Oral Fleroxacin Prophylaxis in Transurethral Surgery
3
0022-5347/96/1561-0146$03.M)/0 THE JOURNAL OF UROLOGY Copyright 0 1996 by AMERICAN UROWICAL ASSOCIATION, INC Vol. 156, 146-148, July 1996 Printed in U.S.A ORAL FLEROXACIN PROPHYLAXIS IN TRANSURETHRAL SURGERY THOMAS C. GASSER, MARC WISARD AND RENO FREI From the Urologic Clinics and Bacteriology Laboratory, University Hospital, Basel, and Urologic Clinics, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland ABSTRACT Purpose: A prospective trial was done to test the efficacy of antimicrobial prophylaxis in patients undergoing transurethral surgery. Materials and Methods: A total of 75 adults with preoperatively sterile urine was randomized to receive either 400 mg. oral fleroxacin once daily or placebo as long as the catheter was in place. Urine cultures were obtained preoperatively and after removal of the catheter just before hospital discharge. Growth of lo4/ml. or more bacteria was considered a positive urine culture. Results: Postoperative urinary tract infection rates were significantly lower in the fleroxacin group (3%) than in the placebo group (23%). Our study demonstrated the benefit of antimicrobial prophylaxis in preventing urinary tract infection after transurethral surgery, including resection of the prostate, in patients with sterile urine. Conclusions: The oral administration of 1 daily tablet of fleroxacin for the duration of cathe- terization is a safe, efficacious and clinically feasible regimen. KEY WORDS: anti-infectiveagents, fluoroquinolone; fleroxacin; prostate; prostatectomy Despite the advent of newer technologies for the treatment of benign prostatic hyperplasia, transurethral resection of the prostate remains a frequent operation in Western coun- tries.' Because transurethral resection has become a safe operation, urinary tract infections continue to be an impor- tant cause of postoperative morbidity and cost. However, controversy remains as to whether antimicrobials should be administered prophylactically.2.3 Therefore, the efficacy of daily oral fleroxacin was evaluated in a prospective, random- ized, placebo controlled study. Fleroxacin was chosen be- cause of its oral form, long half-life of 10 hours, good tissue penetration and antimicrobial spectrum against most uro- pathogens.4," MATERIALS AND METHODS The study was approved by the local ethical committees of our institutions, and written informed consent was obtained from all patients before enrollment. Men and women older than 18 years who were about to undergo transurethral surgery (that is transurethral resection of the prostate and/or bladder tumors, or internal urethrotomy) and who had pre- operatively sterile urine were included in the study. Exclu- sion criteria were a preoperative indwelling urinary catheter, any prosthetic devices (for example prosthetic heart valves), pregnant or lactating women, impaired renal or hepatic func- tion and hypersensitivity to fluoroquinolones. Also excluded from the study were patients who had received antimicrobial therapy within 2 weeks before enrollment or who were re- ceiving any concomitant antimicrobial medication. The study was designed in a single-blind manner to allow measurement of prostatic tissue fleroxacin concentrations. However, for economic reasons antibiotic tissue concentra- tions could only be measured in a limited number of patients, and so we selected those receiving fleroxacin and 8 receiving placebo (controls.) Patients who agreed to participate in the trial received 1 tablet (400 mg. fleroxacin or a placebo iden- tical in shape, odor and appearance) with a sip of water 2 hours preoperatively. The trial medication was continued until the day of catheter removal (usually 24 to 48 hours postoperatively). Patients who had fever were switched im- Accepted for publication January 12. 1996. mediately to an alternative antibiotic. Asymptomatic pa- tients in the placebo group were given antimicrobials, while those in the fleroxacin group were switched to amoxicillin and tobramycin. Transurethral resection was performed in a standard man- ner using a 24F or 26F resectoscope. A 10F cystostomy trocar for low pressure resection was placed immediately preoper- atively and removed at 24 hours in patients with benign prostatic hyperplasia but not in those with bladder tumors or urethral strictures. The genitalia were cleansed with povidone-iodine solution, and a sterile lubricant containing no antiseptic was injected transurethrally before insertion of the resectoscope. A 22F 2-way catheter was placed postoper- atively and cystostomy-to-catheter