Orbital anatomy
43
Anatomy of eye
-
Upload
samten-dorji -
Category
Health & Medicine
-
view
66 -
download
1
Transcript of Orbital anatomy

Anatomy of eye

Outline
• Orbital anatomy• Orbital adnexa• The eye globe

Outline of anatomy of Orbit
• Orbital volume• Bony orbit• Orbital walls• Orbital foramen• Orbital fissure• Peri orbital sinuses• Blood supply and nerve supply

Orbital anatomy
Orbital volume•The volume of each adult orbit is slightly less than 30 cm3. •Pear shaped•The orbital entrance averages about 35 mm in height and 45 mm in width. The maximum width is about 1 cm (behind the anterior orbital margin)•In adults, the depth of the orbit varies from 40 to 45 mm from the orbital entrance to the orbital apex•Both race and sex affect each of these measurements.
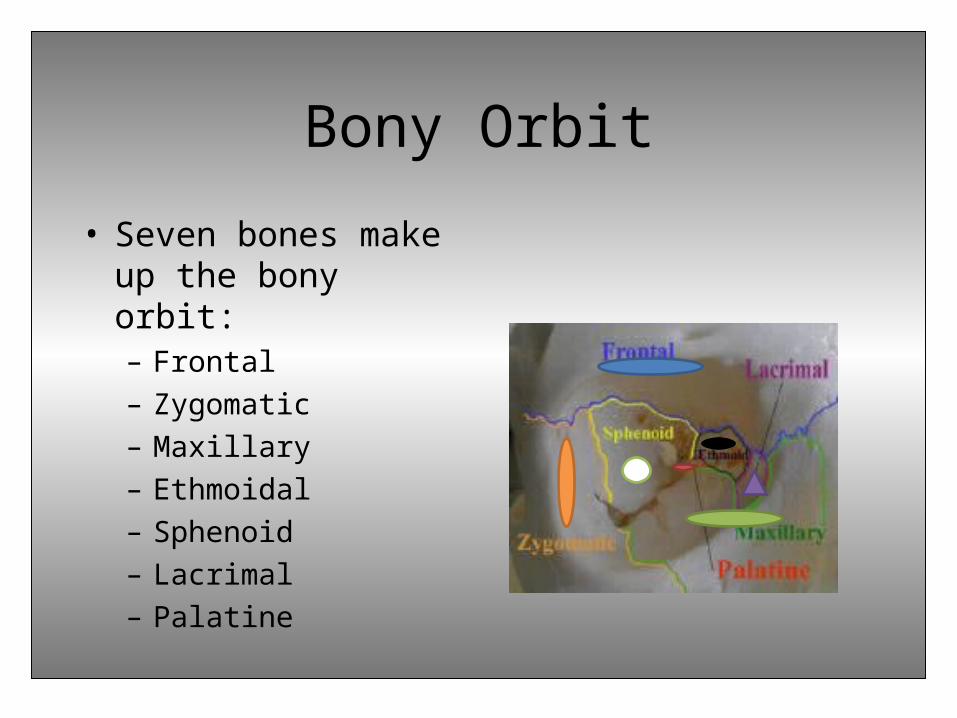
Bony Orbit
• Seven bones make up the bony orbit:– Frontal– Zygomatic– Maxillary– Ethmoidal– Sphenoid– Lacrimal– Palatine

Orbital margin• Forms quadrilateral spiral• Superior margin is formed
by frontal bone• Medial margin formed by
the frontal bone,posterior lacrimal crest of the lacrimal bone and anterior lacrimal crest of the lacrimal bone
• Inferior margin is formed by the maxillary bones and zygomatic bones
• Lateral margin is formed by the zygomatic and the frontal bones

Orbital Roof
• The orbital roof is formed from both the orbital plate of the frontal bone and the lesser wing of the sphenoid bone.
• The anterolateral part of the roof has a depression called the fossa for the lacrimal gland
• The trochlear fossa is situated at the junction of roof and the medial wall

Orbital roof
• RelationsAbove, it is related to frontal lobe cerebrumand meninges
Below, it is related to frontal nerve, levatorpalpebrae superioris, superior rectus, superioroblique, trochlear nerve and lacrimal gland

