Optimal Nutritional Goals for the Cancer...
39
Optimal Nutritional Goals for the Cancer Survivor WENDY DEMARK-WAHNEFRIED, PHD, RD PROFESSOR AND WEBB CHAIR OF NUTRITION SCIENCES ASSOCIATE DIRECTOR OF CANCER PREVENTION & CONTROL UNIVERSITY OF ALABAMA AT BIRMINGHAM WORKING EVERYDAY TO PROVIDE THE HIGHEST QUALITY OF LIFE FOR PEOPLE WITH CANCER
Transcript of Optimal Nutritional Goals for the Cancer...

Optimal Nutritional Goals for
the Cancer Survivor
W E N D Y D E M AR K - WAH N E F R I E D , P H D , R D
P R O F E S S O R AN D W E B B C H AI R O F N U T R I T I O N S C I E N C E S
AS S O C I AT E D I R E C T O R O F C AN C E R P R E V E N T I O N & C O N T R O L
U N I V E R S I T Y O F AL AB A M A AT B I R M I N G H AM
W O R K I N G E V E R Y D A Y T O P R O V I D E T H E H I G H E S T Q U A L I T Y O F L I F E F O R P E O P L E W I T H C A N C E R

Disclosures
AFFILIATION/FINANCIAL
INTERESTS
(prior 12 months)
CORPORATE
ORGANIZATION
Grants/Research Support: No
Corporate
Sponsorship
Scientific Advisory
Board/Consultant:
Speakers Bureau:
Stock Shareholder:
Other

Objectives By the end of this presentation, the observer should be able to…
• Recognize trends in cancer prevalence, mortality and survivorship.
• Identify common issues in cancer survivorship.
• Identify diet and physical activity guidelines for
cancer survivorship and outline the rationale that
supports them.
• List some of the gaps in knowledge related to
nutrition and cancer survivorship
• Identify reliable sources for nutrition and cancer
information.



Number of Cancer Survivors is Steadily
Rising Good News!
14.5 M!

Cancer Survivors at greater risk
- Progressive disease
- Second primaries
- Cardiovascular Disease
- Diabetes
- Osteoporosis
- Sarcopenia
- Functional decline
Cancer Survivorship:
The Bad News

% with Limitations:
Survivors vs. General Population
Hewitt, Rowland, Yancik. J Gerontol. 58:82, 2003

Possible Solutions
Diet Exercise
Depression
Fatigue
Adverse Body Composition
Functional Decline
Comorbidity
Recurrence Growing evidence Growing evidence
Possible benefit Probable benefit Convincing benefit

Cancer-Related Diet & Physical Activity
Recommendations
Rock et al. CA Cancer J Clin 2012; WCRF-AICR 2nd Expert Research Report, http://www.aicr.org
WCRF- AICR (2007) American Cancer Society (2012)
Weight Be as lean as possible without
becoming underweight
Achieve & maintain a healthy weight
Physical
Activity (PA)
Regular PA, >30 min/day Avoid inactivity; PA >150/week;
strength training 2 x week
Dietary
Pattern
Avoid sugary drinks. Limit
energy-dense foods (foods high
in sugar & fat, and low in fiber)
Eat more of a variety of
vegetables, fruits, whole grains
and legumes
Limit consumption of
processed & red meat
Diet High F&V & Whole Grains
• Choose foods & beverages in
amounts that achieve & maintain a
healthy weight
• Eat > 2.5 cups fruits & vegetables/day
• Whole vs. refined grains
• Limit consumption of processed & red
meat
Other Limit salty foods -
Alcohol If drink limit to 1-2 drinks/day If drink limit to 1-2 drinks/day
Supplements Do not use supplements to
protect against cancer

Weight Management & Energy
Balance
Anorexia/Cachexia
• Patients with select respiratory,
G.I. & childhood cancers
• Patients living with advanced
cancer
• Increasing weight to desired
range important for recovery,
well-being, functional status
• Diet & exercise key roles +/-
pharmacotherapy
Overweight/Obesity
• Risk factors for several
cancers, as well as cancer-
related mortality
• Increased weight at diagnosis
is a poor prognostic factor
• Weight gain common during &
after treatment–linked with co-
morbidity, functional decline &
maybe recurrent/progressive
CA

Worldwide rates of obesity and overweight
• Worldwide 35% of adults are overweight and 11% are obese (2008)
doubled since 1980 – prevalence higher in select survivor groups
(breast & prostate)
• 65% of the world's population live in countries where overweight and
obesity kills more people than underweight.
• Medical costs for obese people are $1,429 (USD) higher than those
of normal weight

