OPQC Learning Session: High Risk Moms & Infants Applegate, MD, FACP, FAAP Medical Director, Ohio...
28
Mary Applegate, MD, FACP, FAAP Medical Director, Ohio Department of Medicaid September 2016 OPQC Learning Session: High Risk Moms & Infants
-
Upload
truongdiep -
Category
Documents
-
view
215 -
download
1
Transcript of OPQC Learning Session: High Risk Moms & Infants Applegate, MD, FACP, FAAP Medical Director, Ohio...

Mary Applegate, MD, FACP, FAAP Medical Director, Ohio Department of Medicaid September 2016
OPQC Learning Session: High Risk Moms & Infants

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
9/19/2016 2
OLD:

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
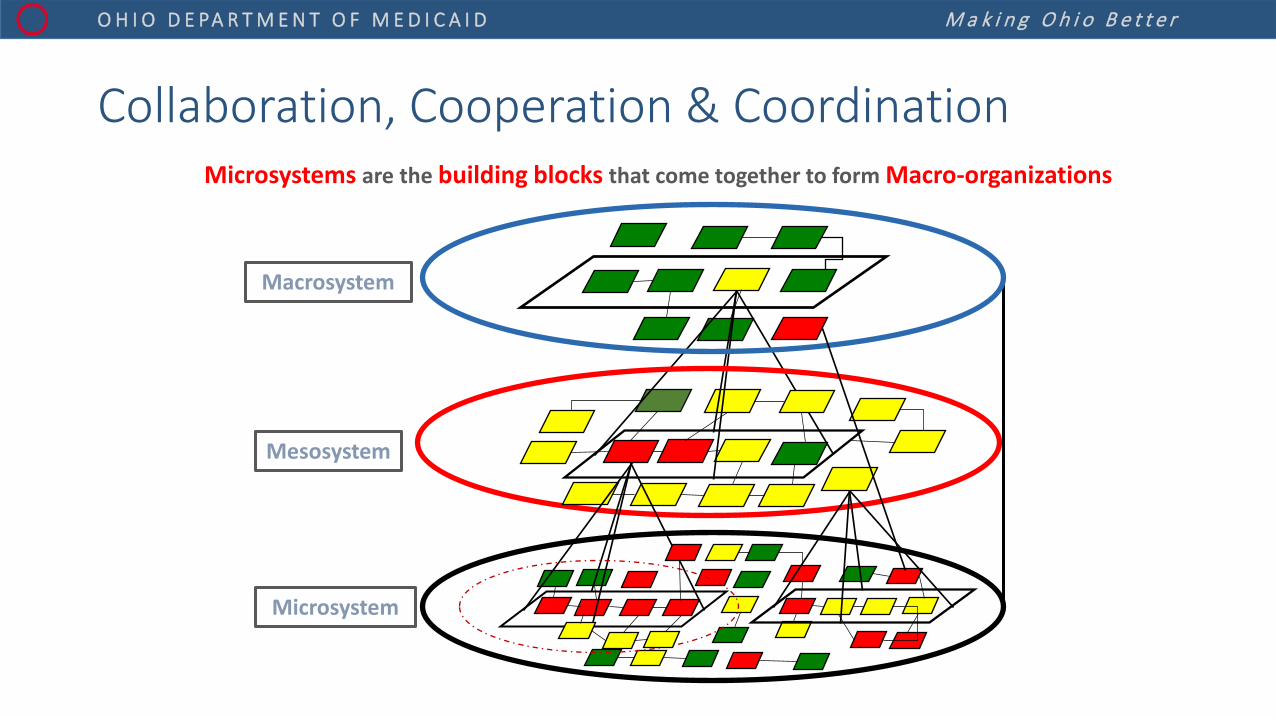
Microsystems are the building blocks that come together to form Macro-organizations
Mesosystem
Microsystem
Macrosystem
Collaboration, Cooperation & Coordination

