Oral complications of radiotherapy in head and neck cancer
8
Am J Cancer 2004; 3 (5): 291-298 THERAPY IN PRACTICE 1175-6357/04/0005-0291/$31.00/0 © 2004 Adis Data Information BV. All rights reserved. Oral Complications of Radiotherapy in Head and Neck Cancer Strategies for Prevention and Management Cai Grau, Christian N. Andreassen, Kenneth Jensen and Jacob C. Lindegaard Department of Oncology and Department of Experimental Clinical Oncology, Aarhus University Hospital, Aarhus, Denmark Contents Abstract ............................................................................................................... 291 1. Acute Adverse Effects .............................................................................................. 292 1.1 Mucositis ....................................................................................................... 292 1.2 Skin Reactions .................................................................................................. 292 1.3 Other Acute Effects ............................................................................................. 292 2. Late Adverse Effects ................................................................................................ 293 2.1 Fibrosis ......................................................................................................... 293 2.2 Xerostomia ..................................................................................................... 293 2.3 Osteoradionecrosis ............................................................................................. 293 3. Radiobiologic Considerations ........................................................................................ 293 3.1 Time, Dose, Fractionation ........................................................................................ 293 3.2 Volume Effects ................................................................................................. 294 3.3 Chemoradiotherapy ............................................................................................ 295 4. Pharmacologic Intervention .......................................................................................... 295 4.1 Topical Mucosal Protectants ..................................................................................... 295 4.2 Pilocarpine ..................................................................................................... 295 4.3 Amifostine ...................................................................................................... 296 4.4 Cytokine Modulation ............................................................................................ 296 5. Conclusion ......................................................................................................... 297 Radiotherapy in the head and neck region constitutes a major therapeutic challenge. Tumors and elective Abstract nodal areas are often in close proximity to radiosensitive normal tissues, a factor which often limits the success of radiotherapy. Acute radiation-induced adverse effects such as mucositis and skin reactions occur during the course of treatment. They are generally reversible and patients normally recover from these adverse effects within 3 months. Late radiation reactions such as fibrosis and osteoradionecrosis occur more than 3 months after treatment. Such reactions are characterized by their gradual progression. Xerostomia is the single most important factor leading to chronic loss of quality of life in head and neck cancer patients. Oral complications can be prevented or modified by altered fractionation, by reducing the irradiated volume, or by pharmacologic intervention. Altered fractionation in the form of acceleration or hyperfractionation has improved the therapeutic ratio in several large clinical studies and a recent meta-analysis. Reducing the high-dose volume, and especially avoiding irradiating sensitive structures, is the basis for the increasing use of conformal and intensity-modulated radiotherapy. Such techniques may eventually allow dose escalation in tumor areas leading to increased local tumor control while keeping morbidity at an acceptable level.
-
Upload
kenneth-jensen -
Category
Documents
-
view
213 -
download
0
Transcript of Oral complications of radiotherapy in head and neck cancer

Am J Cancer 2004; 3 (5): 291-298THERAPY IN PRACTICE 1175-6357/04/0005-0291/$31.00/0
© 2004 Adis Data Information BV. All rights reserved.
Oral Complications of Radiotherapy in Head andNeck CancerStrategies for Prevention and Management
Cai Grau, Christian N. Andreassen, Kenneth Jensen and Jacob C. Lindegaard
Department of Oncology and Department of Experimental Clinical Oncology, Aarhus University Hospital, Aarhus, Denmark
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2911. Acute Adverse Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292
1.1 Mucositis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2921.2 Skin Reactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2921.3 Other Acute Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 292
2. Late Adverse Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2932.1 Fibrosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2932.2 Xerostomia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2932.3 Osteoradionecrosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 293
3. Radiobiologic Considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2933.1 Time, Dose, Fractionation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2933.2 Volume Effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2943.3 Chemoradiotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295
4. Pharmacologic Intervention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2954.1 Topical Mucosal Protectants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2954.2 Pilocarpine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2954.3 Amifostine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2964.4 Cytokine Modulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 296
5. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297
Radiotherapy in the head and neck region constitutes a major therapeutic challenge. Tumors and electiveAbstractnodal areas are often in close proximity to radiosensitive normal tissues, a factor which often limits the success ofradiotherapy.
Acute radiation-induced adverse effects such as mucositis and skin reactions occur during the course oftreatment. They are generally reversible and patients normally recover from these adverse effects within 3months. Late radiation reactions such as fibrosis and osteoradionecrosis occur more than 3 months aftertreatment. Such reactions are characterized by their gradual progression. Xerostomia is the single most importantfactor leading to chronic loss of quality of life in head and neck cancer patients.
Oral complications can be prevented or modified by altered fractionation, by reducing the irradiated volume,or by pharmacologic intervention. Altered fractionation in the form of acceleration or hyperfractionation hasimproved the therapeutic ratio in several large clinical studies and a recent meta-analysis. Reducing thehigh-dose volume, and especially avoiding irradiating sensitive structures, is the basis for the increasing use ofconformal and intensity-modulated radiotherapy. Such techniques may eventually allow dose escalation intumor areas leading to increased local tumor control while keeping morbidity at an acceptable level.