irrigation was continued for 4 to 6 hours. Urine cultures were obtained 1 day preoperatively, shortly after catheter removal and before hospital discharge. Posi- tive urine cultures were defined as a bacteria count of lo4 colony-forming units per ml. or greater. Additionally, in each patient body temperature, blood pressure and heart fre- quency as well as any other clinical or laboratory changes were recorded daily. Fleroxacin concentrations were determined simulta- neously in blood and tissue (prostate or bladder tumor). The blinded samples were analyzed with high performance liquid chromatography. The chi-square and Fisher exact tests were used for statistical analysis. Results are reported as mean and standard deviation. Statistical significance was defined as p S0.05. RESULTS Of 37 patients given fleroxacin and 38 given placebo 14 were excluded from the study, leaving 30 given fleroxacin and 31 given placebo for efficacy analysis. Reasons for exclu- sion were nonsterile baseline culture (4 fleroxacin and 5 placebo), protocol violation due to concomitant antibiotic treatment (1 fleroxacin and 1 placebo) and no postoperative urine culture (2 fleroxacin and 1 placebo). Patient character- istics were comparable between the 2 groups (table 1). The trial drug was administered for a mean of 2.3 -C 1.1 days in the fleroxacin group and 1.8 2 0.8 days in the placebo group (not statistically different). There was no statistical differ- 146
Transcript of Oral Fleroxacin Prophylaxis in Transurethral Surgery

0022-5347/96/1561-0146$03.M)/0 THE JOURNAL OF UROLOGY Copyright 0 1996 by AMERICAN UROWICAL ASSOCIATION, INC
Vol. 156, 146-148, July 1996 Printed in U.S.A
ORAL FLEROXACIN PROPHYLAXIS IN TRANSURETHRAL SURGERY THOMAS C. GASSER, MARC WISARD AND RENO FREI
From the Urologic Clinics and Bacteriology Laboratory, University Hospital, Basel, and Urologic Clinics, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland
ABSTRACT
Purpose: A prospective trial was done to test the efficacy of antimicrobial prophylaxis in patients undergoing transurethral surgery.
Materials and Methods: A total of 75 adults with preoperatively sterile urine was randomized to receive either 400 mg. oral fleroxacin once daily or placebo as long as the catheter was in place. Urine cultures were obtained preoperatively and after removal of the catheter just before hospital discharge. Growth of lo4/ml. or more bacteria was considered a positive urine culture.
Results: Postoperative urinary tract infection rates were significantly lower in the fleroxacin group (3%) than in the placebo group (23%). Our study demonstrated the benefit of antimicrobial prophylaxis in preventing urinary tract infection after transurethral surgery, including resection of the prostate, in patients with sterile urine.
Conclusions: The oral administration of 1 daily tablet of fleroxacin for the duration of cathe- terization is a safe, efficacious and clinically feasible regimen.
KEY WORDS: anti-infective agents, fluoroquinolone; fleroxacin; prostate; prostatectomy
Despite the advent of newer technologies for the treatment of benign prostatic hyperplasia, transurethral resection of the prostate remains a frequent operation in Western coun- tries.' Because transurethral resection has become a safe operation, urinary tract infections continue to be an impor- tant cause of postoperative morbidity and cost. However, controversy remains as to whether antimicrobials should be administered prophylactically.2.3 Therefore, the efficacy of daily oral fleroxacin was evaluated in a prospective, random- ized, placebo controlled study. Fleroxacin was chosen be- cause of its oral form, long half-life of 10 hours, good tissue penetration and antimicrobial spectrum against most uro- pathogens.4,"
MATERIALS AND METHODS
The study was approved by the local ethical committees of our institutions, and written informed consent was obtained from all patients before enrollment. Men and women older than 18 years who were about to undergo transurethral surgery (that is transurethral resection of the prostate and/or bladder tumors, or internal urethrotomy) and who had pre- operatively sterile urine were included in the study. Exclu- sion criteria were a preoperative indwelling urinary catheter, any prosthetic devices (for example prosthetic heart valves), pregnant or lactating women, impaired renal or hepatic func- tion and hypersensitivity to fluoroquinolones. Also excluded from the study were patients who had received antimicrobial therapy within 2 weeks before enrollment or who were re- ceiving any concomitant antimicrobial medication.
