
Opportunities in practice
120
Opportunities in practice Outcome measurement in mental health
Transcript of Opportunities in practice

Opportunities in practice Outcome measurement in mental health

4 Clinical review of area mental health services 1997-2004

Opportunities in practice Outcome measurement in mental health
1

Published by the Mental Health and Drugs Division, Victorian Government, Department of Human Services, Melbourne, Victoria
Authorised by the State Government of Victoria, 50 Lonsdale Street, Melbourne. REVISED March 2009 [Original August 2008]
(080708)
© Copyright, State of Victoria, Department of Human Services, 2008 © Copyright, Commonwealth of Australia 2008
This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without prior written permission from the Commonwealth or Victorian Governments. Requests and inquiries concerning reproduction and rights should be addressed to Mental Health and Drugs Division, Victorian Government.
For electronic copies (including future revisions) visit: www.health.vic.gov.au/mentalhealth/outcomes
Disclaimer
Opinions expressed in this publication are those of the authors and do not necessarily represent any official Government position or view. The authors hold final editorial responsibility for the document and any errors that remain herein.
1. G
etti
ng s
tart
ed2

1.1
Fore
wor
dThe routine measurement of consumer outcomes has been a priority of the National Mental Health Strategy since it was first adopted by Australian Health Ministers in 1992 and is articulated in all subsequent National Mental Health Plans. The measurement of consumer outcomes is also compatible with each jurisdiction’s emphasis on high quality health services and increased consumer and carer participation as articulated in relevant policy documents. Work undertaken during the period of the Second National Mental Health Plan (1998-2003) targeted the development of information infrastructure and workforce skills to support the use of outcome measurement and other quality improvement activities. All states and territories prepared comprehensive Information Development Plans (IDP) to guide their implementation activities.
The National Outcomes and Casemix Collection (NOCC) involves clinicians and consumers measuring changes over time in the health status of a consumer and include both clinician and consumer rated measures. It was introduced across all clinical public mental health services in Australia in 2003-2004 and is reported as a Key Performance Indicator, based on the National Health Performance Framework and linked to the strategic directions of the National Mental Health Plan 2003-2008.
Recognising the complexity of the work required and its national significance, the Australian Government contributed Commonwealth Own Purpose Outlays (COPO) funding under the Australian Health Care Agreements to assist jurisdictions in implementing their Information Development Plans (IDP) to support a range of quality and safety initiatives in specialist mental health care. States and territories have also received additional funding (2005-2008) under Quality Through Outcomes (QTO) agreements (Australian Health Care Agreements) to implement and enhance consumer outcomes in routine clinical practice.
The implementation of routine measurement of consumer outcomes was unprecedented and resulted in significant challenges for mental health services to embed the collection and utilisation of consumer outcomes in clinical practice. Consistent with funding and governance processes of mental health services across Australia, and the different models of service delivery, each state and territory has faced unique challenges in this implementation. Despite the differences, many similarities have been identified, including:
• workforce capacity to routinely collect and utilise consumer outcomes
• workforce development including general training in IT, assessment and documentation and in consumer outcome rating and application
• attitudinal challenges in developing mental health services with a focus on mental health information and a culture of enquiry
• data system accessibility and reporting capabilities
• consumer and carer awareness of, and participation in, the consumer outcome agenda.
The development of this resource was undertaken by the Mental Health and Drugs Division of the Department of Human Services, Victoria through QTO funding (Appendix 1) and draws together the collective experience of each jurisdiction on how consumer outcomes can be used in practice. It has been a challenge to use sufficiently generic and inclusive language to ensure that the content is applicable across age groups (child and adolescent, adult and older person), service settings (inpatient, ambulatory and community residential) and jurisdictions (states and territories). This resource has captured current practice opportunities for focussing on consumer outcomes.
Given that the utilisation of consumer outcomes is evolving, this resource will undergo routine review and revision in the future. Refer to: 1.3 Your invitation
3

1.2
Ack
now
ledg
emen
ts4
This project was developed by the Mental Health and Drugs Division, Department of Human Services Victoria with funding from the Commonwealth Department of Health and Ageing. The resource was developed by Angie Hunter, Project Manager, with extensive input from jurisdictional colleagues. Collectively the following individuals have had extensive experience with public mental health services either in clinical practice and/or expertise in consumer outcomes. This collective experience has been invaluable in the development of this resource.
There have been two distinct phases:
- March – July 2008 involved the original content development
- July – November 2008 involved the refinement of the content.
Phase one - Resource content contributorsJurisdiction Name Contribution capacity
Consumer & Carers Rosemary Lawton Consumer & Carer Workshop
Tania Lewis
Beth Bailey Consumer & Carer WorkshopQuality Through Outcomes Statewide Steering Committee
Australian Mental Health Outcomes Classification Network
Tim Coombs Project planning meetings, NOCC Trainers two day meetingConsumer & Carer Workshop
Australian Capital Territory
Paul Mayers NOCC Trainers two day meeting
Briony Holdsworth
New South Wales Neda Dusevic
Northern Territory Rachel Conn
John Trevor Gregory
Lorin James
Queensland Kathy Stapley NOCC Trainers two day meeting, ACIT Meeting in Brisbane
Erika Heslin ACIT Meeting in Brisbane, North Queensland Visit
Carolyn Dixon North Queensland Visit
South Australia Bev Malone NOCC Trainers two day meeting
Graeme Sanders
Sarah Anstey
Tasmania Ray Kemp
Victoria Glenda Pedwell NOCC Trainers two day meeting, QUATRO VIC consultationQuality Through Outcomes Statewide Steering Committee
Lucy Horgan NOCC Trainers two day meeting, QUATRO VIC consultation
Alex Pleban QUATRO VIC consultation
Karen Williams
Katie Weedon
Joyce Goh Quality Through Outcomes Statewide Steering Committee
Caroline Byrne
Penny Herbert
Jon Kroschel
Western Australia Creswell Surrao NOCC Trainers two day meeting

5
Phase two - Resource refinement
Date Contribution capacity
Stakeholder Group
Name Jurisdiction
16.10.08 2 hours Melbourne
Quality Managers Workshop
Quality Managers/Evaluation Service Improvement Co-ordinators
Rosie Cantley-Smith
Victoria
Lindy Bennett
Gayle Nicols
Pam Marland
Bev Schumacher
Hugh Stern
Mary Hyland
Julie Mission
Neil Woodger
Penny Herbert
Elizabeth Rand
Jo Russell
Tung Nguyen
Kirsten Gabel
Alex Pleban
Joyce Goh
Cathi Richardson
17.10.08 3 hours Melbourne
Consumer & Carer Consultants Workshop
Consumer & Carer Consultants - Victoria
Cate Bourke Victoria
Robyn Jones
Rosemary Lawton
Jon Kroschel
Jon Langford
Eila Lyon
David Guthrie
Jenny Burger
Katie Weedon
Stewart Fenton Queensland
Jacqui Wharton Western Australia

Date Contribution capacity
Stakeholder Group
Name Jurisdiction
31.10.08 7 hours Perth
NOCC trainers Workshop
NOCC trainers Roy Dobson Western Australia
Jo-Anne Dwyer
Robert Edey
Sam Gurusamy
Jodi Henderson
Catherine Hollingworth
Carmel Loughney
Joanne Mabbs
Glenn Moorey
Michael Murphy
Zenebrio Nicoletti
De Spackman
Marika Sapseska
Creswell Surrao
Sharon Thomas
Joan Valley
David Ward
Deborah Easther James McCloy
Karen Williams Victoria
Emma Smith
Sarah Anstey South Australia
Graeme Sanders
6.11.08 6 hours
National Resource Refinement Workshop
Jurisdictional representatives
Bev Malone South Australia
Creswell Surrao Western Australia
Kathy Stapley Queensland
Paul Mayers Australian Capital Territory
Emma Smith Victoria
Neda Dusevic (teleconference)
New South Wales
Tim Coombs AMHOCN
6

Date Contribution capacity
Stakeholder Group
Name Jurisdiction
September – November 2008
Individual Submissions
Australian Mental Health Outcomes Classification Network
Tim Coombs AMHOCN
Clinical Services/Teams
4 clinicians from Royal Children’s Hospital Mental Health Service
Victoria
1 community team RCH-MHS
Cathi Richardson
Sarah Anstey + additional clinicians
South Australia
Graeme Sanders
Jo-Anne Dwyer Western Australia
Consumer and Carer Consultants
Jon Kroschel Victoria
Stewart Fenton Queensland
Juanita Fishwick Western Australia
South Australia
OM Co-ordinators Fiona Pilley Victoria
Kylie Scoullar Victoria
7

This resource was an initial attempt to pull together a wide variety of largely unwritten materials related to outcome measurement in mental health practice. It was also an opportunity to visually represent the opportunities and complexities to facilitate an ongoing dialogue between all involved in this activity.
To ensure relevance, currency and usefulness of the material it will need to be routinely reviewed and updated. It is an ambitious endeavour to create a living, organic and developmental resource to capture dynamic and changing aspects of clinical practice.
To provide input into the resource please visit: www.mhnocc.org/forum
Or speak with Outcome Measurement nominated staff in your service and/or jurisdiction.
1.3
Your
invi
tati
on8

1.4
Nav
igat
ion
How to use this resource
Design Tony Buzan asserts that “a Mind Map is a powerful graphical technique which provides a universal key to unlock the potential of the brain. It harnesses the full range of cortical skills – word, image, number, logic, rhythm, colour and spatial awareness – in a single, uniquely powerful manner. In so doing, it gives you the freedom to roam the infinite expanses of your brain”1.
A mind map is included in the following section, and forms the structure of this resource. There were a number of reasons for developing this resource as a mind map.
Firstly, it is an iterative process requiring simple labelling and association.
Secondly, it creates a structure that allows access to specific sections while representing that section within the whole.
Thirdly, it has the capacity to visually represent the range of possibilities for consumer outcomes in clinical practice.
Navigating this resourceThis resource has captured current practice opportunities focussing on consumer outcomes and, given that the utilisation of consumer outcomes is evolving, it will be reviewed and revised in the future.
The navigation of this resource is via:
• electronic links on the mind map
• traditional page numbering.
1 Buzan’s iMindMap™ Help Manual, page 4
LayoutEach of the branches of the mind map forms a section in the resource. In each section content is laid out in the following order:
• Position, value statement and link to national policy documents.
• Benefits and any risks of a particular approach or method.
• Examples.
This resource has been developed to allow the user to utilise areas of interest. It could also be utilised as part of a local implementation plan using small time-limited projects around a part of a specific section, and reviewed sequentially. This would break it down into smaller ‘do-able sections’ with an end result that the total resource would be covered (eventually) over time.
ContentThe content of this resource is current at November 2008. For clarification of terms refer to the Glossary (Appendix 2).
The content was developed predominantly by staff with a clinical mental health background, and drew on the collective experience of staff involved in the implementation and utilisation of consumer outcomes across Australian states and territories.
9
In addition to the collaborators consulted, the review of a number of intranet/internet sites informed the development of this resource including:
• Mental Health National Outcomes and Casemix Collection www.mhnocc.org
• Queensland Health intranet
• Victorian Department of Human Services internet www.health.vic.gov.au/mentalhealth/
• New Zealand’s National Centre of Mental Health Research - Te Pou internet (specifically the Australasian Mental Health Outcomes Conference 2007 pages) www.tepou.co.nz/page/23-Welcome
The National Outcomes and Casemix Collection (NOCC) involves clinicians and consumers measuring the health status of the consumer and noting change over time. Therefore, a decision was made to refer to the NOCC suite of measures as consumer outcomes rather than routine outcome measurement, ROM or outcome measurement. Consumer outcomes include all NOCC measures, clinician and consumer-rated.
The material contained in this resource is written for mental health clinicians but may also be useful for consumer and carer consultants employed in mental health services. It outlines strategies, principles and techniques for using consumer outcomes in clinical practice. With a few exceptions individuals are not specifically showcased.
ConsiderationsMaking this resource accessible and relevant for mental health clinicians across Australia is challenging as names/labelling vary considerably within services and across jurisdictions. Language used is consciously generic and inclusive to ensure that the content is applicable across age groups, service settings and jurisdictions.
The examples included in this resource are suggestions rather than an exhaustive list. It is critical that mental health clinicians refer to local and jurisdictional requirements related to protocol, policies and procedures and documentation before using any of these examples.
This resource is designed for clinicians and for use in clinical practice. As clinical practice is dynamic and changing, and as consumer outcomes become more embedded into practice, this resource offers a starting point for practice opportunities and continued development. Ideally it will be reviewed regularly by jurisdictional representatives to revise existing content and capture new material.
Consumers and carers are directly involved in consumer outcomes through a process facilitated by a clinician. It is the clinician’s responsibility to offer, explain and discuss completed self-assessment measures.
10

11
This is a LINKED PDF.Clicking on a section name below will take you to that section.
Consumer outcomes -tools for …
1.5
Con
tent
s m
ap

12

1. Getting started… 2 1.1 Foreword 3
1.2 Acknowledgements 4
1.3 Your invitation 8
1.4 Navigation 9
1.5 Content map/list 11
1.6 Key to symbols 15
2. Engaging 17 2.1 Clinician 18
2.2 Consumer 20
2.2.1 Offering 22
2.2.2 Dialogue 31
2.3 Carer 34
2.4 Manager 38
2.5 Partnerships 42
2.6 Endorsements 45
3. Practice 47 3.1 Assessment 48
3.2 Care plans 52
3.3 Review 55
3.4 Discharge 66
3.5 Supervision 67
4. Supporting functions 69 4.1 Documentation 70
4.2 Policies/procedures 72
4.3 Tips and suggestions 74
4.4 Service quality 76
5. Workforce development 81 5.1 Managers 84
5.2 Clinicians 86
5.3 Consumer and carer consultants (or equivalent) 90
5.4 Trainers 92
6. Resources 93 6.1 People 94
6.2 Materials 103
6.2.1 National 103
6.2.2 State and Territory 106
References 111 Websites 111
Published journals, reports, books, presentations, promotional materials 112
Appendices 113 Appendix 1 - Phase one – project overview and consultation processes 113
Appendix 2 - Glossary 117
1.5
Con
tent
s li
st 13

14
1.6
Key
to s
ymbo
lsDialogue Exploration
File Documentation/templates
Mail/postal address Attach
Limitations Waiting/training times
Imperative Schedule
‘Have a cuppa’ Self-assessment measure
Face to face Print
Groups Emerging technologies
Policy/procedures Database
Images from www.istockphoto.com
15

16

National Standards for MentalHealth Servicesendorsed by the AHMAC National Mental Health
Working Group December 1996
2. E
ngag
ing
Standard 3: CoNSumER AND CARER PARtiCiPAtioN Consumers and carers are involved in the planning, implementation and evaluation of the MHS1.
National Practice Standards for the mental Health WorkforceStandard 2: CoNSumER AND CARER PARtiCiPAtioN Mental health professionals encourage and support the participation of consumers and carers in determining (or influencing) their individual treatment and care. They also actively promote, encourage and support the participation of consumers, family members and/or carers in the planning, implementation and evaluation of mental health service delivery2.
According to Hatch (1985) culture “consists of conventional patterns of thought and behaviour, including values, beliefs, rules of conduct, political organisation, economic activity, and the like, which are passed on from one generation to the next”3. Allaire and Firsirotu in 1984 asserted that “what ever else they may be, organisations are...social creations and creators of social meanings”4.
How an organisation or agency understands, internalises and communicates its expectations and values will greatly influence how clinicians practice. It is no surprise then that clinicians who work in organisations that support consumer participation and consumer outcomes are more likely to be engaging in the process.
Consumers and carers are directly involved in consumer outcomes through a process facilitated by a clinician. It is the clinician’s responsibility to offer, explain and discuss completed self-assessment measures.
Medical leadership and engagement in consumer outcomes is vital to the successful implementation and utilisation of consumer outcomes in routine clinical practice.
1 Australian Health Ministers Advisory Council (AMHAC) - National Mental Health Working Group, Information Strategy Committee, National Standards for Mental Health Services, December 19962 Australian Health Ministers Advisory Council (AMHAC) - National Mental Health Working Group, Information Strategy Committee, National Practice Standards for the Mental Health Workforce, September 20023 Jones A and May J. Working in Human Service Organisations A critical introduction, 1992, Longman, Australia (page 229)4 Jones A and May J. Working in Human Service Organisations A critical introduction, 1992, Longman, Australia (page 228)
National Practice Standards for theMental Health Workforce
National Practice Standards for the Mental Health W
orkforce
Endorsed by the AHMAC National Mental Health
Working Group September 2002
National mental Health Services Standard
Engaging 17
18 Engaging
2.1 ClinicianClinicians strive to deliver safe, quality services by engaging with consumers and carers. Clinicians play a key role in mental health service delivery and are therefore integral to consumer outcomes. Clinicians seek to actively involve consumers and carers, where appropriate, in care planning processes.
Clinicians require training in the completion of the measures as well as opportunities to explore how consumer outcomes can inform clinical decision-making. Consumer outcomes provide a tool for multidisciplinary input, review and decision-making. The consumer outcomes also provide evidence for clinicians to identify professional development needs and to manage case loads.
Offering the consumer self-assessment measure is important as it:
• sets the value and expectation that the consumer’s perspective is important
• augments information from other key informants
• provides a baseline for future comparison.
The process of engagement, establishing rapport and developing therapeutic alliance is perhaps one of the most challenging aspects of mental health service delivery. Clinicians rely on their experience and expertise in engaging consumers irrespective of a consumers legal status. Mental health services have measures of clinical recovery implemented in routine practice and the challenge for clinicians is using these measures in a personal recovery orientated frame.
The consumer outcomes provide both opportunities at a single point in time as well as providing the capacity to look at change over time. The conversation between a consumer and clinician needs to focus on both areas of difficulty as well as strengths. Strength based conversation is still compatible with measures that rate according to difficulty or distress. If a consumer has rated an item as zero clinicians can spend time exploring what the consumer attributes the rating to:
• What are their strengths, supports and skills in this area?
• Are some of these transferable to other areas of their life?
While it is important to cover areas of difficulty, identifying areas of improvement or strength is crucial in building a consumer’s capacity to identify and manage their illness.
Engaging clinicians in the consumer outcomes agenda occurs through supporting them to:
• participate in training in the rating and also clinical utility
• showcase the use of consumer outcomes in clinical practice in forums across states and territories
• access information, resources, training materials, and attend forums.
With assistance from the Commonwealth Department of Health and Ageing, Quality Through Outcomes funding in 2005 -2008, jurisdictions have engaged clinicians, consumers and carers in a range of activities to further enhance the clinical utility of consumer outcomes.

Engaging 19
Suggested websites:
www.mhnocc.org www.health.vic.gov.au/mentalhealth/outcomes www.health.gov.au/internet/main/publishing.nsf/Content/mental-pubs-n-workstds www.aasw.asn.au www.ausot.com.au www.amicus-mhna.org www.psychology.org.au

20 Engaging
2.2 Consumer Consumer participation in public mental health services is fundamental to ensuring an effective and responsive system. Mental health services endeavour to actively promote and facilitate involvement by consumers in their treatment and care. Completion rates are influenced by how effectively self-assessments are offered.
The nationally available, aptly named ‘Whose outcome is it anyway? Consumer Self-Assessment in Mental Health’ resource/brochure/DVD was developed by consumers and carers for consumers and carers about the national consumer outcomes initiative and highlights the importance of consumer and carer voices.
Consumer outcomes provide a framework for consumer participation and the self-assessment process must include offering and completing the measure as well as dialogue regarding both the consumer and clinician perspectives as rated by the respective measures. Offering a self-assessment measure can facilitate engagement as well as collaboration between consumers, carers and clinicians. Also, discussion of self-assessment ratings with consumers (and where appropriate with carers) can enrich treatment and care planning. Self-assessment provides the opportunity for consumers, carers and clinicians to track progress through comparisons of ratings over time. Change over time is more difficult to monitor accurately without measurement tools.
Consumers and carers should also be provided with general information on consumers’ and carers’ roles, rights and responsibilities; documentation requirements including privacy and confidentiality; complaints process and consumer and carer structures/programs such as consumer advisory groups. Adequate provision of this information may go some way in allaying consumers’ concerns or uncertainty about consumer outcomes.
Consumers and their carers/families should be provided with verbal and written information on consumer outcomes to enable them to make an informed decision about participation. It is important that information includes how the measure will be used, what the consumer can expect and provides reassurance that their responses will be treated respectfully and discussed with their clinician. Wherever possible, the provision of information should be in the consumer’s preferred language.
Whoseoutcome is it anyway?
QUOTES:(From a workshop involving consumer and
carer consultants as part of the Western
QUATRO Project, September 2005)
“Consumer self assessment is seen as a
vehicle in the consumer’s journey. Used to
discuss goal setting, to assist in evaluating the
service being received and assess when to
move on.”
“What does being valued really look like and
how does it feel?”“Map of recovery; where we are, where we
want to get to.”“Triad - dialogue and relationship with consumer,
carer and case manager. Working together
to identify personal priorities of needs.” “By sharing and exploring the information it
will set up an expectation that the consumer’s
opinion is valued.”
WHERE CAN I GET MORE INFORMATION?
If you have any questions, concerns or would
like to get more information on consumer self
assessment or clinician measures, talk to:• Your mental health clinician• Consumer and/or carer consultants
• Family, friends or carers• Other consumers or consumer groups• Other carers or carer groups• www.mhnocc.org
LOCAL SERVICE INFORMATION
Consumer Self Assessment in Mental Health

Engaging 21
What is the carers’ role?As part of engaging the consumer in consumer outcomes, it is helpful to:
• explore the carer’s overall role in treatment and care
• consider what role they may have in consumer outcomes.
Clearly understanding and articulating expectations on respective roles is important. Consumer outcomes provide an opportunity for identifying different perspectives, highlighting areas of agreement or disagreement, and a way of mapping a consumer’s journey.
Carer or family member involvement in consumer outcomes can take many forms, including:
• Completion of a parent version of the Strengths and Difficulties Questionnaire (SDQ) in child and adolescent mental health services.
• Involvement in a discussion with the consumer and clinician about the measures.
• Encouragement for consumers to (a) complete the self-assessment measure, (b) to return the completed form and (c) ask for feedback on measures.
• Assistance for consumers in completing where appropriate and the consumer feels comfortable. There are instances when a carer may provide assistance to the consumer in completing their self-assessment. It is crucial that the answers provided are the consumers’ perspective and not completed by the carer on the consumers behalf.
• While there is no agreed carer measure for adult or older person services, if a consumer completes a self-assessment the carer could be involved in the dialogue with the clinician and consumer and contribute their perspective (to confirm or challenge), assuming that the consumer has given permission for the carer to be a) involved or b) to see their answers to the self-assessment. The carer could also provide their perspective to enhance the care provided.
• Clinicians need to acknowledge and be sensitive to the potential tensions this may create in the consumer and carer relationship.
• Involvement in care planning incorporating consumer outcomes.
• Clarification with carer/family in understanding the established goals.
For information on the nationally mandated outcomes measures visit the sites detailed in the materials section of this resource.
Refer to: 5.2 Resource materials

22 Engaging
2.2.1 offeringMental health clinicians spend considerable time and energy in preparation and the introduction of a particular type of treatment or therapy with a consumer. It is well acknowledged that there are ’windows of opportunity’ in which engagement can occur with optimal engagement. Consumer outcomes need to be conceptualised in the same way.
The way in which clinicians offer the self-assessment is the best predictor of whether a consumer will complete the self-assessment measure. Like clinical practice in general, the successful offering of the consumer self-assessment requires skill, thought, preparation and effort on the part of the clinician.
It is the clinicians responsibility to ensure the self-assessment measure is offered and completed. There are a number of ways that the consumer self-assessment can be offered and completed including waiting times, face-to-face, groups, by mail or through emerging technologies. For further details on these options see examples box at the end of this section.
Refer to: 2.2.1 Examples
Increasingly services are using a range of processes and roles to enhance and support the offering and completion of the consumer self-assessment measure. If the clinician relinquishes the offering of the self-assessment measure there are missed opportunities for engagement and therapeutic alliance.
Common issuesOffering the self-assessment will be enhanced by consideration and attention to the following key areas of concern, including:
• Providing reassurance regarding privacy and confidentiality
• Consumer self-assessment collection requirements
- Temporary contraindications
- General exclusion criteria
• Special considerations
- Culture
- Literacy
- Language
- Co-existing disabilities/disorders
Refer to: a comprehensive list of items to enhance the offering of the consumer self-assessment go to the AMHOCN checklist in the examples at the end of this section.
Privacy and confidentialityIt is important to recognise that all health consumers have a legislative right to privacy as it relates to their health information and their concerns need to be pro-actively addressed. It is critical that mental health staff inform consumers (and carers where appropriate) about the privacy standards and safeguards. In addition to the legal aspects it is helpful for consumers (and carers where appropriate) to understand the rationale for why information is collected and how this information can assist in the provision of care.