292 Grau et al.
Numerous pharmacologic agents have been evaluated for the prevention and management of both acute andlate complications. The only agent with documented radioprotective activity is amifostine, which can reduce latexerostomia. However, it is still unclear whether amifostine also protects tumor cells. Pilocarpine may relieve latexerostomia in some patients with remaining functional salivary gland reserve. Apart from this limited indication,pharmacologic agents against oral complications should not be used outside of clinical trials.
Head and neck cancers are relatively rare in Europe and occurs 5–7 weeks after the start of radiotherapy, depending on theAmerica, constituting less than 2% of all malignant diseases. On intensity of the regimen.the Indian subcontinent and in other parts of Asia, carcinomas of Mucositis can be very painful, and patients with confluentthe oral cavity and pharynx rank among the most common cancers. mucositis often require opioid treatment. The condition often leadsThe majority of tumors are squamous cell carcinoma, originating to impaired food intake and hospitalization for tube feeding and/orin the mucosal layer of the upper aerodigestive tract. gastrostomy. Breakage of the mucosal barrier also increases the
Most tumors of the head and neck can be effectively managed risk of opportunistic infections.with radiotherapy either alone or in combination with surgery and/or chemotherapy. A typical course of radiotherapy is 60–70Gy in 1.2 Skin Reactions30–40 fractions over 5–7 weeks. The overall 5-year survival forhead and neck carcinoma averages 50% but is heavily influenced
During treatment the skin in the radiation field gradually be-by the extent of the primary tumor and nodal metastases. For
comes red and irritated. In about one-third of patients the surfaceexample, superficial stage I oral cavity lesions can have a locore-
epithelium abrades and causes dry or, in severe cases, moistgional cure rate of >80% compared with <30% for stage IV
desquamation or ulceration in parts of or over the entire radiationdisease in the same region.[1]
field.[3] The severity of the skin reaction depends on the areaRadiotherapy in the head and neck region constitutes a major irradiated and the radiation dose deposited in the outer few milli-
therapeutic challenge. Tumors and elective nodal areas are often in meters. The use of low photon energy, electrons, thick thermoplas-close proximity to radiosensitive normal tissues, a factor which tic mask, or bolus, increases the skin doses and hence the degree ofoften limits the success of radiotherapy. This article describes the skin reactions.most common oral complications radiotherapy for head and neckcancer, as well as current and future strategies for the prevention
1.3 Other Acute Effectsand management of these complications.
Edema of the irradiated tissue is a part of the inflammatory1. Acute Adverse Effectsresponse to radiotherapy-induced trauma. In the oral cavity, edemamay cause problems with swallowing and denture fitting. MostAdverse effects from radiation are typically divided into acutepatients notice dryness of the mouth, changes in taste and loss ofand late reactions. Acute radiation-associated side effects developappetite during the course of radiotherapy.[2]
during the course of treatment. Such effects occur in rapidlyproliferating tissues. They are generally reversible and patientsnormally recover from these adverse effects within 3 months afterradiotherapy.[2]
1.1 Mucositis
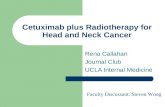
Radiotherapy associated mucositis in the oral cavity is animportant acute reaction since it leads to pain and dysfunction. Thesurface epithelium is partly or completely abraded and the sub-mucosa denuded. Most patients experience patchy or confluentmucositis during a course of curative radiotherapy.[3] Figure 1shows confluent mucositis on the palate in the fifth week ofradiotherapy for oropharyngeal cancer. The maximum reaction
Fig. 1. Example of confluent mucositis in a patient treated with opposedlateral fields for oropharyngeal cancer. The picture was taken in week 5 ofaccelerated radiotherapy (6 fractions per week).
© 2004 Adis Data Information BV. All rights reserved. Am J Cancer 2004; 3 (5)

Oral Complications in Head and Neck Radiotherapy 293
2. Late Adverse Effects mus, multiple discharging fistulae, a large area of exposed bone, ora coexisting fracture.[8,12,13]
Late radiation reactions occur more than 3 months after treat-ment. The reactions are characterized by their gradual progression; 3. Radiobiologic Considerationsthey are generally irreversible and occur in slowly proliferatingtissue.
