 $20Tier 2 $20 $40 $30 $60 $50 $100Tier 3 $40 $80 $50 $100 $75 $150SP See below See below See below
Prescription benefit NMSS/L15–35–60 NMSA15–30%–50% 5000M NMSA15–30%–50%
In pharmacy (30-day supply)
Mail order (90-day supply)
$5,000 out-of-pocket maximum per member, per year
No out-of-pocket maximum
In pharmacy (30-day supply)
Mail order (90-day supply)
In pharmacy (30-day supply)
Mail order (90-day supply)
Tier 1 $15 $30 $15 $30 $15 $30Tier 2 $35 $70 30% 30% 30% 30%Tier 3 $60 $120 50% 50% 50% 50%SP See below 50% N/A 50% N/A
12 13
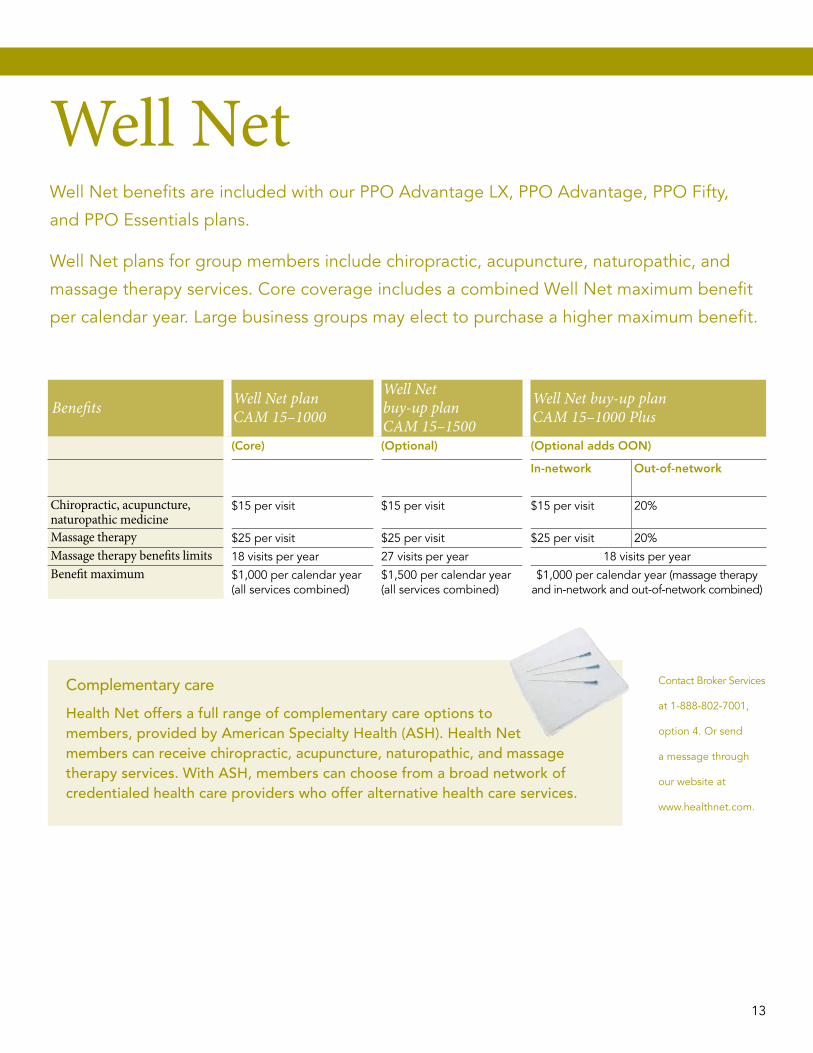
Well NetWell Net benefits are included with our ppO Advantage LX, ppO Advantage, ppO Fifty,
and ppO Essentials plans.
Well Net plans for group members include chiropractic, acupuncture, naturopathic, and
massage therapy services. Core coverage includes a combined Well Net maximum benefit
per calendar year. Large business groups may elect to purchase a higher maximum benefit.