Engaging 23
It is important for mental health staff to be aware of the following:
- Outcome measurement is governed by the same legislation and considerations as other clinical activities and the consumer has a right to privacy, confidentiality and access to their records.
- Once these measures are entered in a consumer’s case notes and/or the local database, self-assessment information becomes part of the consumer’s clinical record. This means that, together with other case notes, the self-assessment information can also be viewed by the treating clinicians in other clinical contexts, such as case review or the development of an Individual Service Plan (ISP) or care plan. These are all routine clinical processes designed to benefit the consumer.
- As with all other consumer data, self-assessment records are treated as strictly confidential. They can be seen, handled and examined only by authorised staff and are covered by all the protections afforded by the relevant state or territory Mental Health Act and Health Records and Information Privacy Acts. It is important to note that some consumers might be reluctant to identify areas of difficulty on the consumer self-assessment if these could be presented to a mental health review board or tribunal.
- Where aggregated outcome measurement data are used for broader purposes of analysis and quality improvement, they must be de-identified regardless of whether they are derived from data gathered by the clinician or consumer self-assessment.
Consumer self-assessment collection requirementsThe collection requirements are articulated in the National Outcomes and Casemix Collection protocol:
National outcomes and Casemix Collection: technical Specification of State and territory reporting requirements for the outcomes and casemix components of ‘Agreed Data’ under National mental Health information Development Funding Agreements Department of Health and Ageing, Canberra, 2002.
It is mandatory for clinicians to offer the consumer self-assessment at certain points, but completion of the measure is always voluntary for consumers. While the national protocol does not require offering in acute inpatient settings however some jurisdictions recognise the value of offering in this setting.
It is important to consider revisiting the consumer’s decision not to participate. Further development of engagement with the clinician, increasing wellness and familiarity with the service, may lead to a shift in the consumers’ willingness and interest in completing the measure.
Even partially completed self-assessment measures are useful and the process of offering provides a good opportunity for engagement.
While it is mandatory for clinicians to offer the self-assessment at certain points there are temporary contradictions and general exclusion criteria detailed below:
temporary contraindications- If the consumer’s current clinical state is severe enough to make it unlikely that their responses to
a self-assessment questionnaire could be obtained or, if their responses were obtained, it would be unlikely that they were a reasonable indication of the person’s feeling and thoughts about their current emotional and behavioural problems and wellbeing.

24 Engaging
- Where an invitation to complete the self-assessment is likely to be experienced as distressing or requires a level of concentration and effort the person feels unable to give.
General exclusion criteriaExclusion criteria are further defined at a jurisdiction and service level related to electronic data systems. Dependent on the state or territory there are a range of recording/coding options and requirements. General exclusions include:
- If the consumer’s cognitive functioning is insufficient to enable the understanding of the task as a result of an organic mental disorder or an intellectual disability.
- If cultural or language issues make the self-assessment measure inappropriate.
Special considerationsClinicians are encouraged to refer to relevant national, state and local policies regarding the use of translators or interpreters, and cultural considerations in working with consumers from culturally and linguistically diverse communities or indigenous consumers. Using consumer outcomes with indigenous consumers has been explored and addressed in various ways including the development of guidelines for completing the clinician rated measures with specific consumer groups.
Cultural considerations are not just unique to CALD and indigenous consumers and the following should be considered:
- A consumer’s cultural community and their right to confidentiality of personal information, given that some cultural communities are small and intimate.
- Cultural implications for participation in consumer self-assessment such as (a) cultural taboos or sensitivities in answering a certain way, (b) cultural expectations regarding who can be approached in the family for liaison with the health service, and (c) a fear of the consequences of answering honestly.
The completion a self-assessment measure can also be influenced by literacy, language and co-existing disabilities/disorders. It is important for clinicians to consider the following:
- Literacy - It is widely accepted that a consumer’s developmental course is affected by the onset and impact of major mental illness. Therefore, it is reasonable to assume that literacy should be considered as a potential barrier to the completion of the consumer self-assessment measure. If literacy is identified as an issue, it is helpful to identify:
A person with whom the consumer feels comfortable to assist with reading and completing the measure. This may be a family member or friend, a support worker or mental health staff. This may include consumer or carer consultants, key worker/case manager or peer support worker. It is important that the consumer feels comfortable to answer the questions without fear of consequences or repercussion. It is important to revisit this issue as the appropriate support person may change over time.
A suitable environment to complete the self-assessment measure. People may feel embarrassed if they have difficulty reading and writing and it is important that the consumer is afforded privacy and sensitivity.
Engaging 25
- Language - Wherever possible, measures should be provided in the consumer’s primary language while recognising that some consumers may not be able to read in their primary language. In addition the use of translators should be considered. Best practice supports the use of independent translators though informal assistance can often be provided by family members, friends or community volunteers. A number of the consumer self-assessment measures have been translated for more information:
Refer to: 6.2 Resource materials
- Co-existing disabilities/disorders - It is also important to consider any difficulties associated with sight, hearing, intellectual capacity, physical disability (particularly from drug-induced movement disorders), or active substance use which may affect a consumers capacity to participate in the self-assessment process.
Enhancing the offering of consumer self-assessmentAs part of the clinical utility materials produced by AMHOCN in 2005, a fidelity checklist5 identifies key components for best practice in offering consumer self-assessment, including [the clinician]:
• Presents consumer self-assessment as a positive experience and a genuine attempt to engage the consumer in treatment planning.
• Assesses for potential difficulties the consumer may have in completing the self-assessment.
• Presents rationale for completion of the consumer self-assessment measure including:
– genuine attempt to understand consumer perspective
– genuine attempt to involve consumer in assessment and care planning
– tool for clinician to monitor progress
– tool for consumer to monitor progress
– information can be used for service development and quality improvement processes.
• Reinforces consumer ownership and personal responsibility for completion of self-assessment, promoting personal responsibility for illness self-management.
• Explains the self-assessment is part of the medical record and subject to the same protections of privacy and confidentiality.
• Supports and encourages the consumer’s completion of the self-assessment in an appropriate manner.
• Provides appropriate assistance and prompting during completion of the measure [while being mindful of the guidelines for prompting].
• Provides positive reinforcement for completion of the measure.
• Offers appropriate assistance if consumer becomes distressed or cannot complete the measure. [In this instance assistance provided should be for the distress not assistance to continuing to complete the measure].
5 AMHOCN, Clinical Utility Training Fidelity Checklist, Enhancing the offering of consumer self-assessment, Materials, 2006

26 Engaging
making the self-assessment measure more engaging With consideration and recognition of local protocols and medical record standards, the more engaging and appealing the actual self-assessment form is, the more likely consumers are to complete it. Consider the following:
• Printing the forms either in colour, or on coloured paper.
• Putting a detachable cover on the form – “How are you feeling? How are you coping?
• Have your say… Will my information be kept private? Yes! All the information received about you is kept strictly private and confidential”6.
• Attaching an information sheet about (a) measure or (b) process – What will happen to it after it is completed? The provision of written information to consumers about self-assessment ought not to be regarded as adequate in terms of the offering and following of these measures.
• Attaching a reply paid self-addressed envelope to enable consumers to send in the completed form, though this method of taking away and returning by mail is not optimal.
• Providing the consumer with a copy of the self-assessment measure.
Examples of completion methodsThere are a variety of methods or ways of completing hard copy consumer self-assessment measures. It is important to provide consumers (and carers in child and adolescent services) a private place to go, and adequate time to complete the self-assessment measure. This list is by no means exhaustive but includes a number of methods for completion, including:
• waiting times
• face-to-face
• groups
• mail out
• emerging technology
Waiting timesTime spent waiting for clinic appointments is often reported as problematic by consumers and carers. However, it may be suggested that where consumers are waiting for an ambulatory clinical appointment the consumer self-assessment could be completed.
If waiting times are going to be used as an opportunity to complete the self-assessment measure, it is critical that there is sufficient information provided to consumers beforehand. Furthermore, it is important to be mindful of privacy in this situation and the potential for distress.
6 Queensland Health, Mental Health Inventory cover

Engaging 27
ideally, this option would be used for existing consumers of the service or those who had completed a self-assessment on a prior occasion. If waiting times are utilised for completion, it is imperative that there is a process to ensure that:
• there are opportunities for the consumer to seek clarification or support if required
• the consumer is thanked for taking the time to complete the measure
• the original self-assessment is provided to the consumers key worker/case manager
• that the key worker/case manager follows up with the consumer
• completed forms are entered into the electronic database.
Face-to-faceClinicians are busy with finite resources and increasing demands on their time. Offering the consumer self-assessment requires an explanation, may involve some encouragement and for some, will also require assistance in completion. So for some consumers, arranging a dedicated time period either at a clinic appointment or a home visit to complete the measure is a good option. Co-ordinating this appointment with the review requirements of the National Outcomes Casemix Collection (NOCC) protocol will ensure that the consumer measure is ready to enter into the database.
One way to use limited time efficiently might be for the clinician and the consumer to complete their respective measures at the same time, but independently. This is likely to promote discussion between the consumer and clinician about all of the measures, which would ultimately be mutually beneficial.
Once the measures are completed and entered into the electronic database you will be able to generate a report/graph. A copy of this could be provided to the consumer at the end of the session for future discussion or provided at the subsequent appointment.
GroupsGroups are utilised in some mental health services for therapy and education, though group programs vary between child and adolescent, adult and older person programs. The offering of a consumer self-assessment is a clinical activity and as such, if this method was used the group would need to be facilitated by appropriately trained mental health clinicians. If the self-assessment measure was introduced in a group setting, there needs to be appropriate attention to facilitating dialogue and ensuring the ratings are followed up by the consumers case manager/key worker.
Offering and completion in a group setting can be problematic from both a privacy perspective and the risk of group coercion for participants to complete a measure when they do not wish to do so. There are some potential limitations of completing the self-assessment measure in a group setting, including:
• It may undermine the clinician and consumer relationship by limiting the opportunity for dialogue and a collaborative process in consumer outcomes.
• Potential to highlight literacy difficulties and therefore cause disengagement.
• Potential to cause distress for the consumer which may be difficult to manage immediately in a group setting.

28 Engaging
• Difficulties in aligning with local collection protocol/requirements.
• Limited to registered consumers and in a setting that collects the consumer self-assessment.
If groups are utilised it is imperative that:
• the voluntary nature of completion is respected
• the consumer is thanked for taking the time to complete the measure
• the original self-assessment is provided to the consumer’s key worker/case manager
• a copy is provided to the consumer to discuss further with their case manager/key worker
• that the key worker/case manager follows up with the consumer
• reassurance and support are provided if consumer has difficulty completing measure or becomes distressed
• completed forms are entered into the electronic database.
Suggestion:
Thinking about groups conducted in your service, are there opportunities to run a session on consumer outcomes?
Exploring and completing consumer self-assessment in a group setting enables:
• discussion of consumer participation and its value
• discussion on the consumer outcomes, including the clinician and consumer measures
• exploration of the consumer self-assessment measure, tricky questions, possibilities of how information could be used
• space at the end for participants to individually complete their self-assessment measure.
Group settings provide support for consumers who need assistance in completing, and an opportunity for normalising issues or distress some of the questions could cause.
mail outIt is common in mental health services for consumers and carers, where appropriate, to receive information and requests from services via the mail.
There are significant limitations to this method including:
• it does not provide an opportunity for consumers to seek clarification
• it does not generally convey value or merit for the consumer to take the time to complete
• lack of follow up procedures to ensure that consumer’s completed forms are returned, acknowledged, followed up and entered onto the database.
If this method is used it is imperative that:
• A warm and inviting letter is included that clearly articulates the value and importance of completing and what they can expect to happen once it is completed – that their key worker/case manager will be notified and will follow up with them the next time they see them, and that the information will be entered into the electronic database to ensure future use of the information.

Engaging 29
• There is adequate information available to the consumer and carer. It is a good idea to include any information sheets/brochures with the form.
• Consumers and carers are encouraged to discuss any concerns with staff from the service.
• Reply paid envelope is included.
• A timeframe for completion and return to the service in order to activate the follow up process to retrieve the completed forms, to follow up with the consumer and discuss the ratings and the process for completion.
Suggestion:
A novel idea might be to add a quality coffee or tea bag and in the letter say something like ‘please take a moment to have a coffee/tea on us, and take a moment to tell us how you feel you are going’.
Child and Adolescent Mental Health Services have reported sending out the Strengths and Difficulties Questionnaire (SDQ) prior to the first session for completion. The ratings are then discussed with the clinician and parent, or clinician, young person and parent at the initial session.
Emerging technologiesSome states and territories are exploring the use of emerging technologies for direct consumer entry of the consumer self-assessment measures. Touch screens or computer entry are potentially more engaging and immediate for some consumers.
There are some potential issues (or risks) with this method, including:
• Sufficient preparation may not have occurred and the consumer is not able to make an informed decision about participating.
• May be intimidating if the self-entry is undertaken in a public place such as in a waiting area or in front of a clinician.
• If the software/hardware does not interface with the statewide databases.
• If consumers self-enter and a report is automatically generated that clinicians may not necessarily review or discuss with the consumer.
Therefore, if this method is used, it is imperative that:
• There are opportunities for the consumer to seek clarification or support if required.
• The consumer is thanked for taking the time to complete the measure.
• There is a mechanism for providing the ratings (self-entered by the consumer) to the consumers key worker/case manager.
• The key worker/case manager follows up with the consumer, and engages in a dialogue about the process and the ratings.
• There is a mechanism to ensure that the ratings are available on the relevant electronic database.

30 Engaging
Areas for further consideration include:
• acceptability of this technology by consumers and carers
• availability and usefulness of the technology
• what happens to the ratings, issues such as data security
• interface with the statewide databases
• capacity to generate reports for consumers once ratings are entered
• the role of the clinician in this process.
While some of these issues are specific to the technology, most are also issues in using hard copy forms.

Engaging 31
2.2.2 DialogueEvery effort must be taken to make consumers feel safe and comfortable to complete and discuss consumer outcomes.
The clinician rated measures are a summary by the clinician of an overall assessment. While the measures are important it is the dialogue and the quality of the dialogue in conjunction with range of mental health information that enhance collaborative care planning. The completion of measures by both clinician and consumer can provide a framework for discussion. Dialogue can be about status at a particular point in time but also an opportunity to discuss change.
The consumer outcome measures are tools to enhance the dialogue by:
• creating a common language
• routinely seeking and valuing the consumers perspective
• providing transparency of the clinician’s assessment which can provide a platform for discussion that is somewhat more removed and objective than ’Well I think you have these problems’ and anecdotal evidence alone
• identifying similarities/differences in perspectives and priorities
• identifying both strengths and difficulties:
- If a consumer has rated an item as zero you can spend time exploring what the consumer attributes the rating to, to identify areas of strength
• Consumers of public mental health services experience areas of difficulty, distress and disability. Therefore, measuring against these areas is helpful to ensure that interventions and treatments can be appropriately targeted with the goal of increasing functioning and reducing distress and difficulty.
• Visually mapping change over time
Engaging in a meaningful dialogue with consumers about their outcomes, especially where there are differences of perspective between the clinician and consumer, can be very challenging for both parties. It takes skill on the part of the clinician to frame the ratings in a way that values both perspectives. It is particularly challenging working with consumers who disagree about the reason or need for treatment.
Some mental health clinicians argue that it is not always possible to discuss consumer outcomes with consumers, particularly those who do not complete a self-assessment measure. The approach implemented by our New Zealand colleagues has been to implement only the HoNOS suites, but the message is clear that these measures need to be discussed with the consumer with the catchphrase ‘Show me my HoNOS’. A consumer self-assessment measure is also being developed in New Zealand.
For examples of how to use consumer outcomes in clinical practice.
Refer to: 3 Practice

32 Engaging
Enhancing the dialogue about consumer outcomesAMHOCN has also developed a fidelity checklist7 which identifies key components for best practice [when clinicians] review and provide feedback on the consumer outcomes. [They] include:
• exploring reasons why items are not completed [while being respectful that consumers may choose not to disclose some things]
• seeking clarification of responses to individual items as required
• providing opportunities for consumer to discuss items in more detail
• providing summary of consumer self-assessment [and clinician rated measures]
• explaining graphical report to consumer [providing clarification as required]
• discussing any change in the presentation of the consumer and its relationship to interventions or personal activities promoting recovery
• discussing consumer self-assessment [and clinician rated measures] in the context of goal setting
• linking summary to collaborative goal setting
• discussing future review of consumer self-assessment
• offering the consumer a copy of the self-assessment.
7 AMHOCN, Clinical Utility Training Fidelity Checklist, Enhancing the dialogue about consumer outcomes, 2006

Engaging 33
Examples There are a variety of ways to engage in dialogue on consumer outcomes and, consistent with practice generally, the capacity to engage in meaningful dialogue is dependent on factors such as:
• available resources including time, access to meaningful reports etc
• consumer language, literacy, cognition, acuity, complexity etc
• skill level of the clinician
• effort and interest by both the clinician and consumer.
Dialogue between clinicians, consumers and possibly carers could focus on:
Consumer self-assessment
• As a process - Was it useful? Were there difficulties?
• Individual items from the most recent completion that were either - (a) left blank, (b) had a rating of some difficulty or issue, (c) had a rating of no difficulty or (d) rated by the consumer in a way not expected or anticipated by the clinician (e.g. where a consumer rated a zero and the clinician has rated those areas as having a difficulty on the clinician measures, or where a consumer has rated a difficulty but the clinician didn’t identify those areas as of difficulty).
• Subscales or total score for the most recent completion.
• Subscale or total score for the most recent and historical completions.
• Comparison of the most recent consumer self-assessment with clinical reference material either at (a) individual item, (b) subscale or (c) total score levels.
• Opportunities to elaborate on the areas highlighted by the consumer self-assessment to look at what is happening in the consumers’ life and the connection/link to their responses.
Clinician rated measures
• Global summary of the suite of measures and areas of either agreement or difference between the consumer and clinician measures.
• Most recent rating of an individual measure by individual items, subscales or total score.
• Recent and historical ratings of an individual measure by individual items, subscales or total score.
• Comparison of most recent individual measure by individual items, subscale or total score with clinical reference material.
• As above, look beyond the scores to discuss the realities for the person which determine the score.
Refer to: 3.3 Review

34 Engaging
2.3 Carer • Carers are important and are valued for their support to consumers and mental health services.
• Active participation by carers is fundamental to ensuring an effective and responsive system.
• Engagement of families and carers has been articulated in a range of local, state and federal policies.
• Carer and consumer information is subject to privacy and confidentiality legislation.
• With the exception of child and adolescent services, there is no NOCC mandated measure for carer/family members version of the consumer measures used in adult and older person mental health services.
• Refer to: 2.2.1 More information on issues related to offering the self-assessment (including the parent version in Child and Adolescent) go do the consumer sections addressing the following:
• Carers not only have expectations but a role in encouraging consumer outcomes collection.
• Providing reassurance regarding privacy and confidentiality
• Consumer self-assessment collection requirements
- Temporary contraindications
- General exclusion criteria
• Special considerations
- Culture
- Literacy
- Language
- Co-existing disabilities/disorders
What is the carers’ role?As part of engaging the consumer in consumer outcomes, it is helpful to:
• explore the carer’s overall role in treatment and care
• consider what role they may have in consumer outcomes.
Clearly understanding and articulating expectations on respective roles is important. Consumer outcomes provide an opportunity for identifying different perspectives, highlighting areas of agreement or disagreement, and a way of mapping a consumer’s journey.
Carer or family member involvement in consumer outcomes can take many forms, including:
• Completion of a parent version of the Strengths and Difficulties Questionnaire (SDQ) in child and adolescent mental health services.
• Involvement in a discussion with the consumer and clinician about the measures.
• Encouragement for consumers to (a) complete the self-assessment measure, (b) to return the completed form and (c) ask for feedback on measures.