3.1 Time, Dose, Fractionation
2.1 Fibrosis Primary radiotherapy with curative intent for head and neckcancer has traditionally required 66–70Gy in 1.8–2.0Gy fractionsSubcutaneous and submucosal fibrosis in the irradiated areadelivered five times per week. A substantial number of clinicaldevelops from months to years after treatment. Most cases ofreports indicate that a prolongation in overall treatment time mayfibrosis are subclinical and do not affect patients’ quality of life. Inresult in loss of tumor control.[14-16] Several clinical studies and amore severe cases, fibrosis can lead to trismus, impaired functionrecent meta-analysis have documented the beneficial effect ofof the tongue and other structures in the aerodigestive tube. Thisaltered fractionation in the form of acceleration (shorter overallcan lead to swallowing problems and chronic malnutrition. Be-treatment times) or hyperfractionation (smaller doses per fraction).cause of the severity of these complications, fibrosis has always
The Danish Head and Neck Cancer Study Group (DAHANCA)been a significant dose-limiting factor in radiotherapy.6 & 7 trial tested moderate acceleration by comparing two strate-gies with the same total dose (66Gy in 33 fractions) given with
2.2 Xerostomiaeither five or six fractions per week.[17] Between January 1992 andDecember 1999, of the 1485 patients treated with primary radio-All salivary glands are radiosensitive, and severe irreversibletherapy alone, 1476 elgible patients were randomly assigned todysfunction is noticed at 26–30Gy, i.e. at a dosage much belowreceive five (n = 726) or six (n = 750) fractions per week at thethat required to cure the patient.[4] Consequently, xerostomia is ansame total dose and fraction number. The median overall treatmentextremely common adverse effect of head and neck radiotherapy.times were 39 days (six-fraction group) and 46 days (five-fractionXerostomia may cause impaired chewing, swallowing, andgroup). Overall, the 5-year locoregional control rates were 70%speech, as well as dental problems. Xerostomia is the single mostand 60% for the six-fraction and five-fraction groups, respectivelyimportant factor leading to loss of quality of life in head and neck(p = 0.0005). Disease-specific survival improved (73 vs 66% forcancer patients.[5,6]
six and five fractions, p = 0.01) but not overall survival. The rate ofacute radiation-related morbidity was significantly higher in the2.3 Osteoradionecrosisaccelerated fractionation group with a 53% incidence of confluentmucositis compared with 33% in the conventional treatment groupOsteoradionecrosis is a clinical diagnosis based on mucosal(p < 0.0001). The mucositis healed within 3 months of the start ofulceration and bone exposure lasting more than 3 months. Thetreatment. The probability of developing any severe late radiation-pathophysiologic explanation for the late changes in the bone isrelated complication, mainly in the form of late cutaneous fibrosis,related to vascular damage. Osteoradionecrosis is often initiatedmucosal atrophy, or necrosis, did not differ significantly betweenby dental extraction, denture pressure, or other mechanical trauma.the fractionation groups. Six fractions per week is now standardWith proper pre-radiotherapy dental evaluation with revision ofbaseline treatment in Denmark.all potential infectious foci, and with dental care including caries
A Polish study has taken this rationale further.[18] The trialprophylaxis during and after radiotherapy, the risk of osteoradion-randomized patients with head and neck cancers to receive sevenecrosis can be kept below 5%.[7] Limited lesions can often beradiation treatments of 2Gy per week each or the conventional fivecontrolled with conservative measures.[8] Hyperbaric oxygen treat-fractions per week of 2Gy each. The authors found an unaccept-ment induces neovascularization and thereby increased healingably high rate of acute and consequential late complications in thecapacity. It has a well documented role in the prevention of7-day arm. They are now using a smaller fraction size of 1.8Gy perosteoradionecrosis associated with post-irradiation tooth extrac-fraction and the consequential late damage has been reducedtion and other minor or major surgery in the irradiated area, andsignificantly.also in the treatment of osteoradionecrosis together with seques-
trectomy.[9-11] Resection or reconstructive surgery, often combined The Vancouver Cancer Centre tested accelerated fractionationwith hyperbaric oxygen before and after surgery, is recommended by giving two daily fractions of 2Gy compared with conventionalas primary treatment in patients with excessive pain, severe tris- treatment in a phase III trial.[19] Grade 3 and 4 acute toxicity was
© 2004 Adis Data Information BV. All rights reserved. Am J Cancer 2004; 3 (5)

294 Grau et al.
significantly higher in the accelerated arm, leading to closure of involving 6515 patients were included. The median follow-upthe study after accrual of 82 patients. There was no between-group period was 5.8 years. For accelerated or hyperfractionated radio-difference in tumor control. therapy, an absolute survival benefit of 3% for accelerated or
The concept of hyperfractionation was initially tested in the hyperfractionated radiotherapy, from 36% to 39%, at 5 years andEORTC (European Organisation for Research and Treatment of an absolute benefit on locoregional control of 7% from 46% toCancer) protocol 22791.[20] The trial compared conventional frac- 53% were found. An absolute 5% improvement in locoregionaltionation of 70Gy in 35–40 fractions in 7–8 weeks with 80.5Gy in control by modified fractionation was seen.70 fractions in 7 weeks using two fractions of 1.15Gy per day. A
In conclusion, numerous clinical studies have documented thattotal of 356 patients were entered. Local tumor control was signifi-
altered fractionation – by moderate acceleration and/or hyperfrac-cantly higher in the hyperfractionation arm (59% vs 40%). A trend
tionation – is beneficial compared with conventional fractionationtoward improved survival was also noted. There was no difference
and should be considered as standard in contemporary head andin late normal tissue damage between the two treatment modali-
neck radiotherapy.ties.