Complementary care
Health Net offers a full range of complementary care options to members, provided by American Specialty Health (ASH). Health Net members can receive chiropractic, acupuncture, naturopathic, and massage therapy services. With ASH, members can choose from a broad network of credentialed health care providers who offer alternative health care services.
Contact Broker Services
at 1-888-802-7001,
option 4. Or send
a message through
our website at
www.healthnet.com.
Benefits Well Net plan CAM 15–1000
Well Net buy-up plan CAM 15–1500
Well Net buy-up plan CAM 15–1000 Plus
(Core) (Optional) (Optional adds OON)
In-network Out-of-network
Chiropractic, acupuncture, naturopathic medicine
$15 per visit $15 per visit $15 per visit 20%
Massage therapy $25 per visit $25 per visit $25 per visit 20%Massage therapy benefits limits 18 visits per year 27 visits per year 18 visits per yearBenefit maximum $1,000 per calendar year
(all services combined)$1,500 per calendar year (all services combined)
$1,000 per calendar year (massage therapy and in-network and out-of-network combined)
12 13

Health Net Dental underwriting guidelinesEligibility rules must be the same for medical and dental. Minimum employer contribution must be 50 percent of employee-only dental coverage.
Integrated – The enrollment between subscribers and dependents for dental and medical must match exactly. A minimum of 5 employees must enroll. A minimum of 10 employees must enroll on a plan with orthodontia.
Standalone – Dental-only coverage without medical. A minimum of 10 employees must enroll and 75 percent of those eligible must enroll.
Freestanding – The enrollments in medical and dental between subscribers and dependents do not have to match. A minimum of 10 employees must enroll, and 75 percent of those eligible must enroll.
Optional Dental
Essentials Dental
Benefits D50-16-500Annual deductible per person $50
Annual deductible per family N/A
Annual plan maximum per person $500
Lifetime orthodontic Not covered
Diagnostic and preventive1 100% in-network / 80% out-of-network
Basic services 60% in-network / 50% out-of-network
Endodontic, periodontal and oral surgery Not covered
Major services Not covered
Orthodontic services Not covered
Benefits D25-185- 1500
D25-1855-1500
D25-1855-2000
D50-185- 1000
D50-185- 1500
D50-185- 2000
D50-1855-2000
D100-185-1000
D100-185-1500
D100-185-2000
D100-1855-2000
Annual deductible per person $25 $25 $25 $50 $50 $50 $50 $100 $100 $100 $100
Annual deductible per family $75 $75 $75 $150 $150 $150 $150 $300 $300 $300 $300
Annual plan maximum per person $1,500 $1,500 $2,000 $1,000 $1,500 $2,000 $2,000 $1,000 $1,500 $2,000 $2,000
Lifetime orthodontic services per person Not covered $1,500 $2,000 Not covered Not covered Not covered $2,000 Not covered Not covered Not covered $2,000In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
Diagnostic and preventive1 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Basic services 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80%
Endodontic, periodontal and oral surgery 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80%
Major services 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50%
Orthodontic services Not covered 50% 50% Not covered Not covered Not covered 50% Not covered Not covered Not covered 50%
Benefits D50-1855-1500
D100-1855-1000
D50-185-1500V
D100-185-1000V
D100-555-1000V DP25-1855-1500 DP50-1855-1500 DP100-185-1000V
Annual deductible per person $50 $100 $50 $100 $100 $25 $50 $100
Annual deductible per family $150 $300 $150 $300 $300 $75 $150 $300
Annual plan maximum per person $1,500 $1,000 $1,500 $1,000 $1,000 $1,500 $1,500 $1,000
Lifetime orthodontic services per person $1,500 $1,000 Not covered Not covered Not covered $1,500 $1,500 Not coveredIn- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
In- and out- of-network
IN OON IN OON IN OON
Diagnostic and preventive1 100% 100% 100% 100% 50% 100% 80% 100% 80% 100% 80%
Basic services 80% 80% 80% 80% 50% 80% 60% 80% 60% 80% 60%
Endodontic, periodontal and oral surgery 80% 80% 50% 50% 50% 80% 60% 80% 60% 50% 50%
Major services 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50%
Orthodontic services 50% 50% Not covered Not covered Not covered 50% 50% 50% 50% Not covered
14 15

Christian Aparicio,Health Net We make using health care benefi ts simple.