Engaging 35
• Assistance for consumers in completing where appropriate and the consumer feels comfortable. There are instances when a carer may provide assistance to the consumer in completing their self-assessment. It is crucial that the answers provided are the consumers’ perspective and not completed by the carer on the consumers behalf.
• While there is no agreed carer measure for adult or older person services, if a consumer completes a self-assessment the carer could be involved in the dialogue with the clinician and consumer and contribute their perspective (to confirm or challenge), assuming that the consumer has given permission for the carer to be a) involved or b) to see their answers to the self-assessment. The carer could also provide their perspective to enhance the care provided.
• Clinicians need to acknowledge and be sensitive to the potential tensions this may create in the consumer and carer relationship.
• Involvement in care planning incorporating consumer outcomes.
• Clarification with carer/family in understanding the established goals.
There are a variety of ways to engage in dialogue on consumer outcomes and, consistent with practice generally, the capacity to engage in meaningful dialogue is dependent on factors such as:
• available resources including time, access to meaningful reports etc
• consumer and carer literacy
• skill level of the clinician effort and interest by both the clinician and consumer (young person and parent/caregiver in CAMHS).
Suggested websites:
www.health.gov.au/internet/mentalhealth/publishing.nsf/Content/doha-plan-1 www.health.vic.gov.au/mentalhealth/cpg/families.htm

36 Engaging
Enhancing the dialogue about consumer outcomesFor this section, consumer includes both young person and parent/caregiver in CAMHS.
AMHOCN has also developed a fidelity checklist8 which identifies key components for best practice [when clinicians] review and provide feedback on the consumer outcomes. [They] include:
• exploring reasons why items are not completed [while being respectful that consumers may choose not to disclose some things]
• seeking clarification of responses to individual items as required
• providing opportunities for consumer to discuss items in more detail
• providing summary of consumer self-assessment [and clinician rated measures]
• explaining graphical report to consumer [providing clarification as required]
• discussing any change in the presentation of the consumer and its relationship to interventions or personal activities promoting recovery
• discussing consumer self-assessment [and clinician rated measures] in the context of goal setting
• linking summary to collaborative goal setting
• discussing future review of consumer self-assessment
• offering the consumer a copy of the self-assessment.
Dialogue between clinicians and consumer (including parents/caregivers in CAmHS and possibly carers in Adult/older Person):
Consumer (young person and parent/caregiver* in CAMHS) self-assessment
• As a process - Was it useful? Were there difficulties?
• Individual items from the most recent completion that were either - (a) left blank, (b) had a rating of some difficulty or issue, (c) had a rating of no difficulty or (d) rated by the consumer (young person and parent/caregiver in CAMHS) in a way not expected or anticipated by the clinician (e.g. where a consumer rated a zero and the clinician has rated those areas as having a difficulty on the clinician measures, or where a consumer (young person and parent/caregiver in CAMHS) has rated a difficulty but the clinician didn’t identify those areas as difficulties).
• Subscales or total score for the most recent completion.
• Subscale or total score for the most recent and historical completions.
• Comparison of the most recent consumer (young person and parent/caregiver in CAMHS) self-assessment with clinical reference material either at (a) individual item, (b) subscale or (c) total score levels.
8 AMHOCN, Clinical Utility Training Materials Fidelity Checklist, Enhancing the dialogue about consumer outcomes, 2006

Engaging 37
• Opportunities to elaborate on the areas highlighted by the consumer (young person and parent/caregiver in CAMHS) self-assessment to look at what is happening in the consumers’ life and the connection/link to their responses.
* This could also include multiple versions of the consumer self-assessment measure at a single collection point and may include similarities/differences between parent and parent, parent and teacher, or young person and teacher.
Clinician rated measures
• Global summary of the suite of measures and areas of either agreement or difference between the consumer and clinician measures.
• Most recent rating of an individual measure by individual items, subscales or total score.
• Recent and historical ratings of an individual measure by individual items, subscales or total score.
• Comparison of most recent individual measure by individual items, subscale or total score with clinical reference material.
• As above, look beyond the scores to discuss the realities for the person which determine the score.

38 Engaging
2.4 manager Managers are culture carriers and their:
• Commitment to consumer and carer participation will greatly influence the focus of service delivery.
• Commitment to consumer engagement in consumer outcomes will greatly influence the uptake of this activity by clinicians.
• Leadership is critical for the successful implementation, integration and utilisation of consumer outcomes.
Managers are well informed and engaged:
• Drawing on a range of information sources to understand, manage, monitor and inform decisions about their services.
• Requiring information and opportunities for skill development about the measures themselves, how clinicians might be able to utilise them and also, how they as managers might be able to use the information.
• In a comprehensive information development agenda and are excellent advocates and supporters of consumer outcomes.
• Recognising breadth of the consumer outcomes initiative and its implications for practice change.
• Grappling with how to incorporate consumer outcomes data at both the individual and aggregate levels.
Managers are actively planning the delivery of mental health service:
• Striving to ensure the delivery of safe quality mental health services and utilise a range of existing structures to manage this such as clinical and corporate governance, quality committees etc.
• Consumer outcomes can help inform the process of planning, delivering and evaluating services.
Managers or team leaders in public mental health services typically have a clinical background so a review of the factors for engaging clinicians is helpful. It is important to consider what management skills and knowledge they have to determine how consumer outcomes could inform their work.

Engaging 39
Providing supporting structures Consumer outcomes should be incorporated into clinical and corporate governance processes and can be enhanced by operational support that the organisation provides to its clinicians. Quality managers and quality frameworks are well placed to support the completion and use of consumer outcomes in routine practice.
Access to professional development opportunities enables clinicians to remain aware, interested and current. Agencies need to acknowledge the breadth of professional development requirements for mental health clinicians including discipline-specific, treatment modality-specific, operational requirements e.g. information systems, consumer outcomes, advanced level training for trainers, managers, supervisors.
Managers who actively promote and facilitate supervision processes at both the professional and operational levels will provide opportunities for clinicians to:
• Manage workloads including understanding of intensity, complexity and interventions (e.g. consumer outcome collection history).
• Monitor case loads and complexity (e.g., by number of items of clinical significance each clinician in a team has on their list) to enhance case allocation.
• Assess consumer outcomes – note consumers who are improving (possible plans for discharge), those not improving (possible plans for referral or additional supports) as well as those who remain the same. It could also provide an opportunity to explore issues related to offering and engagement in meaningful dialogue on the consumer self-assessment measure.
• Discuss multidisciplinary perspectives on a consumer’s presentation, interventions and outcomes.
• To explore the impact of their values and beliefs, professional identity, morale and identification of long term professional development as they relate to the consumer outcome agenda.
In addition to formalised supervision, peer support and mentoring are very powerful and non-threatening approaches that can be used to enhance skills in the workplace or to model a particular value and behaviour. Having ‘champions’ or people with a particular interest or skill work alongside clinicians who would like to enhance their skills, for example, using computers, consumer outcomes databases, reporting, observation of clinician and consumer in self-assessment process either in offering or engaging in dialogue etc. Mentoring Works states that “Although the evidence is limited, mentoring is more effective as an ’all round’ approach than off site training” with positive outcomes such as “higher retention rates, improved productivity, improved cohesion and loyalty, increased skill leading to better client outcomes” 9.
Services can provide tangible assistance by acknowledging and valuing the roles of ‘champions’, trainers and mentors. Services can do this by:
• providing clear expectations of the roles and responsibilities for these roles
• ensuring there is adequate infrastructure to support the roles such as regular meetings, mentoring and training opportunities
• acknowledging the time requirement for these roles and ensuring that this time commitment is considered as part of their workload.
9 www.mentoringworks.com.au/notice.html

40 Engaging
Examples for how managers might be involved
managers have a significant role to play in strengthening:• Infrastructure and supporting information development and utilisation.
• Processes which are clear and consistent. For example documentation requirements, entry and exit criteria from programs/teams etc.
• Consumer and carer participation that is actively encouraged and valued including the provision of structural support and resources.
• Monitoring role such as:
– compliance of their team, service or jurisdiction of reporting requirements – minimum data set including consumer outcomes
– effectiveness of their team, service or jurisdiction. How do we do this now? Consumer outcomes are being included in the development of stage two performance indicators in the effectiveness domain of the National Health Performance Framework - Health System Performance.
• Showcasing areas of innovative practice.
• Articulation and communication of expectations for consumer outcomes including training, support for clinicians, compliance, and engagement of consumers in self-assessment and in using the consumer outcomes ratings.
• Opportunities for training including orientation, rater/rating and use of consumer outcomes.
• Integration of consumer outcomes in routine clinical practice:
- collection should occur following a comprehensive assessment
- utilisation at a consumer level should occur in clinical reviews, developing care plan, clinical supervision and in routine discussions with consumers and carers
- utilisation at an aggregated level should occur in existing service quality processes such as accreditation, program evaluation and quality improvement activities and committees.
• Identifying, utilising and developing outcome measurement champions.
• Use of aggregated consumer outcomes to identify areas for professional development.
• Knowledge base of team skills and strengths and encouraging mentoring.
Refer to: 4.4 Service quality

Engaging 41
Example of consumer outcomes used for case load
2005 - AmHoCN Newsletter issue 9ADON - Community Manager, Caulfield Aged Psychiatry Service gave a presentation entitled “Can HoNOS be Used as a Case Load Management Tool?”
She outlined how the HoNOS is being used within her service to develop clinician understanding of the core business, including the need to define key intake and discharge criteria and an understanding of the burden of caseloads. So, for example, a HoNOS score of greater than 12 indicates the need for referral to the “Acute Care” team. While HoNOS scores of 10 - 12 are given a high contact weighting (time consuming and significant workload). A HoNOS score of 6 - 10 indicates the necessity for medium contact, between weekly – fortnightly visits, but with agency liaison and support. While HoNOS scores of 4 - 6 indicate low contact and relatively stable. For those consumers with HoNOS scores below 4, clinicians are encouraged to consider discharge or shared care. Sandra concludes: “Whilst there is still a way to go, I believe there is reason to determine the value of existing tools to drive effective case management, clinical interventions and clinical priority.”
www.mhnocc.org/amhocn/HoNOS_%20as_a_%20caseload_management_tool.pdf
2007 - Australasian mental Health outcomes Conference – NZ Paper presentation by Sandra Keppich-Arnold, Associate Director of Nursing and Operations, Alfred Psychiatry, AUSTRALIA
Paper 5: Using outcome measurement as an adjunct to caseload management improves clinical interventions and reduces case load demands
www.tepou.co.nz/page/323-Speakers-039-Presentations-Day-One
2008 - QuAtRo ViC Bulletin 3 (march 2008) - melbourne“Sandra Keppich-Arnold presented an informative case study where discussion of a very low HoNOS 65+ score in a clinical review meeting raised questions that led to an extensive review of the consumer’s care. Problems of isolation and social withdrawal revealed underlying mental health difficulties, more effective treatment was provided, and the woman was able to re-establish her former active and social life.”
www.health.vic.gov.au/mentalhealth/outcomes/quatro-bulletins/march08.pdf

42 Engaging
2.5 PartnershipsMental health clinicians actively engage with a range of service providers and support agencies to support consumers in managing their illness and achieving their goals. Where consumers have consented to sharing their consumer outcomes information across services, it is worthwhile considering:
• If there is a process for sharing consumer outcomes with external agencies? If so:
– How is this information provided? – Verbally, total scores, total and subscale, as part of other information, stand alone reports.
• Does the external organisation collect consumer outcomes? If so:
– What are they?
– Are they shared with the consumer?
– Are they available for sharing with the mental health service?
• Does the external organisation utilise aggregate level outcomes data? If so:
– How do they use it?
– Where is it obtained?
– Are consumers of their service aware of this?
Non-Government organisations (NGo)
Peak bodies There are a number of local, state and federal peak bodies for mental health who play a powerful role in lobbying for quality mental health care. While use of individual consumer outcomes is unlikely in these organisations, there is potential for consideration and utilisation of aggregate level consumer outcomes.
Examples of national peak bodies:
• SANE - www.sane.org
• Mental Health Council of Australia - www.mhca.org.au/AboutUs/ListMemberOrgs.html
• Mental Health Carers ARAFMI Australia - www.arafmiaustralia.asn.au
Examples of state level peak bodies include:
Victoria
• Victorian Mental Illness Awareness Council - www.vmiac.com.au
• Victorian Mental Health Carers Network - www.carersnetwork.org
South Australia
• Mental Health Coalition – https://owa.sagems.sa.gov.au/exchweb/bin/ redir.asp?URL=http://www.mhca.org.au/donate.html
• Carers SA
• Health Consumers Alliance Inc of South Australia

Engaging 43
Support agenciesIt is common for consumers of public mental health services to access non-government organisations for non-clinical support and activities. There is considerable variety in the types of non-government organisations accessed by consumers of public mental health services, from psychiatric disability or mental health-specific, to generic community and private agencies.
Consumer outcomes could be used to inform:
• referral to an external support agency by longitudinally mapping consumers areas of difficulty and improvement
• prioritising areas for activities or input by the support agency and can inform joint management plans
• consumers perspective on their progress.
It is important to consider the interface between the support agency and the clinical mental health service. Consider the following questions:
• If there is a process for sharing consumer outcomes with external agencies? If so:
– How is this information provided? – Verbally, total scores, total and subscale, as part of other information, stand alone reports.
• Does the external organisation collect consumer outcomes? If so:
– What are they?
– Are they shared with the consumer?
– Are they available for sharing with the mental health service?
• Does the external organisation utilise aggregate level outcomes data? If so:
– How do they use it?
– Where is it obtained?
– Are consumers of their service aware of this?
Government departmentsConsumers of public mental health services are often engaged with a range of local, state or federal government departments, including:
• health (general/acute) and ageing
• education, employment and workplace relations
• families, housing, community services and indigenous affairs
• human services
• disability
• income support (Centrelink)
• child protection
• juvenile justice
• corrections
• police
• immigration and citizenship.
44 Engaging
The relationships with, and information requirements for, each of these departments varies considerably. Consequently, the way in which mental health services provide information will vary in type, breadth, method and frequency. Notwithstanding these requirements and variation in the consumer presentation and needs, it is helpful to consider opportunities consumer outcomes could provide.
General practiceIt is common practice for consumers accessing public mental health services to have shared care arrangements with general practice clinics and general practitioners. In addition to the two federal government initiatives outlined below, it is helpful to consider general practitioners and their:
• understanding of consumer outcomes
• potential role, for example:
– provision of collateral information in line with the collection requirements (admission, 91-day review or discharge) to inform the completion of the measures by the mental health clinician
– obtaining copies of the measures as part of their information source, particularly the consumer self-assessment measure. Could be sent a copy of the scores together with individual care plan (if not already included) where care is shared/on discharge to GP.
Examples of specific programs delivered through general practice that may have a role in utilising or collecting consumer outcomes:
• Mental Health Nurse Incentive Program
– www.medicareaustralia.gov.au/provider/incentives/mental-health.jsp
– www.medicareaustralia.gov.au/provider/incentives/files/2111-mental-health-nurse-incentive-program-program-guidelines.pdf
• Better Access to Mental Health Care Initiative
– www.primarymentalhealth.com.au/site/index.cfm?display=15129
• Mental Health Shared Care with General Practice

Engaging 45
2.6 Endorsements AMHOCN, in collaboration with Barwon Health, the lead agency of the Victorian Western Cluster Quality through Outcomes Project, has produced a range of promotional and educational materials called ‘Whose outcome is it anyway? Consumer Self-assessment in Mental Health’.
A DVD outlining the views of consumers, carers and clinicians has also been produced. This DVD is a training resource that explores the opportunities afforded by routine outcome measurement in clinical practice. Hard copies of the promotional materials including a “novelty flipper card” along with copies of the DVD and associated training materials are available on request to AMHOCN.
Consumer and carer QUOTES10:
• ‘Consumer self-assessment is seen as a vehicle in the consumer’s journey. Used to discuss goal setting, to assist in evaluating the service being received and assess when to move on.’
• ‘What does being valued really look like and how does it feel?’
• ‘Map of recovery; where are we, where we want to get to.’
• ‘Triad - dialogue and relationship with consumer, carer and case manager. Working together to identify personal priorities of needs.’
• ‘By sharing and exploring the information it will set up an expectation that the consumer’s opinion is valued.’
‘Consumer perspective Helen Connor, Consumer Representative mental Health Council of Australia, was a member of a discussion panel at the outcomes Conference titled ’mental Health outcomes: lessons learnt and challenges for implementation’11
Helen stressed the importance of clinicians engaging with consumers and carers regarding outcome measures. “It takes more than just handing a glossy brochure, saying it is your choice and then not really explaining it. The collection of outcome measures is only good if it enables consumers and clinicians to sit down and engage together and work in partnership. It is essential that all outcome measure results be shared with the consumer, not just the consumer rated measure. When you share all the results it is then about sitting down and having a discussion about why there may be differences in clinician and consumer rated measures. This will provide valuable information and will assist in the development of a care plan that meets the consumers identified needs”.
Whoseoutcome is it anyway?
QUOTES:(From a workshop involving consumer and
carer consultants as part of the Western
QUATRO Project, September 2005)
“Consumer self assessment is seen as a
vehicle in the consumer’s journey. Used to
discuss goal setting, to assist in evaluating the
service being received and assess when to
move on.”
“What does being valued really look like and
how does it feel?”“Map of recovery; where we are, where we
want to get to.”“Triad - dialogue and relationship with consumer,
carer and case manager. Working together
to identify personal priorities of needs.” “By sharing and exploring the information it
will set up an expectation that the consumer’s
opinion is valued.”
WHERE CAN I GET MORE INFORMATION?
If you have any questions, concerns or would
like to get more information on consumer self
assessment or clinician measures, talk to:• Your mental health clinician• Consumer and/or carer consultants
• Family, friends or carers• Other consumers or consumer groups• Other carers or carer groups• www.mhnocc.org
LOCAL SERVICE INFORMATION
Consumer Self Assessment in Mental Health
10 Australian Mental Health Outcomes Classification Network, ‘Whose outcome is it anyway? Consumer Self Assessment in Mental Health’ brochure, 2006
11 Queensland Health, Outcomes Initiative Update 8
46 Engaging
SA Forum 7/4/08 A day with a Consumer/Carer focus
Tania Lewis, consumer consultant, presented ‘The Ripple Effect A consumer’s view of why we should embrace Outcome Measures’. This presentation was very powerful and had a really positive impact on participants including clinicians, consumers and carers. The presentation is available on the SA website www.health.sa.gov.au/mentalhealth/Default.aspx?tabid=99.
Articles
David Guthrie, Mishka McIntosh, Tom Callaly, Tom Trauer and Tim Coombs, Barwon Health: Community and Mental Health, Geelong, Victoria, Australia, Consumer attitudes towards the use of routine outcome measures in a public mental health service: A consumer-driven study, International Journal of Mental Health Nursing (2008) 17, 92–97.
Clinician
Quotes12
• “I like the consumer focus” (RN)
• “They are easy to use” (Indigenous Mental Health Worker)
• “It quantifies a lot” (Social Worker)
• “Gives information to feedback to the consumer” (Child and Youth Coordinator and Psychologist)
• “Reports and graphs are really good” (RN)
• “Good start, but needs refinement” (Psychologist)
• “Its all been said, so I can’t add too much more” (Remote Area RN)’
mHi and SDQ: Positive Feedback13
“Positive feedback is being received about the Adult (MHI) and CYMHS (SDQ) consumer self rated outcome measures. Some feedback from clinicians has indicated that initially they were sceptical; however, they are now finding that consumers can complete the measures, they want to fill them out and they value the opportunity to provide this information. In addition, clinicians have noted the measures provide more information than they have gathered in their assessments alone and at times it has challenged their initial case formulation. This supports the experience of Victorian clinicians who have shared similar experiences and accordingly value the information gathered through consumer self rated measures.”
12 Queensland Health, Outcomes Initiative Update 7
13 Queensland Health, Outcomes Initiative Update 9

Practice 47
Public mental health services are configured in three main service settings:
• acute inpatient
• ambulatory
• community residential.
The process of assessment, review, referral and discharge and the subsequent documentation of these processes are critical in providing a safe quality mental health service. In the unfortunate situation of adverse events or critical incidents, the quality of the care and the quality of the documentation is often called into question.
The recording of consumer outcomes follows an assessment by the clinician. Therefore the clinician ratings should confirm or correspond to the information contained in the consumer’s clinical file. There should be an entry in the clinical file to indicate if a consumer self-assessment has been offered and the result of that offering. Consumer outcomes information should be considered in all aspects of clinical practice and utilised, where appropriate.
If the clinician rated consumer outcomes are completed following an assessment and are making overt a clinician’s assessment, then it is important to explore the occurrence of missing items. Missing items might occur because an item has been skipped or because the rater has opted for a rating of 7, 8 or 9 (unable to rate ) on the clinician rated measures. Consider:
• What might it mean if, following an assessment, there are areas that are unknown or unable to be rated?
• What does it mean if there are subsequent 7, 8 or 9 on later collection occasions?
3. P
ract
ice

48 Practice
3.1 AssessmentNational Standards for mental Health Services Standard 11.3 – ASSESSmENt AND REViEW, Consumers and their carers receive a comprehensive, timely and accurate assessment and a regular review of progress.
11.3.5 The assessment process is comprehensive and, with the consumer’s informed consent, includes the consumer’s carers (including children), other service providers and other people nominated by the consumer.
11.3.6 The assessment is conducted using accepted methods and tools14.
National Practice Standards for the mental Health Workforce Standard 7: ASSESSmENt, tREAtmENt, RELAPSE PREVENtioN AND SuPPoRt Mental health professionals provide or ensure that consumers have access to a high standard of evidenced-based assessment, treatment, rehabilitation and support services which prevent relapse and promote recovery. They monitor the appropriateness and effectiveness of interventions15.
Assessment is a key function of mental health service delivery. Assessments and case formulations are routinely completed for consumers of public mental health services, they may be comprehensive or as a routine monitoring function. A range of complex information is available from multiple perspectives, and consumer outcomes present one way of making the information on the consumer journey readily accessible.
Assessments should be informed by all available information on a consumer including collateral information from key informants such as case manager and family members, history documented in both the inpatient and community files, and information available on the electronic databases. A review of the consumer’s inpatient file and access to community file is time intensive and limited by access and availability to medical records.
Documentation is essential for good mental health care and yet, there is considerable variability in the quality of assessments undertaken and their documentation. The clinician rated consumer outcomes provide a standardised process for overting the clinicians’ judgement following an assessment. Consumer outcomes provide a common language for clinicians, consumers, teams, organisations and also for jurisdictions.
National Standards for MentalHealth Servicesendorsed by the AHMAC National Mental Health
Working Group December 1996
National Practice Standards for theMental Health Workforce
National Practice Standards for the Mental Health W
orkforce
Endorsed by the AHMAC National Mental Health
Working Group September 2002
14 Australian Health Ministers Advisory Council (AMHAC) - National Mental Health Working Group, Information Strategy Committee, National Standards for Mental Health Services, December 1996
15 Australian Health Ministers Advisory Council (AMHAC) - National Mental Health Working Group, Information Strategy Committee, National Practice Standards for the Mental Health Workforce, September 2002

Practice 49
Assessments can occur for:
• new consumers who have never accessed public mental health services
• new consumers to a service who have been seen in another service
• existing consumers transferring to another program in your service
• existing consumers who have been treated in another setting (for example an ambulatory consumer who has been admitted and discharged from an acute inpatient unit and now returning to ambulatory care)
• known consumers who have been previously discharged.
Assessments require:
• obtaining information from key informants
• reviewing all available information
• assessment of the consumer.
Assessments will inform decisions regarding most appropriate actions such as:
• referral to external agency - no further assessment or specialist intervention required
• conducting a further assessment with possibility of brief interventions
• admission in an acute psychiatric inpatient unit, a community residential unit or into a community mental health service.
Example
How might consumer outcomes be used at entry into ambulatory setting following an assessment?
For new consumer:
• Are there group programs that could be accessed?
• Has referral to additional/external supports been undertaken?
• Has this consumer accessed a mental health program/initiative delivered through general practice? If so, are consumer outcomes available from this?
• How consumer outcomes inform the plan for immediate management of the consumer (i.e. why you managed the client as you did following assessment)?
• For intake/assessment teams, the ratings may help the decision regarding management of the consumer through a general practice program such as Mental Health Nurse Incentive Program or Better Access to Mental Health Care Initiative or another program in the community (referral plan).