The RTOG (Radiation Therapy Oncology Group) 90-03 study3.2 Volume Effectscompared the efficacy of hyperfractionation and two types of
accelerated fractionation individually against standard fractiona-tion.[21] The four arms were as follows: standard fractionation at There is a clear correlation between the amount of irradiated2Gy per fraction per day; hyperfractionation at 1.2Gy per fraction tissue and the risk and severity of both acute and late oral compli-twice daily to 81.6Gy/68 fractions/7 weeks; accelerated fractiona- cations. This is called the volume effect. In conventional head andtion with a 2-week split after 38.4 Gy; and accelerated fractiona- neck radiotherapy using opposed lateral fields (figure 2), the fieldtion with concomitant boost for the last 12 treatment days to 72Gy/ size is a reasonable surrogate for the irradiated volume. Figure 342 fractions/6 weeks. This large trial (1113 patients) showed that shows the influence of field size on acute mucosal and skinpatients treated with hyperfractionation and accelerated fractiona- reactions as well as late fibrosis.[25] Another tissue with cleartion with concomitant boost had significantly better locoregional volume dependency is the parotid gland. Several studies havecontrol (p = 0.045 and p = 0.050, respectively) than those treated shown that sparing a proportion of the total gland mass maywith standard fractionation. There was also a trend toward im- prevent late xerostomia.[4,26-28] An example of this effect is shownproved disease-free survival (p = 0.067 and p = 0.054, respective- in figure 4: a series of 61 patients with oropharyngeal cancer werely) although the difference in overall survival was not significant.
treated either with bilateral fields encompassing both parotids orPatients treated with accelerated fractionation with split had a
with ipsilateral wedged pairs sparing the contralateral gland. Pa-similar outcome to those treated with standard fractionation. All
tients in the latter group had significantly less grade 3 xeros-three altered fractionation groups had significantly more acute
tomia.[4,26,29]adverse effects than the standard fractionation group. There wasno significant increase in late effects.
Other studies have used a combination of acceleration andhyperfractionation. In the Medical Research Council study withCHART (continuously hyperfractionated accelerated radiother-apy), a compressed schedule with 54Gy in 36 fractions over 12days was tested versus conventional radiotherapy.[22] Although nooverall difference in treatment outcome was observed, the resultsdemonstrate that the total dose can be reduced if the overalltreatment time is also reduced. The EORTC 22851 randomizedtrial compared conventional radiotherapy (70Gy/35 fractions/7weeks) with 72Gy/45 fractions/32 days given as accelerated split-course therapy.[23] In this study a significant increase in locore-gional control was achieved, but at the expense of a significantincrease in both acute and late morbidity.
A recent meta-analysis has compiled a large amount of frac-tionation data.[24] Fifteen randomized trials (from 1970 to 1998)
Fig. 2. Schematic representation of typical opposed lateral fields used innon-conformal (two-dimensional) radiotherapy of head and neck cancer.
© 2004 Adis Data Information BV. All rights reserved. Am J Cancer 2004; 3 (5)

Oral Complications in Head and Neck Radiotherapy 295
sucralfate, used for mechanical stabilization of the eroded mucosa,and various antibiotics, antiseptics, and immunoglobulins aimed atreducing secondary infections. The mitotic activity in the basalcell layer has been stimulated by topical silver nitrate or hydrogenperoxide application.
A recent meta-analysis identified 59 studies within this area.[40]
Overall, the interventions reduced the odds of developing severeoral mucositis by 36%. Subgroup analysis suggested that only thenarrow-spectrum antibacterial lozenges were effective. The powerof the aggregated data for the other drug classes was insufficient todetect differences. Perhaps more importantly, when the outcomeof treatment was assessed by patients, no significant differencewas seen between the treatment and the control groups. Methodo-logic limitations were evident in many of the studies.
Field size (cm2)
40 60 80 100 120 140 160
Per
cent
age
of p
atie
nts
0
20
40
60
80
100 Skin desquamationConfluent mucositisSubcutaneous fibrosis
Fig. 3. Influence of field size on the incidence of acute and late reactions.Data from the International Atomic Energy Agency (IAEA) mitomycin trial(n = 458).[25]
Based on the current data, there is no unequivocal evidence to3.3 Chemoradiotherapy justify the use of such agents outside clinical trials.
The concomitant use of cisplatin-based chemotherapy during4.2 Pilocarpineradiotherapy has been shown to improve outcomes in advanced
head and neck tumors.[30] Given the same intensity of radiother-Pilocarpine has been evaluated as a treatment for xerostomia. Inapy, chemotherapy causes a large increase in the incidence of
the post-irradiation setting, pilocarpine seems to alleviate subjec-acute skin and mucosal reactions.[31-34] By lowering the radiationtive xerostomia, presumably by stimulating remaining functionaldose and introducing a treatment break, the acute toxicity of thesalivary glands. Johnson et al.[41] studied 207 patients who hadcombined regimen becomes less pronounced,[35,36] but such aneach received 40Gy or more. Pilocarpine improved saliva produc-approach raises the question of whether a similar therapeutiction and significantly relieved symptoms of xerostomia after irra-outcome could have been obtained by radiotherapy alone.diation for cancer of the head and neck, with minor adverse effectsCompared with radiotherapy alone, chemoradiotherapy seemsthat were predominantly limited to sweating. Similar results haveto increase late toxicity, but to various degrees.[32-35,37-39] However,been shown in a French cooperative study.[42]
good morbidity data, especially concerning late toxicity, aresparse. More chemoradiotherapy studies with normal tissue end-points are needed.