Benefi ts D25-185-1500
D25-1855-1500
D25-1855-2000
D50-185-1000
D50-185-1500
D50-185-2000
D50-1855-2000
D100-185-1000
D100-185-1500
D100-185-2000
D100-1855-2000
Annual deductible per person $25 $25 $25 $50 $50 $50 $50 $100 $100 $100 $100
Annual deductible per family $75 $75 $75 $150 $150 $150 $150 $300 $300 $300 $300
Annual plan maximum per person $1,500 $1,500 $2,000 $1,000 $1,500 $2,000 $2,000 $1,000 $1,500 $2,000 $2,000
Lifetime orthodontic services per person Not covered $1,500 $2,000 Not covered Not covered Not covered $2,000 Not covered Not covered Not covered $2,000In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
Diagnostic and preventive1 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Basic services 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80%
Endodontic, periodontal and oral surgery 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80%
Major services 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50%
Orthodontic services Not covered 50% 50% Not covered Not covered Not covered 50% Not covered Not covered Not covered 50%
Benefi ts D50-1855-1500
D100-1855-1000
D50-185-1500V
D100-185-1000V
D100-555-1000V DP25-1855-1500 DP50-1855-1500 DP100-185-1000V
Annual deductible per person $50 $100 $50 $100 $100 $25 $50 $100
Annual deductible per family $150 $300 $150 $300 $300 $75 $150 $300
Annual plan maximum per person $1,500 $1,000 $1,500 $1,000 $1,000 $1,500 $1,500 $1,000
Lifetime orthodontic services per person $1,500 $1,000 Not covered Not covered Not covered $1,500 $1,500 Not coveredIn- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
In- and out-of-network
IN OON IN OON IN OON
Diagnostic and preventive1 100% 100% 100% 100% 50% 100% 80% 100% 80% 100% 80%
Basic services 80% 80% 80% 80% 50% 80% 60% 80% 60% 80% 60%
Endodontic, periodontal and oral surgery 80% 80% 50% 50% 50% 80% 60% 80% 60% 50% 50%
Major services 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50%
Orthodontic services 50% 50% Not covered Not covered Not covered 50% 50% 50% 50% Not covered
Plus plans• Include orthodontia• Endodontics, periodontia and oral
surgery are reimbursed at tier 2 (Basic)• Hold harmless on MAA if network
provider used; otherwise, no benefi t distinction in- versus out-of-network
• MAA is 90th percentile of HIAA
Value plans• No orthodontia• Endodontics, periodontia and oral
surgery are covered at tier 3 (Major)• Hold harmless on MAA if network
provider used; otherwise, no benefi t distinction in- versus out-of-network
• MAA is 90th percentile of HIAA
Preferred• PPO-type dental plan, higher benefi t
in network• DP 25 and DP 50: Endodontics,
periodontia and oral surgery are covered at tier 2 (Basic) and include orthodontia
• DP 100: Endodontics, periodontia and oral surgery are covered at tier 3 (Major) and do not include orthodontia
• MAA is 90th percentile of HIAA for OON
Essentials• No orthodontia • Covers preventive and basic services
only, no major
14 15
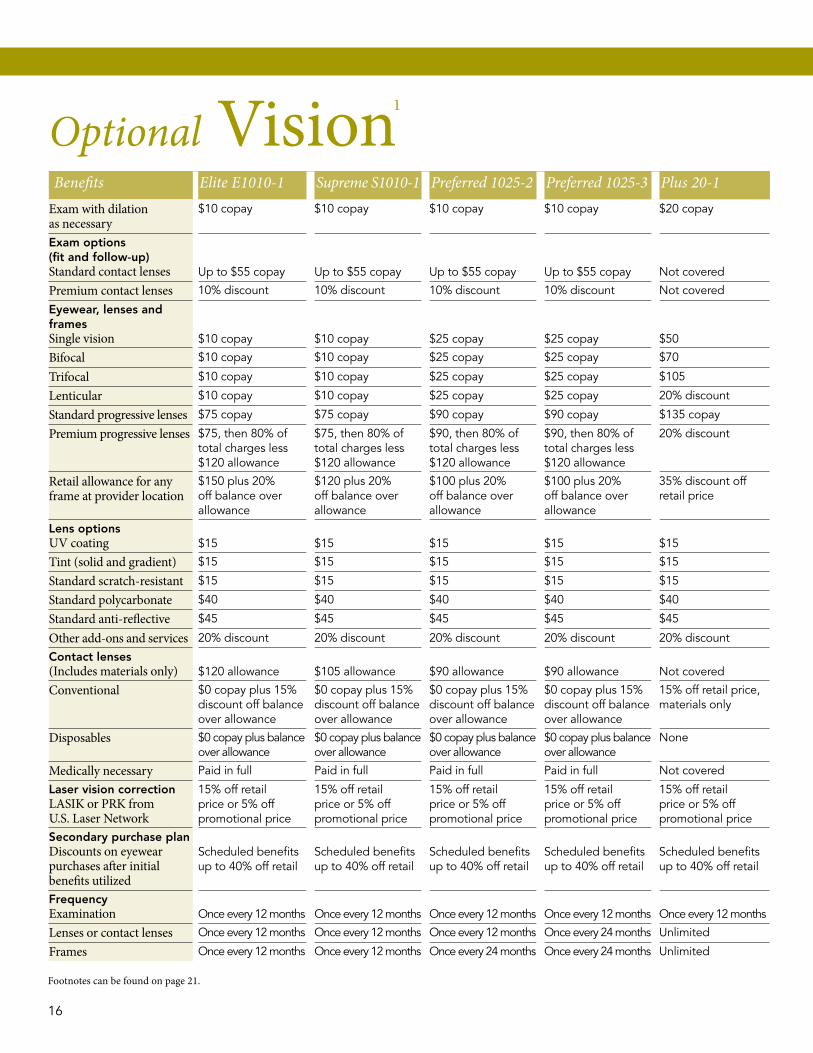