50 Practice
For existing consumers:
• Is this consumer returning to ambulatory care following an admission and discharge from an acute inpatient unit? If so how does their presentation now compare with the presentation on previous returns to an ambulatory setting?
• Is the consumer prepared to complete a consumer self-assessment? Is this consistent with previous collections? What have they identified as issues?
• Would this consumer benefit from more intensive treatment?
• Would referral to community residential program (where they exist) be appropriate?
• Are there group programs that could be accessed?
• Has referral to additional/external supports been undertaken?
• The consumer outcomes might inform the needs assessment (which will inform the Care Plan).
How might consumer outcomes be used at admission to inpatient unit following an assessment?Consider the following:
• Has this consumer been admitted before? If so how does this presentation compare to the previous admissions? Are individual items, subscale or totals similar or different?
• Is this consumer an existing consumer of the mental health service? If so, what is their usual level of functioning and symptom severity? Have they previously completed a self-assessment measure? If so, what did they identify as issues?
• Is this consumer’s admission assessment consistent with “like” consumers? That is, how does this consumer’s HoNOS/HoNOSCA/HoNOS65+ compare with other consumers on admission to an inpatient unit?
• For both new and existing consumers:
– What do the measures suggest regarding the goals of the admission and the treatment needs/strategies during the admission (for instance, that might be targeted by psychosocial strategies, e.g., sleep, anxiety management, referrals to accommodation agencies etc)?
For new consumers:
• Would this consumer benefit from referral to ambulatory services (though this may be easier to determine on review in the inpatient setting)?
• Are there group programs that could be accessed?
• Has referral to additional/external supports been undertaken?
• Has this consumer accessed better mental health program or access to mental health nurse practitioners? If so, are consumer outcomes available from this?

Practice 51
For existing consumers:
• Is the level of community care sufficient?
• Would this consumer benefit from a more intensive level of support?
• Would referral to community residential program (where they exist) be appropriate?
• Are there group programs that could be accessed?
• Has referral to additional/external supports been undertaken?
Refer to: 3.3 Review

52 Practice
3.2 Care plansNational Standards for mental Health Services 10.6 Each consumer has an individual care plan within their individual clinical record which documents the consumer’s relevant history, assessment, investigations, diagnosis, treatment and support services required, other service providers, progress, follow-up details and outcomes16.
It is important to follow relevant local or jurisdiction documentation suites and care plan templates.
Care plans are another opportunity for consumers and carers (where appropriate) and clinicians to articulate goals and planned interventions. They should be developed in collaboration with consumers and carers and are particularly important where there are multiple clinicians or agencies involved as it provides a space to clarify respective roles and perspectives.
The completion of the clinician rated consumer outcomes are summaries of this assessment, making overt the clinicians judgement. Care plans are informed by assessments and dialogue between the consumer, clinician, carer and other relevant service. Consumer outcomes are a part of the assessment process.
In order to ensure the consumer perspective is included in the development or review of the care plan, it is important to provide sufficient notice and time for offering and completion of the self-assessment measure.
Generally speaking, there is considerable variation in care plans between consumers, clinicians, teams, services and jurisdictions. While responding to variability in consumer needs is important, the variation often occurs in relation to:
• the value and expectation of the plan
• quality of information included
• degree of collaboration with consumers in the completion and review
• frequency with which they are reviewed
• process for which they are developed, with some services requiring the plan to be:
– written with the consumer in the consumers language
– developed by the clinician with input after development by the consumer
– signed by the consumer with some requiring indication of whether the consumer (a) agrees, (b) were involved in its development and/or review or (c) just provided a clinician developed copy.
• process for which they are reviewed with some services requiring the plan to be reviewed by the:
– clinician
– treating doctor
– multidisciplinary team.
• inclusion and reference to other activities such as risk assessment and consumer outcomes.
National Standards for MentalHealth Servicesendorsed by the AHMAC National Mental Health
Working Group December 1996
16 Australian Health Ministers Advisory Council (AMHAC) - National Mental Health Working Group, Information Strategy Committee, National Standards for Mental Health Services, December 1996

Practice 53
Examples
Consumer identified areasThe consumer outcomes can also identify areas of strength for the consumer and it is important that these are also acknowledged. These areas of strength can then be drawn on when working towards goals.
While there is significant variation in the type of information in care plans (however named), ideally they should be largely informed by consumer-identified needs. For some consumers who are not actively involved in their treatment, or who are unwell, this may not be possible. This information could be informed by:
• consumer self-assessment ratings
• clinician ratings of consumer outcomes
• dialogue between the consumer and clinician.
It is unrealistic to expect that consumers and clinicians will have the same perspective. By virtue of their experience, knowledge, training and values they will have different explanations on attribution, expectations and outcomes as well as having different priorities and goals. Consumer outcomes are a unique opportunity for the consumer to rate how they think they are going. This process complements and enriches the clinician’s assessments and ratings.
Disagreement can be healthy and can form the basis for exploring differences in perspectives thereby providing opportunities for a genuine and effective therapeutic relationship.
inclusion of clinically significant items (rating of 2 or more on the HoNoS/HoNoSCA/HoNoS65+) The basic rule of thumb is that a rating of 2 or more on the HoNOS/HoNOSCA/HoNOS65+ is clinically significant and should at least be monitored. It is recommended that a rating of 2 or more should be included in the consumer’s treatment and management plan. Discussion of clinically significant items is one way to prioritise areas for consumer and clinicians for future interventions. This is a guide only and sometimes issues that are rated 0 or 1 might be included in a treatment plan and should be negotiated with the consumer and carer.
inclusion of carer perspective A process for negotiating the focus of the care plan and respectfully valuing all perspectives is vital. The capacity to elicit the carer’s perspective and to facilitate inclusion of this into the care plan will be dependent on the relationship between the clinician/consumer, clinician/carer (or parent), and the consumer/carer.

54 Practice
Child and adolescent/youth mental health services
The parent version of the Strengths and Difficulties Questionnaire (SDQ) makes it relatively easy to integrate carer perspectives. Inclusion in the care plan might consider:
• Areas of agreement and disagreement between youth and parent ratings.
• Areas of similarity or difference between the young person, parent and clinician between the self-rated and clinician rated measures.
Adult and older person mental health services
The absence of a carer measure in the consumer outcomes suite for adult and older person mental health services makes the routine inclusion of carers’ perspectives more difficult. This process might be complicated by consumer consent issues for the active participation of carers in treatment and planning. Depending on the therapeutic alliance between clinician and consumer and clinician and carer, it is possible to consider the following for inclusion in the care plan:
• What is the carer’s perspective on the clinician and consumer ratings? Are the identified areas of difficulty consistent with the carer’s perspective?
• What is the carer’s contribution to assisting the consumer manage their difficulties? If the carer support was not provided, would there be other areas of difficulty identified?
• What does the carer identify as priority areas? What role might they play in assisting the consumer to manage those areas?

Practice 55
3.3 Review National Standards for mental Health Services 11.3.14 The MHS ensures that the assessment is continually reviewed throughout the consumer’s contact with the service17.
Consumers accessing public mental health services present with complex needs and routine review of both the consumer’s presentation and the clinician’s interventions is critical to ensure concerted effort towards an end goal of enhanced quality of life for the consumer and their family.
In addition to the mandated requirements for review, such as mental health review boards/tribunals and multidisciplinary clinical reviews, a review might be undertaken when a consumer transfers to another team/program in your service, or because a consumer has requested a review.
Review of multiple consumer outcome collections can be a helpful way of tracking change for consumers who find it difficult to:
• Prioritise areas to focus on
• Identify change and improvement using the consumer outcomes to explore:
– What has changed and why?
– What has not changed?
– What interventions have been tried for clinically significant issues?
– What interventions might be tried?
– What other circumstances in the consumer’s life are contributing the measures increasing/decreasing/staying the same?
The clinician rated consumer outcomes are completed following an assessment by the clinician and the ratings should support clinical judgement. These ratings may negate areas of concern or justify a particular treatment decision.
A risk assessment or review should be informed by all available information including observation, information from key informants and previous histories/documentation and should also include the consumer’s perspective. The consumer self-assessment measure is one way of obtaining the consumers perspective.
National Standards for MentalHealth Servicesendorsed by the AHMAC National Mental Health
Working Group December 1996
17 Australian Health Ministers Advisory Council (AMHAC) - National Mental Health Working Group, Information Strategy Committee, National Standards for Mental Health Services, December 1996

56 Practice
Examples of reviews Consumer outcomes could be used in one of the following types of review:
• multidisciplinary
- clinical review
- transfers
• statutory body
- mental health review board/tribunal
- Office of Chief Psychiatrist)
• additional supports/external agencies
• group program
• clinical supervision
• review requested by the consumer.
multidisciplinary review Most consumers of public mental health services have complex needs and benefit from a multidisciplinary review of their presentation as well as an exploration of multi-faceted treatment and interventions. This type of review is usually undertaken through the clinical review processes. In addition to the routine multidisciplinary clinical review, on occasions consumers may be referred for discipline-specific assessment and treatment, for example to an occupational therapist for skills in daily living or a social worker for family therapy. The consumer outcomes can provide an overview of clinician and consumer perceived difficulties over time. The longitudinal capacity of the consumer outcomes can provide the evidence and can inform the referral request.
Clinical review
Most consumers of public mental health services have complex needs and benefit from a multidisciplinary review of their presentation as well as an exploration of multi-faceted treatment and interventions. This type of review is usually undertaken through the clinical review processes.
Clinical review or ward round processes vary considerably across services. Incorporation of the consumer outcomes provides a structure for dialogue about the consumer’s presentation and the clinician’s interventions. Incorporation into the clinical review will require preparation by the presenting clinician. Some teams will use data projectors and laptops during the review
National Standards for mental Health Services
11.3.17 All active consumers, whether voluntary or involuntary, are reviewed at least every three months. The review should be multidisciplinary, conducted with peers and more experienced colleagues and recorded in the individual clinical record 18.
National Standards for MentalHealth Servicesendorsed by the AHMAC National Mental Health
Working Group December 1996
18 Australian Health Ministers Advisory Council (AMHAC) - National Mental Health Working Group, Information Strategy Committee, National Standards for Mental Health Services, December 1996

Practice 57
to either complete measures live, to generate the graphs live while some other teams will print out the graphs and present these to the meetings. Both of these technologies can enhance the process, however use of consumer outcomes can occur successfully without either of these approaches when preparation is undertaken.
The National Outcomes and Casemix Collection (NOCC) Protocol provide a minimum requirement for collection. Scheduled clinical reviews may not be aligned with the NOCC 91-day collection requirement for consumer outcomes, this may be because a consumer has had an admission or discharge into an inpatient unit, or a discretionary review may have been completed. If this is the case there are two options to tie in the consumer outcomes with a scheduled clinical review, with number one being the recommended option:
1. Complete a discretionary review (also known as ad hoc review, review other) to tie in with the upcoming clinical review. If the consumer outcomes are going to be presented at the clinical review it is really important to offer the consumer self-assessment measure with sufficient time to allow a completed copy to be returned prior to a scheduled clinical review to ensure that all relevant measures are available for the review meeting. Also there needs to be sufficient time for the completed measures to be discussed with the consumer.
2. Use all existing collections in the review and collect at the next scheduled 91-day requirement. There could potentially be some issues with using the ratings in this way because it may mean that the relevance/currency of the ratings is limited. That is, a person’s presentation today might be markedly different from the ratings completed some weeks previously.
Examples for clinical reviews
Exploration of consumer perspective
Consumer participation in self-assessment can highlight issues related to therapeutic alliance, engagement in treatment/therapy, acceptance of illness as well as differentiating priorities in treatment goals between the consumer and clinician. Consider the following:
• What was the reaction of the consumer to completing a self-assessment measure?
• What was the extent of participation - discussion, partially completed or fully completed? Has this participation changed? For example, have they previously participated and now refusing or have they previously refused and now participating.
• What were the ratings and how do they relate to your perception of difficulty/distress?
• How did they respond to feedback on the consumer measure?
• How did they respond to feedback on the clinician measure?
• What is the consumers understanding of the clinical review process and how their consumer outcomes inform this?
For more information on offering the consumer self-assessment including considerations like literacy, cultural status and ways to promote completion:
Refer to: 2.2.1 Offering

58 Practice
Rate as a group
This activity is perhaps most useful in teams where there are more than one clinician involved in the consumers care. Rating as a group is an opportunity to share perspectives, developing an understanding and confidence of the measures and engaging collaborative information exchange, development of the use of a consistent terminology and language. Subsequently this technique can improve inter-rater reliability.
Rating as a group can be done:
• Prior to the clinical review enabling the team to work through points of difference considering all perspectives and sources of information. This enables discussion in the round or review to focus on actions and interventions.
• As part of the clinical review for consumers where there is significant difference of opinion and is a helpful way of gaining agreement for interventions.
Exploration of clinically significant items (rating of 2 or more on the HoNoS)
treatment/management Planning HoNoS/CA/65+ Clinical Prompt monitor?
Active treatment or management
plan?
Clin
ical
ly
sign
ifica
nt
4 severe/ very severe problem
most severe category for consumers with this problem. Warrants recording in clinical file, should be incorporated in care plan (nb, person can get worse)
yes yes
3 moderate problem
warrants recording in clinical file, should be incorporated in care plan
yes yes
2 mild problem
warrants recording in clinical notes, may or may not be incorporated in Care Plan
yes maybe
Not
cl
inic
ally
si
gnifi
cant 1 minor
problemrequires no formal action, may or may not be recorded in clinical file
maybe no
0 no problem problem not present no no
(Version modified by QUATRO VIC for staff training)
The basic rule of thumb is that a rating of 2 or more on the HoNOS/HoNOSCA/HoNOS65+ is clinically significant and should at least be monitored. It is recommended that a rating of 2 or more should be included in the consumer’s treatment and management plan. Discussion of clinically significant items is one way to prioritise areas for consumer and clinicians for future interventions. This is a guide only and sometimes issues that are rated 0 or 1 might be included in a treatment plan and should be negotiated with the consumer and carer.
There are other activities underway nationally to provide advice on what a junior clinician might do with a particular rating on the HoNOS suites.

Practice 59
Exploration of one measure at one point in time
Review of one measure at one point in time is limited, especially for the clinician measures as the clinician may not glean anything new if they have completed the rating. However, it does help to justify the management plan and perhaps any new goals established in the review as well as possibly being helpful to members of the clinical team not directly involved in the assessment. The consumer self-assessment measure can provide new information and a different perspective and can indicate areas of agreement and disagreement between the consumer and clinician. This process may alter team members’ perspectives.
For a new consumer, there will only be one collection occasion in which to review. Comparison of this individual collection with the clinical reference material may be beneficial. Is the rating for the consumer consistent with other similar consumers’ ratings? If not, are the ratings higher or lower and what might that mean for the proposed period of care.
Exploration of difference between consumer and clinician measures
It is unrealistic to expect that consumers and clinicians will have the same perspective. By virtue of their experience, knowledge, training and values they will have different explanations on attribution, expectations and outcomes as well as having different priorities and goals. Consumer outcomes are a unique opportunity for the consumer to rate how they think they are going. This process complements and enriches the clinician’s assessments and ratings.
Disagreement can be healthy and can form the basis for exploring differences in perspectives thereby providing opportunities for a genuine and effective therapeutic relationship.
For example a consumer who is on a community treatment order receiving mandated treatment who rates themselves as having absolutely no problems might be at risk of deteriorating if the order is removed and people become non-compliant with treatment, they may deteriorate, and risk relapse. Equally a consumer, who rates significant areas of distress but who the clinician rates low, might be at risk of re-presenting if being considered for discharge.
Exploration of ratings for consumers who are stable/unchanged
It is often easier to identify consumers who are obviously getting better or worse and to make recommendations on treatment interventions. However, the ability to identify small or incremental change is difficult without measurement tools. The routine use of measurement tools will not only allow identification of small or transient change they also identify those consumers who remain stable. A consumer who remains unchanged across multiple time points may warrant consideration of different treatment or therapies. If we anticipate that there is further improvement or gains to be made then we may be unlikely to continue with the same approach. Consumer outcomes may also provide a baseline for determining where the consumer has come from and how sustained has previous improvement been.
For this group of consumers, prioritise one or two clinically significant items that have remained stable where focused energy, treatment and interventions will be undertaken and where you would expect a change by the next review.
Again check the clinical reference material. Are there similar consumers who remain stable/unchanged?

60 Practice
Exploration of ratings for consumers considered for transfer or discharge
In addition to other clinical data/information the consumer outcomes provide longitudinal evidence of deterioration, lack of change or improvement which can be used to advocate for referral or acceptance into or out of specific programs. Transfer could occur to (a) replace the team/clinician currently engaged with the consumer or to (b) complement the therapies already provided.
Consider whether this consumer would benefit from referral and transfer to a:
• less intensive service (from crisis/mobile support to case management/continuing care)
• more intensive service (from case management/continuing care to mobile/crisis support)
• discipline specific therapist
• community residential service
• therapeutic or educational group program run by the mental health service
• external agency.
Consumer outcomes can support the decision to transfer or closure.
Consider whether this consumer is suitable for discharge from the mental health service. For some consumers there is anxiety in being discharged from a mental health service to community supports and general practitioner. The consumer outcomes can longitudinally represent change and improvement and consequently allay the consumer’s fears. As part of the discharge process and plan, it is useful for consumers and their families to include areas of previous difficulty and the strategies/treatment to manage or alleviate these areas.
Exploration of consumers over multiple collection occasions
File reviews are time intensive and limited by the quality of the information recorded. Perhaps the greatest benefit of consumer outcomes is the standardised format and routine requirement which allows easy comparison of assessments over time.
Comparison of one measure across multiple time points identifies areas of improvement or deterioration and provides evidence for continuing with a current treatment or therapy, or application of alternative or additional supports. It is possible to review measures by individual item, subscale or total score.
In reviewing the clinician rated measure over multiple time points:
• Is the number of clinically significant items increasing, stable or decreasing?
• Are the clinically significant items stable or different between collections?
• Are there changes/differences in the ratings consistent with areas of intervention and/or knowledge of other changes in the consumer’s circumstances (change may not be intervention related) and your expectations of change?

Practice 61
In reviewing the consumer rated measure over multiple time points, what does it mean if:
• Consumer has gone from refusal, to partially completing to fully completing? Or vice versa.
• Consumer rates the exact same way every time? For example rating all zeros.
• Consumer has been able to identify their areas of strength and difficulty that are increasingly consistent with others perspectives?
The consumer outcomes provide an opportunity to analyse factors and consumer profiles related to readmission and relapse. This can be done in one of three ways, ratings on admission, ratings on discharge or variation in ratings between admission and discharge.
Comparison of admission ratings
• Are the scores (total, subscale or item) similar on each admission, are they lower or higher?
• Is there a change in the types of issues/difficulties?
Comparison of discharge ratings
• Are the scores (total, subscale or item) similar on each discharge, are they lower or higher?
• Is there a change in the types of issues/difficulties?
Comparison between previous admissions and discharges – clinician rated measures
Is there:
• No change? It is rare for consumers to be admitted and discharged on the same score over multiple admissions.
• Increase? It appears that the consumer’s level of functioning and symptom severity is improving with each admission. That is in addition to the general/expected reduction from admission to discharge the change is greater for example total score ratings on admission and discharge (16-12, 16-10, 18-8).
• Stable? That is there is a consistent level of reduction in total score regardless of actual score. For example a consistent reduction of 5 (20-15, 18-13, 19-14, 16-11).
• Decrease? It appears that the consumer’s level of functioning and symptom severity is worsening and that while there continues to be an ’artificial’ change from admission to discharge the actual level of improvement on each admission is getting less. For example (20-15, 20-16, 21-16, 20-18).
• Identification of what needs to be addressed in subsequent care plans to address the pattern of relapse if a similar precipitant is identified for each admission (e.g., substance misuse, communication skills)?
Ratings over multiple time points (including the difference in perspective) can be used in case conferencing, referral to practitioner or other appropriate services (non-tertiary service) to convince consumer to have involvement of external agency.

62 Practice
using HoNoS to help plan for care and recovery
This framework was developed by Malcolm Stewart in New Zealand and can be used with any type of service that rates any of the HoNOS family of measures, whether they are child and adolescent services, working-age adults, or older adults. The tool proposes ways the HoNOS suite of measures can be used in planning care and recovery and is broken into three sections:
1. Are we the right service?
2. Check out the three Cs – Concordance, Change, Concerns
3. Choose the top priority.
There are a range of resources to support this process including both a ‘video’ and PowerPoint presentation about using this strategy, the ‘Quick-Guide’ posters that are given to individual trainees and put up on meeting room walls, and an ‘MDT Form’ to help people to think through a case and present it to their teams. These are all available free of charge and can be accessed via the internet. There is potential for this model to be adapted to include all the NOCC measures used in Australia.
For more information visit: www.tepou.co.nz/page/420-Information-Utility
Comparison with clinical reference material (e.g. AmHoCN DSt)
The clinical reference material provides an opportunity for clinicians, consumers and families to confirm if the consumer’s presentation is consistent with other similar consumers. That is, normative data compares an individual to the community in general whereas the consumer outcomes clinical reference material available on the AMHOCN web-based decision support tool compares a consumer with the population under public mental health care. This can be a normalising process for consumers and carers and can also be a point of reference for discussion if the ratings are lower or higher than for similar consumers.
To log onto the DST: http://wdst.mhnocc.org/
transfers For mental health clinicians the concept of continuity of care and consumer pathways poses some challenges for the implementation of the NOCC consumer outcomes at ‘transfer’ points within the same age grouping. Particularly in the area of transfer:
• between teams/programs in a service setting
• from one service setting to another service setting.
In addition to the national protocol there are likely to be local business rules for collections and reviews undertaken when a consumer transfers within a setting or across a setting.
Practice 63
Within settings (for example Ambulatory–Ambulatory)
A number of consumers access multiple services across a variety of service settings within the same mental health service though arrangements differ across jurisdictions. Some consumers will access:
• Multiple services concurrently for example, a case managed/continuing care consumer may during periods of crisis also access a brief intensive crisis/assertive home based treatment.
• While others will move from one to the other for example moving from a case managed/continuing care team to a longer term intensive treatment and rehabilitation team.
Where there is no change in setting such as a transfer within the ambulatory setting, consumer outcomes are not required.
However, the consumer outcomes provide longitudinal evidence of deterioration, lack of change or improvement which can be used to advocate for referral or acceptance into or out of specific programs. In addition to providing evidence for referral to a new or additional program, the consumer outcomes collection enables identification of outcomes as a result of interventions. That is while there is no change in setting and no requirement for consumer outcomes a team/program could complete a consumer outcome review other (also known in some jurisdictions as ad hoc review or discretionary review) at entry into the team/program and again on exit from the program.
Across settings (for example Ambulatory–inpatient)
Embedding the NOCC protocol into clinical practice has been particularly difficult for existing consumers who move between settings such as Ambulatory to Inpatient. The rationale for collecting at this point is simple; there has been considerable change in the consumer’s presentation to warrant an admission where treatment is intensive and more restrictive.
There are some challenges for mental health clinicians in this protocol requirement, such as:
• Continuity of care and ongoing involvement of the case manager/key worker. That is the consumer has not been ‘discharged’ and therefore the requirement to complete discharge consumer outcomes is perceived as inappropriate or meaningless.
• Admission (and possible discharge in the case of a brief crisis admission) may occur without the case manager/key worker knowledge.
Most services have developed local business rules to assist clinicians in meeting this requirement of the collection protocol.