The study was designed in a single-blind manner to allow measurement of prostatic tissue fleroxacin concentrations. However, for economic reasons antibiotic tissue concentra- tions could only be measured in a limited number of patients, and so we selected those receiving fleroxacin and 8 receiving placebo (controls.) Patients who agreed to participate in the trial received 1 tablet (400 mg. fleroxacin or a placebo iden- tical in shape, odor and appearance) with a sip of water 2 hours preoperatively. The trial medication was continued until the day of catheter removal (usually 24 to 48 hours postoperatively). Patients who had fever were switched im-
Accepted for publication January 12. 1996.
mediately to an alternative antibiotic. Asymptomatic pa- tients in the placebo group were given antimicrobials, while those in the fleroxacin group were switched to amoxicillin and tobramycin.
Transurethral resection was performed in a standard man- ner using a 24F or 26F resectoscope. A 10F cystostomy trocar for low pressure resection was placed immediately preoper- atively and removed at 24 hours in patients with benign prostatic hyperplasia but not in those with bladder tumors or urethral strictures. The genitalia were cleansed with povidone-iodine solution, and a sterile lubricant containing no antiseptic was injected transurethrally before insertion of the resectoscope. A 22F 2-way catheter was placed postoper- atively and cystostomy-to-catheter irrigation was continued for 4 to 6 hours.
Urine cultures were obtained 1 day preoperatively, shortly after catheter removal and before hospital discharge. Posi- tive urine cultures were defined as a bacteria count of lo4 colony-forming units per ml. or greater. Additionally, in each patient body temperature, blood pressure and heart fre- quency as well as any other clinical or laboratory changes were recorded daily.
Fleroxacin concentrations were determined simulta- neously in blood and tissue (prostate or bladder tumor). The blinded samples were analyzed with high performance liquid chromatography. The chi-square and Fisher exact tests were used for statistical analysis. Results are reported as mean and standard deviation. Statistical significance was defined as p S0.05.
RESULTS
Of 37 patients given fleroxacin and 38 given placebo 14 were excluded from the study, leaving 30 given fleroxacin and 31 given placebo for efficacy analysis. Reasons for exclu- sion were nonsterile baseline culture (4 fleroxacin and 5 placebo), protocol violation due to concomitant antibiotic treatment (1 fleroxacin and 1 placebo) and no postoperative urine culture (2 fleroxacin and 1 placebo). Patient character- istics were comparable between the 2 groups (table 1). The trial drug was administered for a mean of 2.3 -C 1.1 days in the fleroxacin group and 1.8 2 0.8 days in the placebo group (not statistically different). There was no statistical differ-
146
ORAL FLEROXACIN PROPHYLAXIS IN TRANSURETHRAL SURGERY 147
TABLE 1. Patient demographics and diagnoses Parameter Fleroxacin (30 pts.) Placebo (31 pts.)
Mean age i- SD (yrs.1
No. men/No. women 2911 2813
69.6 i 11.3 72.8 -t 11.5
70.5 f 5.7 74.4 2 11.1 Mean wt. t SD (kg.)
No. prostatic hyperplasia 16 18 No. prostatic Ca 3 1 No. bladder tumor 11 11 No. urethral stricture 0 1
There was no statistical difference between the groups.
TABLE 2. Results of postoperative urine culture No. Pts. (76)
Fleroxacin Placebo Urine Culture
Neg. 29 (97)* Pos. 1 (3)
* p = 0.0244 (Fisher's exact test, 1-sided).
24 (77)* 7 (23)
ence in duration of postoperative urinary catheterization (2.2 2 1.2 days in the fleroxacin group versus 1.8 2 0.8 days in the placebo group) or hospital stay (5.0 versus 5.4 days, respectively).