Orbital roof
Clinical applications•As the roof is perforated neither by major nerves nor by blood vessels, it can be easily nibbled away in transfrontal orbitotomy. •The roof is reinforced laterally by the greater wing of sphenoid & anteriorly by superior orbital margin so the fractures which involve frontal bone tend to pass towards the medial side.
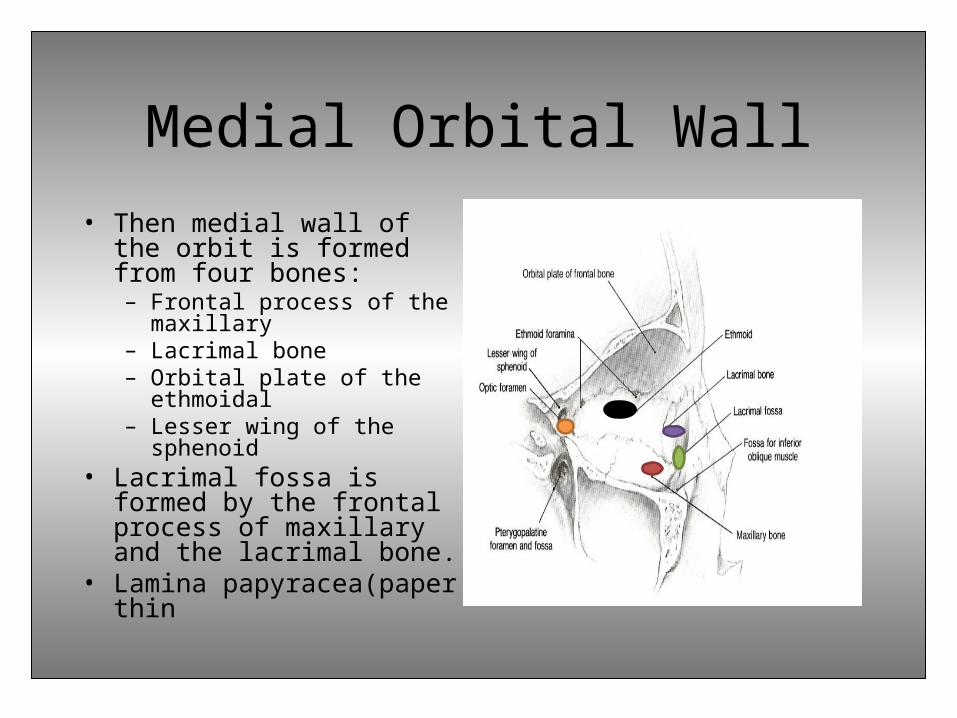
Medial Orbital Wall• Then medial wall of the orbit
is formed from four bones:– Frontal process of the
maxillary– Lacrimal bone– Orbital plate of the
ethmoidal– Lesser wing of the sphenoid
• Lacrimal fossa is formed by the frontal process of maxillary and the lacrimal bone.
• Lamina papyracea(paper thin
Medial Orbital Wall
• Relations
Medial to the medial wall lie anterior ethmoidal air sinuses, middle meatus of nose, middle
and posterior ethmoidal sinuses and sphenoidal air sinuses.
The orbital surface of medial wall is related to superior oblique muscle
and medial rectus muscle. In between the two muscles lie
anterior ethmoidal nerve, posterior ethmoidal nerve, infra trochlear
nerve, terminal branch of ophthalmic artery