64 Practice
Statutory body
mental health review board/tribunal
Mental health review boards/tribunals are usually established under the jurisdictional mental health legislation to conduct reviews of, and hear appeals by, psychiatric patients being treated involuntarily. Documentation processes and membership varies across jurisdictions.
To date the submission of consumer outcomes by clinicians to the Board, or the Board’s request for consumer outcomes information has been limited. Given that consumer outcomes can validate and confirm a clinician’s position, they may increasingly be supplied to the Board. Additionally, as Boards and consumers become more aware of the availability of this information the request for inclusion is likely to increase. It is important to note that some consumers might be reluctant to identify areas of difficulty on the consumer self-assessment if these are being presented to the mental health review board/tribunals or in other courts.
Consumer outcomes are of value when:
• The recommendations proposed by the treating team are validated by the clinician measures.
• The mental health board/tribunals use the consumer self-assessment in the context of requesting specific information on collaboration/consultation with the consumer to ascertain their views/wishes as well as consideration of the guardian/family member or primary carers wishes.
• Multiple assessments are synthesised and mapped over time.
For example a consumer who is on a community treatment order receiving mandated treatment who rates themselves as having absolutely no problems might be at risk of deteriorating if the order is removed. When consumers become non-compliant with treatment, they may deteriorate, and risk relapse. Equally a consumer, who rates significant areas of distress while the clinician rates low, might be at risk of re-presenting if discharged.
Chief psychiatrist offices
Chief psychiatrists are appointed in each jurisdiction (except Tasmania and Northern Territory) with responsibility under the relevant mental health legislation to monitor statutory practices. The roles vary but may include:
• Monitoring clinical standards of psychiatric practice and treatment provided by public mental health services.
• Responding to complaints from consumers, carers and others.
The Chief psychiatrist’s office could utilise consumer outcomes information to augment other clinical information provided or requested for consumers of mental health services.

Practice 65
Additional supports/external agencies As part of the routine review of consumer’s needs and opportunities, most consumers of public mental health services will require referral to additional supports and external agencies. Consumer outcomes can identify areas of difficulty and focus areas for intervention. Areas of difficulty often change and the consumer outcomes can provide a framework for identifying improvement which may not be immediately recognisable.
Group program Consumers often access specific therapeutic or education group programs offered by the mental health service. There is usually no change in setting for existing ambulatory consumers, so consumer outcomes are not automatically required. Previous collections of consumer outcomes provide longitudinal evidence of deterioration, lack of change or improvement which can be used to advocate for referral or acceptance into or out of group programs.
In addition to providing evidence for referral to a new or additional program, the consumer outcomes collection enables identification of change following specific interventions. That is, while there is no change in setting and no requirement for consumer outcomes, a group co-ordinator could complete a review other (also known in some jurisdictions as ad hoc review or discretionary review) at entry and again at exit from the group program.
Clinical supervision There are occasions when clinicians might benefit from a more comprehensive review of a particular consumer’s presentation, which could be explored in clinical supervision.
www.aasw.asn.au/adobe/publications/Practice%20Standards_Supervision.pdf
Refer to 3.5 Supervision
Review requested by the consumer Clinicians should encourage, support and facilitate a consumer requested review process.
The nationally available ‘Whose outcome is it anyway? Consumer Self-Assessment in Mental Health’ promotional materials state “It’s time to tell your side of the story. Everyone working together towards a better outcome for you”.19
It is reasonable for a consumer of public mental health services to request a formal review of their treatment and care by the:
• multidisciplinary clinical review
• mental health review board/tribunal
• Chief psychiatrist.
In addition to this a consumer may request a review and:
• revision of their individual care/service/recovery plan
• completion of their consumer outcomes.
Whoseoutcome is it anyway?
QUOTES:(From a workshop involving consumer and
carer consultants as part of the Western
QUATRO Project, September 2005)
“Consumer self assessment is seen as a
vehicle in the consumer’s journey. Used to
discuss goal setting, to assist in evaluating the
service being received and assess when to
move on.”
“What does being valued really look like and
how does it feel?”“Map of recovery; where we are, where we
want to get to.”“Triad - dialogue and relationship with consumer,
carer and case manager. Working together
to identify personal priorities of needs.” “By sharing and exploring the information it
will set up an expectation that the consumer’s
opinion is valued.”
WHERE CAN I GET MORE INFORMATION?
If you have any questions, concerns or would
like to get more information on consumer self
assessment or clinician measures, talk to:• Your mental health clinician• Consumer and/or carer consultants
• Family, friends or carers• Other consumers or consumer groups• Other carers or carer groups• www.mhnocc.org
LOCAL SERVICE INFORMATION
Consumer Self Assessment in Mental Health
19 Australian Mental Health Outcomes Classification Network, ‘Whose outcome is it anyway? Consumer Self Assessment in Mental Health’ brochure, 2006

66 Practice
3.4 Discharge Discharge planning begins at the point of assessment. The decision to discharge a consumer from a service should be a clinical decision and made following assessment (ideally face-to-face) and collateral from key informants including the consumer.
National outcomes and Casemix Collection (NoCC) discharge requirementsFor all clinician rated measures clinicians need to refer to the individual measure rating guidelines. In relation to the consumer self-assessment:
• Clinicians are also required to either offer or identify relevant temporary contraindication or exclusion criteria.
• Consumers can choose to complete the measure.
The collection requirements are articulated in the NOCC protocol:
National outcomes and Casemix Collection: technical Specification of State and territory reporting requirements for the outcomes and casemix components of ‘Agreed Data’ under National mental Health information Development Funding Agreements Department of Health and Ageing, Canberra, 2002
There are some practical difficulties in collecting the mandated discharge measures when an existing ambulatory consumer is admitted to an inpatient unit or disengages from follow-up. Even when a consumer who has disengaged is discharged:
- This decision is usually made on the basis of second or third hand information, for example communication with a GP, family member, partner etc.
- The clinician rated discharge measures can be completed on all available information.
- If a clinician is unable to make an informed estimate of the severity/difficulty of an item on the basis of all available information, there is capacity to select an unable to rate option for the HoNOS or LSP-16. Coding (for example rating of 7 or 9) of these items is dependant on data system and jurisdiction option. It is important to remember that missing items may effect calculation of subscale and total scores depending on data system.
The consumer outcomes can help alleviate the natural fear that exists around discharge. For example:
• For some consumers there is anxiety in being discharged from a mental health service to community supports and general practitioner and the consumer outcomes can longitudinally represent change and improvement and consequently allay the consumer’s fears.
• For some staff and family there is an anxiety in discharging a consumer from an acute inpatient unit. For some consumers there is a high level of difficulty and disability which is managed in the community continuously. For consumers who have multiple admissions, the outcomes can show that while the discharge rating is higher than the general population under care it is consistent for this consumer.
For more information on:
• offering the self-assessment go to Refer to: 2.2.1 Offering
• consumer self-assessment collection requirements Refer to: 2.2.1 Offering

Practice 67
National Standards for MentalHealth Servicesendorsed by the AHMAC National Mental Health
Working Group December 1996
3.5 Supervision National Standards for mental Health Services 9.20 The MHS ensures that staff have access to formal and informal supervision.
11.3.15 Staff of the MHS involved in providing assessment undergo specific training in assessment and receive supervision from a more experienced colleague20.
Most clinicians have access to professional/clinical, operational supervision or a combination of these to facilitate competent and independent practice. A number of guidelines have been developed by specific professions in the area of supervision. The distinction between the different types of supervision are not clear and more often then not the areas explored are interrelated and the supervision is more a combination of both professional and operational. Generally though:
• Professional supervision provides a platform for reviewing professional standards, therapeutic approaches and the dynamics in the relationship between the consumer and clinician. It is usually undertaken with a senior of the same discipline.
• Operational/line management supervision provides a platform for reviewing role responsibility, practice standards, HR requirements and professional development as well as caseload monitoring. It is usually undertaken by the team leader or program manager.
“Supervision is most effective when it is valued by both the supervisor and supervisee, when both parties are motivated and able to give it a high priority, and where there is recognition of the rights and needs of the supervisee as an adult learner”21.
Illustrated in the examples below clinical supervision incorporates both operational and professional components.
20 National Mental Health Working Group, National Standards for Mental Health Services, December 199621 National Practice Standards of the Australian Association of Social Workers: Supervision, page 1, July 2000

68 Practice
ExamplesConsumer outcomes could be used in supervision to:
• Identify profiles of consumers on case load by using tools, for example, consumer outcomes summary reports per consumer to assist in managing workload through understanding of intensity, complexity and interventions (e.g. consumer outcome collection history).
• Clarify and articulate the interventions/therapies being used for a particular consumer.
• Assess consumer outcomes - those that are improving (possible plans for discharge), those that are not improving (possible plans for referral or additional supports) as well as those who remain the same. It could also provide an opportunity to explore issues related to the offering of and engagement in meaningful dialogue on the consumer self-assessment measure.
• Discuss multidisciplinary perspectives on consumer’s presentation, interventions and outcomes.
• Identify alternative or complementary interventions/therapies for a particular consumer.
• Practice offering the consumer self-assessment (for example using the AMHOCN Clinical Utility Fidelity Checklist).
• Practice offering the consumer feedback on consumer outcomes (for example using the AMHOCN Clinical Utility Fidelity Checklist).
• Explore clinicians values and attitudes and their impact on therapeutic alliance.
• Explore clinicians values, beliefs and attitudes on consumer self-assessment process.
• Explore organisational values and attitudes and their impact on clinical practice.
• Identify training requirements and opportunities.
Suggested websites:
www.aasw.asn.au/adobe/publications/Practice%20Standards_Supervision.pdf

The commitment to consumer outcomes is articulated in the:
National mental Health Plan 2003 -2008 outcome 28: Comprehensive implementation and further development of routine consumer outcome measures in mental health
Key direction 28.1:
Continue to support and develop outcome measurement systems, including full implementation of routine outcome measurement systems, in the mental health sector and for use by other mental health providers and related service sectors.
Key direction 28.2:
Establish a national strategy in collaboration the Commonwealth, States and Territories for database development, data analysis (which may include normative comparisons and benchmarking exercises), dissemination and training.
Key direction 28.3:
Support the implementation of routine outcome measurement22.
4. S
uppo
rtin
g fu
ncti
ons
National Mental Health Plan 2003–2008Australian Health Ministers, July 2003
22 Australian Health Ministers, National Mental Health Plan 2003–2008. Canberra: Australian Government, 2003.
Supporting functions 69

70 Supporting functions
4.1 Documentation National Standards for mental Health Services 11.3.8 The assessment is recorded in an individualised clinical record in a timely and accurate manner23.
National Practice Standards Standard 10: DoCumENtAtioN AND iNFoRmAtioN SYStEmS Mental health professionals maintain a high standard of documentation and information systems on clinical interventions and service development, implementation and evaluation to ensure data collection meets clinical, monitoring and evaluation needs24.
The completion of consumer outcomes is fundamentally a clinical activity that supports decision making and enhances the planning, implementation and review of care plans.
Consumer outcomes are governed by the same legislation and considerations as other clinical activities; including privacy and confidentiality of medical records and personal information and freedom of information.
information system All states and territories require entry of the consumer outcomes into their electronic databases. Actual ratings for all the measures are required to be entered into state and territory databases. Offering of the consumer self-assessment is mandatory at certain collection occasions but voluntary for the consumer to complete. Therefore most electronic databases request the clinician to identify additional items for these measures, such as not offered (and why), offered and refused, offered and completed (entry of actual ratings).
Mental health clinicians are involved in consumer outcomes collection in both the completion of the clinician measures and offering the self-assessment. Consequently clinicians are responsible (regardless of whether they self-enter or delegate to another member of staff) for the accurate and timely entry of consumer outcomes ratings into electronic databases.
The completion and recording of consumer outcomes is a clinical activity, and in an adverse event or through the process of freedom of information, clinicians may be required to justify incomplete, inaccurate or inconsistent consumer outcome records.
There is variability across Australia as to whether administrative staff or clinicians enter the consumer outcomes ratings. It has been demonstrated that where clinicians are familiar with the data system and involved in both data entry and data extraction there is greater likelihood that the ratings will be complete, accurate and utilised.
National Practice Standards for theMental Health Workforce
National Practice Standards for the Mental Health W
orkforce
Endorsed by the AHMAC National Mental Health
Working Group September 2002
National Standards for MentalHealth Servicesendorsed by the AHMAC National Mental Health
Working Group December 1996
23 National Mental Health Working Group, National Standards for Mental Health Services, December 1996
24 National Mental Health Working Group, National Practice Standards for the Mental Health Workforce, September 2002

Supporting functions 71
If clinicians are not responsible for data entry, they need to ensure that the forms are:
• Complete - Do not leave clinician measure items empty as these forms are clinical documents and it is not appropriate for administrative staff to be making a judgement attributing a code for incomplete measures with missing items.
• Legible to ensure accurate data entry.
• Timely.
Hard copy file The recording of consumer outcomes follows an assessment by the clinician. Therefore the clinician ratings should confirm or correspond to the information contained in the consumer’s clinical file. There should be an entry in the clinical file to indicate when a consumer self-assessment has been offered and the outcome of that offering.
For most services the consumer’s clinical record will be a hard copy file but for services with electronic records this would be the area you write case notes.
When documenting the offering and/or completion, of the consumer self-assessment it is important to detail:
• When - date, and the time taken (if known). If it takes a long time to explain and assist the consumer complete their measure this might be an indication of the level of support required, the impact of their illness or possibly the consumer’s engagement with the service.
• What - the items that (a) indicate areas of concern identified by the consumer, (b) were left blank, and (c) areas that are different from corresponding areas rated by the clinician.
• Action - what you are going to do now? For example present to clinical review, review care plan and associated supports. It is really important that there are clear plans to follow up with consumers after their participation in the self-assessment process, regardless of whether the consumer refused, partially or fully completed.
Refer to: 2.2.2 Dialogue

72 Supporting functions
4.2 Policies/procedures Policies and procedures are valuable for further embedding activities into clinical and corporate practice. They provide platforms for sustainability and have links with accreditation.
ExamplesA number of services have developed specific policies and procedures for outcome measurement. Ideally consumer outcomes should be integrated into existing policies and procedures, such as case/clinical review, discharge planning, engagement of consumers etc.
In developing policies and procedures around consumer outcomes it is helpful to consider the following:
Performance measures Compliance with NOCC protocol
Protocol Are they clearly identified and defined?
Is there a link to existing documents and resources?
Local systems and it Who is responsible for electronic systems including entry of the ratings and extraction of reports?
What are the expectations for inclusion of consumer outcomes in individual consumer records?
What are the expectations that clinicians will provide consumers and their families with hard copy reports?
Application How the ratings are expected to be used? It is important to recognise and detail the range of opportunities for utilisation of consumer outcome ratings dependant on the collection occasion.
What are the expectations for feedback to consumers and their families?
Are we providing a holistic picture including information on the clinician and consumer measures?
Are we using the consumer outcomes to inform care planning?
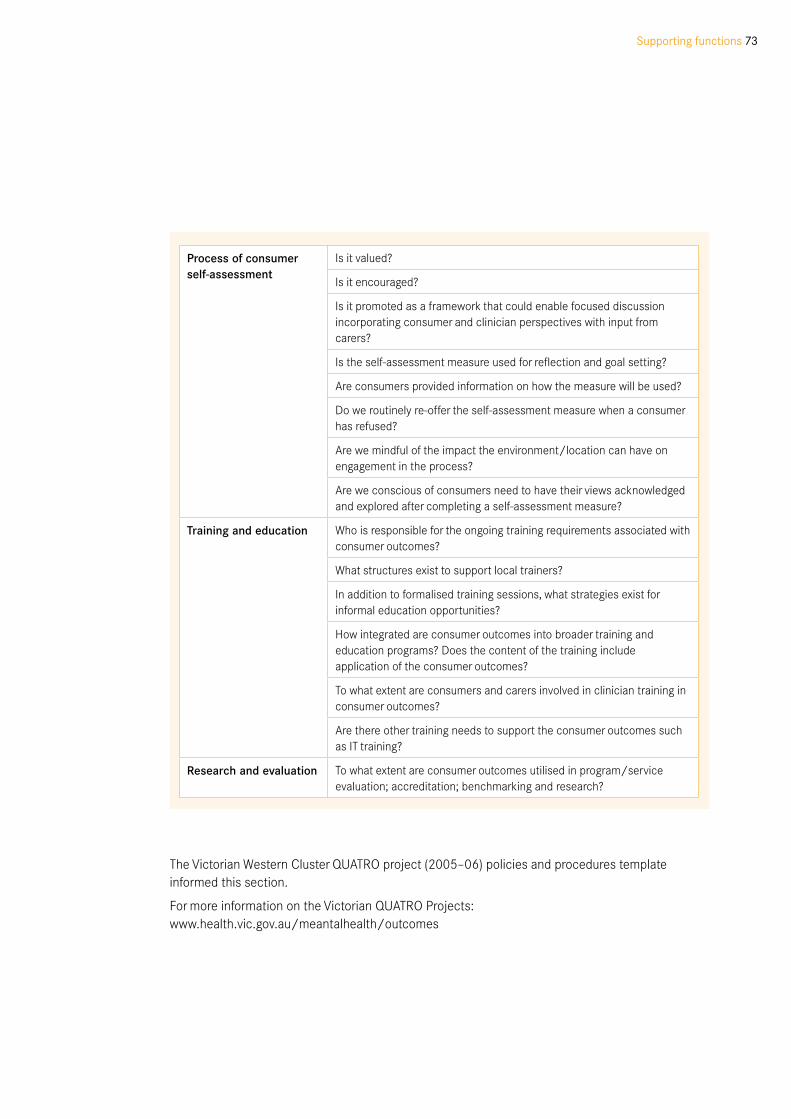
Supporting functions 73
The Victorian Western Cluster QUATRO project (2005–06) policies and procedures template informed this section.
For more information on the Victorian QUATRO Projects: www.health.vic.gov.au/meantalhealth/outcomes
Process of consumer self-assessment
Is it valued?
Is it encouraged?
Is it promoted as a framework that could enable focused discussion incorporating consumer and clinician perspectives with input from carers?
Is the self-assessment measure used for reflection and goal setting?
Are consumers provided information on how the measure will be used?
Do we routinely re-offer the self-assessment measure when a consumer has refused?
Are we mindful of the impact the environment/location can have on engagement in the process?
Are we conscious of consumers need to have their views acknowledged and explored after completing a self-assessment measure?
training and education Who is responsible for the ongoing training requirements associated with consumer outcomes?
What structures exist to support local trainers?
In addition to formalised training sessions, what strategies exist for informal education opportunities?
How integrated are consumer outcomes into broader training and education programs? Does the content of the training include application of the consumer outcomes?
To what extent are consumers and carers involved in clinician training in consumer outcomes?
Are there other training needs to support the consumer outcomes such as IT training?
Research and evaluation To what extent are consumer outcomes utilised in program/service evaluation; accreditation; benchmarking and research?

74 Supporting functions
4.3 tips and suggestions Desktop The simpler it is to find, the more likely it will be used. A great time saver for busy clinicians is to have the relevant consumer outcome links and documents available on their desktop. Suggested links include:
• local database/electronic record
• local reporting tool
• state or territory website - both intranet and internet. Frequently asked questions section and formal communications about the NOCC protocol should be book marked.
• state or territory aggregated reporting (for those with authorisation to access)
• national website - www.mhnocc.org
• national web-based decision support tool – http://wdst.mhnocc.org
Colour coding forms With consideration and recognition of local protocols and medical record standards, the more engaging and appealing the actual form is the more likely consumers are to complete it.
Because there are so many versions of the Strengths and Difficulties Questionnaire (SDQ) it is helpful to colour code the different versions.
For example all initial/entry versions could be on pink paper with follow up versions on blue paper. In addition to colour coding differentiating parents from youth versions could be done by placing a sticker on the youth versions.
Availability of consumer self-assessment forms Make sure forms are available and accessible by placing copies:
• in interview rooms or clinicians’ offices
• near the car keys, whiteboard, filing cupboards etc
• in staff meeting rooms
• in cars
• at reception desk/counter.
Hang a ’Whose outcome is it anyway? Consumer Self-assessment in Mental Health’ poster near the available copies.
Stapling brochures or information sheets for consumers and carers to the self-assessment form is another way to ensure clinicians have ready access to all the materials required by consumers and carers.
Whoseoutcome is it anyway?
QUOTES:(From a workshop involving consumer and
carer consultants as part of the Western
QUATRO Project, September 2005)
“Consumer self assessment is seen as a
vehicle in the consumer’s journey. Used to
discuss goal setting, to assist in evaluating the
service being received and assess when to
move on.”
“What does being valued really look like and
how does it feel?”“Map of recovery; where we are, where we
want to get to.”“Triad - dialogue and relationship with consumer,
carer and case manager. Working together
to identify personal priorities of needs.” “By sharing and exploring the information it
will set up an expectation that the consumer’s
opinion is valued.”
WHERE CAN I GET MORE INFORMATION?
If you have any questions, concerns or would
like to get more information on consumer self
assessment or clinician measures, talk to:• Your mental health clinician• Consumer and/or carer consultants
• Family, friends or carers• Other consumers or consumer groups• Other carers or carer groups• www.mhnocc.org
LOCAL SERVICE INFORMATION
Consumer Self Assessment in Mental Health

Supporting functions 75
information packsMental health services commonly compile packs with information about available services, consumer and carer rights and responsibilities and complaints processes. If these packs already exist it is really important to ensure that information on consumer outcomes is included. Consumer outcomes are routinely required in mental health services not an add-on or something special. Therefore it is a good idea to include consumer outcomes in general packs rather than making specific packs for consumer outcomes. If these packs don’t currently exist rather than creating one just for consumer outcomes, create a general pack including consumer outcome information.
Consumer and carer consultants like other mental health staff have an important role in making information packs available to consumers and carers of the service.