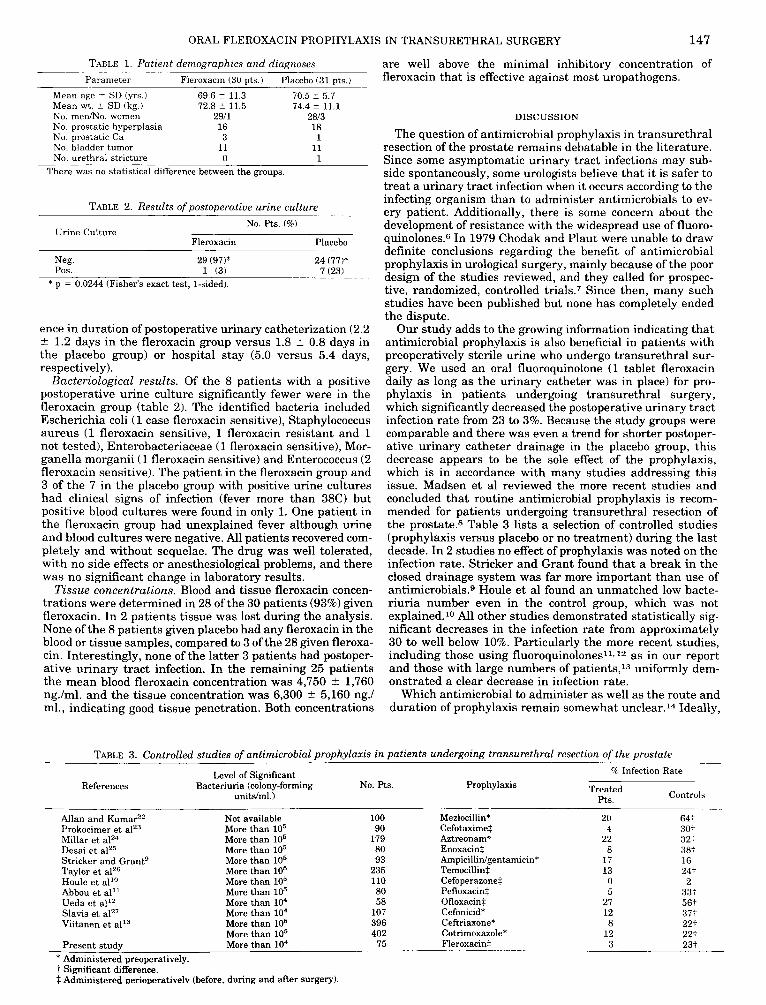
Bacteriological results. Of the 8 patients with a positive postoperative urine culture significantly fewer were in the fleroxacin group (table 2). The identified bacteria included Escherichia coli ( 1 case fleroxacin sensitive), Staphylococcus aureus (1 fleroxacin sensitive, 1 fleroxacin resistant and 1 not tested), Enterobacteriaceae (1 fleroxacin sensitive), Mor- ganella morganii (1 fleroxacin sensitive) and Enterococcus (2 fleroxacin sensitive). The patient in the fleroxacin group and 3 of the 7 in the placebo group with positive urine cultures had clinical signs of infection (fever more than 38C) but positive blood cultures were found in only 1. One patient in the fleroxacin group had unexplained fever although urine and blood cultures were negative. All patients recovered com- pletely and without sequelae. The drug was well tolerated, with no side effects or anesthesiological problems, and there was no significant change in laboratory results.
Tis sue concentrations. Blood and tissue fleroxacin concen- trations were determined in 28 of the 30 patients (93%) given fleroxacin. In 2 patients tissue was lost during the analysis. None of the 8 patients given placebo had any fleroxacin in the blood or tissue samples, compared to 3 of the 28 given fleroxa- cin. Interestingly, none of the latter 3 patients had postoper- ative urinary tract infection. In the remaining 25 patients the mean blood fleroxacin concentration was 4,750 t 1,760 ng./ml. and the tissue concentration was 6,300 -+ 5,160 ng.1 ml., indicating good tissue penetration. Both concentrations
are well above the minimal inhibitory concentration of fleroxacin that is effective against most uropathogens.