Benefits Elite E1010-1 Supreme S1010-1 Preferred 1025-2 Preferred 1025-3 Plus 20-1Exam with dilation as necessary
$10 copay $10 copay $10 copay $10 copay $20 copay
Exam options (fit and follow-up)Standard contact lenses Up to $55 copay Up to $55 copay Up to $55 copay Up to $55 copay Not covered
Premium contact lenses 10% discount 10% discount 10% discount 10% discount Not covered
Eyewear, lenses and framesSingle vision $10 copay $10 copay $25 copay $25 copay $50
Bifocal $10 copay $10 copay $25 copay $25 copay $70
Trifocal $10 copay $10 copay $25 copay $25 copay $105
Lenticular $10 copay $10 copay $25 copay $25 copay 20% discount
Standard progressive lenses $75 copay $75 copay $90 copay $90 copay $135 copay
Premium progressive lenses $75, then 80% of total charges less $120 allowance
$75, then 80% of total charges less $120 allowance
$90, then 80% of total charges less $120 allowance
$90, then 80% of total charges less $120 allowance
20% discount
Retail allowance for anyframe at provider location
$150 plus 20% off balance over allowance
$120 plus 20% off balance over allowance
$100 plus 20% off balance over allowance
$100 plus 20% off balance over allowance
35% discount off retail price
Lens optionsUV coating $15 $15 $15 $15 $15
Tint (solid and gradient) $15 $15 $15 $15 $15
Standard scratch-resistant $15 $15 $15 $15 $15
Standard polycarbonate $40 $40 $40 $40 $40
Standard anti-reflective $45 $45 $45 $45 $45
Other add-ons and services 20% discount 20% discount 20% discount 20% discount 20% discount
Contact lenses(Includes materials only) $120 allowance $105 allowance $90 allowance $90 allowance Not covered
Conventional $0 copay plus 15%discount off balance over allowance
$0 copay plus 15% discount off balance over allowance
$0 copay plus 15% discount off balance over allowance
$0 copay plus 15% discount off balance over allowance
15% off retail price,materials only
Disposables $0 copay plus balance over allowance
$0 copay plus balance over allowance
$0 copay plus balance over allowance
$0 copay plus balance over allowance
None
Medically necessary paid in full paid in full paid in full paid in full Not covered
Laser vision correctionLASIK or PRK from U.S. Laser Network
15% off retail price or 5% off promotional price
15% off retail price or 5% off promotional price
15% off retail price or 5% off promotional price
15% off retail price or 5% off promotional price
15% off retail price or 5% off promotional price
Secondary purchase planDiscounts on eyewear purchases after initial benefits utilized
Scheduled benefitsup to 40% off retail
Scheduled benefitsup to 40% off retail
Scheduled benefitsup to 40% off retail
Scheduled benefitsup to 40% off retail
Scheduled benefitsup to 40% off retail
FrequencyExamination Once every 12 months Once every 12 months Once every 12 months Once every 12 months Once every 12 months
Lenses or contact lenses Once every 12 months Once every 12 months Once every 12 months Once every 24 months Unlimited
Frames Once every 12 months Once every 12 months Once every 24 months Once every 24 months Unlimited