4. Pharmacologic Intervention
Over the years, numerous attempts have been made to developpharmacologic strategies to protect normal tissues against theeffects of radiation. Efforts have focused on the important andfrequent adverse reactions such as mucositis, fibrosis, and xeros-tomia. Systemically, a large number of substances have shownvariable degrees of radioprotective properties. However, the vastmajority of these are either too weak in terms of radioprotection,too toxic, or without any apparent mechanisms to ensure selectivenormal tissue protection. Therefore, only a very limited number ofsubstances are currently of clinical relevance for the preventionand treatment of radiation-induced adverse events.[40]
4.1 Topical Mucosal Protectants
Topical strategies to modify mucositis include a heterogeneousgroup of agents with different attack points. Examples are
Xerostomia grade
Per
cent
age
of p
atie
nts
0
20
40
60
80
0 1 2 3
Ipsilateral RT (n = 27)Bilateral RT (n = 34)
Fig. 4. Subjective xerostomia recorded in patients receiving either parotid-sparing ipsilateral conformal radiotherapy (RT) or conventional bilateralfields for oropharyngeal carcinoma. All between-treatment differenceswere significant (p < 0.0001). From K. Jensen and C. Grau (unpublisheddata).
© 2004 Adis Data Information BV. All rights reserved. Am J Cancer 2004; 3 (5)

296 Grau et al.
While pilocarpine seems to be useful for the treatment of late 4.4 Cytokine Modulationxerostomia, its use during radiotherapy for prevention or reductionof subsequent radiation-induced xerostomia is still equivocal. Increasing evidence indicates that both acute and late normalHaddad and Karimi[43] performed a small randomized trial with tissue reactions after radiotherapy are closely related to persistentpilocarpine 5mg three times daily. Compared with placebo, pilo- overproduction of certain cytokines such as interleukin (IL)-1,carpine significantly reduced subsequent radiation-induced xeros-
IL-6, IL-10, tumor necrosis factor-α, and transforming growthtomia. A Canadian study by Warde and coworkers,[44] however,
factor (TGF)-β.[45] It is assumed that a cascade reaction is initiatedcame to a different conclusion. Patients (n = 130) were random-immediately after irradiation and that this cascade remains activeized in a double-blind manner to receive either pilocarpine ormonths or years after radiotherapy.[51,52] TGF-β1 seems to play aplacebo three times daily starting on the first day of radiotherapy
and continuing for 1 month after treatment. No difference was crucial role in the development of radiation-induced fibrosis.[53]
observed between the pilocarpine-treated patients and the placebo Ameliorating radiation-induced damage by pharmacologicallygroup in the severity of xerostomia score as assessed by linear
manipulating inflammatory and profibrotic cytokines represents aanalog scale at baseline and 1, 3, and 6 months after treatment. In
fascinating alternative strategy in radioprotection: the list of agentsaddition, no difference was apparent in the severity of mucositis or
includes lisofylline, essential fatty acids, superoxide dismutase,quality of life during radiotherapy.pentoxyfilline and α-tocopherol.[53,54] The sparse data suggest that
such substances may have a role in prevention and amelioration of4.3 Amifostine normal tissue injury. Furthermore, some of these substances seem
to have the ability to reverse established fibrosis, thus providingAmifostine is without doubt the most comprehensively tested the basis for a therapeutic strategy.[55] However, depending on the
radioprotective agent. In head and neck cancer, a series of clinical agent, such toxicity antagonists may carry their own toxicities, andtrials have been conducted to test the ability of amifostine to
manipulation of processes related to growth, differentiation andprotect against mucositis and xerostomia.[45-48] McDonald et al.[47]
repair may also potentially affect tumor response. All these aspectsshowed that amifostine had acceptable tolerability when adminis-
need to be carefully evaluated.tered with daily radiotherapy and improved salivary gland func-tion. From a biologic point of view, this is probably a result of theextreme radiosensitivity of the serous acini combined with arelatively high uptake and retention of amifostine and its metabo-lites in the parotid glands.[45]
A large multicenter trial, with participation from NorthAmerica, Germany, and France, recruited 315 patients in theperiod 1995–1997.[46] Amifostine significantly reduced moderateto severe acute xerostomia, and significantly more patients hadpreserved saliva production. There was no significant difference inthe incidence of acute mucositis between randomization groups.Analysis at the 18-month follow-up showed no significant differ-ence in locoregional tumor control, disease-free survival, or over-all survival for patients treated with or without amifostine. Thetrial was, however, not powered to detect any influence of amifos-tine on local tumor control. This is a major concern, since the drughas been found to cause tumor protection in animal models.[49]
In summary, although it is well documented that clinicallyrelevant radioprotection of the salivary glands can be achievedwith amifostine, the standard use of the drug outside clinicalprotocols seems unjustified.[50] In this context it is important tokeep in mind that protection of salivary glands could also beachieved by conformal avoidance (figure 4 and figure 5).