Medial Orbital Wall
Clinical applications • It is the thinnest wall of the orbit so it is frequently fragmented as a result of indirect blow out fractures.• This accounts for ethmoiditis being the most common cause of orbital cellulitis, especially in children. •The medial wall is frequently eroded by inflammatory lesions, cysts and neoplasms
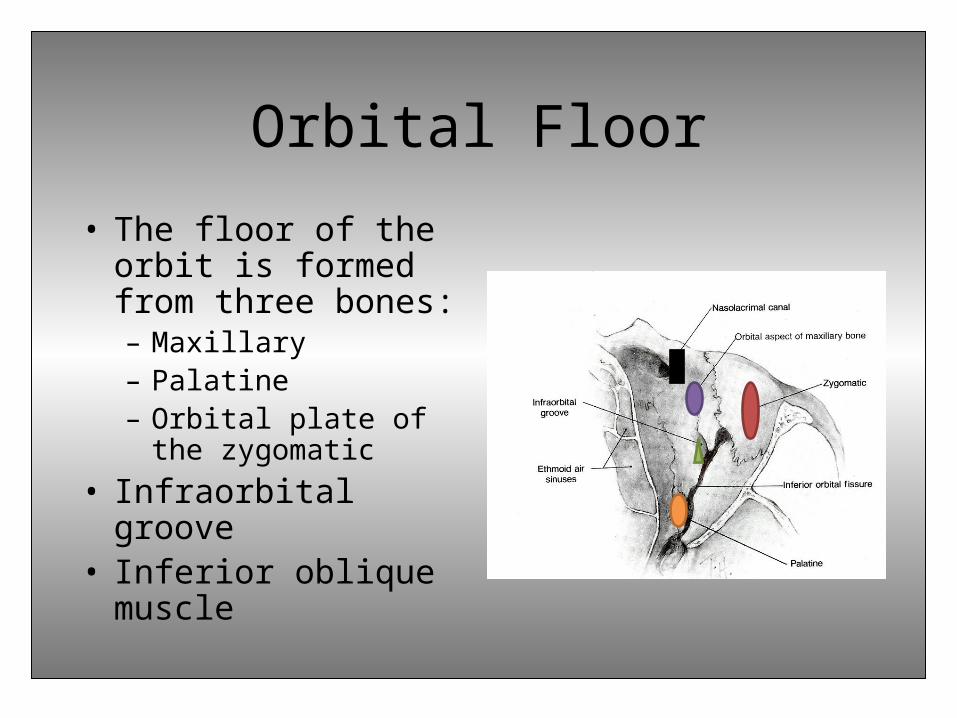
Orbital Floor
• The floor of the orbit is formed from three bones:– Maxillary– Palatine– Orbital plate of the
zygomatic• Infraorbital groove• Inferior oblique
muscle
Orbital Floor
• Relations
Below it is related to maxillary air sinus
Above it is related to inferior rectus muscle,
inferior oblique muscle and nerve to inferior oblique.

Orbital Floor
Clinical applications•The orbital floor being quite thin is commonly involved in ‘blow- out fractures’ due to unsupported dome of maxillary sinus and plus the infra orbital groove & canal weaken the already thin floor further.•It is easily invaded by tumors of the maxillary antrum

Lateral Orbital Wall
• Thickest and strongest• Formed from two bones:
– Zygomatic– Greater wing of the sphenoid
• Lateral orbital tubercle (Whitnall’s tubercle):
check ligament of lateral rectus muscle Suspensory ligament of eye ball Lateral palpebral ligament Aponeurosis of the levator muscle Whitnall ligament

Lateral Orbital Wall
• Relations
Medially it is related to
lateral rectus, lacrimal nerve
and vessels and zygomatic
nerve
Lateral Orbital Wall
Clinical applications•The anterior half of globe is not covered by bone on lateral side. Hence, palpation of retrobulbar tumors is easier from the lateral side.• It is the strongest portion of the orbit and needs to be sawed open in lateral orbitotomy. •The zygomaticosphenoid suture is an important landmark during surgery.

Orbital ForamenThe optic foramen•Leads from middle cranial fossa to the apex of orbit.•6.5mm in diameter•Lesser wing of sphenoid bone•Conducts the optic nerve, opthalmic artery and sympathetic fibers from the carotid plexus.