Optional Vision1
Footnotes can be found on page 21.
16 17

Power Wellness!Leverage Decision Power® today for a healthy, productive workforce
Health Net’s Power Wellness options for employers
35.7% of U.S. adults
are obese1 – A person
who maintains a
healthy weight saves
$1,400 annually
(on average) in
medical costs2.
Wellness programs have the potential to improve the health and well-being
of individual employees. But to foster a healthy workforce and see meaningful
results, employers need to understand their population’s health risks, so they
can offer the right programs and implement them well. Health Net can help.
Start-Up – Health assessment packageA convenient package that can help any organization committed to making healthy changes get started building their employee wellness program. Includes:
• A wellness toolkit to help employers promote their health risk assessment initiative and take the next steps to wellness.
• Reporting on aggregate Health Risk Questionnaire (HRQ) results for a deeper understanding of the organization’s wellness needs (to ensure confidentiality, 50+ completions are required).
Screenings – Biometric screenings packageHealth professionals from our trusted wellness partner can come to the workplace to help employees gain a deeper and more accurate understanding of their health. Employers will have access to discounts on these valued services through Health Net’s preferred pricing. Includes everything in our Start-Up package, plus onsite biometric screenings, with:
• Fingerstick test of total cholesterol (TC), HDL, TC/HDL ratio, and blood glucose.• Body mass index from self-reported height and weight.• Blood pressure and pulse readings.• Feedback and counseling throughout the screening process, with reminders for high-risk
employees to follow up with their physician.
Connect – Primary care physician (PCP) engagement packageThis package encourages employees to learn more about their health and make a connection by reaching out to their pCp with their HRQ results. Employers will have access to discounts on these valued services through Health Net’s preferred pricing. Includes everything in our Start-Up package, plus:
• A convenient, integrated incentive program, offering gift cards (employers choose the value, and are responsible for costs) for employees who complete the HRQ and visit their pCp to discuss the results.
16 17

Health Net members already have access to a broad range of wellness resources through Decision Power. Our Power Wellness packages help employers harness and build on those resources to meet the workplace wellness goals – Because when employees know their unique health risks, they can make healthier choices and live better.
Power Wellness is designed for employers with company policies that encourage healthy behaviors and strong leadership support for employee wellness. Talk to your Health Net representative to find out which package is the best fit for your clients. Employers may even choose to combine packages to optimize their results.
