
Orbital Tumors - University of Texas Medical Branch · Evaluation – laboratory and imaging ......
69
Orbital Tumors Michael Underbrink, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 31, 2001
-
Upload
trinhkhanh -
Category
Documents
-
view
217 -
download
2
Transcript of Orbital Tumors - University of Texas Medical Branch · Evaluation – laboratory and imaging ......

Orbital Tumors
Michael Underbrink, MD
Faculty Advisor: Shawn Newlands, MD, PhD
The University of Texas Medical Branch
Department of Otolaryngology
Grand Rounds Presentation
October 31, 2001

Anatomy - Bony

Anatomy - Bony

Anatomy - Bony

Anatomy - Bony

Anatomy - Bony

Anatomy – Fascial Compartments

Anatomy – Fascial Compartments

Anatomy – Eyelid

Anatomy – Eyelid

Anatomy – Blood Supply

Anatomy – Blood Supply

Anatomy – Lacrimal System
Secretory and excretory system
Secretory
Lacrimal gland
Conjunctival goblet cells, accessory subconjunctival
glands and meibomian glands
Excretory
Removes tears via contraction of the eyelids

Anatomy – Lacrimal System
Evaluation of Orbital Tumors
Good history and physical examination
Elicit history of allergies, sinus infection, epistaxis,
or nasal congestion
PMHx – thyroid?, autoimmune?
Ophthalmic exam essential
Look for visual acuity/fields, ocular motility and
pupillary responses (RAPD); palpate

Evaluation Continued
Exophthalmos – 90%
“Worm’s eye” view
Protrusion more than
21mm beyond rim
One globe displaced >
2mm relative to the other
Direction of displacement
important

Evaluation – laboratory and imaging
CBC, ESR, and TFT’s
Imaging most important to define extent and
location
Ultrasonography – inexpensive, safe, cystic vs. solid
CT scanning – most widely used, bony landmarks
MRI – useful for intracranial disease and vascular
lesions
Arteriography – good for certain vascular disease

Pediatric Orbital Tumors
Differs substantially from adult types
More often congenital lesions and infectious
Most common – cystic lesions (dermoids)
2nd most common – vascular lesions
Most common malignancy - rhabdomyosarcoma
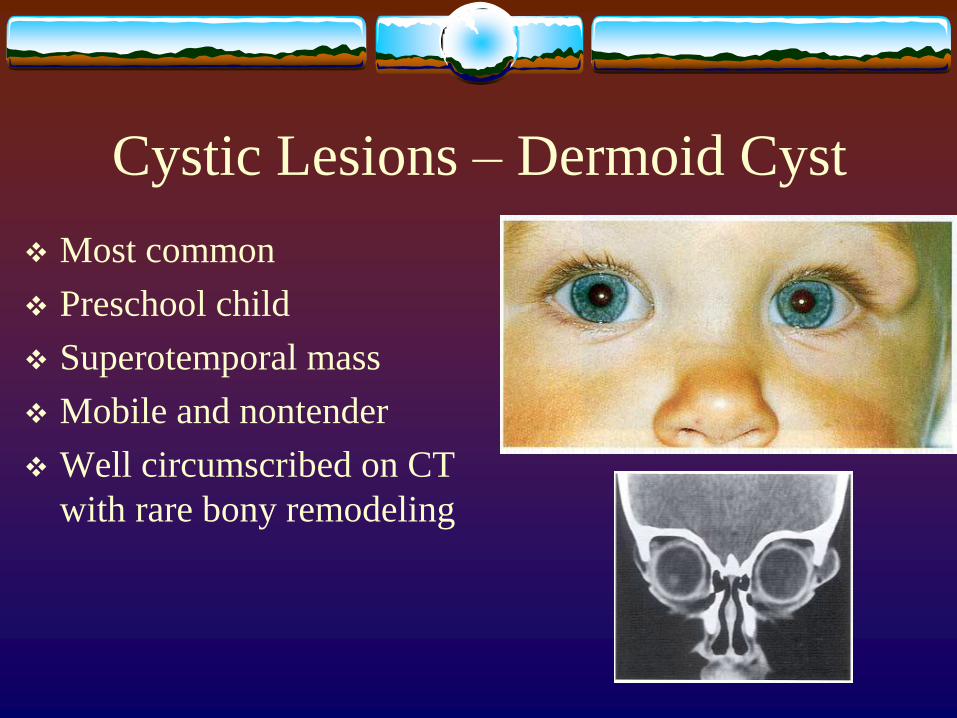
Cystic Lesions – Dermoid Cyst
Most common
Preschool child
Superotemporal mass
Mobile and nontender
Well circumscribed on CT
with rare bony remodeling