76 Supporting functions
4.4 Service quality
National Practice Standards for the mental HealthWorkforce Standard 9: SERViCE PLANNiNG, DEVELoPmENt AND mANAGEmENt
Mental health professionals develop and acquire skills to enable them to participate in the planning, development, implementation, evaluation and management of mental health services to ensure the delivery of coordinated, continuous and integrated care within the broad range of mainstream health and social services.
Standard 11: EVALuAtioN AND RESEARCH
Mental health professionals systematically monitor and evaluate their clinical practice, consistent with the National Standards for Mental Health Services and relevant professional standards to ensure the best possible outcomes for consumers, family members and/or carers. Where possible, they participate in or conduct research, to promote quality practice and seek funded educational opportunities to become conversant with current research25.
“…without information debates are simply matters of difference of opinion - the NOCC data provide a common communication tool and the beginnings of evidence based dialogue...”26
The Commonwealth Department of Health and Ageing has provided funding to states and territories since 2005 through the Commonwealth Own Purpose Outlay (COPO) Quality Through Outcomes (QTO). This funding has provided opportunities for concerted efforts on utilisation of consumer outcomes at the individual level for clinical decision making.
Before we can begin to use this information for quality improvement processes we had to establish the collection. As compliance increases and the data quality improves the consumer outcomes present a range of potential service quality applications that warrant further exploration.
Some examples include using consumer outcomes data for resource allocation, and for developing specialist clinical interventions to address identified consumer/carer need. Other ideas include areas for research, such as changes in consumer outcomes in relation to the clinical interventions provided.
National mental Health Performance FrameworkUnder the National Mental Health Strategy, states and territories have committed to the development of a national framework to monitor the performance of public mental health services. The National Mental Health Performance Subcommittee has been established to facilitate the implementation and development of performance measurement and benchmarking in Australia. For more information visit: www.mhnocc.org/Benchmarking.
National Practice Standards for theMental Health Workforce
National Practice Standards for the Mental Health W
orkforce
Endorsed by the AHMAC National Mental Health
Working Group September 2002
25 National Mental Health Working Group, National Practice Standards for the Mental Health Workforce, September 2002
26 AMHOCN, PowerPoint Presentation, December 2006

Supporting functions 77
Key Performance Indicators (KPI) should report variability, with recognition of the ceiling effect (can’t get better) and the floor effect (can’t get worse). Meaningfulness and simplicity are key features of adopted key performance indicators. Developing indicators is a complex undertaking and the selection criteria for KPI are:
• sensitive to change
• meaningful
• simple to use
• casemix adjustable
• statistically robust.
Currently national KPI includes consumer outcomes in the capability domain as ‘outcome readiness’. That is, there are services capable of routinely collecting consumer outcome measures. Collection or compliance has been steadily improving though not all services maintain the 85% compliance target. Work continues federally for adoption of consumer outcomes KPI in responsiveness (consumer self-assessment), and effectiveness domains (HoNOS suites).
In addition to the nationally developed KPI suite, states and territories have made significant investments in developing and implementing service level KPI. Funding permitting this developmental area will continue to evolve.
Suggested reading:
NMHWG Information Strategy Committee Performance Indicator Drafting Group (2005), Key Performance Indicators for Australian Public Mental Health Services, ISC Discussion Paper No.6 Australian Government, Department of Health and Ageing, Canberra
Consumer outcome reporting capabilityOnce the consumer outcomes measures are completed and entered into the electronic database that information is captured in each of the following levels of reports:
• consumer level reports generated locally for use at the consumer, clinician or team/program level
• aggregate level de-identified consumer data generated by jurisdiction for jurisdiction organisations
• aggregate level de-identified consumer data generated by AMHOCN from jurisdiction submitted data. This data is presented in the following formats:
– Adherence to the Requirements of the Data Collection Protocols for the National Outcomes and Casemix Collection (NOCC) provided by AMHOCN to each state and territory. www.mhnocc.org/amhocn/Reports/
– The ‘Decision Support Tool’ (DST) enables users to compare profiles of their consumers against the national aggregate and was originally available as an Access download from the website. Enhancements were made to this and it is now available as a web-based tool http://wdst.mhnocc.org/. All NOCC measures (except Focus of Care in Adult and Older Person) are available. The benefit of DST with the potential for inclusion of clinical prompts would be an opportunity to standardise practice, to prompt clinicians to clinical reference material and practice guidelines. The tool is accessible to everyone so it is important how information is presented. It might be good for consumers to see where they sit relative to others.
Key Performance Indicators for Australian PublicMental Health Services
IS
CD
PN .5
R E P O RT O F P E R F O R M A N C E I N D I C ATO R D R A F T I N G G RO U PI N F O R M AT I O N S T R AT E G Y C O M M I T T E E
A H M A C N AT I O N A L M E N TA L H E A LT H W O R K I N G G RO U P
effectiveappropriate
efficientresponsiveaccessible
safecontinuous
capablesustainable

78 Supporting functions
There is considerable variation in what is available locally and at the jurisdiction level with some variations in things such reporting parameters and immediacy of the reporting capacity. An overall reporting framework was developed to provide “a conceptual basis for the reporting of analyses of the Mental Health National Outcomes and Casemix Collection (NOCC) Data Sets. It is prepared specifically for those information users who intend to develop and analyse reports from NOCC data collected locally (be it at the jurisdictional or organisational level). The Reporting Framework details the key underlying assumptions used in the development on the National standard reports to date. As such, it is an ‘evolving’ document. As further analyses and reporting is undertaken with the national data, it can be anticipated that there will be refinement to the underlying assumptions. These refinements will be documented in each release of Standard Reports as well as in subsequent versions of the Reporting Framework.”27
Example consumer outcomes in service quality
incorporation• To what extent are consumer outcomes utilised in program/service evaluation; accreditation;
benchmarking and research?
• Have consumer outcomes been considered for inclusion in risk adjustment for KPI?
Compliance‘Compliance with the National Outcomes and Casemix Collection (NOCC) protocol may identify process issues. Consider the following:
• Is there clarity about who is responsible for ensuring consumer outcomes ratings are entered on electronic databases?
• Are there compliance issues within a team/program?
– If so, are they limited to a specific collection occasion?
– What activities might be required to redress this?
• Are there compliance variations between similar teams/programs?
– If so, what is this attributed to?
27 www.mhnocc.org

Supporting functions 79
use of ratingsConsumer outcome measure ratings provide another source of clinical information with the added advantage of being aggregated and reported. Consider the following:
Confirmation or difference in clinical information
• Are the consumer outcomes rating scores confirmed by documentation in clinical file?
• Is there evidence in the clinical file that a consumer self-assessment was offered and/or discussed?
• Are those consumer self-assessment not offered due to acuity consistent with what would be expected in the ratings on the clinician measures?
• Is there evidence in the care plan that the outcome measures have been used to identify areas of need/strength or have they been related to goal setting in some way?
trends
• What is the incidence of incomplete clinician rated measures (rating 7, 8 or 9)?
– What is the incidence of incomplete clinician rated consumer outcomes on subsequent collection occasions?
– If the clinician measures summarise the clinicians assessment, what activities are being considered to improve the clinicians capacity to cover each area in their assessment to enable them to rate each item?
• What is the incidence of ratings of zero or one on the clinician rated measures?
– Is this consistent with consumer profile for that team/program?
– If not, what activities might be undertaken to redress this?
• What is the percentage of clinically significant items for HoNOS suites?
– What might this say about consumers accessing a particular team/program?
– Is this stable, increasing or decreasing?
– What additional supports/programs might be required to address the identified areas of difficulty?
– What support or training might be required for staff on a particular team/program that has a high number of consumers presenting with a particular subset of difficulties?

80 Supporting functions
ExpectationsRoutine outcome measurement (consumer outcomes) was introduced in Australian clinical mental health services in 2003 as a key strategy of the national agenda to strengthen evidence based culture and practice. As collection of outcome measures is mandatory in all public (and private hospital) mental health services (with nationally agreed exceptions), ongoing training for clinical staff in accurately completing and using the measures is essential. Implementation of routine consumer outcomes is also reliant on effective leadership at all levels and building the capacity of information technology systems to produce meaningful reports. Increasing the knowledge and confidence in consumer outcomes among consumer and carer consultants will enhance collaborative practice and service improvement initiatives.
Action to consolidate systems for workforce development, consumer and carer involvement, improved reporting capability, and providing effective leadership have been developing in or across states and territories through Quality Through Outcomes funded activities and initiatives. Consequently a range of resources have been developed to support consumer outcomes. Establishment of sustainable and enduring systems for training will be a vital step for consolidation of a workforce capable of collecting and meaningfully using consumer outcomes in the future.
As an example, the Victorian Department of Human Services, Draft Victorian Outcome Measurement Training Framework has been incorporated into the following sections detailing the competencies, minimum requirements and timeframe for the five types of training:
• orientation• managers/leaders• clinicians • consumer and carer consultants (or their equivalents)• trainers.
Linking to key policies and strategies• The routine measurement of clinical outcomes is an initiative under the
National Mental Health Strategy that was introduced across all clinical public mental health services in Australia in 2003-2004 and is now part of the third National Mental Health Plan 2003-2008.
• Key Performance Indicators for Australian Public Mental Health Services (2005) report proposes a set of key performance indicators for use in Australia’s public sector mental health services that is based on the National Health Performance Framework and linked to the strategic directions of the National Mental Health Plan 2003-2008.
• The measurement of consumer outcomes in mental health is compatible with the emphasis placed on high quality health services, consumer and carer participation and improving outcomes articulated in jurisdictional plans.
Roles and responsibilitiesThe roles and responsibilities related to training and workforce development should be articulated for each of the following key stakeholders:
• Australian Mental Health Outcomes and Casemix Network (AMHOCN)
• jurisdictional departments
5. W
orkf
orce
dev
elop
men
t
Key Performance Indicators for Australian PublicMental Health Services
I N F O R M A T I O N S T R A T E G Y C O M M I T T E ED I S C U S S I O N P A P E R N O .5
R E P O RT O F P E R F O R M A N C E I N D I C ATO R D R A F T I N G G RO U PI N F O R M AT I O N S T R AT E G Y C O M M I T T E E
A H M A C N AT I O N A L M E N TA L H E A LT H W O R K I N G G RO U P
effectiveappropriate
efficientresponsiveaccessible
safecontinuous
capablesustainable
National Mental Health Plan 2003–2008Australian Health Ministers, July 2003
Workforce development 81

82 Workforce development
• funded consumer outcome positions/programs
• mental health services
• funded training, education and workforce development programs
• trainers – funded and portfolio holders
• consumer and carer consultants (or their equivalents)
• participants of consumer outcomes training.
In addition to formalised training sessions the full potential for consumer outcomes in clinical practice and in ensuring data integrity will require a commitment by mental health clinicians and services to the development of ‘learning environments’ where consumer outcomes are routinely used and applications are further developed. Examples of these would include clinical review meetings, clinical/operational supervision, peer mentoring etc. There is also a role for other development activities such as annual Australasian Mental Health Outcomes Conference, statewide forums and research activities. For more information visit: http://amhoc2008.com.au
training deliveryInitial materials were developed in 2002. The Australian Mental Health Outcomes and Casemix Classification Network (AMHOCN) developed and distributed basic training materials in 2005 and clinical utility materials in 2006.
In the absence of a nationally articulated outcome measurement framework, the following competency areas, minimum requirements and recommendation duration were taken from a Draft Victorian Outcome Measurement Training Framework.
The Australian Mental Health Outcomes and Casemix Classification Network (AMHOCN) have carriage for NOCC training accreditation. A national training framework, including NOCC rater certification and trainer accreditation and e-learning for NOCC, will in part be developed through AMHOC 2008 pre-conference workshop November 2008. Following this workshop a discussion paper will be developed and contribution sought from the mental health sector.
Each state and territory has developed and implemented different training models. Despite this difference there is a shared recognition that training is required at different levels dependent on target audience. Generally there are three tiers of training requirements from orientation, basic or rater training and utility. Experience suggests that inclusion of clinical utility training with the rater training is beneficial. In addition to the types or tiers of training required it has also been identified that training needs differ dependent on the target audience with three key groups identified, managers/leaders, mental health clinicians as well as consumer and carer consultants.
Bearing in mind the specific training requirements and models utilised in each state and territory the following proposed training components are included in an attempt to differentiate between the training requirements as a guide only.
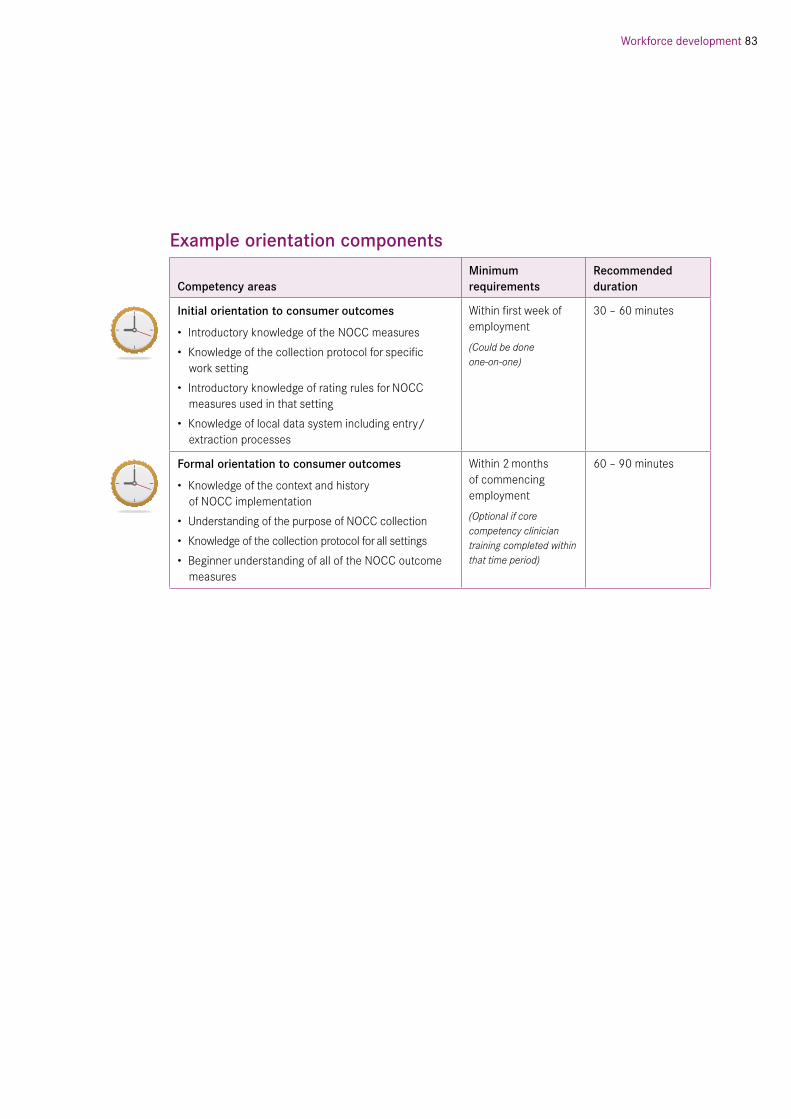
Workforce development 83
Example orientation components
Competency areas minimum requirements
Recommended duration
initial orientation to consumer outcomes
• Introductory knowledge of the NOCC measures
• Knowledge of the collection protocol for specific work setting
• Introductory knowledge of rating rules for NOCC measures used in that setting
• Knowledge of local data system including entry/extraction processes
Within first week of employment
(Could be done one-on-one)
30 – 60 minutes
Formal orientation to consumer outcomes
• Knowledge of the context and history of NOCC implementation
• Understanding of the purpose of NOCC collection
• Knowledge of the collection protocol for all settings
• Beginner understanding of all of the NOCC outcome measures
Within 2 months of commencing employment
(Optional if core competency clinician training completed within that time period)
60 – 90 minutes

84 Workforce development
5.1 managers Example managers/leaders training componentsThis training is designed for staff employed in leadership/supervisory/management roles involved in the use but not the completion of the measures.
Competency areas minimum requirements
Recommended duration
opportunity to workshop possibilities for mental health information
• Develop mental health information literacy
• Explore role and possibilities of supporting functions for developing and using mental health information
• Developing a culture of enquiry and developing an understanding of how to sustain quality mental health information collection and utilisation
• Skill development to analyse aggregate data to see if changes/improvements to system are happening
• Explore strategies for motivating staff to value the collection and use mental health information
Within first month
2 hour blocks or a half day
overview of consumer outcomes – collection and utility
• Knowledge of the context, history and purpose of NOCC
• Knowledge of items that each of the measures cover
• Awareness of the challenges and opportunities for the consumer self-assessment process
• Detailed knowledge of the collection protocol
• Understanding and interpreting individual consumer reports
• Overview of how consumer outcomes can be utilised in clinical practice including clinical decision making (reviews/care plans), also with consumers and carers
• Knowledge of available aggregate data
In addition to this session manager should attend a clinical review to observe use of consumer data in clinical decision making.
Within first month
(Not required if clinical core competency basic and advanced have been completed)

Workforce development 85
Competency areas minimum requirements
Recommended duration
Consumer outcome data informing service quality
Skill development to enable interpretation and application of aggregated consumer outcome data presented at the:
• Team or service level to better manage teams/services
• Team or service level to inform service planning
• Jurisdiction and national level to understand individual consumers (DST), trends and service profiles.
• Awareness of how the team/unit/service “looks” according to what they have collected such as service/team profile, complexity of cases, clinical significance, outcomes demonstrated etc. (where these reports exist)
While primarily delivered to mangers and team leaders this session would be useful for all mental health staff involved in using consumer outcome aggregate data.
90 – 120 minutes

86 Workforce development
5.2 Clinicians Mental health clinicians have considerable skills, knowledge and expertise having undertaken discipline specific undergraduate degrees and for some postgraduate qualifications. Professional development opportunities and access to supervision varies considerably across mental health services.
Participation in the consumer outcomes initiative affects nearly all aspects of clinical service delivery and most clinicians will have areas where their skills and knowledge excel and also areas that require further skill development.
Child and adolescent mental health clinicians require specific training in CAMHS consumer outcomes while adult and older person measures can be trained either in combination or separately.
Consumer and carer involvement in consumer outcomes training for clinicians is a powerful way of promoting:
• The value of collecting and using measurement tools.
• That clinician rated and self-rated measures provide opportunities to elicit multiple perspectives.
• Measurement tools can assist in prioritising and negotiating goals.
Utilisation of existing programs/training strategies would provide an avenue for sustainable consumer outcome training, such as:
• Identification and integration of consumer outcome training into broader discipline based activities, for example graduate nurse programs and psychiatric registrar rotations, would ensure that consumer outcomes are understood and integrated as a mandatory clinical activity.
• Mental health training providers.
• Universities, particularly postgraduate degrees.
Generic skill requirements Ongoing skill development in the following areas will enable active participation in consumer outcomes:
• knowledge and understanding of consumer outcomes - rationale, how to rate the measures and use of consumer outcomes ratings
• ability to interpret consumer ratings and engage in dialogue with consumer
• ability to offer the self-assessment including a rationale, instilling value in the process and ensuring time to explore issues/fears
• understanding clinical information systems
• ability to provide support and possibly assistance to consumers in the completion of the self-assessment
• ability to facilitate meaningful dialogue on consumer outcomes with consumers and carers
• skills in clinical review preparation, presentation and documentation
• skills in incorporating consumer outcomes into care planning.

Workforce development 87
Example
Rate an existing consumer as a group This activity is perhaps more useful in teams where there are more than one clinician involved in the consumer care. Rating as a group is an opportunity to share perspectives, developing an understanding, and confidence of the measures and engaging collaborative information exchange, development of the use of a consistent terminology and language. Subsequently this technique can improve inter-rater reliability.
All services hold regular staff meetings that discuss clinical issues, business information (service changes, new policies/procedures etc) and provide a space for staff development (external and internal presentations). Some services have embedded consumer outcomes into these meetings in the staff development component. For example one staff member leads the discussion by utilising one of the examples from this resource:
• case-manager describing how they introduced and talked about consumer outcomes with a consumer.
• Consultant psychiatrist presenting information about discrepancies between clinical perception (HoNOS and LSP-16 ratings) and consumer perception (for example, BASIS-32® ratings) for discussion by all staff.

88 Workforce development
Example clinician training components
Competency areas minimum requirements
Recommended duration
Rater training
• Knowledge of the context, history and purpose of NOCC
• Detailed knowledge of the collection protocol
• Knowledge of the rating rules for clinician rated consumer outcome measures
• Skills in completing HoNOS suites through practice ratings of clinical vignettes
• Knowledge of suite of NOCC measures
• Awareness of the challenges and opportunities for the consumer self-assessment process
• Skills in offering consumer self-assessments
• Beginner understanding of consumer level reports
• Awareness of possibility for consumer outcomes in clinical practice
Refresher training - rater
For clinicians who have already had previous training in NOCC measures and some experience in collection:
• Enhanced skills in effective/accurate rating.
• Improved inter-rater reliability.
• Enhanced experience/skill in use of measures at clinical level.
• Enhanced understanding of information use and need to collect quality information.
Other strategies to enhance inter-rater reliability include:
a) Refresher training sessions – including rating new clinical vignettes, revision of rating rules.
b) Discussion of ratings in clinical review meetings.
c) Team rating a known consumer and comparing ratings.
d) Rating training vignettes individually or as a team.
All mental health clinicians should complete this training within 2 months of commencement of employment within a mental health service (or when a change in age setting occurs).
a) & d) Annually
b) & c) Regularly
Half day
a) 120 minutes
b) 5-10 minutes
c) 15 -20 minutes
d) 10 minutes

Workforce development 89
Competency areas minimum requirements
Recommended duration
Advanced clinical training:
• Understanding and interpreting individual consumer reports.
• Skills in discussing consumer outcomes with consumers and carers.
• Knowledge of, and skills in, utilising consumer outcomes in clinical practice (e.g. care plans, clinical review, discharge planning).
• Skills in accessing and interpreting clinical reference material (e.g. compare individual consumer scores with clinical reference material available nationally on DST).
• Knowledge of, and skills in, utilising consumer outcomes in service planning and evaluation.
• Awareness of how the team/unit/service “looks” according to what they have collected such as service/team profile, complexity of cases, clinical significance, outcomes demonstrated etc (where access to these types of reports is possible).
All mental health clinicians should complete this training within 2 months of commencement of employment in a mental health service (or when a change in age setting occurs).
Half day
Using consumer outcomes should be explored regularly in routine meetings.

90 Workforce development
5.3 Consumer and carer consultants (or equivalent)Consumer and carer consultants as discussed here refer to roles employed by mental health services.
Consumer and carer consultant/advisor roles vary across states and territories but it is suffice to say that these roles are fundamentally designed to support and assist in improving outcomes for people receiving mental health services. While consumer and carers bring a wealth of personal experience and knowledge to these roles, they also require opportunities for professional development and training. Currently, skill building for consumer and carer consultants has not been prioritised.
Consumer and carer consultants or advisors have the potential to play a pivotal role in consumer outcomes providing that they are:
• Not expected to be the primary engager of consumers and carers in consumer outcomes, this is a service wide responsibility with clinicians taking the primary role.
• Provided with key materials and resources related to consumer outcomes.
• Provided opportunities to develop skills to interpret consumer outcome information to use it for service quality.
• Offered professional development opportunities to enhance general skills as well as focused sessions on consumer outcomes including creative ways for managing resistance.