Fig. 5. Typical wedge-pair field arrangement in a patient receiving parotis-sparing ipsilateral conformal radiotherapy for tonsillar carcinoma. The pa-tient was treated at the Department of Oncology, Aarhus University Hospi-tal, Denmark. The arrows indicate radiation fields.
© 2004 Adis Data Information BV. All rights reserved. Am J Cancer 2004; 3 (5)

Oral Complications in Head and Neck Radiotherapy 297
15. Overgaard J, Hjelm-Hansen M, Johansen LV, et al. Comparison of conventional5. Conclusionand split-course radiotherapy as primary treatment in carcinoma of the larynx.Acta Oncol 1988; 27 (2): 147-52
Radiation therapy in the head and neck area leads to acute and 16. Overgaard J, Alsner J, Eriksen J, et al. Importance of overall treatment time for theresponse to radiotherapy in patients with squamous cell carcinoma of the headlate adverse effects due to the presence of many radiosensitiveand neck. Rays 2000; 25 (3): 313-9structures in the irradiated volume.
17. Overgaard J, Hansen HS, Specht L, et al., on behalf of the Danish Head and NeckThe success of accelerated and hyperfractionated radiotherapy Cancer Study Group. Five compared with six fractions per week of convention-
al radiotherapy of squamos-cell carcinoma of head and neck: DAHANCA 6 & 7regimens has led to an increase in the incidence of acute complica-randomized control trial [published erratum appears in Lancet 2003 Nov 8; 362:
tions, emphasizing the need for good supportive care during 1588]. Lancet 2003; 362: 933-40treatment. Pharmacologic agents to protect against acute adverse 18. Skladowski K, Maciejewski B, Golen M, et al. Randomized clinical trial on 7-day-
continuous accelerated irradiation (CAIR) of head and neck can. Radiothereffects, especially mucositis, have not been successful so far, andOncol 2000; 55 (2): 101-10
these agents should not be used outside clinical trials. The only 19. Jackson SM, Weir LM, Hay JH, et al. A randomised trial of accelerated versusconventional radiotherapy in head and neck cancer. Radiother Oncol 1997; 43agent with documented radioprotective activity is amifostine,(1): 39-46which can reduce late xerostomia. However, it is still undeter-
20. Horiot JC, Le Fur R, N’Guyen T, et al. Hyperfractionation versus conventionalmined whether amifostine also protects tumor cells. Finally, pro- fractionation in oropharyngeal carcinoma: final analysis of a randomized trial
of the EORTC cooperative group of radiotherapy. Radiother Oncol 1992; 25tection against both acute and late complications can be obtained(4): 231-41by reducing the irradiated high-dose volume by conformal or
21. Fu KK, Pajak TF, Trotti A, et al. A Radiation Therapy Oncology Group (RTOG)intensity-modulated radiotherapy. phase III randomized study to compare hyperfractionation and two variants of
accelerated fractionation to standard fractionation radiotherapy for head andneck squamous cell carcinomas: first report of RTOG 9003. Int J Radiat OncolAcknowledgmentBiol Phys 2000; 48 (1): 7-16
22. Dische S, Saunders M, Barrett A, et al. A randomised multicentre trial of CHARTThis review was funded by the Danish Cancer Society. The authors have
versus conventional radiotherapy in head and neck cancer. Radiother Oncolno conflicts of interest that are directly relevant to the content of this review. 1997; 44 (2): 123-36
23. Horiot JC, Bontemps P, van den Bogaert W, et al. Accelerated fractionation (AF)compared to conventional fractionation (CF) improves loco-regional control inReferences the radiotherapy of advanced head and neck cancers: results of the EORTC
1. Greene FL, American Joint Committee on Cancer, American Cancer Society. 22851 randomized trial. Radiother Oncol 1997; 44 (2): 111-21AJCC cancer staging handbook. 6th ed. New York: Springer, 2002 24. Bourhis J, Syz N, Overgaard J, et al. Conventional versus modified fractionated
2. Trotti A. Toxicity in head and neck cancer: a review of trends and issues. Int J radiotherapy: meta-analysis based on Individual data of patients with head andRadiat Oncol Biol Phys 2000; 47 (1): 1-12 neck squamous cell carcinoma (HNSCC) [abstract]. Radiother Oncol 2002; 64