Increases in Cancer Risk with Overweight & Obesity
0
20
40
60
80
100
120
140
160
Overweight Obesity
WHO: IARC 2002/WCRF –AICR 2007
Breast (post-menopause)
Colon Endometrium Kidney Pancreas Esophagus
Probable Evidence that Cancer of the Ovary & Gallbladder are Weight-Related

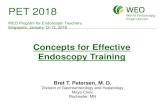
0 7 6 5 4 3 2 1 8
Prostate (> 35)
Multiple Myeloma (> 35)
Gallbladder (> 30)
Colon and rectum (> 35)
Esophagus (> 30)
Stomach (> 35)
Pancreas (> 35)
Liver (> 35)
NHL (> 35)
All cancers (> 40)
Kidney (> 35)
1.34
1.49
1.52
1.70
1.71
1.76
1.84
1.91
1.94
2.61 4.52
0 7 6 5 4 3 2 1 8 9 11 10
Multiple myeloma (> 35)
Colon and rectum (> 35)
Breast (> 40)
Gallbladder (> 30)
Esophagus (> 30) Pancreas (> 40)
Cervical (> 35) Kidney (> 40) Uterus (> 40)
Liver (> 35) All cancers (> 40)
NHL (> 35)
Ovarian (> 35)
1.44
1.46
1.51
1.68
1.88
1.95 2.12
2.13
2.64
2.76
3.20
4.75 6.25
Relative Risk of Death (95% confidence interval)
Obesity and Cancer-related Mortality
Females
Males
Calle EE et al. NEJM.348:1625, 2003.

Prognostic Effects of Weight Gain Among Individuals
with Breast and Prostate Cancer:
Results of 2 Meta-Analyses
Group
(year)
# of
studies
Sample RR (95% CI) for every 5 kg/m2
increase in BMI from pre- to
post-dx
Chan et
al. (2014)
82 213,075 women
with breast cancer
Breast CA Specific Mortality
1.29 (0.97-1.72)
Total Mortality
1.08 (1.01-1.15)
Cao & Ma
(2011)
6 cohort 18,203 men with
prostate cancer
Biochemical Recurrence
1.21 (1.11-1.31)
Prostate CA Specific Mortality
1.20 (0.99-1.46)

Potential Mechanisms Whereby
Obesity Influences Cancer
Obesity Cancer
Adipokines/Growth Factors
Inflammation
Sex Steroids
Insulin
Increased Substrate Levels
(glucose & free fatty acids)
Diabetes other Comorbidities
Binding Proteins/Receptors
Metformin, Statins and Other
Pharmacologic Agents Adapted from Irwin et al.

Weight Loss Interventions
• 1st trial de Waard 102 post-menopausal breast cancer survivors Europ J Cancer Prev 2:233, 1993
• 14 weight loss trials in breast cancer (2-18 months). No adverse events. 57% resulted in >5% loss of body weight. Clinically significant benefits in HbA1C, insulin, inflammatory markers, QoL, lipids, physical functioning and B/P with 5-9% weight loss.
• In field or in analysis SUCCESS-C pre/post breast cancer (n=1,400-1,600) 2-yrs, telephone counseling + mailed materials vs. mailed materials
LISA 336 post menopausal, telephone counseling + mailed materials vs. mailed materials
DIANA-5 pre/post breast cancer (n=1,417) 5-yrs, clinic-based vs. mailed materials
Choice 259 post menopausal – low CHO vs. low fat vs. control
ENERGY pre/post menopausal (N=692), Clinic based+ telephone counseling + mailed materials vs. standard care
Reeves M et al. Obesity Rev doi 10.1111/obr/12190 2014

Interest in Obesity & Cancer Increasing
IOM Workshop on Cancer Survival and Recurrence Oct 2011
2014 Nov 1;32(31):3568-74

2012 American Cancer Society (ACS)
Nutrition & Physical Activity Guidelines for Cancer Survivors
Achieve and maintain a healthy weight
If overweight or obese, limit high calorie foods & beverages increase physical
activity to promote weight loss
Engage in regular physical activity
• Avoid inactivity; resume normal activities as soon as possible following dx
• Exercise >150 minutes/week
• Include strength training exercises at least 2 days/week
Achieve a dietary pattern that is high in vegetables, fruits and whole grains
• Follow ACS Guidelines on Nutrition & Physical Activity for Cancer Prevention
- Choose foods & beverages in amounts that achieve/maintain a healthy weight
- Limit processed and red meat
- Eat > 2.5 cups of vegetables & fruits/day
- Choose whole grains instead of refined grain products
- If you drink ETOH, drink <1 drink/day for ♀ & 2 drinks/day for ♂
Supplements
• Try to obtain nutrients through diet, first.
• Consider only if a nutrient deficiency is biochemically or clinically observed, or if
intakes fall persistently below recommended levels as assessed by an RD.
CA CANCER J CLIN (2012) DOI.10.3322/CAAC.21142 www.cacancerjounral.com