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D It takes a village…
•

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
High Risk Population Efforts: Observations • NICU infants
» BSI, hospital processes • Mothers at Risk for Preterm Birth
» EED, hospital processes » Progesterone – hospital & * outside hospital processes
• Addicted Infants » NAS hospital processes
• Addicted mothers » *pre-hospital processes
• Technology dependent infants » hospital processes, *post-hospital processes
9/19/2016 6
M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
How DO We Get Off the Ground Floor?
• Step back for broader perspective • Set audacious goals (Cut preterm births by 50%, End racial disparities) • Think about high level pieces of work (Key Driver) & partners • Then drill down • Patiently
• Result? A different solution & direction collectively
• Examples…
9/19/2016 7

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D 8
Ohio Minds Matter: Safer Prescribing of Antipsychotic Medications for Ohio’s Youth
Foster Care Mandate
Conduct Research & Build Collaborative Partnerships
Conduct Initial Pilot
Establish Best Clinical Practice with Shared Decision Making
Lessons Learned Guide Systems Reform
2011
2012
2016
2012
2013-14
2013
Launch Collaborative Pilots & Family/Patient Empowerment Effort
Measures: • Antipsychotic (AAP) medications in children less than 6 years of age • 2 or more concomitant AAP medications for over 2 months duration. • 4 or more psychotropic medications in youth <18 years of age.
Sustainability through HEDIS measures in MCP contracts
Burning platform
Demonstration
Evaluation

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Learning from Systems Observations 9
Behavioral Health Systems Re-Design

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Date Milestones in Progesterone Performance Improvement Effort July 2013 • MCPs coverage expanded to statewide
• Presumptive eligibility for Pregnant women • Enhanced Maternal Care Requirements integrated into Managed Care Plan Provider Agreement
October 2013 • Go Live--Ohio Benefits self-service portal January 2014 • Medicaid Expansion–women under 138% of FPL newly eligible under ACA
May 2014 • Vital Statistics linked to Medicaid Claims to Identify High Risk Women based on previous preterm birth October 2014 • CMS approval of redesigned federally mandated performance improvement project
Dec 2014—June 2015
• Managed Care Plans trained on QI process and appropriate use of Progesterone for High Risk Women
Spring 2015
• Progesterone performance improvement project (Medicaid MCPs and OPQC affiliated sites) begins • Community-based infant mortality budget initiatives in to address health equity issues
July-September 2015 • Minimize Medicaid and MCP disenrollment due to annual redetermination
• Clinicians communicating pregnancy status (“skinny form”) • MCPs assigning care managers • Care Manager responsible for notifying county of pregnancy to ensure ongoing eligibility
November 2015 • All 23 OPQC sites use the skinny communication form identifying progesterone candidates
Feb 2016 • Removal of PA on all forms of Progesterone and associated Home Health Visits

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
OPQC Progesterone Project 2014 - 2016 Reductions in % of Births < 32 Weeks to Mothers on Medicaid with History of Previous PTB 21% decrease in Participating Hospitals
ODH Birth Registry Monthly Data January 2012 – February 2016
21%
IMPACT: This equates to 33 fewer babies < 32 weeks born to mothers in the Medicaid program, 26 of whom were African-American
*

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Death Rates Per 100,000 for Drug Poisoning (All Manner), by Year, Ohio vs. US, 2000-2015
12
0
5
10
15
20
25
30
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Rate
per
100
,000
per
sons
US Rate
Ohio Rate
Source: ODH Office of Vital Statistics

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Crack Cocaine
Prescription drugs led to a larger overdose epidemic than illicit drugs ever have.
Heroin
Heroin & Rx opioids
Drug Overdose Epidemics in Ohio, 1979 - 2015
0
500
1000
1500
2000
2500
3000
3500
JCAHO establishes pain standards & modified

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Unintentional Drug Overdose Deaths of Ohio Residents by Specific Drug(s) Involved, 2000-15*
14 Source: ODH Bureau of Vital Statistics; Analysis Conducted by ODH Injury Prevention Program
-
200
400
600
800
1,000
1,200
1,400
1,600
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
NU
MBE
R O
F DE
ATHS
cocainebenzodiazepinesheroinPrescription Opioids*Fentanyl (illicit and prescription)
• Prescription Opioids not including Fentanyl; Fentanyl was not captured in the data prior to 2007 as denoted by the dashed line