We’ll help you bring the power of wellness to your clients’ workforce.
Almost 67 million
Americans have high
blood pressure –
High blood pressure
accounts for nearly
$131 billion in direct
health care costs
each year3.
1 Cynthia L. Ogden et al., “Prevalence of Obesity in the United States, 2009–2010,” NCHS Data Brief No. 82 (January 2012), accessed 27 February 2013, http://www.cdc.gov/nchs/data/databriefs/db82.pdf.
2“Adult obesity facts,” CDC.gov, accessed 27 February 2013, http://www.cdc.gov/obesity/data/adult.html.3 “Getting blood pressure under control: High blood pressure is out of control for too many Americans,” CDC.gov, accessed 27 February 2013, http://www.cdc.gov/features/vitalsigns/hypertension/.
18 19

Health Net values your partnership and the opportunity to serve your clients who participate in our commercial employer groups. We’re committed to delivering exceptional service and operational excellence through a local and long-standing staff that processes claims, answers customer service inquiries, and services our employer groups. Our secure website off ers easy online access to services such as premium billing, enrollment and eligibility, and electronic funds transfer.
Decision Power®Health Net’s unique Decision Power® program off ers all members 24/7 access to clinicians who can answer questions and off er advice about chronic medical conditions and routine medical care.
Because employees have the peace of mind off ered by personal Decision Power clinicians, they can spend fewer hours worrying about their own or family members’ health conditions and be more productive.
Online enrollment and billingOnline enrollment and billing allows your clients to manage enrollments and changes, pay their bills and run reports at HealthNet.com.Th ese fast, paper-free solutions make it quick and easy to manage enrollment and billing administration with a single login. Not only will your clients save time with self-service,
they’ll have peace of mind knowing their employees’ details are managed with the latest security and privacy technology. Once registered, employers can:
• Enroll employees and dependents.
• Cancel and reinstate coverage.
• Pay bills online and schedule payments.
• Manage multiple payment options.
• Run enrollment reports.
Primary client administrators can create a user account by logging in to www.healthnet.com. From there, information is entered to:
• create a user profi le,
• grant access privileges, and
• set notifi cation preferences.
For fi rst time users, go to www.healthnet.com and click on “Register”. You will need the policy ID or group numbers. (If the policyholder ID number is less than 9 digits, add preceding zeroes as shown in this example: policyholder ID “1234” would become 000001234.) On future logins, your clients will click on Employer, then select Manage Enrollment or Pay My Bill. Th e account is now ready to use.
Employers Manage Th eir Health Plan – Online
Information at the
click of a button.
18 19
First time users go to www.healthnet.com and click “Register.” Returning users click “Login.”Th e menu at the top of the page is a great way to start:
• My Health Plan – Coverage and benefi t details.
• My Plan Activity – Claims, authorization, referrals, and appeals.
• ProviderSearch – Find a doctor, urgent care, hospitals, medical groups, other facilities, and ancillary services.
• Wellness Center – Resources for every stage of health.
• Member Support – Learn how to order ID cards, fi nd covered drugs, fi le a medical claim, and more.
Quick Links (under “How can we help you today?”)• My Coverage – Pull up benefi t specifi cs
about your plan.
• My Prescriptions – Find a pharmacy near your work or home.
• My Claims – View your explanation of benefi ts (EOB).
• My Account – Order ID card, print a temporary ID card and change your doctor.
Group Plan Members Doing More Online
Find member discounts, wellness programs, a hospital comparison tool, a treatment cost estimator, and more.
Rasika Patankar,Health NetWe champion solutions that are as unique as the clients you serve.
20 2120

Footnotes and disclaimers
This schedule presents general information only. Certain services require prior authorization or must be performed by a specialty care provider. Members refer to their contract and other benefit materials for details, limitations and exclusions.
Pages 2–31 Members must meet the specified deductible each calendar year (January 1 through December 31) before Health Net pays any claims.