3. Kaanders JH, Ang KK. Early reactions as dose-limiting factors in radiotherapy. Suppl. 1: 25Semin Radiat Oncol 1994; 4 (2): 55-67
25. Grau C, Prakash AJ, Jabeen K, et al. Radiotherapy with or without mitomycin c in4. Eisbruch A, Ten Haken RK, Kim HM, et al. Dose, volume, and function the treatment of locally advanced head and neck cancer: results of the IAEA
relationships in parotid salivary glands following conformal and intensity- multicentre randomised trial. Radiother Oncol 2003; 67 (1): 17-26modulated irradiation of head and neck cancer. Int J Radiat Oncol Biol Phys
26. Lee N, Xia P, Quivey JM, et al. Intensity-modulated radiotherapy in the treatment1999; 45 (3): 577-87of nasopharyngeal carcinoma: an update of the UCSF experience. Int J Radiat
5. Epstein JB, Emerton S, Kolbinson DA, et al. Quality of life and oral functionOncol Biol Phys 2002; 53: 12-22
following radiotherapy for head and neck cancer. Head Neck 1999; 21 (1): 1-1127. Maes A, Weltens C, Flamen P, et al. Preservation of parotid function with6. Jensen AB, Hansen O, Jorgensen K, et al. Influence of late side-effects upon daily
uncomplicated conformal radiotherapy. Radiother Oncol 2002; 63 (2): 203-11life after radiotherapy for laryngeal and pharyngeal cancer. Acta Oncol 1994;28. Hazuka MB, Martel MK, Marsh L, et al. Preservation of parotid function after33 (5): 487-91
external beam irradiation in head and neck cancer patients: a feasibility study7. Friedman RB. Osteoradionecrosis: causes and prevention. Natl Cancer Instusing 3-dimensional treatment planning. Int J Radiat Oncol Biol Phys 1993; 27Monogr 1990; 9: 145-9(3): 731-78. Beumer J, Harrison R, Sanders B, et al. Osteoradionecrosis: predisposing factors
29. Chao KS. Protection of salivary function by intensity-modulated radiation therapyand outcomes of therapy. Head Neck Surg 1984; 6 (4): 819-27in patients with head and neck cancer. Semin Radiat Oncol 2002; 12 (1 Suppl.9. Thorn JJ, Kallehave F, Westergaard P, et al. The effect of hyperbaric oxygen on1): 20-5irradiated oral tissues: transmucosal oxygen tension measurements. J Oral
30. Pignon JP, Bourhis J, Domenge C, et al. Chemotherapy added to locoregionalMaxillofac Surg 1997; 55 (10): 1103-7treatment for head and neck squamous-cell carcinoma: three meta-analyses of10. David LA, Sandor GK, Evans AW, et al. Hyperbaric oxygen therapy andupdated individual data. MACH-NC Collaborative Group. Meta-Analysis ofmandibular osteoradionecrosis: a retrospective study and analysis of treatmentChemotherapy on Head and Neck Cancer. Lancet 2000; 355 (9208): 949-55outcomes. J Can Dent Assoc 2001; 67 (7): 384
31. Adelstein DJ, Saxton JP, Lavertu P, et al. A phase III randomized trial comparing11. Marx RE, Johnson RP, Kline SN. Prevention of osteoradionecrosis: a randomizedconcurrent chemotherapy and radiotherapy with radiotherapy alone in resect-prospective clinical trial of hyperbaric oxygen versus penicillin. J Am Dentable stage III and IV squamous cell head and neck cancer: preliminary results.Assoc 1985; 111 (1): 49-54Head Neck 1997; 19 (7): 567-7512. Jereczek-Fossa BA, Orecchia R. Radiotherapy-induced mandibular bone compli-
32. Wendt TG, Grabenbauer GG, Rodel CM, et al. Simultaneous radiochemotherapycations. Cancer Treat Rev 2002; 28 (1): 65-74versus radiotherapy alone in advanced head and neck cancer: a randomized13. Maier A, Gaggl A, Klemen H, et al. Review of severe osteoradionecrosis treatedmulticenter study. J Clin Oncol 1998; 16 (4): 1318-24by surgery alone or surgery with postoperative hyperbaric oxygenation. Br J
Oral Maxillofac Surg 2000; 38 (3): 173-6 33. Calais G, Alfonsi M, Bardet E, et al. Randomized trial of radiation therapy versus14. Withers HR, Taylor JM, Maciejewski B. The hazard of accelerated tumor clonogen concomitant chemotherapy and radiation therapy for advanced-stage oro-
repopulation during radiotherapy. Acta Oncol 1988; 27 (2): 131-46 pharynx carcinoma. J Natl Cancer Inst 1999; 91 (24): 2081-6
© 2004 Adis Data Information BV. All rights reserved. Am J Cancer 2004; 3 (5)