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
15
EpiAid Data Results: OARRS Data
• Majority of heroin and fentanyl decedents not prescribed opioids at the time of death (~75%)
• However, over 60% of fentanyl and heroin decedents had a history of opioid prescription at some point in the 6-7 years preceding their death. Of those:
» 50% were prescribed a max opioid dose of >= 50 MME » 35% were prescribed a max opioid dose of >= 90 MME

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Medicaid Trends in Opioid Use: Gender & Age Groups
9/19/2016 16
Proportion of all eligible Medicaid beneficiaries ages 12-24 with an opioid claim, by gender and age.
Source: Medicaid Claims and encounter data for calendar years 2007-2014, including all Medicaid claims paid through January 2016.
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
2007 2008 2009 2010 2011 2012 2013 201412-17 Female 12-17 Male All 18-24 Female 18-24 Male

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Timeline: Opioid Prescribing Policy and Initiatives 2011 2012 2013 2014 2015 2016
Law Enforcement
• Closure of “pill mill” pain clinics
• Regulatory tightening
• $3M invested in BH programs through local jails
• Enhanced training on heroin epidemic
• Addiction Treatment PP
• Enhanced training on overdose investigations
Prevention Services
• “Don’t Get Me Started” - an opioid abuse campaign
• “Start Talking!” youth drug prevention program, Drug court, housing investments
• OARRS integration into EHR
Guiding Appropriate Prescribing
• Release of low-dose protocols: buprenorphine & Suboxone
• Opioid guidelines for emergency/acute care settings
• Drop Box Program
• Opioid guidelines for chronic, non-terminal pain
• Health Resource Toolkit for providers
• Mandatory Prescription Drug Monitoring Program
• Opioid guidelines for management of acute pain
• CDC guidelines
Expanding Access to Treatment and Recovery
• Expanded use of MAT • (Medication Assisted
Treatment) • SOLACE
• Project “DAWN” • NAS treatment
protocol development
• Legislation: first responders may administer naloxone
• SBIRT implementation grant
• MOMS Program develops best practices for opioid-dependent mothers & newborns (NAS)
• Legislation to allow pharmacists to dispense Naloxone without an Rx
• More than 800 Ohio pharmacies offer naloxone without an Rx
Medicaid Initiatives
• Coverage of MAT services
• Expansion of Medicaid coverage
• Development and monitoring of measures for opioid guidelines
• Behavioral Health Redesign
• Data transparency • ?Build into value-
based purchasing?

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Proposed Metrics for Ohio Guidelines for the Management of Acute Pain Outside of Emergency Rooms**
Quarter
Total Dispensed to Ohio Patients Acute Pain All Ohio Patients Acute Pain Acute Pain Acute Pain
Total Opioid Doses per Quarter Total Patients w/ One Opiate Rx Average Units* per Rx
Median Units* per Rx
Average MED per Rx # of New Rx # of Refills
Authorized
2013-1 192,209,367 65,005,666 1,269,245 554,867 35.68 30 46.48 1,608,433 501,293 2013-2 195,878,652 69,557,428 1,290,987 575,145 36.22 30 46.15 1,699,224 554,742 2013-3 195,569,758 67,259,765 1,289,107 568,288 35.11 30 46.98 1,689,019 606,384 2013-4 194,404,281 68,923,642 1,279,984 564,525 35.25 30 46.51 1,692,429 602,200 2014-1 186,140,901 63,994,883 1,239,947 540,952 34.82 30 47.02 1,607,058 564,829 2014-2 191,155,531 70,795,398 1,283,677 576,941 34.38 30 48.95 1,817,106 653,881 2014-3 189,982,798 66,283,613 1,284,549 564,559 34.09 30 47.14 1,746,819 363,731 2014-4 183,351,431 61,462,971 1,255,522 551,867 34.79 30 48.72 1,628,833 179,922 2015-1 174,295,997 59,578,844 1,198,446 539,805 34.77 30 47.83 1,577,654 153,962 2015-2 177,555,743 67,003,562 1,223,520 566,705 36.74 30 47.49 1,674,530 165,072 2015-3 173,965,312 58,447,099 1,202,883 549,798 33.29 24 48.73 1,613,056 137,911 2015-4 175,410,470 67,227,653 1,215,623 569,296 37.51 30 50.19 1,628,181 164,375 2016-1 173,574,887 54,142,565 1,181,968 522,345 33.39 24 50.69 1,497,536 114,816
*Units - Solid dosage units only (eg. tablets, capsules, patches). Liquids and powders are not included.
**For the purposes of these metrics, a prescription is considered to be for the management of acute pain if the patient not been dispensed an opioid prescription in the 90 days prior to the beginning of the given quarter