Workforce development 91
Example consumer and carer consultant training components
Competency areas minimum requirements
Recommended duration
opportunity to workshop possibilities for mental health information:
• Introduction to mental health information development.
• Clarify role opportunities in developing and using mental health information.
• Identification of opportunities to utilise aggregate data, including what is available.
• Explore strategies for ensuring a focus on the consumer perspective remains on the consumer outcome agenda.
• Skill development to analyse aggregate data to see if changes/improvements to system are happening.
Within 3 months
2hour blocks or a half dayoverview of consumer outcomes – collection and utility:
• Knowledge of the context, history and purpose of NOCC.
• Knowledge of items that each of the measures cover.
• Awareness of the challenges and opportunities for the consumer self-assessment process.
• An awareness of the collection protocol.
• Overview of how consumer outcomes can be utilised in clinical practice including clinical decision making (reviews/care plans), also with consumers and carers.
• An overview on how consumer outcomes can be used with consumers and carers.
Within 6 months
Co-facilitators/trainers (consumer and carer consultants):
• Knowledge and skills in training.
• Awareness of data collection and reporting systems.
• Knowledge of the challenges and opportunities for the consumer self-assessment process.
• Working knowledge and use of training materials and other resources (e.g. Decision Support Tool).
• Knowledge of common areas of misunderstanding/errors with consumer outcome collection and their resolution.
• Skills in responding to frequently asked questions.
• Confidence and support to challenge participants assumptions regarding the consumer self-assessment process.
• Has a recognised role in consumer outcomes training
• Completed all relevant consumer outcomes training
• Values:
- information development, collection and use
- consumer and carer perspectives, participation and consumer self-assessment process
Half day

92 Workforce development
5.4 trainers There is considerable variation across jurisdictions regarding the appointment, capacity (formalised training role), qualifications (Cert IV in workplace assessment and training etc) and requirements for trainers in consumer outcomes. Jurisdictions have also implemented quite different training programs including:
• train-the-trainer model
• small pool of appointed staff
• accredited trainers.
The provision of training in a number of jurisdictions is undertaken by trainers as an add-on to their primary role. The sustainability for training and trainer requirements continues to be an area for development.
There have been a number of identified benefits from involving consumers and carer consultants in training clinicians in consumer outcomes:
• positive response from clinicians
• felt their involvement made a difference
• more confident about being involved in training
• raised profile within service.
Example trainers training components
Competency areas minimum requirements Recommended duration
trainers (clinicians) providing clinical core competency – rater/advanced training:
• Knowledge and skills in training.
• Knowledge in data collection and reporting systems and capacity to translate knowledge to participants.
• Awareness of the challenges and opportunities for the consumer self-assessment process.
• Working knowledge and use of training materials and other resources (e.g. Decision Support Tool).
• Knowledge of common areas of misunderstanding/errors with consumer outcome collection and their resolution.
• Skills in responding to frequently asked questions.
• Skills in challenging participants assumptions regarding the consumer self-assessment process.
• Has a recognised role in consumer outcomes training.
• Generic skills as a trainer.
• Values information development, collection and use.
• Values consumer and carer perspectives, participation and consumer self-assessment process.
• Completed consumer outcome rater and advanced training.
• Experience in using consumer outcomes in clinical practice.
Half day

6. R
esou
rces
A number of resources have been suggested or referenced throughout this resource.
This section refers to those resources specifically designed for the National Outcomes and Casemix Collection (NOCC).
Considerable energy has gone into the development of resources and information primarily for clinicians. This has involved the development of:
• websites and webpages
• protocol documents, including - technical specifications
• training materials - national through AMHOCN, at a jurisdiction and local level. Training materials including rater and clinical utility
• information sheets and brochures
• frequently asked questions webpages and forum.
The emphasis on mental health information is going to increase not fade away and it has been suggested that to sustain the momentum for consumer outcomes going forward will require two types of resources:
• people who are informed, skilled and provide leadership in both the collection and utilisation of mental health information.
• materials for each target audience - consumers, carers, mental health clinicians, managers/team leaders, trainers, and resource people pitched at relevant levels.
Resources 93

94 Resources
6.1 People Mental health information is everybody’s business. It involves all stakeholders in mental health services. The barriers experienced in implementing consumer outcomes in mental health services have been considerable. This process is unprecedented or unparalleled in Australian mental health services and the process of routinely measuring consumer outcomes has highlighted many areas for further development.
In order to embed consumer outcomes into clinical practice staff identified as resource people (including trainers) need access to support structures such as mental health information/outcomes working groups, steering committees or implementation groups. These structures need to ensure that there is co-ordination of activities in line with an overarching vision and aim. The overarching structures should ensure that consumer outcome priorities are identified and managed and activities are targeted.
All people involved in the co-ordination, management and development in the use of, consumer outcomes in clinical practice need to be provided opportunities for networking, mentoring and skill development.
outcomes Resource People (oRP) and outcomes trainersItems in italics were taken from additional comments and placed in one of the following five sections and items in square brackets are added to make it general not jurisdiction specific.
1. What should be the key responsibilities of an oRP? (Some of the points in this section depend on how the position/role is defined or organised for example in/out of the team).
• Person who can provide education and training; provide advice on completing measures and entering data and on interpretation within the team; a model of the use of the [data system] and information; promoting clinical utility.
• A team member well accepted by the team not considered as external.
• Identification of people who are struggling and support and mentor them and delivering a process around this to embed in day-to-day practice.
• Contribute to the development of business rules around the ORP role and expectation and delivery of support for team members; attend meetings and provide feedback to and from statewide practice and local team practice.
• Continue to develop their own knowledge of information systems and demonstrate use of information in the system using the [funded jurisdictional teams] and other clinical resources.
• Reporting to line management positive and negative information issues; interface with manager and other key players especially [staff that manage mental health information].
• Facilitate development of workplace policies and practices and procedures that facilitate data collection.
• Reference point for accessing resources and skills and motivator for teams.
• Resource in clinical review; assist in the interpretation and meaning of information.
• Show leadership in the use of clinical information to support planning at all levels of service; be a catalyst for change.
Resources 95
• Use information in benchmarking.
• Attend relevant meetings and training sessions.
• Prepare case review lists in advance so staff know when to complete measures.
• ORP should be able to reset passwords.
Activities that promote data quality in terms of validity, reliability, accuracy and timeliness of the consumer outcomes data.
2. What are realistic expectations of an oRP?
a) From their team
• ORP assists the team to improve skills in clinical utility and facilitate better performance at district level.
• Demonstrate a high degree of knowledge of the system and the ability to articulate this to team members (walk the walk); should be able to inspire clinicians; motivator for participation and learning; clarify problems and challenges within the system.
• Facilitate broad skill development including their own e.g. forums, workshops etc.
• Follow through on [consumer self-assessment] completion issues; willingness to drive consumer involvement.
• Be accessible.
• Work to resolve issues with others.
• Skills in extracting information from the system and demonstrate how to utilise reporting capacities.
• Creates a culture that reflects [data use] as an integral part of the continuum of care.
b) From the service
• Reporting to line management any difficulties or problems regarding implementation.
• Effective communication, commitment and enthusiasm and belief in benefit and value of resource passing information on to the team.
• Running and interpreting reports in discussion with line management.
• ‘Go to’ person with information regarding mental health information and support in use.
• Network with other ORP; support management in the use of data in service planning/mapping.
• Demonstrate using systems in correlation [non-integrated data systems]
• Time to provide training and support staff and to be up skilled.
• Recognition.
• Improved data collection [and use].
• Manager should have written into position descriptions that they are accountable for collections.
• Routine part of clinical practice.

96 Resources
c) other
• Liaise with [jurisdictional funded teams] to continue to progress development to reduce barriers including reporting of difficulties/barriers within team.
• Cleansing of data either directly or facilitating.
• Pass information onto the team.
• Leadership from above and within the team.
• Regular feedback/input between [Mental Health Information Managers] and ORP
• Improvement in consumer participation in mental health service provision.
• Engagement of medical staff.
• [Provide training to consumers and carers in the use and interpretation of OMs.]
3. What qualities and skills make an effective oRP?
• Patience, effective communication, approachable, quick learner, sense of humour, availability and tolerant.
• Able to work out what teams need and to integrate knowledge requirements with type of service.
• Ability to work with other ORP.
• Clinical credibility within a team (not new clinician); good clinical experience.
• Be familiar with able to access, troubleshoot and navigate the system.
• Be proactive and take personal responsibility in regard to access and continuing development of knowledge.
• Innovative and passionate about mental health information.
• Self-motivated and responsible; innovative, thinks outside the square.
• Good computer skills.
• [The ability to communicate with non-clinical people the value and use of the consumer outcomes.]
4. What sustains an oRP?
a) Resources
• Clinicians’ handbook and references.
• Access to trained staff and mentors, support network, training/ ORP Resource days and forums, supervision, clear contact with [jurisdictional funded teams], and steering group.
• Recognition and acknowledgement.
• Benchmarking activities.
• Computer access.
• Time, support of line manager, time to be released from role, and more than one ORP per site.
Resources 97
b) Structures and processes
• Realistic goals and standardised processes.
• Training linked to orientation.
• Clear and concise, systematic and not too cumbersome.
• Linking care plans to outcome measures, flowcharts for forms and data entry points.
• Local outcomes trainer to educate, motivate and drive.
• Admin support, and support from line and upper management.
• Leadership by action and example.
• Dedicated ORP days.
• Clear reporting process for ORP to manage issues with TL’s and line mangers.
• Clear lines of responsibility to [jurisdictional funded teams] etc.
c) training
• Regular updates including [data system], time off to attend and backfill, recognition of importance of training, consistent training and training packages and orientation.
• Collaboration with other ORP.
d) other
• Needs to be able to support other teams that don’t have an ORP.
• ORP email network and online network.
• Tangible recognition/badge/certificate/cash bonus.
5. What barriers impede oRP in their role?
• Culture of organisation, lack of support from management, lack of recognition, relationship with key stakeholders, and support from medical staff.
• Attitudes, reluctance of clinicians to use the [data] system and implications for ORP role.
• Staff who believe they are competent but aren’t, and [who] are unwilling to accept support, and need to have minimum competency requirements.
• Staff skills and high staff turnover.
• Time, workloads, finances/resources, computer access, and lack of computer skills.
• Orientation for new staff.
• Clarity of ORP role, retention of ORP, and team acceptance of role as support to clinicians.
• Fitting specialist teams into the [data collection protocol and data] system28.
28 Queensland Health, Outcomes Resource Person Development Activity Summary – Queensland Northern Area Outcomes Forum, 16 May 2008.

98 Resources
ExamplesThe principal responsibility of a consumer outcomes resource person is to drive the routine collection and use of mental health information in their Mental Health Service. The role involves a range of responsibilities that will be determined by available resources, skill level and number of resource people in any given area.
Possible roles include:
• Mentoring (individual, group, team based) in practical application such as:
– offering the self-assessment
– providing feedback on the self-assessment
– providing feedback on the clinician measures
– promoting compliance to the collection protocol
– using consumer outcomes in clinical reviews
– using consumer outcomes to inform future intervention options
– data system – entry and/or extraction
– interpretation of consumer level reports.
• Guidance or expert advice to clinicians/teams on:
– protocol collection
– business processes and rules for collection and utilisation of consumer outcomes
– application and analysis of consumer outcomes.
• Providing guidance or advice to managers by:
– identifying and communicating current work-practice issues
– developing and implementing workable solutions to current work-practice issues
– promoting consumer outcome information to inform service planning and improving models of service delivery.
• Provide guidance and advice to consumer and carer consultants:
– interpretation of consumer outcome reports at systematic advocacy level such as at quality meetings.
• Reporting:
– provide recommendations to improve reporting processes
– provide ad hoc advice or reports to the Executive as requested
– generating reports to the team/team leader regarding current compliance with collection (where possible).

Resources 99
• Networking:
– participation in consumer outcomes activities (national conference, statewide forums, local networking meetings)
– disseminate and actively promote communication tools such as updates, newsletters available locally, from state or territory department, and nationally.
• Progressing mental health information development and use:
– monitor the quality of the information being entered into the database and addressing problems which may arise
– liaison with relevant committee/work group or funded positions that oversees consumer outcomes collection and utilisation
– chairing the local working group
– problem identification, escalation and resolution in collaboration with key stakeholders, state or territory department, and AMHOCN.
• Training role.
Cairns Mental Health Information: Outcomes Resource Person roles and responsibility document informed this section.

100 Resources
Consumer and carer consultants (or equivalent)Consumer and carer consultants are an invaluable resource for mental health services to strengthen consumer and carer engagement. Their potential roles in consumer outcomes should focus at systemic approach to consumer and carer engagement by facilitating clinicians’ capacity and awareness rather than being the primary driver.
Consumer and carer consultants have a range of skills, knowledge and abilities as well as variation in roles, responsibilities and job expectations. There is an ongoing need for training and support to enhance skills of consumer and carer consultants to enable them to effectively and equally participate within Mental Health Services.
Consumer Advisory Groups (CAG) or consumer consultants are resourced to run focus groups to explore the consumer self-assessment measure used in their jurisdiction and provide feedback and/or a protocol to their service about how their consumers would like the self-rated measure offered to them and also how they would like follow up discussions to occur. This would be a good way to increase participation and at the same time perhaps try to promote sensitive and respectful practice in relation to self-rated measures.
Most consumer and carer consultants (or their equivalents) are employed in clinical mental health services. There are however a small number of positions with a dedicated focus either on statewide activities, an education role or in developer/policy role. This group of staff will have additional workforce development requirements which have not been articulated in this resource.
Depending on position requirements and resources some consumer and carer consultants will be in a position to run groups for consumers and carers regarding the consumer outcomes to increase awareness, provide education and clarify expectations. These groups could be delivered to consumers and carers together or each group separately.

Resources 101
ExamplesThe role involves a range of responsibilities that will be determined by available resources, skill level and number of other resource people (clinicians or other consumer and carer consultants) in any given area.
Possible roles include:
• Promoting the value of consumer self-assessment with:
– clinical teams
– consumer and carer groups including how they can get the most out of the consumer self-assessment process.
• Involvement in training/workshop for clinicians on:
– offering the self-assessment
– providing feedback on the self-assessment
– providing feedback on the clinician measures.
• Development of materials for consumers and carers about consumer outcomes nationwide plain English version.
• Guidance to clinicians/teams on:
– consumer self-assessment challenges
– how consumer outcomes could be used in dialogue with consumer and/or carer and in clinical decision making.
• Providing guidance or advice to managers by:
– identifying and communicating current work-practice issues
– promoting consumer outcome information to inform service planning and improving models of service delivery.
• Understanding and using outcome measures to provide leadership in service planning, improving models of service delivery and developing a truly recovery orientated mental health system.

102 Resources
• Reporting:
– provide recommendations to improve reporting processes
– involvement in service development for consumer take-home reports.
• Networking:
– participation in consumer outcomes activities (national conference, statewide forums, local networking meetings and cross jurisdictional meetings)
– disseminate and actively promote communication tools such as updates, newsletters available locally, from state or territory department, and nationally.
• Progressing mental health information development and use:
– liaison with relevant committee/work group or funded positions that oversees consumer outcomes collection and utilisation
– problem identification, escalation and resolution in collaboration with key stakeholders, state or territory department, and AMHOCN
– participation in activities for the development of a carer measure in adult and older person mental health services
– role in garnering and recording consumers opinions/perspectives about consumer outcomes.
• Consumer evaluation of service implementation of consumer outcomes, some questions that could be asked are:
– How well did the service inform all consumers about all the consumer outcome measures?
– How well did the service inform all consumers about the self rating tools?
– How well did the service inform all consumers about how consumer outcomes would be used (within the treating team, within the service, within the state, at the national level)?
– How well did the service engage with consumers in discussing the consumers individual ratings?
– How well did the service inform all consumers how their own individual ratings (clinician and consumer rated) would be incorporated into care plans?
- How well did the service use OM for benchmarking service development and quality improvement?
For more information:
David Guthrie, Mishka McIntosh, Tom Callaly, Tom Trauer and Tim Coombs, Barwon Health: Community and Mental Health, Geelong, Victoria, Australia, Consumer attitudes towards the use of routine outcome measures in a public mental health service: A consumer-driven study, International Journal of Mental Health Nursing (2008) 17, 92–97
• Co-facilitator training role.

Resources 103
6.2 materials States and territories have developed information brochures for consumers and carers about the consumer outcome agenda. These materials are typically pitched at the general awareness raising level and are not necessarily written in consumer or carer friendly language.
The ‘Whose outcome is it anyway? Consumer Self-assessment in Mental Health’ brochure and poster was developed by consumers and carers for consumers and carers. These materials are general and talk about the consumer self-assessment process.
In developing this resource a gap has been identified for more targeted and detailed materials that clinicians could provide consumers and carers on the measures in the NOCC suite. It has been recommended that these materials should be written in consumer and carer friendly language. While outside of scope for this particular resource, preliminary discussions have taken place about the value of developing this type of materials.
Each state and territory has an internet address accessible by consumers and carers. There is significant variation in the extent of information contained on these sites with a number of jurisdictions utilising their intranets for consumer outcomes information which are not accessible by consumers and carers.
6.2.1 National Child and adolescent/youth mental health services
Strengths and Difficulties Questionnaires (SDQ) All Australian Child and Adolescent/Youth Mental Health Services utilise the Strengths and Difficulties Questionnaire (SDQ). This questionnaire is in the public domain and everybody can access the forms at: www.sdqinfo.com/b1.html.
translationsAll translations of the SDQ are undertaken/commissioned by the author of the SDQ Robert Goodman. The SDQ translations follow the UK English version not the Australian English version. This means there are some variation in wording of a couple of questions but more importantly there is only one parent version for 4 - 16 year old unlike the NOCC version which splits parents into 4-10 and 11-17. This issue was forwarded by Victorian Department of Human Services, to the CAMHS outcomes expert group November 2007 meeting for advice on possible implications for completion and entry of translated versions. No outcome has been received. The SDQ Vietnamese is in development with finalisation and availability on the SDQ website remains unknown.
Whoseoutcome is it anyway?
QUOTES:(From a workshop involving consumer and
carer consultants as part of the Western
QUATRO Project, September 2005)
“Consumer self assessment is seen as a
vehicle in the consumer’s journey. Used to
discuss goal setting, to assist in evaluating the
service being received and assess when to
move on.”
“What does being valued really look like and
how does it feel?”“Map of recovery; where we are, where we
want to get to.”“Triad - dialogue and relationship with consumer,
carer and case manager. Working together
to identify personal priorities of needs.” “By sharing and exploring the information it
will set up an expectation that the consumer’s
opinion is valued.”
WHERE CAN I GET MORE INFORMATION?
If you have any questions, concerns or would
like to get more information on consumer self
assessment or clinician measures, talk to:• Your mental health clinician• Consumer and/or carer consultants
• Family, friends or carers• Other consumers or consumer groups• Other carers or carer groups• www.mhnocc.org
LOCAL SERVICE INFORMATION
Consumer Self Assessment in Mental Health

104 Resources
The SDQ is translated into the following languages and (D) denotes drafts:
Afrikaans Farsi Japanese Serbian
Amharic Finnish Kannada (D) Sinhalese
Arabic French Khmer Slovak
Basque Gaelic (D) Korean Slovene
Bengali Gallego Lithuanian Somali
Bulgarian German Macedonian Spanish
Catalan Greek Malay (D) Spanish (Rio de la Plata)
Chinese Greenlandish Maltese Swedish
Croatian Gujarati Norwegian Tamil (D)
Czech Hebrew Pashto Thai
Danish Hindi Polish (D) Turkish
Dari Hmong Portuguese (Brazil) Ukranian (D)
Dutch Hungarian Portuguese (Portugal) Urdu
English (Australia) Icelandic Punjabi Welsh
English (UK) Indoensian Romanian Xhosa
English (USA) Irish (D) Russian Yoruba
Estonian Italian Sami
Australian mental Health outcomes and Classification NetworkAustralian mental Health outcomes and Classification Network (AmHoCN) provides the authoritative focal point for national leadership in the development of outcomes and casemix concepts in mental health and is currently funded until June 2008. Broadly, AMHOCN performs three roles, including:
1. Provide a data bureau function to receive and process the mental health outcomes and casemix data submitted by states and territories. This function will be undertaken by Strategic Data, a Victorian company with expertise in the establishment and management of large data sets.
2. Act as a specialist research and development group for the analysis, reporting and ongoing development of mental health outcomes and casemix information at a national level while also providing a resource for such work at state and territory level. This function will be undertaken by the University of Queensland and the University of Melbourne, primarily Dr Philip Burgess and Dr Jane Pirkis.
3. Act as a national training and service development resource centre for the ongoing use of outcomes and casemix measures, designed to both inform and improve practice through workforce training, benchmarking and related activities. This function will be undertaken by The New South Wales Institute of Psychiatry, primarily Mr Tim Coombs and Dr Louise Newman.