Cystic Lesions – Dermoid Cyst
Deeper lesions usually
show bony abnormality
May present with
proptosis and visual c/o
Surgical excision at
around 1 year of age

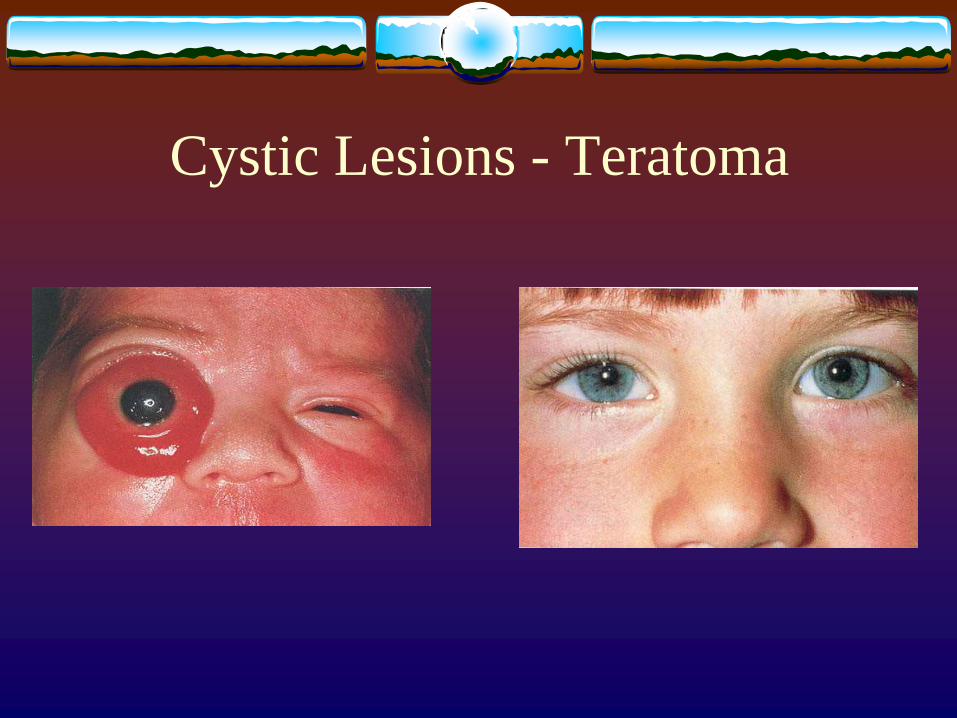
Cystic Lesions - Teratoma
Rare congenital germ-cell
tumors
Ectodermal, mesodermal
and endodermal elements
Present at birth, usually
with significant morbidity
Massive proptosis with
large intraconal masses
Cystic Lesions - Teratoma

Cystic Lesions - Teratoma

Vasculogenic Lesions – Capillary
Hemangioma 1/3 diagnosed at birth
90% visible by 6 months
Most common presenting as superficial tumor that
develops “strawberry” appearance
Enlarge with Valsalva
CT/MRI show diffusely infiltrating non-
encapsulated mass