2 The annual out-of-pocket maximum includes the annual deductible. After reaching the out-of-pocket maximum in a calendar year, we will pay covered services during the rest of that calendar year at 100% of our contract rates for PPO services and at 100% of MAA for out-of-network (OON) services. Member is still responsible for OON billed charges that exceed MAA.
3Deductible is waived. 4 Coinsurance for inpatient hospital services is applicable for each admission for the hospitalization of an adult, pediatric or newborn patient. If a newborn patient requires admission to an intermediate or intensive care nursery, a separate coinsurance for inpatient hospital services will apply.
5Copayment is waived if member is admitted.6 For mental health or chemical dependency services, members call 1-800-977-8216. 7Payments do not apply to the annual out-of-pocket maximum.
Pages 4–51 Members must meet the specified deductible each calendar year (January 1 through December 31) before Health Net pays any claims. Family coverage means the subscriber and spouse; the subscriber and child(ren); or the subscriber, spouse and child(ren). Under family coverage, each member’s covered expenses count toward the deductible, but the specified family coverage deductible must be met before Health Net pays any claims.
2 The annual out-of-pocket maximum includes the annual deductible. After reaching the out-of-pocket maximum in a calendar year, we will pay covered services during the rest of that calendar year at 100% of our contract rates for PPO services and at 100% of MAA for out-of-network (OON) services. Member is still responsible for OON billed charges that exceed MAA.
3Deductible is waived.4 Coinsurance for inpatient hospital services is applicable for each admission for the hospitalization of an adult, pediatric or newborn patient. If a newborn patient requires admission to an intermediate or intensive care nursery, a separate coinsurance for inpatient hospital services will apply.
5 For mental health or chemical dependency services, members call 1-800-977-8216.
Pages 6–71 Members must meet the specified deductible each calendar year (January 1 through December 31) before Health Net pays any claims.
2 The annual out-of-pocket maximum includes the annual deductible. After reaching the out-of-pocket maximum in a calendar year, we will pay covered services during the rest of that calendar year at 100% of our contract rates for PPO services and at 100% of MAA for out-of-network (OON) services. Member is still responsible for OON billed charges that exceed MAA.
3Deductible is waived.4 Coinsurance for inpatient hospital services is applicable for each admission for the hospitalization of an adult, pediatric or newborn patient. If a newborn patient requires admission to an intermediate or intensive care nursery, a separate coinsurance for inpatient hospital services will apply.
5Copayment is waived if member is admitted.6 For mental health or chemical dependency services, members call 1-800-977-8216. 7Payments do not apply to the annual out-of-pocket maximum.
Pages 8–91 Members must meet the specified deductible each calendar year (January 1 through December 31) before Health Net pays any claims.
2 The annual out-of-pocket maximum includes the annual deductible. After reaching the out-of-pocket maximum in a calendar year, we will pay covered services during the rest of that calendar year at 100% of our contract rates for PPO services and at 100% of MAA for out-of-network (OON) services. Member is still responsible for OON billed charges that exceed MAA.
3 Coinsurance for inpatient hospital services is applicable for each admission for the hospitalization of an adult, pediatric or newborn patient. If a newborn patient requires admission to an intermediate or intensive care nursery, a separate coinsurance for inpatient hospital services will apply.
4 To prior authorize mental health or chemical dependency services, members call 1-800-977-8216.
5Payments do not apply to the annual out-of-pocket maximum.
Pages 10–111 Members must meet the specified deductible each calendar year (January 1 through December 31) before Health Net pays any claims.
2 The annual out-of-pocket maximum includes the annual deductible. After reaching the out-of-pocket maximum in a calendar year, we will pay covered services during the rest of that calendar year at 100% of our contract rates for PPO services and at 100% of MAA for out-of-network (OON) services. Member is still responsible for OON billed charges that exceed MAA.