DISCUSSION
The question of antimicrobial prophylaxis in transurethral resection of the prostate remains debatable in the literature. Since some asymptomatic urinary tract infections may sub- side spontaneously, some urologists believe that it is safer to treat a urinary tract infection when it occurs according to the infecting organism than to administer antimicrobials to ev- ery patient. Additionally, there is some concern about the development of resistance with the widespread use of fluoro- quinolones.6 In 1979 Chodak and Plaut were unable to draw definite conclusions regarding the benefit of antimicrobial prophylaxis in urological surgery, mainly because of the poor design of the studies reviewed, and they called for prospec- tive, randomized, controlled trials.? Since then, many such studies have been published but none has completely ended the dispute.
Our study adds to the growing information indicating that antimicrobial prophylaxis is also beneficial in patients with preoperatively sterile urine who undergo transurethral sur- gery. We used an oral fluoroquinolone (1 tablet fleroxacin daily as long as the urinary catheter was in place) for pro- phylaxis in patients undergoing transurethral surgery, which significantly decreased the postoperative urinary tract infection rate from 23 to 3%. Because the study groups were comparable and there was even a trend for shorter postoper- ative urinary catheter drainage in the placebo group, this decrease appears to be the sole effect of the prophylaxis, which is in accordance with many studies addressing this issue. Madsen et a1 reviewed the more recent studies and concluded that routine antimicrobial prophylaxis is recom- mended for patients undergoing transurethral resection of the prostate.8 Table 3 lists a selection of controlled studies (prophylaxis versus placebo or no treatment) during the last decade. In 2 studies no effect of prophylaxis was noted on the infection rate. Stricker and Grant found that a break in the closed drainage system was far more important than use of antimicrobials.9 Houle et a1 found an unmatched low bacte- riuria number even in the control group, which was not explained.10 All other studies demonstrated statistically sig- nificant decreases in the infection rate from approximately 30 to well below 10%. Particularly the more recent studies, including those using fluoroquinolonesll. 12 as in our report and those with large numbers of patients,13 uniformly dem- onstrated a clear decrease in infection rate.
Which antimicrobial to administer as well as the route and duration of prophylaxis remain somewhat unclear.14 Ideally,
T ~ L E 3. Controlled studies of antimicrobial prophylaxis in patients undergoing transurethral resection of the prostate %' Infection Rate Level of Simificant
References I
Bacteriuria (colony-forming No. Pts. unitdml.)
Allan and Kumar"2 Not available Prokocirner et al'" More than lo5 Millar e t a12" More than lo5 Desai e t aI2" More than lo5 Stricker and Grantg More than lo5 Taylor e t alZ6 More than lo5 Houle et all0 More than lo5 Abbou et al" More than lo5 Ueda et all2 More than lo4 Slavis e t ai2' More than lo4 Viitanen et all3 More than lo5
More than lo5 Present study More than lo4
* Administered preoperatively. t Significant difference. t Administered Deriooerativelv (before. durine and after surmrv).
Prophylaxis Controls Treated
PtS.
100 90
179 80 93
235 110 80 58
107 396 402
75
Mezlocillin* Cefotaxime: Aztreonad Enoxacin: Ampicillidgentamicin* Temocillint Cefoperazonet Pefloxacint Ofloxacin: Cefonicid* CeRriaxone* Cotrimoxazole* Fleroxacint
20 4
22 8
17 13 0 5
27 12 8
12 3
64: 30+ 32: 38+ 16 24: 2
33: 56: 37: 22: 22t 23;

148
the antimicrobial chosen should be sensitive against all uro-
ORAL FLEROXACIN PROPHYLAXIS IN TRANSURETHRAL SURGERY
laxis in urologic surgery: a critical review. J. Urol., 121: 695, pathogens likely to be encountered, easily administered, free of side effects and cost-effective. Since their development approximately a decade ago, newer fluoroquinolones have been widely used to treat urinary tract infections. These antimicrobial drugs are safe and efficacious against a wide spectrum of gram-negative and gram-positive bacteria, in- cluding most uropathogens. The possibility for oral adminis- tration renders fluoroquinolones an attractive choice for use in urology. We showed that a daily dose of fleroxacin leads to high blood and tissue concentrations, which were several times greater than the minimal inhibitory concentration of most bacteria encountered in the urinary tract.5 This finding is well in accordance with previous studies.15
The regimen of drug administration was slightly different from other similar studies. With further perfection of trans- urethral surgery postoperative urinary catheter drainage be- comes shorter. Because removal of the catheter risks bacte- remia (catheter chills),l6 we chose to administer the drug for as long as the Foley catheter was in place, usually 24 to 48 hours. Thus, most patients received 2 or 3 tablets of fleroxa- cin and this regimen is clinically feasible.