Capillary Hemangioma

Capillary Hemangioma
Usual course
Normal at birth – noticed at one month – enlarge till 1 to
2 years of age – spontaneous involution by age 4 to 8 yr
Cosmetic sequelae minimal
Visual complications – amblyopia or astigmatism
Major complications – superinfection, ulceration
Rare complications – Kasbach-Merrit, HO cardiac

Capillary Hemangioma - Outcome

Capillary Hemangioma - Treatment
Indications include any complication
Medical therapy – steroids (systemic, intralesional)
or interferon
Radiation therapy
Surgical resection for unresponsive or well-
encapsulated lesions

Capillary Hemangioma

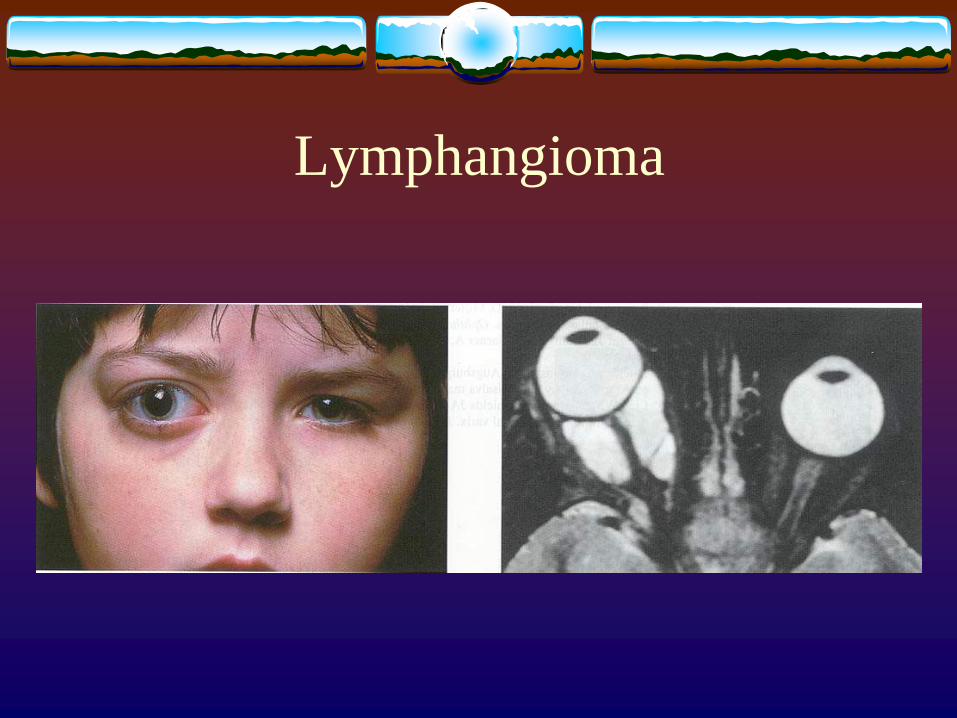
Lymphangioma
Benign congenital vascular malformations
May involve conjunctiva, eyelids or deep orbit
Usually identified prior to teenage years
Usually slow enlargement and increasing proptosis
Sudden proptosis from hemorrhage into cyst
No enlargement with Valsalva
CT/MRI shows multi-compartmental nature

Lymphangioma
Lymphangioma
Lymphangioma
Treatment for significant proptosis, corneal
exposure or optic nerve compression
Debulking and cyst drainage usually
Complete removal often not possible
Rhabdomyosarcoma
Most common malignant tumor in children
Presents within 1st decade
Rapid unilateral proptosis and globe displacement
CT scan shows irregular margins and often bony
destruction
Excisional biopsy ASAP for diagnosis if suspected

Rhabdomyosarcoma

Rhabdomyosarcoma
Take as much tumor as
possible on biopsy
Disseminated or gross
residual disease after
biopsy carries 35% 5-year
survival rate
Chemotherapy and XRT
after biopsy (90% 5-yr for
localized disease)