298 Grau et al.
34. Olmi P, Crispino S, Fallai C, et al. Locoregionally advanced carcinoma of the 45. Takahashi I, Nagai T, Miyaishi K, et al. Clinical study of the radioprotectiveoropharynx: conventional radiotherapy vs accelerated hyperfractionated radio- effects of Amifostine (YM-08310, WR-2721) on chronic radiation injury. Int Jtherapy vs concomitant radiotherapy and chemotherapy: a multicenter random- Radiat Oncol Biol Phys 1986; 12 (6): 935-8ized trial. Int J Radiat Oncol Biol Phys 2003; 55 (1): 78-92
46. Brizel DM, Wasserman TH, Henke M, et al. Phase III randomized trial of35. Brizel DM, Albers ME, Fisher SR, et al. Hyperfractionated irradiation with or amifostine as a radioprotector in head and neck cancer. J Clin Oncol 2000; 18
without concurrent chemotherapy for locally advanced head and neck cancer. N(19): 3339-45
Engl J Med 1998; 338 (25): 1798-80447. McDonald S, Meyerowitz C, Smudzin T, et al. Preliminary results of a pilot study
36. Merlano M, Benasso M, Corvo R, et al. Five-year update of a randomized trial ofusing WR-2721 before fractionated irradiation of the head and neck to reduce
alternating radiotherapy and chemotherapy compared with radiotherapy alonesalivary gland dysfunction. Int J Radiat Oncol Biol Phys 1994; 29 (4): 747-54in treatment of unresectable squamous cell carcinoma of the head and neck. J
Natl Cancer Inst 1996; 88 (9): 583-9 48. Bourhis J, De Crevoisier R, Abdulkarim B, et al. A randomized study of very
accelerated radiotherapy with and without amifostine in head and neck squa-37. Denis F, Garaud P, Bardet E, et al. Late toxicity results of the GORTEC 94-01mous cell carcinoma. Int J Radiat Oncol Biol Phys 2000; 46 (5): 1105-8randomized trial comparing radiotherapy with concomitant radiochemotherapy
for advanced-stage oropharynx carcinoma: comparison of LENT/SOMA, 49. Lindegaard JC, Grau C. Has the outlook improved for amifostine as a clinicalRTOG/EORTC, and NCI-CTC scoring systems. Int J Radiat Oncol Biol Phys radioprotector? Radiother Oncol 2000; 57 (2): 113-82003; 55 (1): 93-8
50. Lindegaard JC. Has the time come for routine use of amifostine in clinical38. Staar S, Rudat V, Stuetzer H, et al. Intensified hyperfractionated accelerated
radiotherapy practice? Acta Oncol 2003; 42 (1): 2-3radiotherapy limits the additional benefit of simultaneous chemotherapy: results
51. Herskind C, Bamberg M, Rodemann HP. The role of cytokines in the developmentof a multicentric randomized German trial in advanced head-and-neck cancer.of normal-tissue reactions after radiotherapy. Strahlenther Onkol 1998; 174Int J Radiat Oncol Biol Phys 2001; 50 (5): 1161-71
Suppl. 3: 12-539. Henk JM. Controlled trials of synchronous chemotherapy with radiotherapy in52. Hill RP, Rodemann HP, Hendry JH, et al. Normal tissue radiobiology: from thehead and neck cancer: overview of radiation morbidity. Clin Oncol (R Coll
Radiol) 1997; 9 (5): 308-12 laboratory to the clinic. Int J Radiat Oncol Biol Phys 2001; 49 (2): 353-65
53. Martin M, Lefaix J, Delanian S. TGF-beta1 and radiation fibrosis: a master switch40. Sutherland SE, Browman GP. Prophylaxis of oral mucositis in irradiated head-and-neck cancer patients: a proposed classification scheme of interventions and and a specific therapeutic target? Int J Radiat Oncol Biol Phys 2000; 47 (2):meta-analysis of randomized controlled trials. Int J Radiat Oncol Biol Phys 277-902001; 49 (4): 917-30
54. Trotti A. Toxicity antagonists in head and neck cancer. Semin Radiat Oncol 1998;41. Johnson JT, Ferretti GA, Nethery WJ, et al. Oral pilocarpine for post-irradiation 8 (4): 282-91
xerostomia in patients with head and neck cancer. N Engl J Med 1993; 329 (6):55. Lefaix JL, Delanian S, Vozenin MC, et al. Striking regression of subcutaneous390-5
fibrosis induced by high doses of gamma rays using a combination of pentoxi-42. Horiot JC, Lipinski F, Schraub S, et al. Post-radiation severe xerostomia relieved
fylline and alpha-tocopherol: an experimental study. Int J Radiat Oncol Biolby pilocarpine: a prospective French cooperative study. Radiother Oncol 2000;
Phys 1999; 43 (4): 839-4755 (3): 233-9
43. Haddad P, Karimi M. A randomized, double-blind, placebo-controlled trial ofconcomitant pilocarpine with head and neck irradiation for prevention of Correspondence and offprints: Dr Cai Grau, Department of Oncology,radiation-induced xerostomia. Radiother Oncol 2002; 64 (1): 29-32
Aarhus University Hospital, Norrebrogade 44, Bldg 5, DK-8000 Aarhus C,44. Warde P, O’Sullivan B, Aslanidis J, et al. A phase III placebo-controlled trial of
Denmark.oral pilocarpine in patients undergoing radiotherapy for head-and-neck cancer.E-mail: [email protected] J Radiat Oncol Biol Phys 2002; 54 (1): 9-13
© 2004 Adis Data Information BV. All rights reserved. Am J Cancer 2004; 3 (5)