3Deductible is waived.4 Coinsurance for inpatient hospital services is applicable for each admission for the hospitalization of an adult, pediatric or newborn patient. If a newborn patient requires admission to an intermediate or intensive care nursery, a separate coinsurance for inpatient hospital services will apply.
5For mental health or chemical dependency services, members call 1-800-977-8216. 6Payments do not apply to the annual out-of-pocket maximum.
Page 14–151The deductible does not apply to diagnostic and preventive services.
Page 161 Members receive an out-of-network allowance for all plans (except Plus 20-1), including exam with dilation as necessary up to a $40 allowance; standard plastic lenses up to allowances of $40 (single vision), $60 (bifocal) or $80 (trifocal or lenticular), as applicable; retail allowance for any frame at provider location up to a $45 allowance; and contact lenses up to a $105 allowance. Refer to your contract for terms and conditions of coverage.
Members will receive a 20 percent discount on remaining balance beyond plan coverage at participating providers, which may not be combined with any other discounts or promotional offers. The discount does not apply to the provider’s professional services or to contact lenses. Retail prices may vary by location. Discounts do not apply for benefits provided by other group benefit plans. Allowances are one-time-use benefits; no remaining balance. Lost or broken materials are not covered.
Group Plan Members Doing More Online
20 21

For more information please contactHealth Net Health Plan of Oregon, Inc.13221 SW 68th Pkwy., Ste. 200Tigard, OR 972231-888-802-7001
Broker services Monday through Friday, 7:30 a.m. to 5:00 p.m. 1-888-802-7001, option 4
Assistance for the hearing and speech impairedMonday through Friday, 8:00 a.m. to 5:00 p.m. TTY/TDD 1-888-802-7122
www.healthnet.com
When services are performed by a provider who is not in our ppO network, your expenses include a calendar year deductible, fixed dollar amounts for certain services, and a fixed percentage of Maximum Allowable Amount (MAA) rates for other services. We pay out-of-network providers based on MAA rates, not on billed amounts. MAA rates may often be less than the amount a provider bills for a service. Out-of-network providers may therefore hold you responsible for amounts they charge that exceed the MAA rates we pay. Amounts that exceed our MAA rates are not covered and do not apply to your annual out-of-pocket maximum. Your responsibility for any amounts that exceed our MAA payment is shown on this schedule as MAA.
This document is only a summary of health coverage. You have the right to view the plan Contract. To obtain a copy of this document, contact your Health Net Sales Representative at 1-888-802-7001. The plan Contract, which a member will automatically receive after enrolling, contains the terms and conditions, as well as the governing and exact contractual provisions of Health Net Health plan of Oregon, Inc. coverage. This brochure presents general information only. Certain services require prior authorization or must be performed by a specialty care provider. Refer to your contract and other benefit materials for details, limitations and exclusions.
You have access to Decision power through your current enrollment with Health Net Health plan of Oregon, Inc. and Health Net Life Insurance Company.
Decision power is not part of Health Net’s commercial medical benefit plans. It is not affiliated with Health Net’s provider network, and it may be revised or withdrawn without notice. Decision power services, including clinicians, are additional resources that Health Net makes available to enrollees enrollees of the above listed Health Net companies.
6029536 OR106115 (9/13) Health Net Health plan of Oregon, Inc. and Health Net Life Insurance Company are subsidiaries of Health Net, Inc. Health Net and Decision power are registered service marks of Health Net, Inc. All other identified trademarks/service marks remain the property of their respective companies. All rights reserved.










![ALASKA COMPREHENSIVE HEALTH INSURANCE ASSOCIATION … PPO POLICY 0111 final 11-29-10.pdf · GR-(PPO)-2011 1 [01/11] ALASKA COMPREHENSIVE HEALTH INSURANCE ASSOCIATION ASSOCIATION PPO](https://static.fdocuments.in/doc/165x107/5b7d89b87f8b9a717e8c6bf3/alaska-comprehensive-health-insurance-association-ppo-policy-0111-final-11-29-10pdf.jpg)