Optic foramen
Clinical applications•Optic foramen enlargement is commonly seen with optic nerve gliomas.•Blunt trauma may cause optic canal fracture, haematoma at the orbital apex or shearing at the nerve of foramen resulting in optic nerve damage
Orbital Foramen
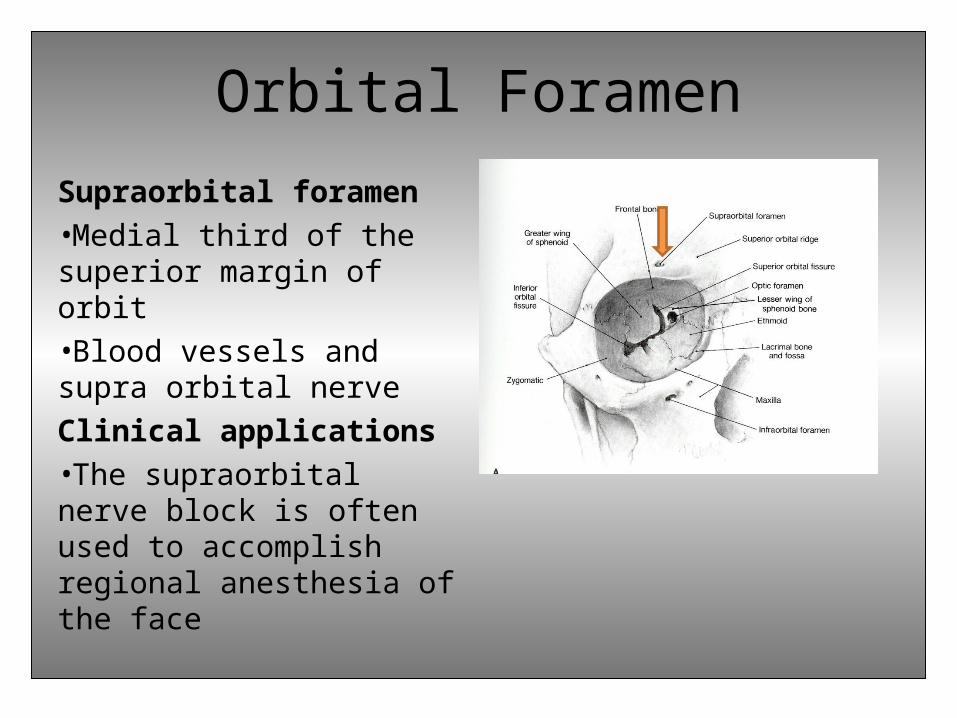
Supraorbital foramen•Medial third of the superior margin of orbit•Blood vessels and supra orbital nerveClinical applications•The supraorbital nerve block is often used to accomplish regional anesthesia of the face

Orbital Foramen
• Anterior ethmoidal foramen transmits the anterior ethmoidal vessel and nerve
• Posterior ethmoidal foramen transmits the posterior vessels and nerve through the frontal bone

Orbital Foramen• Zygomatic foramen contains
zygomaticofacial and zygomatico temporal branches of zygomatic nerve and zygomatic artery
• The infraorbital foramen contains the infraorbital artery, infraorbital vein, and infraorbital nerve.
• Clinically, the infraorbital foramen provides a route of spread for infection or maxillary tumors to the orbit and the skull base.

Orbital Fissure
Superior orbital fissure•Located between the greater and lesser wings of sphenoid•22mm long•Spanned by the common tendinious ring of the rectus muscle(annulus of zinn)

Superior orbital fissure• Above the ring, the
superior orbital fissure transmits the
lacrimal nerve of CN5 frontal nerve of CN5 Trochlear nerve superior opthalmic vein
• Within the ring superior and inferior division
oculomotor nerve nasociliary branch of CN5 sympathetic roots of ciliary
ganglion abducen nerve

Clinical applications
• When idiopathic inflammation preferentially involves the superior orbital fissure, the Tolosa-Hunt syndrome (painful ophthalmoplegia) results.
Orbital Fissure
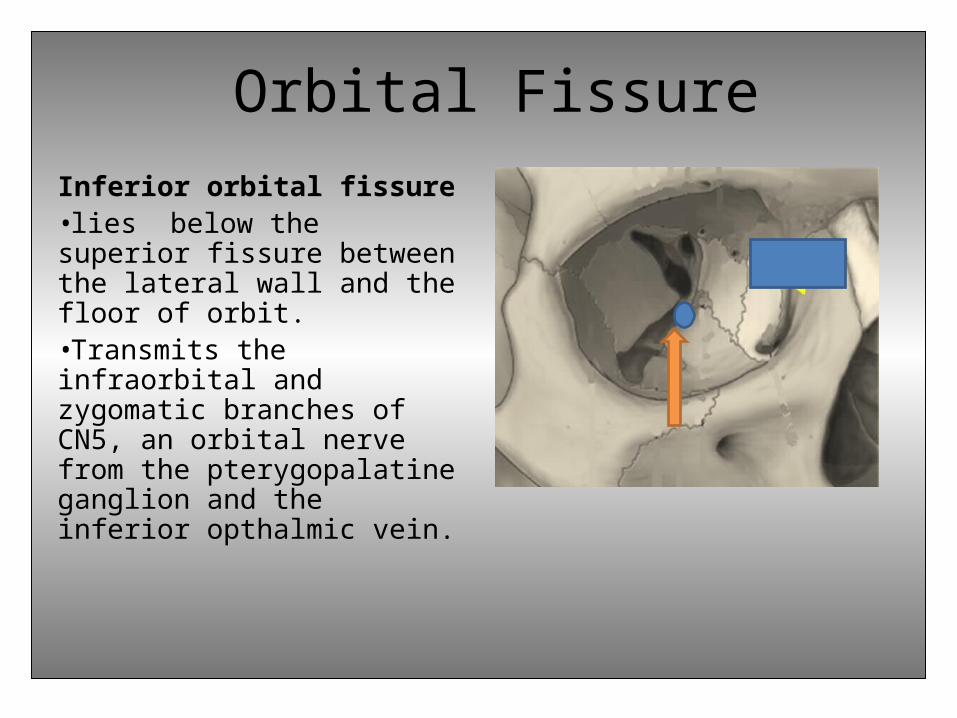
Inferior orbital fissure•lies below the superior fissure between the lateral wall and the floor of orbit.•Transmits the infraorbital and zygomatic branches of CN5, an orbital nerve from the pterygopalatine ganglion and the inferior opthalmic vein.