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
0
50
100
150
200
250
300
350
400
450
500
Back Ortho Abdominal Migraine Dental UTI
Female Male
Number of Pain Episodes per 1,000 Beneficiaries [Ages 12-24]
19
Source: Medicaid Claims and encounter data for calendar year 2013, including all Medicaid claims paid through June 2014.

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Trends in Dependency and Poisoning [Ages 12-24 and 12-64]
N2013 = 42,140 [12-64]
N2013 = 3,155 [12-64]
N2014 = 10,737 [12-24]
N2014 = 1,425 [12-24]
Proportion of beneficiaries ages 12-24 and 12-64 who received a diagnosis of opiate dependency, abuse, or poisoning and had an opiate claim within the same year.
*Excludes poisoning by heroin 965.01
20
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
1.6%
2007 2008 2009 2010 2011 2012 2013 2014
Ages 12-24 - Opioid dependence and abuse
Ages 12-24 - Poisoning by opiates & related narcotics*
Source: Medicaid Claims and encounter data for calendar years 2007-2014, including all Medicaid claims paid through January 2016.
System capacity crisis
14 19 21 25
33
50
70
88
108
122
0
20
40
60
80
100
120
140
Rate
per
10,
000
Year
NAS inpatient hospitalization rate per 10,000 live births
Ohio, 2004-2013
Source: Ohio H

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
How Can we Think About NAS and MOMS Differently with Sustainability in Mind? • ? A patient centered medical home for maternity population? • ? Episodes of Care for Medication Assisted treatment? • How might the Re-Design of the behavioral health system impact the care
and outcomes of these families?
• Do we have the data, content, evidence, partners, sequencing, scope intensity of ideal practice sufficiently delineated for an effective bundle?
9/19/2016 21
M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
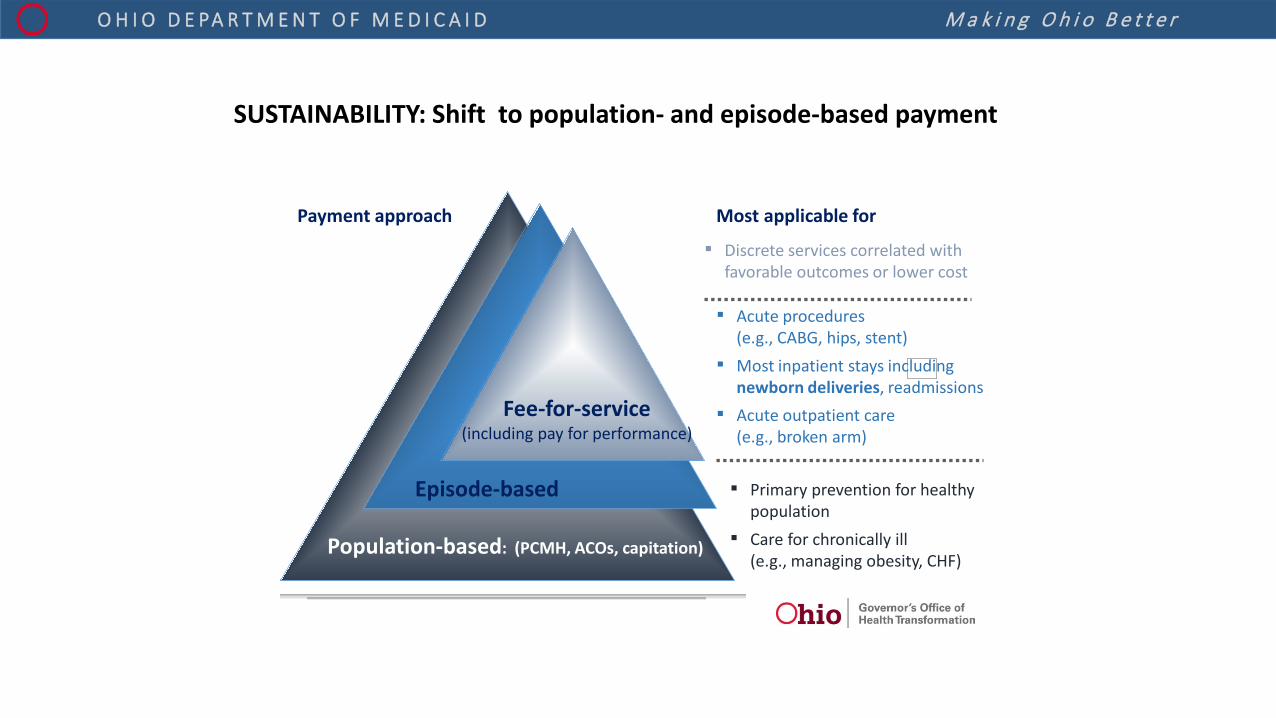
SUSTAINABILITY: Shift to population- and episode-based payment
Payment approach Most applicable for
▪ Primary prevention for healthy population
▪ Care for chronically ill (e.g., managing obesity, CHF)
▪ Acute procedures (e.g., CABG, hips, stent)
▪ Most inpatient stays including newborn deliveries, readmissions
▪ Acute outpatient care (e.g., broken arm)
▪ Discrete services correlated with favorable outcomes or lower cost
Population-based: (PCMH, ACOs, capitation)
Episode-based
Fee-for-service (including pay for performance)