Cochrane Review: Exercise on Quality of Life Post-treatment
40 trials with 3694 participants Mishra et al. Cochrane Database Rev 2012
Outcome # studies/N Evidence Qual Positive effects
Overall QOL, <12 weeks 11/826 Low 0.48 (0.16-0.81)
Overall QOL, 6 mo 2/115 Moderate 0.46 (0.09-0.84)
Anxiety, <12 weeks 4/455 Low -0.26 (-0.4 to -0.07)
Emotional well being 8/632 Low 0.33 (0.05 to 0.61)
Fatigue, <12 weeks 10/745 Moderate -0.82 (-1.50 to -0.14)
Fatigue, 12 wks-6 mo 3/246 Low -0.42 (-0.83 to -0.02)
Pain, <12 weeks 4/289 Moderate -0.29 (-0.55 to -0.04)
Sexuality, 6 mo 2/193 Moderate 0.40 (-0.72 to -0.20)
Sleep disturbance, <12 weeks 8/438 Moderate -0.46 (-0.72 to -0.20)
Social functioning, <12 weeks 5/386 Very low 0.45 (0.02 to 0.87)
Social functioning, 6 months 2/110 Moderate 0.49 (0.11 to 0.87)

Forest plot of the relations of change in physical activity (PA) from
pre- to post-diagnosis to total mortality and cancer mortality.
Schmid D , and Leitzmann M F Ann Oncol 2014;25:1293-1311
© The Author 2014. Published by Oxford University Press on behalf of the European Society for
Medical Oncology. All rights reserved. For permissions, please email:

2012 American Cancer Society (ACS)
Nutrition & Physical Activity Guidelines for Cancer Survivors
Achieve and maintain a healthy weight
If overweight or obese, limit high calorie foods & beverages increase physical
activity to promote weight loss
Engage in regular physical activity
• Avoid inactivity; resume normal activities as soon as possible following dx
• Exercise >150 minutes/week
• Include strength training exercises at least 2 days/week
Achieve a dietary pattern that is high in vegetables, fruits and whole grains
• Follow ACS Guidelines on Nutrition & Physical Activity for Cancer Prevention
- Choose foods & beverages in amounts that achieve/maintain a healthy weight
- Limit processed and red meat
- Eat > 2.5 cups of vegetables & fruits/day
- Choose whole grains instead of refined grain products
- If you drink ETOH, drink <1 drink/day for ♀ & 2 drinks/day for ♂
Supplements
• Try to obtain nutrients through diet, first.
• Consider only if a nutrient deficiency is biochemically or clinically observed, or if
intakes fall persistently below recommended levels as assessed by an RD.
CA CANCER J CLIN (2012) DOI.10.3322/CAAC.21142 www.cacancerjounral.com

Red Meat Consumption & Cancer–Related
Mortality • Pooled analysis of 37,698 men from the Health Professionals
Follow-up Study and 83,644 women from the Nurses' Health Study
• 9464 cancer deaths during 2.96 million person-years of follow-up.
Q1
(ref)
Q2 Q3 Q4 Q5 P Trend HR (95% CI) for 1
svg day-1 increase
Total Red
Meat
1 1.05
0.98-1.12
1.09
1.02-1.16
1.16
1.08-1.24
1.19
1.11-1.28
<.001 1.10 (1.07-1.13)
Not
Processed
1 1.03
0.97-1.10
1.03
0.96-1.10
1.09
1.02-1.16
1.17
1.10-1.26
<.001 1.10 (1.06-1.14)
Processed 1 1.03
0.97-1.10
1.08
1.01-1.15
1.08
1.01-1.15
1.14
1.07-1.22
<.001 1.16 (1.09-1.23)
• Substitution estimates of 1 serving/day of other foods (e.g., fish, poultry, nuts,
legumes, low-fat dairy, and whole grains) for 1 serving/day of red meat were
associated with a 7% to 19% lower mortality risk. Estimates suggest that
9.3% of deaths in men and 7.6% in women could have been prevented at
follow-up if there was a reduction in 0.5 servings/day (~42 g/day) of red meat.
Pan A et al. Arch Intern Med March 12, 2012