Resources 105
The Commonwealth Department of Health and Ageing established a website to support the Mental Health National Outcomes and Casemix Collection. It can be found at www.mhnocc.org.This site aims to support the implementation of routine consumer OM Australia’s public mental health sector. The purpose of NOCC is to improve the quality of mental health services through better understanding and use of information about the outcomes for consumers of mental health services. This site provides key resources on mental health outcomes and case complexity measurement and provides a forum for sharing ideas, views and experience. The site is intended to be used by clinicians, managers, consumers, carers, policymakers, researchers and all other interested stakeholders. training resources on this site include:
• Rater training including an extensive range of resources (PowerPoint slides, manuals, vignettes) for CAMHS, Adult and Aged Persons, available from www.mhnocc.org/amhocn/Training_Resources/.
• Clinical utility training Resources - ‘Whose Outcome is it Anyway?’ AMHOCN in collaboration with Barwon Health the lead agency of the Victorian Western Cluster Quality through Outcomes Project produced a range of promotional and educational materials including:
• Poster - ‘Whose Outcome is it Anyway?’
• Brochure - ‘Whose Outcome is it Anyway?’
• Flipper Card - ‘Whose Outcome is it Anyway?’
• A DVD of consumers, carers and clinicians that explores the opportunities that routine OM holds in clinical practice.
• Clinical utility training manual, PowerPoint slides and vignettes for CAMHS, Adult and Aged.
Hard copies of the promotional materials including a ”novelty flipper card” along with copies of the DVD and associated training materials are available on request.
Clinicians also have access to the decision support tool which contains clinical reference material generated by AMHOCN from data submitted by each jurisdiction and can be found at http://wdst.mhnocc.org.
For information on outcome measurement undertaken internationally:• Activities in Ohio - www.mh.state.oh.us/oper/outcomes/outcomes.index.html
• MH Smart in New Zealand - www.huttvalleydhb.org.nz/Article.aspx?ID=623
• Australasian Mental Health Outcomes Conference 2007
– www.tepou.co.nz/page/323-Speakers-039-Presentations-Day-One
– www.tepou.co.nz/page/324-Speakers-039-Presentations-Day-Two
– www.tepou.co.nz/page/325-Speakers-039-Presentations-Key-Notes
Whoseoutcome is it anyway?
QUOTES:(From a workshop involving consumer and
carer consultants as part of the Western
QUATRO Project, September 2005)
“Consumer self assessment is seen as a
vehicle in the consumer’s journey. Used to
discuss goal setting, to assist in evaluating the
service being received and assess when to
move on.”
“What does being valued really look like and
how does it feel?”“Map of recovery; where we are, where we
want to get to.”“Triad - dialogue and relationship with consumer,
carer and case manager. Working together
to identify personal priorities of needs.” “By sharing and exploring the information it
will set up an expectation that the consumer’s
opinion is valued.”
WHERE CAN I GET MORE INFORMATION?
If you have any questions, concerns or would
like to get more information on consumer self
assessment or clinician measures, talk to:• Your mental health clinician• Consumer and/or carer consultants
• Family, friends or carers• Other consumers or consumer groups• Other carers or carer groups• www.mhnocc.org
LOCAL SERVICE INFORMATION
Consumer Self Assessment in Mental Health

106 Resources
6.2.2 State and territory
States
Victoria
information is available at:
A comprehensive website has divided into six major areas can be found at:
www.health.vic.gov.au/mentalhealth/outcomes/index.htm
• About Outcome Measurement
• Consumers and Carers
• Mental Health Clinicians
• Sustainability & Quality through Outcomes
• Resources
• Application of OM in Victoria Frequently Asked Questions (FAQ)
This website is accessible to the general public. In addition, a number of Victorian mental health services have placed information on their local Intranet.
Victorian “Outcome Measurement in Clinical Mental Health Services Program Management Circular” was disseminated in July 2007 and articulates the Department of Human Services expectations. This is available at: www.health.vic.gov.au/mentalhealth/pmc/outcome-measurement.htm.
Information brochures for consumers and carers are available at: www.health.vic.gov.au/mentalhealth/outcomes/concare.htm#info_books.
Measuring consumer outcomes in clinical mental health services: A training manual for services in Victoria 2nd Edition 2003 was developed and distributed. This manual has seven major sections – Introduction, CAMHS, Adult, Aged persons, Training, Glossary, and Resources. The resources section is broken into five sections being General, CAMHS, Adult and Aged Persons. The manual also includes a DVD with vignettes. The sections of the manual are available electronically on the website:
www.health.vic.gov.au/mentalhealth/outcomes/resource5a.htm.
Most mental health services in Victoria have developed staff resources/manual that are available in hard copy or on local intranets.
if you need more information contact:
Senior Project OfficerQuality ServicesSector Quality and Workforce DevelopmentMental Health and Drugs DivisionDepartment of Human Services GPO Box 4057 Melbourne Victoria 3001

Resources 107
Consumer self-assessment - BASiS-32® translations
To strengthen participation and use of outcome measures among consumers from culturally and linguistically diverse backgrounds, the Department of Human Services has commissioned translations of the adult consumer self-assessment measure, the BASIS-32®, into a number of community languages:
Arabic, Cambodian, Chinese, Filipino (Tagalog), Finnish, French, Greek, Italian, Japanese, Korean, Portuguese, Spanish, Thai and Vietnamese.
Engagement of interpreters should also be considered when discussing and using outcome measures with consumers from culturally and linguistically diverse backgrounds. As the BASIS-32® is protected by copyright and not in the public domain; the Department of Human Services is unable to make copies of the BASIS-32® translations available on its website. However they can be posted on local service intranet sites. Translated Versions of the BASIS-32® are available to consumers of public clinical mental health services from culturally and linguistically diverse backgrounds in Victoria.
South Australia
information is available at:
Website is under development: www.health.sa.gov.au/mentalhealth.
if you need more information contact:
Central NOCC CoordinatorMental Health UnitPO Box 287Rundle Mall 5001Adelaide
Consumer self-assessment K-10
There is a reference to the Mental Health National Outcomes Casemix Collection internet site www.mhnocc.org from the SA Health Internet site, where translations of the K10 can be sourced, languages are:
Arabic, Bosnian, Chinese, Croatian, English, Farsi, Greek, Hindi, Italian, Korean, Macedonian, Serbian, Spanish, Tagalog, Turkish, Vietnamese.
tasmania
information is available via intranet site:
Coding References are available on the intranet site. This provides the HONOS glossaries. Our clinicians currently have limited access to the intranet.
if you need more information contact:
Data Management and Reporting ConsultantDepartment of Health and Human ServicesPhone: (03) 6230 7727

108 Resources
Consumer self-assessment - BASiS-32® translations – No translations available.
Western Australia
information is available:
Website is under development, www.comhwa.health.wa.gov.au/one/index.asp.
if you need more information contact:
Senior Program ManagerMental Health DivisionDepartment of Health189 Royal StreetEast Perth WA 6001 Phone: 08 9222 2349
Consumer self-assessment K-10
Our website links to the MHNOCC.ORG website which provides the translations of the consumer self-assessment in other languages.
Queensland
information is available:
Information is available via an intranet site, which cannot be accessed externally. Contents include: self-directed learning package for clinicians, clinician reference manual, outcome measurement forms.
if you need more information contact:
Area Clinical Information Team (ACIT) Co-ordinator can be contacted for more information.
Consumer Self-Assessment - mHi
MHI Translations Online - The Transcultural Mental Health Centre has provided assistance in translating the Mental Health Inventory forms into 13 languages including Arabic, Croatian, Filipino, Khmer, Serbian and Vietnamese. The MHI translations can be accessed through the Information Systems & Management Team intranet site (QHEPS).
New South Wales
information is available:
Information is available on the NSW Health intranet for clinicians o download and use as required.
if you need more information contact:
Project Manager MHOATInforMH: Building Knowledge, Supporting Services, Improving Care

Resources 109
InforMHMacquarie HospitalPO Box 169North Ryde NSW 1670
Consumer Self-Assessment – Kessler-10 translations
K10 and consumer brochures have been translated into the following 15 languages:
Arabic, Bosnian, Croatian, Greek, Hindi, Korean, Macedonian, Spanish, Tagalong, Vietnamese, Chinese, Farsi, Italian, Serbian, Turkish.
territories
Northern territory
information is available at:
Information is available via an intranet site (http://internal.health.nt.gov.au/family/mental/mental.shtml) , which cannot be accessed externally. Contents include: Self-directed learning package for clinicians, Clinician Reference Manual, K10 forms, with, besides English, translations into 15 languages (taken from NSW Transcultural Mental Health), also SDQ forms and ICP forms for Adults and Older Persons, and Child and Adolescent ICP.
if you need more information contact:
Either:
- Comet Project Officers- Senior Policy Officer, Workforce Development and Clinical Standards- Information Officer
Mental Health ProgramPO Box 40596CasuarinaNT 0811Phone: 08 8999 2553
Consumer Self-Assessment – Kessler-10 translations
K10 translations available on NT Government Intranet, are based on the NSW MHOAT standard suite of translations. Languages are: Arabic, Chinese, Farsi, Hindi, Korean, Serbian, Tagalog, Vietnamese, Bosnian, Croatian, Greek, Italian, Macedonian, Spanish, Turkish.

110 Resources
Australian Capital territory
information is available internally:
http://acthealth/c/HealthIntranet?a=da&did=2157623 (This is only available on our Intranet site, resources are available to staff of ACT health)
Information includes outcome measurement resources, information system details (database manual, electronic reporting of outcomes measures including NOCC suite of measures), clinical documentation manuals, outcomes measures glossaries, self-assessment forms.
Information available to the public: http://www.health.act.gov.au/c/health?a=sp&pid=1148966417
(Outcomes resources not yet available via the Internet currently under development pending service reform)
if you need more information contact:
{Interim contact} Paul Mayers Mental Health Business Analyst Mental Health – ACT PO Box 825 CANBERRA ACT 2601 Ph: (02) 6205 1313
Consumer self-assessment – BASiS-32® (Adult and older Persons) and SDQ (Child and Adolescent and Parent/Carer)
Self-assessment outcomes measures are provided/offered to consumers and potential consumers of mental health services. Availability of translations of these tools into other languages is being pursued based on the work conducted in Victoria with respect to the BASIS-32®. Self-assessment measures currently available in English only, this is being reviewed for need and accessibility to those population groups who use other languages that may potentially access public mental health services in the ACT.

Australian Federal Government’s Department of Health and Ageing
www.health.gov.au/internet/main/publishing.nsf/Content/mental-pubs-n-workstds www.health.gov.au/internet/mentalhealth/publishing.nsf/Content/doha-plan-1
Australian Association of Social Workers
www.aasw.asn.au/
www.aasw.asn.au/adobe/publications/Practice%20Standards_Supervision.pdf
Better Access to mental Health Care initiative
www.primarymentalhealth.com.au/site/index.cfm?display=15129
mental Health Carers ARAFmi Australia
www.arafmiaustralia.asn.au
mental Health Coalition
https://owa.sagems.sa.gov.au/exchweb/bin/redir.asp?URL=http://www.mhca.org.au/donate.html
mental Health Council of Australia
www.mhca.org.au/AboutUs/ListMemberOrgs.html
mental Health National outcomes and Casemix Collection
www.mhnocc.org
www.mhnocc.org/Benchmarking
www.mhnocc.org/amhocn/Training_Resources
mental Health Nurse Association
www.amicus-mhna.org
mental Health Nurse incentive Program
www.medicareaustralia.gov.au/provider/incentives/mental-health.jsp
www.medicareaustralia.gov.au/provider/incentives/files/2111-mental-health-nurse-incentive-program-program-guidelines.pdf
mH Smart in New Zealand
www.huttvalleydhb.org.nz/Article.aspx?ID=623
mentoring Works
www.mentoringworks.com.au/notice.html
ohio Department of mental Health
www.mh.state.oh.us/oper/outcomes/outcomes.index.html
New Zealand’s National Centre of mental Health Research – te Pou
www.tepou.co.nz/page/23-Welcome
www.tepou.co.nz/page/420-Information-Utility
www.tepou.co.nz/page/323-Speakers-039-Presentations-Day-One
www.tepou.co.nz/page/324-Speakers-039-Presentations-Day-Two
www.tepou.co.nz/page/325-Speakers-039-Presentations-Key-Notes
SANE
www.sane.org
South Australian Department of Health
www.health.sa.gov.au/mentalhealth/Default.aspx?tabid=99
the Australian Psychological Society Ltd
www.psychology.org.au
Websites
Ref
eren
ces References 111

112 References
Victorian Department of Human Services
www.health.vic.gov.au/mentalhealth/
www.health.vic.gov.au/mentalhealth/outcomes
www.health.vic.gov.au/mentalhealth/cpg/families.htm
www.health.vic.gov.au/mentalhealth/outcomes/concare.htm#info_books
www.health.vic.gov.au/mentalhealth/outcomes/index.htm
Victorian mental Health Carers Network
www.carersnetwork.org
Victorian mental illness Awareness Council
www.vmiac.com.au
Published journals, reports, books, presentations, promotional materialsAustralian Health ministers Advisory Council (AmHAC) - National mental Health Working Group, information Strategy Committee, Commonwealth of Australia:
• National Standards for Mental Health Services, December 1996 – currently under review• National Practice Standards for the Mental Health Workforce, September 2002
Jones A and May J, Working in Human Service Organisations A critical introduction, Longman, Australia, 1992.
Mental Health National Outcomes and Casemix Collection: Technical specification of State and Territory reporting requirements for the outcomes and casemix components of ‘Agreed Data’, Version 1.50, Department of Health and Ageing, Canberra, 2003.
NMHWG Information Strategy Committee Performance Indicator Drafting Group, Key Performance Indicators for Australian Public Mental Health Services, ISC Discussion Paper No.6 Australian Governement, Department of Health and Ageing, Canberra, 2005.
Pirkis J, Burgess P, Kirk P, Dodson S & Coombs T, ‘Review of standardised measures used in the National Outcomes and Casemix Collection (NOCC) Version 1.2’ Australian Mental Health Outcomes and Classification Network ‘Sharing Information to Improve Outcomes’ An Australian Government funded initiative, May 2005.
Published by Queensland Health:
• Outcomes Initiative Updates 7, 8, 9 • Cairns Mental Health Information: Outcomes Resource Person roles and responsibility document• Outcomes Resource Person Development Activity Summary – Queensland Northern Area Outcomes Forum
16 May 2008, 2008, Queensland.
Published by the Australian Association of Social Workers:
• National Practice Standards of the Australian Association of Social Workers: Supervision, July 2000
Published by the Australian mental Health outcomes Classification Network:
• Clinical Utility Materials, 2006• ’Whose outcome is it anyway? Consumer Self-assessment in Mental Health’ brochure, 2006• PowerPoint presentation, December 2006
Published by the Department of Human Services Victoria:
• Mental Health and Drugs Division, Department of Human Services, Draft Victorian Outcome Measurement (OM) Training Framework, Victoria, 2008.
• Victorian Western Cluster QUATRO Project, Policies and Procedures Template, 2006
Published by tony Buzan imindmaptm
• Help Manual

Victoria secured Quality Through Outcomes funding provided by Department of Health and Ageing through Commonwealth Own Purpose Outlay, to undertake a national initiative focusing on enhancing the utility of consumer outcome measures for collaborative planning. This project included targeted consultation with jurisdictional representatives/funded teams in adult and aged services in Queensland, who use the Mental Health Inventory, Victoria (BASIS-32®) and NSW (K-10), and the Strengths and Difficulties Questionnaire (SDQ) used nationally in CAMHS ensuring that all of the consumer self-assessment measures are covered. In addition, broader liaison with other states and territories was undertaken.
This phase of resource development was overseen by Veronica Spillane, Manager, Office of the Chief Psychiatrist, Mental Health and Drugs Division, Department of Human Services Victoria.
The project objectives were:
• To explore options to assist clinicians in engaging with consumers in OM in a way that contributes to collaborative care planning.
• To identify barriers and/or difficulties experienced by clinicians in engaging with consumers, with a view to identifying resources and strategies to overcome these.
Anticipated project deliverables:
• Summary of general lessons from Jurisdictional templates completed by states and territories for May 2008 NOCC Trainers Meeting.
• General strategies and techniques resource.
• Preliminary exploration for information sheets/brochures for consumers and carers.
This project was developed and delivered in collaboration with the Australian Mental Health Outcomes Classification Network and finished in June 2008.
A facilitated discussion regarding the concept and usability of this resource was undertaken with 70 mental health clinicians attending the Northern Forum in Cairns.
App
endi
ces
Appendix 1Phase one – project overview and consultation processes
Appendices 113

114 Appendices
Phase one - consultation process
Consultation for the development of a draft general resource for clinicians
27 March 2008 Western Australia - phone call and email contribution
April 2008 Queensland - meeting with Area Clinical Information Team in Brisbane (2-4 April), meeting with ACIT and local resource person in Townsville (22-24 April) discussion in journal club with Charters Towers Mental Health Service
April 2008 South Australia - attendance at two day forum (day 1 consumer, day 2 clinician) in Adelaide (7-8 April), attended two clinical reviews at Noarlunga and meeting with Noarlunga NUM (9 April)
17 April 2008 Victoria - meeting with QUATRO VIC team representatives (17 April and another scheduled for 29 May)
20 April 2008 Template emailed to jurisdiction representatives (requested completion by 16 May)
Consultation on the draft general resource for clinicians
15 May 2008 Facilitated session at Cairns Forum (70 participants 1 hour)
20 -21 May 2008
Jurisdictional meeting - Day 1 Training, Day 2 National Project - workshop to refine the project resources
23 May 2008 Consumer and carer advisor workshop - to develop and refine the general strategies and techniques resource and to develop info sheets for consumers and carers
28 May 2008 Consultation with Clinical Advisors to Victorian Chief Psychiatrist
29 May 2008 Consultation with QUATRO VIC team
2 June 2008 Consultation with Corporate Publication DHS for publication options
5 June 2008 Consultation with MH-OAT and MHIDP
10 June 2008 Presentation to Victorian Quality Through Outcomes Statewide Steering Committee and invitation to feedback on resource

Appendices 115
Phase one - consultation forums attendee list
Jurisdiction Name Position Consultation Activity
Consumer & Carers
Rosemary Lawton Consumer Consultant, Royal Children’s Hospital, Integrated Mental Health Program
Consumer & Carer Workshop
Tania Lewis Consumer Advisor, work well consulting
Consumer & Carer Workshop
Beth Bailey Carer, Victorian Mental Health Carers Network
Consumer & Carer Workshop
AMHOCN Tim Coombs Director Training and Service Development
Project planning meetings
NOCC Trainers two day meeting
Consumer & Carer Workshop
ACT Paul Mayers NOCC Trainers two day meeting
Briony Holdsworth
NSW Neda Dusevic NSW MH-OAT Manager NOCC Trainers two day meeting
Jenny Wildgoose NSCCAHS Quality Systems Manager MHIUMF Consultation
Rhian Davies SSWAHS MH-OAT Manager
Genevieve Watt SSWAHS MH-OAT Manager
Urszula Stratton GSAHS MH-OAT/MHIDP Manager
Aleks Konjevic GSAHS MH-OAT/MHIDP Manager
Glen Bowcock NSCCAHS MHIDP Project Officer
Jarod Hamilton NSCCAHS MH-OAT Manager
Tony Druce HNEAHS MHIDP Manager
Malini Sivabalan CHW MHIDP Manager
Margaret Martin HNEAHS MH-OAT Manager
Nadine Wheeler HNEAHS MHIDP Manager
Dale Owens JH MH-OAT Manager
Karen Smith SWAHS MHIDP Manager
Ron Catanzaro NSCCAHS MHIDP Manager
Colin Scott Associate Director Operations & Systems, InforMH
Keiron McGlone Manager Systems Development, InforMH
Kylie Ramachenderan HNEAHS MHIDP Coordinator
NT Rachel Conn Comet Project Officer NOCC Trainers two day meeting
John Trevor Gregory Team Leader, Central Australia Mental Health Service
Lorin James Senior Policy Officer, Workforce Development and Clinical Standards

116 Appendices
Queensland Kathy Stapley A/ Area Clinical Information Team Leader
ACIT Meeting in Brisbane NOCC Trainers two day meeting
Maree Lacey ACIT Meeting in Brisbane
Erika Heslin Area Clinical Information Team Northern Area
ACIT Meeting in Brisbane North Queensland visit
Carolyn Dixon North Queensland visit
Diana Bissett Mental Health Information Manager Cairns
Queensland Rachel Duffy OT – CTRU Charters Towers - Journal Club ConsultationMichelle Ramm OT – CMH
Monique Stewart OT – CMH
Kirsty Rossiter CNC – CMH
Patricia Buck RN – CTRU
Nick Pavlichok NUM – CTRU
Tanya Porter Indigenous Mental Health Worker – CMH
Carole Davis CN – CTRU
Connie Faber RN – CTRU
Chris Sleight SAHP – CTRU
SA Bev Malone Project Officer, Central National Outcomes & Casemix Collections Coordination, Mental Health Unit
SA Health
SA visit; NOCC Trainers two day meeting
Graeme Sanders Outcomes Coordinator
Mental Health Research and Outcomes Unit CNAHS
Sarah Anstey Project Officer, Southern Mental Health
NOCC Trainers two day meeting
2-day SA forum Clinicians Supporting the Consumer Journey
Noarlunga Transitional Care
Southern Adelaide Health Service Observation of integrating consumer outcomes in clinical review and discussionSouthern Mobile
Assertive Care
Terena Slattery Clinical Nurse Manager - Morier Ward, Noarlunga Health services
Meeting
Tasmania Ray Kemp Data Management and Reporting Consultant
NOCC Trainers two day meeting
Victoria Glenda Pedwell QUATRO VIC Team Leader NOCC Trainers two day meeting
QUATRO VIC consultationLucy Horgan Project Officer (Clinician)
Alex Pleban Project Officer (Clinician) QUATRO VIC consultation
Karen Williams Project Officer (Clinician)
Katie Weedon Project Officer (Consumer Participation)
QUATRO VIC consultation
Quality through Outcomes Statewide Steering Committee
Office Chief Psychiatrist – Clinical Advisors
WA Creswell Surrao Senior Program Manager NOCC Trainers 2 day meeting

Appendices 117
Appendix 2Glossary
term Definition
Carer Carer refers to nominated carers, family members or friends who play a vital role in supporting a consumer with a mental illness who accesses public mental health services. They are usually parents/caregivers in Child and Adolescent Mental Health Services. They are important partners with mental health services in improving the health and wellbeing of the people for whom they care.
Carer assessment In Australian Child and Adolescent/Youth Mental Health Services there is a parent/caregiver version of the Strengths and Difficulties Questionnaire (SDQ), the consumer self-assessment measure.
Carer consultant A person with experience as a carer for a person with a mental illness.
Care plan Generic phrase used for all individual consumer level planning. May also be known as individual service plan, treatment plan (not necessarily the jurisdiction mental health legislation requirement) or management plan.
Clinician rated measures
Purpose
A measure designed for completion by a clinician of public mental health services rated following an assessment of a consumer as defined in the National Outcomes and Casemix Collection (NOCC).
measures
Child and Adolescent
• Health of Nation Outcome Scale Children and Adolescents (HoNOSCA)
• Factors Influencing Health Status (FIHS)
• Children’s Global Assessment Scale (CGAS)
Adult
• Health of Nation Outcome Scale (HoNOS)
• Life Skills Profile (LSP-16)
• Focus of Care (FOC)
Older Person
• Health of Nation Outcome Scale 65+ (HoNOS65+)
• Life Skills Profile (LSP-16)
• Focus of Care (FOC)
• Resource Utilisation Groups – Activities of Daily Living (RUG-ADL)
Clinical review Multidisciplinary review of consumers of public mental health services conducted with peers and more experienced colleagues.
Clinical supervision Clinical supervision incorporates both operational and professional practice components.
Consumer Consumer refers to a person with a mental illness who accesses public mental health services.
Consumer consultant
A person with experience of mental illness who is employed by a mental health service. Role definitions vary but are usually different from individual advocates or peer workers and have a quality improvement aspect.
Consumer outcomes
Consumer outcomes in this resource refers to all measures included in the National Outcomes and Casemix Collection (NOCC).

118 Appendices
term Definition
Consumer self-assessment
Purpose
A measure designed for completion by a consumer (and parent/caregiver in child and adolescent) of Australian mental health services. Consumer self-assessment refers to the consumer rated measures used in National Outcomes and Casemix Collection (NOCC).
measures
Child and Adolescent
• Strengths and Difficulties Questionnaire (SDQ) – youth, parent and teacher versions
Adult & Older Person
• Kessler-10
• Behaviour and Symptom Identification Scale-32
• Mental Health Inventory
Dialogue A conversation or discourse between two or more persons; in this resource it refers to a collaborative process between clinician and consumer with the possibility of involving carers.
Jurisdiction Includes all Australian states (New South Wales, Victoria, Queensland, Tasmania, South Australia, Western Australia) and territories (Australian Capital Territory, Northern Territory).
Overt Open and observable; not hidden, concealed, or secret.
www.dictionary.com. The American Heritage® Dictionary of the English Language, Fourth Edition. Houghton Mifflin Company, 2004. http://dictionary.reference.com/browse/overt (accessed: July 05, 2008).
‘Making overt’ refers to clinicians making their assessment of a consumer open and defensible.
NOCC National Outcomes and Casemix Collection is the collection protocol for the reporting requirements of the outcomes and casemix components of ‘Agreed Data’ endorsed by state and territory Health Ministers.


