Value-Based Alternatives to Fee-for Service
Fee for Service Pay for Performance
Patient-Centered Medical Home
Episode-Based
Payment
Accountable Care
Organization
Fee for Service Incentive-Based Payment Transfer Risk
Ohio’s State Innovation Model (SIM) focuses on (1) increasing access to comprehensive primary care and (2) implementing episode-based payments
Payment for services rendered
Payment based on improvements in cost or outcomes
Payment encourages primary care practices to organize and deliver care that broaden access while improving care coordination, leading to better outcomes and a lower total cost of care
Payment based on performance in outcomes or cost for all of the services needed by a patient, across multiple providers, for a specific treatment condition
Payment goes to a local provider entity responsible for all of the health care and related expenditures for a defined population of patients
v

High performing primary care practices engage in these activities to keep patients well and hold down the total cost of care

Ohio CPC Clinical Quality Requirements
Detailed requirement definitions will be posted on the Ohio Medicaid website
Must pass 50%
Note: All CMS metrics in relevant topic areas were included in list except for those for which data availability poses a challenge (e.g., certain metrics requiring EHR may be incorporated in future years)
Pediatric Health (4)
Category Measure Name
Behavioral Health (4)
Women’s Health (5)
Adult Health (7)
0576 Mental Health Both Follow up after hospitalization for mental illness
NQF # Population health priority Population
Breast Cancer Screening 2372 Cancer Adults
Well-Child Visits in the First 15 Months of Life 1392 Pediatrics
Well-Child visits in the 3rd, 4th, 5th, 6th years of life 1516 Pediatrics
Adolescent Well-Care Visit HEDIS AWC
Pediatrics