Dietary Patterns
Prudent vs. Western
Team (year) Sample Diet CA Mortality
HR (95% CI)
Other Cause
Mortality
HR (95% CI)
Kroenke (2005) 2619 Breast
CA
Prudent 1.07 (0.66-1.73) 0.54 (0.31-0.95)
Western 1.01 (0.60-1.70) 2.31 (1.23-4.32)
Kwan (2009) 1901 Breast
CA
Prudent 0.79 (0.43-1.43) 0.35 (0.17-0.73)
Western 1.20 (0.62-2.32) 2.15 (0.97-4.77)
Vrieling (2013) 2522 Post-
menopausal
Breast
Prudent 0.89 (0.59-1.35) 0.81 (0.40-1.61)
Western 3.69 (1.66-8.17) 0.99 (0.64-1.52)
Meyerhardt
(2007)
1009 Stage
III CRC
Prudent
1.13 (0.77-1.67)
1.32 (0.86-2.04)
Western 2.85 (1.75-4.63) 2.32 (1.36-3.96)
Diet Quality: 3-of-4 studies show significant protective effect for overall mortality,
one shows significant protection for cancer specific mortality (George 2011 & 2014;
Izano 2013; Kim 2011)

Women’s Healthy Eating & Living
(WHEL) Study
Pierce JP et al. JAMA 298: 289, 2007
• Sample: 3088 early stage breast cancer survivors dx’d within 4 yrs
• Intervention: 5 vegetable servings plus 16 oz of vegetable juice; 3 fruit servings; 30 g of fiber; and 15% to 20% of energy intake from fat
• Follow-up: Up to 10 years
• Comments: No weight loss, baseline F&V ~ 7.4 servings/day
Intervention Control
Total Breast Cancer Events 256 262
Total Breast Cancer Deaths 127 135
Total Deaths 155 160
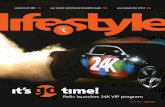
Pierce JP et al. JAMA 298: 289, 2007

0
5
10
15
20
25
All Patients ER positive ER negative
Low Fat Diet
Regular Diet
Results of the Women’s Intervention Nutrition Study (WINS) Show Reduced Rates of Recurrence in Patients Assigned to a Low Fat Diet (n=2,437)
Chlebowski et al. JNCI 98:1767, 2006
P =.034 P =.277
P =.018
Recu
rren
ce R
ate
s (
% o
f p
op
ula
tio
n)

Alcohol
• Direct association with cancers of the kidney, head and neck and primary risk of breast cancer (“no amount of alcohol is safe”
• If you are a survivor of head and neck cancer you should not drink alcohol since it will increase your chance complication and reduce survival
• If you are a survivor of other cancers the choice is less clear – it may increase your risk of recurrence (breast cancer) but also decrease your risk of death due to cardiovascular disease

Associations Between Alcohol-Use and
Second Primaries (Select Studies) Team (yr) Primary
CA
Sample Median
F/U
Results
HR (95%CI)
Lin et al.
(2005)
HNSCC 123 SPT in 1257
Cases
73M Daily Drinkers at dx
2.1 (1.4-3.3)
Trentham-
Dietz et al.
(2008)
Breast
CA 10,953 BCA cases
488 Breast SPT
132 CRC SPT
113 Endometrial SPT
36 Ovarian SPT
84M >7 drinks/wk 1-yr post-dx
1.09 (0.78-1.53)
1.92 (1.03-3.43)
0.84 (0.42-1.69)
0.55 (0.18-1.72)
Knight et al.
(2009)
Breast
CA
708 Asynchronous
contralateral BC vs.
1399 unilateral Ctrls
60M
(mean)
Ever Reg Drank 1.3 (1.0-1.6)
Post-dx Drinker 1.2 (0.9-1.5)
Do et al.
(2003)
HNSCC 201 SPT in 1181 pts in
13 cis RA RCT
12M Continued Drinking
1.3 (1.0-1.7)
Leon et al.
(2009)
HNSCC 257 MSPT vs. 257
matched Ctrls
48M vs
126M
Continued Drinking
5.2 (3.3-7.9)
Li et al.
(2009)
ER+
Breast
CA
365 Asynchronous
contralateral BC vs.
726 unilateral Ctrls
101M Current Drinker
1.9 (1.1-3.2)