Of 75 patients 9 (12%) had to be excluded from the study due to preoperative urinary tract infection. Even with every reasonable effort to identify bacteriuria preoperatively, up to 19% of the patients will unknowingly be infected during surgery.17 In a study that included these unsuspected cases the treated patients fared significantly better than the non- treated patients with respect to febrile episodes, complica- tions and length of hospital stay.lS In another study up to 21% of men undergoing transurethral resection of the pros- tate for obstruction had a prostatic infection, placing them at high postoperative risk.19 However, 82% of these patients had a negative urine culture preoperatively, which provides sufficient reason to administer antimicrobials prophylacti- cally to patients with preoperatively sterile urine. Moreover, urethral stricture formation has occurred more often in pa- tients who did not receive antimicrobials.20.21
In conclusion, a once daily oral administration of 400 mg. fleroxacin as long as the catheter is in place is safe, effica- cious and clinically feasible to prevent urinary tract infection in patients who undergo transurethral surgery and have sterile urine preoperatively.
Fleroxacin was provided by F. Hoffmann-La Roche Ltd., Basel, Switzerland.
REFERENCES
1. Mebust, W. K, Holtgrewe, H. L., Cockett, A. T. K, Peters, P. C. and Writing Committee: Transurethral prostatectomy: imme- diate and postoperative complications. A cooperative study of 13 participating institutions evaluating 3,885 patients. J . Urol., 141: 243, 1989.
2. Kaiser, A. B.: Antimicrobial prophylaxis in surgery. New Engl. J. Med., 316 1129, 1986.
3. Gasser, T. C., Graversen, P. H. and Madsen, P. 0.: Antimicrobial prophylaxis in surgery. Letter to the Editor. New Engl. J. Med., 316: 1089, 1987.
4. Gasser, T. C., Graversen, P. H. and Madsen, P. 0.: Fleroxacin (Ro 23-6240) distribution in canine prostatic tissue and fluids. Antimicrob. Agents Chemother., 31: 1010, 1987.
5. Naber, K. G., Sorgel, F., Kees, F., Schumacher, H., Metz, R. and Grobecker, H.: In-vitro activity of fleroxacin against isolates causing complicated urinary tract infections and concentra- tions in seminal and prostatic fluid and in prostatic adenoma tissue. J. Antimicrob. Chemother., suppl. D, 22: 199, 1988.
6. Ena, J., Amador, C., Martinez, C. and de la Tabla, V. 0.: Risk factors for acquisition of urinary tract infections caused by ciprofloxacin resistant Escherichia coli. J . Urol., 153: 117, 1995.
7. Chodak, G. W. and Plaut, M. E.: Systemic antibiotics for prophy-
1979. 8. Madsen, P. O., Larsen, E. H. and Dorflinger, T.: The role of
antibacterial prophylaxis in urologic surgery. Urology, suppl., 26 38, 1985.
9. Stricker, P. D. and Grant, A. B.: Relative value of antibiotics and catheter care in the prevention of urinary tract infection after transurethral prostatic resection. Brit. J . Urol., 61: 494, 1988.
10. Houle, A. M., Mokhless, I., Sarto, N. and Elhilali, M. M.: Peri- operative antibiotic prophylaxis for transurethral resection of the prostate: is it justifiable? J . Urol., 142 317, 1989.
11. Abbou, C., Chopin, D., Nguyen, M., Theodon, P., Antiphon, P., Goulois, R. and Bouleau, D.: Short-term pefloxacin prophy- laxis in transurethral resection of the prostate. Rev. Infect. Dis., suppl. 5, 11: S1361, 1989.