Rhabdomyosarcoma

Optic Nerve Glioma
3rd most common in children
May occur randomly although often associated
with NF type I (up to 50%)
Mean age – 8 years
Proptosis and visual symptoms
Headache and pain with intracranial extension
Diagnosis clinically and radiographically

Optic Nerve Glioma

Optic Nerve Glioma
CT/MRI shows fusiform enlargement of optic nerve
MRI for intracranial extension
Significant mortality once into chiasm
Must be excised while confined to nerve, esp. if blind or proptotic

Fibrous Dysplasia
Most often fibro-osseous
tumor
Occurs in 1st two decades
Replacement of normal
bone with immature
woven bone
Polyostotic (Albright’s)
and monostotic types

Fibrous Dysplasia

Fibrous Dysplasia
Usually stabilize after puberty
Conservative treatment the rule
Complete resection preferable for significant
cosmetic deformity or vision loss
Craniofacial reconstruction with neurosurgeon

Metastatic Tumor: Neuroblastoma
Most frequent in kids
Neuroblastoma accounts for 10% of all childhood malignancies
Primary: usually adrenal
Bilateral metastasis with eyelid ecchymoses and proptosis common
Survival rate – 15%

Adult Orbital Tumors
Vary significantly from children
Most common
Carcinomas
Pseudotumor
Lacrimal gland tumors
Lymphomas
Cysts, meningiomas, vascular tumors

Paranasal Sinus Masses
Masses of the paranasal sinus potentially can
spread to involve the orbit
Most common: mucocele
Neoplasms of this area are uncommon, but
frequently involve orbit
Benign tumors push periorbita, malignant invade

Mucoceles
Obstruction of ostium in a
sinus
Enlarging fluid filled sinus
Erodes through bony orbit
wall
Most arise from frontal
and ethmoid
CT – homogenous mass

Mucoceles

Neoplasms of Paranasal Sinus
Uncommon
Most common – SCCa
Orbital invasion in 2/3 of patients with SCCa
Glandular malignancies from minor salivary
glands or respiratory epithelium
Orbital extensive gives poor prognosis
Biopsy to Dx; radical resection to treat

Neoplasms of Paranasal Sinus
Orbital Pseudotumor
Idiopathic orbital inflammation
1905 by Birch-Hirschfiel first described
Excludes systemic diseases (sarcoid, thyroid,
autoimmune and Wegener’s)
2nd to 7th decade
Multifocal involvement of any orbital structure

Orbital Pseudotumor
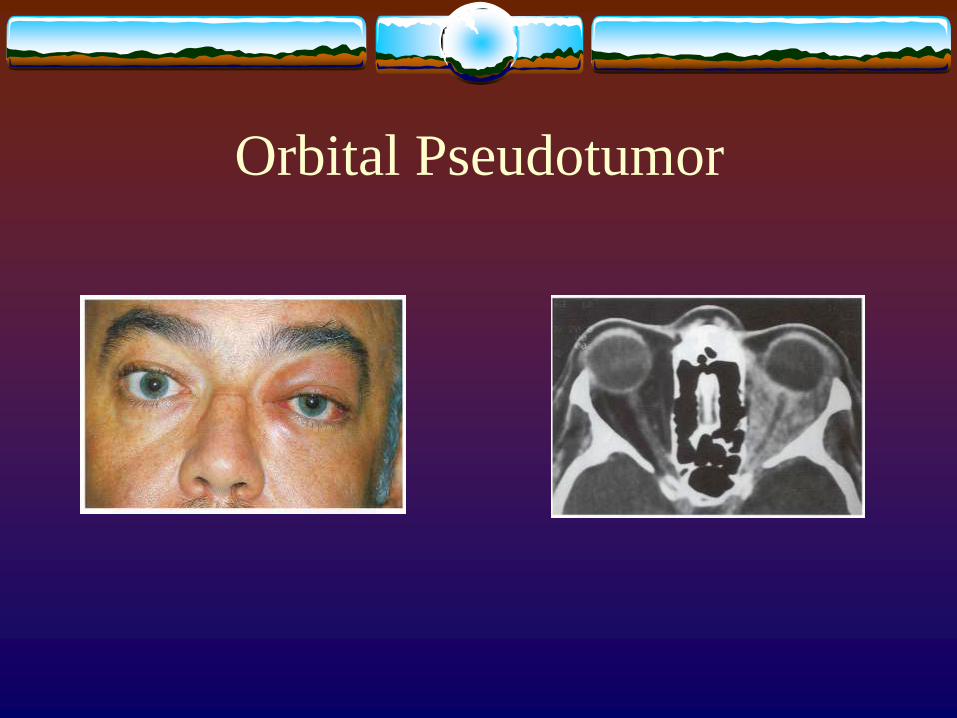
Proptosis – acute onset of a few days
Eyelid swelling, chemosis and diplopia also common
Visual loss with optic nerve involvement
CT findings – hazy enlargement of affected structures
Treatment – Steroids, immunosuppresive meds, radiation therapy when steroids adverse
Orbital Pseudotumor