2012 American Cancer Society (ACS)
Nutrition & Physical Activity Guidelines for Cancer Survivors
Achieve and maintain a healthy weight
If overweight or obese, limit high calorie foods & beverages increase physical
activity to promote weight loss
Engage in regular physical activity
• Avoid inactivity; resume normal activities as soon as possible following dx
• Exercise >150 minutes/week
• Include strength training exercises at least 2 days/week
Achieve a dietary pattern that is high in vegetables, fruits and whole grains
• Follow ACS Guidelines on Nutrition & Physical Activity for Cancer Prevention
- Choose foods & beverages in amounts that achieve/maintain a healthy weight
- Limit processed and red meat
- Eat > 2.5 cups of vegetables & fruits/day
- Choose whole grains instead of refined grain products
- If you drink ETOH, drink <1 drink/day for ♀ & 2 drinks/day for ♂
Supplements
• Try to obtain nutrients through diet, first.
• Consider only if a nutrient deficiency is biochemically or clinically observed, or if
intakes fall persistently below recommended levels as assessed by an RD.
CA CANCER J CLIN (2012) DOI.10.3322/CAAC.21142 www.cacancerjounral.com

Dietary Supplements & Cancer
• Several cell culture & animal studies showing a benefit of various single nutrients and foods
• ATBC & CARET trials shows show increased risk of lung cancer in b-carotene arms
• SELECT trial shows higher risk of prostate cancer with vitamin E and higher risk of diabetes with selenium.
• Several meta-analyses show significantly higher mortality with vitamin E & b-carotene
• Results of NIH-AARP (n=295,344) show increased risk of fatal prostate cancer among men taking >7 multi-vitamins/week (RR: 1.98; 95% CI:1.07-3.66) Lawson et al. (2007)

Mayne S T et al. Cancer Res 61:1457-63, 2001
RCT of b-Carotene (50 mg/d) vs. Placebo (51M median follow-up)
254 Cases w/ Stage I/II Head & Neck Squamous Cell Cancer
SPT or local recurrence, P = 0.59
HR = 0.69 (95%CI 0.39-1.35) SPT Head & Neck
HR = 1.44 (95%CI 0.62-3.39) SPT Lung

Bairati et al. JNCI ;97:481-8, 2005
Cancer-free survival (no recurrence & no SPT among participants randomly assigned to the
supplement arm (solid line) or to the placebo arm (dotted line)
Second Primary HR 2.88 (95%CI 1.56-5.31)
RCT of a- Tocopherol + b-Carotene vs. Placebo (52M median follow-up)
540 Cases w/ Stage I/II Head & Neck Squamous Cell Cancer

Bottom Line on Supplements
Rely on Food as a Source of Nutrients But , if considering supplements
-Have dietitian analyze diet for deficiency
- Check blood levels of nutrients
- Consider lowest dosage & most complex preparation
- If currently on supplements wean off slowly.
Calcium V.S.
Miracle
in a
Bottle

Synergy between Lifestyle Practices?
• Early stage breast cancer survivors in Multi-ethnic Cohort (n=670) Compared with inactive survivors consuming poor-quality diets, survivors engaging in any physical activity and consuming better-quality diets had an 89% reduced risk of death from any cause HR: 0.11 (0.04-0.36) and a 91% reduced risk of death from breast cancer HR: 0.09 (0.01- 0.89). (George et al. 2011)
• In 1490 early stage breast cancer survivors a combination of 5+ daily servings of F&V + accumulating 540+ MET-min/w associated with a doubling of survival HR: 0.56 (0.31 - 0.98) (Pierce et al. 2007)
• In 2193 post-menopausal breast cancer survivors from Iowa Woman’s Health Study those who were most adherent vs. least adherent (6-8 vs. 0-4) to AICR/WCRF guidelines had a 33% lower mortality rate (Inoue-Choi et al. 2013)

Rates of Overweight & Obesity among Cancer
Survivors:
Results of Two National Surveys
Overweight Obese Total
U.S. Survivors 37.0% 21.9% 58.9%
Canadian
Survivors
34.4% 18.4% 52.8%
Bellizzi et al. JCO 2005; Courneya et al. CANCER 2008

Blanchard et al, JCO 2008.
Many cancer survivors do not adhere to recommendations
(ACS Cancer Survivors II Study, n=9,105)

More Research is Needed
• Optimal timing
• Specific content, sequencing
and dose
• Impact on array of outcomes
• Mechanisms of action
• Factors that moderate effect
(cancer-type, tumor
characteristics, treatment, age,
co-morbidity, gender, etc.)
• Optimal delivery channel
(dissemination)
• Cost-effectiveness

Resources
• American Cancer Society: www.cancer.org
• Academy of Nutrition and Dietetics: www.eatright.org
• American Institute for Cancer Research: www.aicr.org
• Centers for Disease Control: www.cdc.gov/HealthyLiving
• National Center for Complementary & Alternative Medicine: http://nccam.nih.gov

http://aspo.org
March 15-17th
Birmingham, AL
Interactive Poster Sessions on Obesity and E-cigarettes
Preconference Workshop: Underserved Cancer Survivors