Weight assessment and counseling for nutrition and physical activity for children/adolescents: BMI assessment for children/adolescents
0024 Obesity, physical activity, nutrition
Pediatrics
Postpartum care 1517 Infant Mortality Adults
Preventive care and screening: tobacco use: screening and cessation intervention
0028 Substance Abuse Both
0105 Mental Health Adults Antidepressant medication management
Initiation and engagement of alcohol and other drug dependence treatment
0004 Substance Abuse Adults
Med management for people with asthma 1799 Both 0018 Heart Disease Adults Controlling high blood pressure (starting in year 3)
Comprehensive Diabetes Care: HgA1c poor control (>9.0%)
0059 Diabetes Adults
Statin Therapy for patients with cardiovascular disease HEDIS SPC
Heart Disease Adults
Comprehensive diabetes care: HbA1c testing 0057 Diabetes Adults
HEDIS ABA
Obestiy Adults Adult BMI
Comprehensive diabetes care: eye exam 0055 Diabetes Adults
Live Births Weighing Less than 2,500 grams N/A Infant Mortality Adults
Timeliness of prenatal care 1517 Infant Mortality Adults
Cervical cancer screening 0032 Cancer Adults
▪ Measures will be refined based on learnings from initial roll-out
▪ Hybrid measures that require electronic health record (EHR) may be added to the list of core measures
▪ Hybrid measures may replace some of the core measures
▪ Reduction in variability in performance between different socioeconomic demographics may be included as a CPC requirement
Measures will evolve over time
M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
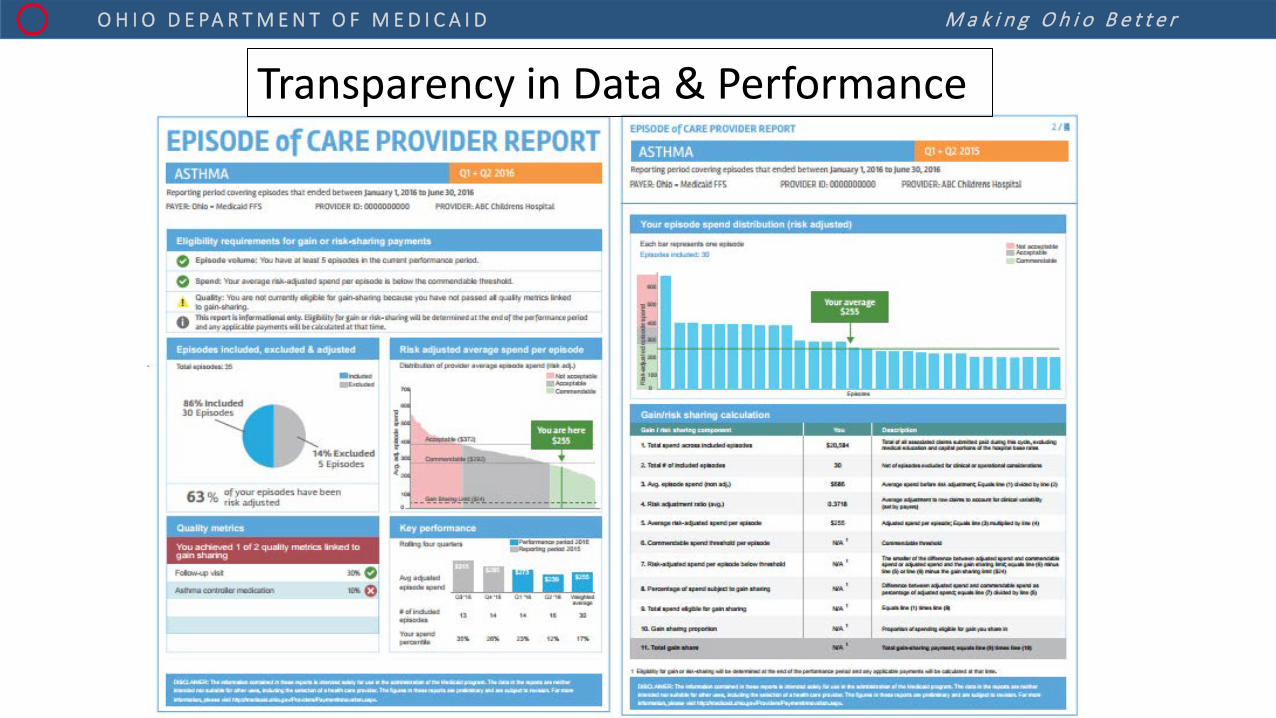
Transparency in Data & Performance

M a k i n g O h i o B e t t e r O H I O D E PA R T M E N T O F M E D I C A I D
Next Steps: Together
• Thank you
• Think • Plan • Collaborate • Act • Share (data, insights)
• Repeat
9/19/2016 27