Lacrimal Gland Tumors
Enlargement of lacrimal fossa with displacement
of globe and no inflammatory signs
50% epithelial, 50% lymphoproliferative
CT scan – lymphoid show smooth enlargement of
gland, epithelial are irregular
Primary epithelial neoplasms of lacrimal gland are
rare

Lacrimal Tumor – Pleomorphic
Adenoma Benign mixed tumor
Most common of these
20 to 50 years
Painless proptosis with
inferior/medial globe
displacement
Many months or years
Excisional biopsy (total)

Lacrimal Tumor – Adenoid Cystic
Carcinoma Most common malignant
of these
Progressive onset of symptoms
Pain and numbness
CT with bony destruction and infiltration
50% mortality, requires aggressive surgical Tx
Lymphoid Tumors
Incidence between 4 to 13 % of all orbital tumors
Primary or secondary to systemic disease
Most patients who present with localized orbital
disease will develop systemic lymphoma
Presents between age 50 and 70
Anterior, “salmon patch” mass causing progressive
painless proptosis

Lymphoid Tumors

Lymphoid Tumors
Generous biopsy needed to make diagnosis
Systemic workup necessary
Localized orbital lymphoma – XRT
Systemic lymphoma – XRT + chemotherapy
Consultation of oncologist should be obtained

Orbital Meningiomas
4th to 7th decade of life, rare in children
Most (70%) invade from cranium
Primary orbital meningiomas may arise from optic
nerve
Proptosis, visual disturbances, headache and
diplopia
CT/MRI fusiform enlargement of optic nerve

Orbital Meningiomas

Schwannomas
Neurilemoma – benign, non-invasive peripheral
nerve tumor, from any nerve in orbit
Rare, ages 20 to 70 years
CT/MR show well circumscribed ovoid mass
Most commonly intraconal, may be extraconal
(trochlear, supraorbital nerves)

Schwannomas
Cavernous Hemangioma
a.k.a encapsulated venous malformation
Most common vascular lesion of adults
Peak incidence – middle age (40 years)
Women > men
Slowly progressive painless proptosis over several
years
do not enlarge with Valsalva, but grow slowly

Cavernous Hemangioma
CT/MRI reveals well-
defined mass, oval
Homogeneous with
increased density – CT
MRI – isointense to
muscle
Treatment –surgical
excision, recur rarely

Cavernous Hemangioma

Metastatic Tumors
8% of all orbital tumors
Most common in women – breast (& overall)
Most common in men – prostate & lung
Symptoms – proptosis, diplopia, pain, vision loss
Presents in 7th decade
Prognosis is very poor (avg. survival 10 months)
XRT usual; Chemo and Hormonal occasional

Metastatic Tumor - Breast

Conclusions
Orbital anatomy very complex with close
association to sinuses and cranial vault
Broad range of diseases and tumors
Important to recognize the signs of possible orbital
malignancy
Ophthalmologic consultation always
Often need multi-specialty cooperation


