Inferior orbital fissure
Clinical applications•The inferior orbital fissure extends more anteriorly than the superior orbital fissure, ending about 20 mm from the anterior orbital rim. This structure serves as a posterior landmark in the surgical subperiosteal dissection along the orbital floor.• Immediately beneath the infraorbital fissure lies the pterygoid space with the temporalis fossa laterally; blunt trauma to the temporalis muscle can result in orbital hemorrhage via this connection

Periorbital SinusesFrontal sinus•The frontal sinus lies deep to the superior orbital rim and drains into the middle meatus via the frontonasal duct. •Each sinus is a single chamber with intrasinus septae, which give it a scalloped appearance radiologically. Clincial application•The frontal sinus is a common site for mucocele development which can extend into the orbit.

Periorbital SinusesMaxillary sinus•largest of the sinuses•the sinus roof is the orbital floorClinical applications•The maxillary sinus drains into the middle meatus through an ostium located near the level of the orbital floor, thus orbital tissues that are displaced in surgery or trauma may obstruct the ostium.

Periorbital SinusesEthmoid and sphenoid sinuses•The ethmoid sinuses are shaped like a box slightly wider posteriorly where it articulates with the sphenoid •The medial walls of the orbit, which borders the nasal wall anteriorly and ethmoidal sinus and sphenoid sinus posteriorly are almost parallel..
Ethmoid and sphenoid sinus
Clinical applications•It is important to be aware of the anatomic relationship of anterior ethmoid air cells to the lacrimal sac fossa when performing external dacryocystorhinostomy during creation of ostium

Blood Supply
• Internal carotid artery• External carotid artery

Blood SupplyOpthalmic artery•arises from the ICA and is the major blood supply of the orbit•Orbital group•Ocular groupLong ciliary arteryShort ciliary arteryAnterior ciliary arteryCentral retinal arteryMuscular artery
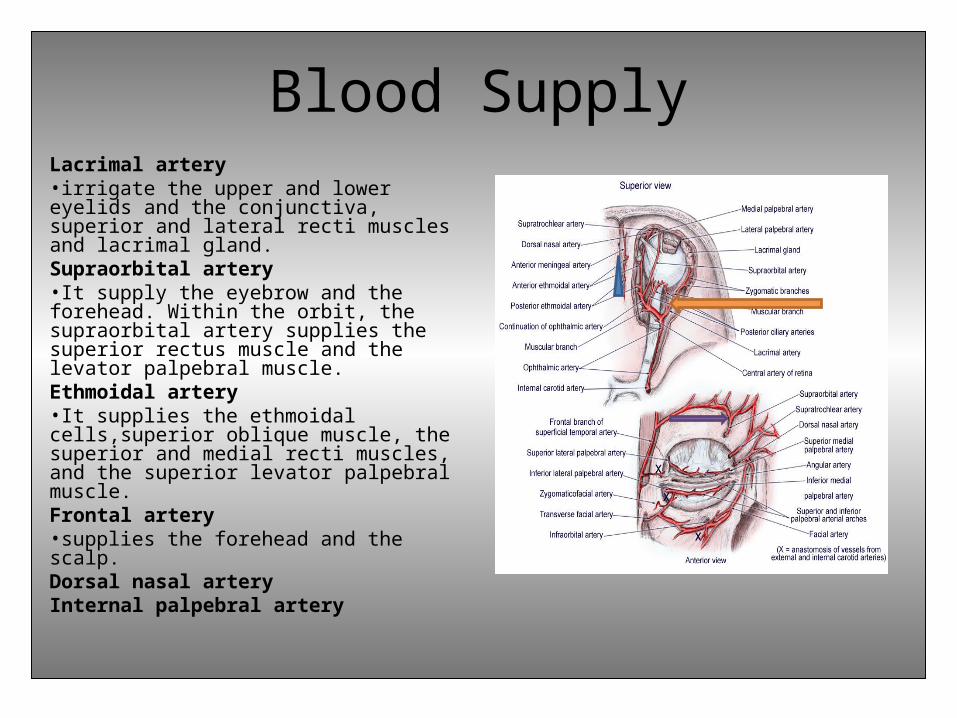
Blood SupplyLacrimal artery•irrigate the upper and lower eyelids and the conjunctiva, superior and lateral recti muscles and lacrimal gland. Supraorbital artery•It supply the eyebrow and the forehead. Within the orbit, the supraorbital artery supplies the superior rectus muscle and the levator palpebral muscle.Ethmoidal artery •It supplies the ethmoidal cells,superior oblique muscle, the superior and medial recti muscles, and the superior levator palpebral muscle.Frontal artery•supplies the forehead and the scalp. Dorsal nasal arteryInternal palpebral artery