12. Ueda, S., Matsuoka, K., Yamashita, T., Yoshitake, N., Yoshizumi, O., Noguchi, M., Hayashi, K, Noda, S. and Eta, K.: Antibiotic prophylaxis with ofloxacin in patients undergoing transurethral prostatectomy. In: Proceedings 3rd Interna- tional Symposium on New Quinolones, Vancouver, Canada, July 12-14,1990, Eur. J . Clin. Microbiol. Infect. Dis., suppl., p. 322, 1991.
13. Viitanen, J., Talja, M., Jussila, E., Nurmi, M., Permi, J., Puolakka, V.-M., Rintala, E., Salmela, H., Tiitinen, J., Tuhkanen, K. and Elo, J.: Randomized controlled study of chemoprophylaxis in transurethral prostatectomy. J . Urol., 150 1715, 1993.
14. Mebust, W. K.: Prophylactic antibiotics in transurethral surgery. J . Urol., 160 1734, 1993.
15. Cullmann, W., Geddes, A. M., Weidekamm, E., Urwyler, H. and Braunsteiner, A,: Fleroxacin: a review of its chemistry, micro- biology, toxicology, pharmacokinetics, clinical efficacy and safety. Int. J . Antimicrob. Agents, 2: 203, 1993.
16. Sullivan, N. M., Sutter, V. L., Mims, M. M., Marsh, V. H. and Finegold, S. M.: Clinical aspects of bacteremia after manipu- lation of the genitourinary tract. J. Infect. Dis., 127: 49, 1973.
17. Shearman, C. P.: Antibiotic prophylaxis in transurethral pros- tatectomy. Letter to the Editor. Brit. J. Surg., 7 4 653, 1987.
18. Hargreave, T. B., Hindmarsh, J. R., Elton, R., Chisholm, G. D. and Gould, J. C.: Short-term prophylaxis with cefotaxime for prostatic surgery. Brit. Med. J . 284: 1008, 1982.
19. Gorelick, J . I., Senterfit, L. B. and Vaughan, E. D., Jr.: Quanti- tative bacterial tissue cultures from 209 prostatectomy speci- mens: findings and implications. J . Urol., 1 3 9 57, 1988.
20. Grabe, M. and Hellsten, S.: Long-term follow-up after transure- thral prostatic resection with or without a short pen-operative antibiotic course. Brit. J. Urol., 57: 444. 1985.
21. Hammarsten, J . and Lindqvist, K.: Norfloxacin as prophylaxis against urethral strictures following transurethral resection of the prostate: an open, prospective, randomized study. J. Urol., 150 1722, 1993.
22. Allan, W. R. and Kumar, A,: Prophylactic mezlocillin for trans- urethral prostatectomy. Brit. J. Urol., 57: 46, 1985.
23. Prokocimer, P., Quazza, M., Gibert, C., Lemoine, J. E., Joly, M. L., Dureuil, B., Moulonguet, A,, Manuel, C. and Desmonts, J . M.: Short-term prophylactic antibiotics in patients under- going prostatectomy: report of a double-blind randomized trial with 2 intravenous doses of cefotaxime. J. Urol., 135: 60, 1986.
24. Millar, M. R., Inglis, T., Ewing, R., Clark, P., Williams, R. E. and Lacey, R. W.: Double-blind study comparing aztreonam with placebo for prophylaxis of infection following prostatic surgery. Brit. J. Urol., 6 0 345, 1987.
25. Desai, K. M., Abrams, P. H. and White, L. 0.: A double-blind comparative trial of short-term orally administered enoxacin in the prevention of urinary infection after elective transure- thral prostatectomy: a clinical and pharmacokinetic study. J. Urol., 139 1232, 1988.
26. Taylor, E. W. and Lindsay, G.: Antibiotic prophylaxis in trans- urethral resection of the prostate with reference to the influ- ence of preoperative catheterization. J. Hasp. Infect., 12: 75, 1988.
27. Slavis, A. S., Miller, J. B., Golji, H. and Dunshee, C. J.: Compar- ison of single-dose antibiotic prophylaxis in uncomplicated transurethral resection of the prostate. J. Urol., 147: 1303, 1992.