Blood SupplyVenous Blood supplyVortex veins•The vortex veins provide drainage for the uveal tract (choroid, ciliary body, iris) and drain into superior and inferior opthalmic veinsSuperior ophthalmic vein•The superior ophthalmic vein is the main venous channel for the superior orbit. it drains to the cavernous sinus. Inferior ophthalmic vein•The inferior ophthalmic vein provides a channel for inferior drainage. .

Blood supply
Clinical applications•In cases of severe orbital infection, the valveless venous system allows spread of infected emboli to the cavernous sinus and can cause cavernous sinus thrombosis

Innervation of the Orbit• The innervation of the orbit
can be divided into 4 functional components:
general somatic efferent general somatic afferent general visceral efferent special sensory afferent • The general somatic
efferents include the motor division of the oculomotor nerve (CN III), the trochlear nerve (CN IV), and the abducens nerve (CN VI).

Innervation of the OrbitOculomotor nerve•The oculomotor nerve supplies the superior rectus muscle and the levator palpebrae superioris, medial rectus, inferior rectus, and inferior oblique. Trochlear nerve•The trochlear nerve innervates the superior oblique muscle.Abducens nerve•The abducens nerve innervates the lateral rectus. •The relatively long intracranial course of the abducens nerve makes it susceptible to injury secondary to trauma, tumor, aneurysm, and infection. .

Innervation of the orbit
Trigeminal nerve•The trigeminal nerve, supplies the general sensory innervation to the orbit •the oculocardiac reflex is triggered by afferent fibers of the trigeminal nerve, which synapse with visceral motor nucleus neurons of the vagal nerve in the reticular formation of the brainstem. It causes bradycardia, hypotension, and nausea when pressure is applied to the globe or when the extraocular muscles are stretched

Innervation of the OrbitOphthalmic and other nerves•Within the orbit, the ophthalmic nerve branches into the lacrimal, frontal, and nasociliary nerves. •The lacrimal nerve innervates the lacrimal gland•The frontal branch innervate the eyebrow and scalp. •The nasociliary branch enters the orbit through the annulus of Zinn and then gives off short and long ciliary nerves to the globe. •The long ciliary nerves are responsible for dilatation of the pupil. • The infratrochlear nerve is also a branch of the nasociliary nerve and provides sensory innervation to the medial lower lid, side of nose, conjunctiva, and lacrimal sac.

Thank you

References• Fundamentals and principles of ophthalmology(2012-2013)-
American Academy of ophthalmology• Clinical Anatomy of Orbit and Common Orbital Disease-
Dr.M.Kokilam, MS Resident, Aravind Eye Hospital, Madurai• Orbit anatomy http://
emedicine.medscape.com/article/835021-overview• Duane’s Clinical ophthalmology Chapter 21
Orbital Anatomy and Its Clinical ApplicationsDeborah D. Sherman, Cat N. Burkat and Bradley N. Lemke
• Anatomy of The Bony Orbit-Some Applied Aspects Patnaik V.V.G., 2Bala Sanju, 3Singla Rajan K. Department of Anatomy, Government Medical College, Patiala. Amritsar. Department of Oral & Maxillofacial Surgery, SGRD Institute of Dental Sciences & Research, Amritsar.