Opioid Sensitivity in Children with and without ... · J35.01), but not obstructive sleep apnea, or...
10
PERIOPERATIVE MEDICINE ANESTHESIOLOGY, V 130 • NO XXX XXX 2019 1 C hildhood obstructive sleep apnea, defined by periodic, partial or complete obstruction of the upper airway during sleep, is a common disorder in pediatric patients, with a prevalence as high as 5.7%. 1,2 Children with obstructive sleep apnea often present for surgery and other procedures that require general anesthesia. In fact, the treatment of obstructive sleep apnea is the primary indi- cation for more than 75% of children undergoing tonsil- lectomy with or without adenoidectomy. 3 Tonsillectomy is the most common pediatric operation performed in the United States, with more than 500,000 tonsillectomies per- formed annually. 4 Unfortunately, children at high risk for obstructive sleep apnea are three times more likely to have posttonsillectomy respiratory complications and apneic adverse events than children at low risk for obstructive sleep apnea, 5,6 and the rate of complications in patients with obstructive sleep apnea posttonsillectomy (16 to 27%) is substantially increased compared to that of the general pediatric postoperative population (0 to 1.3%). 7–11 These complications include oxygen desaturation, hypercapnia, obstructive apneas requiring continuous positive airway pressure or airway instrumentation, unexpected intensive care unit admission, and in rare cases, death. Concerns for a heightened risk of opioid induced respi- ratory depression make the perioperative use of opioids in children with obstructive sleep apnea particularly chal- lenging, if not controversial. It has been suggested that they may be at risk from overdose if administered what would otherwise be considered a normal dose of opioid. 6 Indeed, some pediatric surgical centers automatically reduce by half ABSTRACT Background: Opioids are a mainstay of perioperative analgesia. Opioid use in children with obstructive sleep apnea is challenging because of assump- tions for increased opioid sensitivity and assumed risk for opioid-induced respiratory depression compared to children without obstructive sleep apnea. These assumptions have not been rigorously tested. This investigation tested the hypothesis that children with obstructive sleep apnea have an increased pharmacodynamic sensitivity to the miotic and respiratory depressant effects of the prototypic μ-opioid agonist remifentanil. Methods: Children (8 to 14 yr) with or without obstructive sleep apnea were administered a 15-min, fixed-rate remifentanil infusion (0.05, 0.1, or 0.15 μg · kg -1 · min -1 ). Each dose group had five patients with and five without obstructive sleep apnea. Plasma remifentanil concentrations were measured by tandem liquid chromatography mass spectrometry. Remifentanil effects were measured via miosis, respiratory rate, and end-expired carbon dioxide. Remifentanil pharmacodynamics (miosis vs. plasma concentration) were compared in children with or without obstructive sleep apnea. Results: Remifentanil administration resulted in miosis in both non- obstructive sleep apnea and obstructive sleep apnea patients. No differ- ences in the relationship between remifentanil concentration and miosis were seen between the two groups at any of the doses administered. The administered dose of remifentanil did not affect respiratory rate or end- expired carbon dioxide in either group. Conclusions: No differences in the remifentanil concentration–miosis relation were seen in children with or without obstructive sleep apnea. The dose and duration of remifentanil administered did not alter ventilatory param- eters in either group. (ANESTHESIOLOGY 2019; 130:00–00) Opioid Sensitivity in Children with and without Obstructive Sleep Apnea Michael C. Montana, M.D., Ph.D., Lindsay Juriga, B.S., Anshuman Sharma, M.D., Evan D. Kharasch, M.D., Ph.D. ANESTHESIOLOGY 2019; 130:00–00 Submitted for publication April 17, 2018. Accepted for publication January 28, 2019. From the Department of Anesthesiology, Washington University in St. Louis, School of Medicine, St. Louis, Missouri (M.C.M., L.J., A.S., E.D.K.); and the Department of Anesthesiology, Duke University School of Medicine, Durham, North Carolina (E.D.K.). Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. All Rights Reserved. Anesthesiology 2019; 130:00–00 Michael M. Todd, M.D., served as Handling Editor for this article. A preliminary version of this study entitled “Remifentanil in Children with and without Obstructive Sleep Apnea” was presented at the Society for Pediatric Anesthesiology Annual Meeting in Colorado Springs, Colorado, April 1–3, 2016. EDITOR’S PERSPECTIVE What We Already Know about This Topic • Children with obstructive sleep apnea are at greater risk for post- operative hypoxia and other respiratory events as compared with children without this disorder • There is some reason to believe that children with obstructive sleep apnea may be at greater risk for opioid-induced respiratory depres- sion due to increased sensitivity to the drugs What This Article Tells Us That Is New • The authors hypothesized that children with obstructive sleep apnea would be more sensitive to the effects of an opioid (remifentanil) on pupil size—a very good indicator of opioid effects • While remifentanil did reduce pupil size in the expected dose- related fashion, there were no differences between children with obstructive sleep apnea and those without • While the authors did not observe any differences in the effect of remifentanil on respiration, the study was not designed to examine this factor in detail Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited. <zdoi;10.1097/ALN.0000000000002664> Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019
Transcript of Opioid Sensitivity in Children with and without ... · J35.01), but not obstructive sleep apnea, or...

PerioPerative Medicine
ANESTHESIOLOGY, V 130 • NO XXX XXX 2019 1
Childhood obstructive sleep apnea, defined by periodic, partial or complete obstruction of the upper airway
during sleep, is a common disorder in pediatric patients, with a prevalence as high as 5.7%.1,2 Children with obstructive sleep apnea often present for surgery and other procedures that require general anesthesia. In fact, the treatment of obstructive sleep apnea is the primary indi-cation for more than 75% of children undergoing tonsil-lectomy with or without adenoidectomy.3 Tonsillectomy is the most common pediatric operation performed in the United States, with more than 500,000 tonsillectomies per-formed annually.4 Unfortunately, children at high risk for
obstructive sleep apnea are three times more likely to have posttonsillectomy respiratory complications and apneic adverse events than children at low risk for obstructive sleep apnea,5,6 and the rate of complications in patients with obstructive sleep apnea posttonsillectomy (16 to 27%) is substantially increased compared to that of the general pediatric postoperative population (0 to 1.3%).7–11 These complications include oxygen desaturation, hypercapnia, obstructive apneas requiring continuous positive airway pressure or airway instrumentation, unexpected intensive care unit admission, and in rare cases, death.
Concerns for a heightened risk of opioid induced respi-ratory depression make the perioperative use of opioids in children with obstructive sleep apnea particularly chal-lenging, if not controversial. It has been suggested that they may be at risk from overdose if administered what would otherwise be considered a normal dose of opioid.6 Indeed, some pediatric surgical centers automatically reduce by half
aBStractBackground: Opioids are a mainstay of perioperative analgesia. Opioid use in children with obstructive sleep apnea is challenging because of assump-tions for increased opioid sensitivity and assumed risk for opioid-induced respiratory depression compared to children without obstructive sleep apnea. These assumptions have not been rigorously tested. This investigation tested the hypothesis that children with obstructive sleep apnea have an increased pharmacodynamic sensitivity to the miotic and respiratory depressant effects of the prototypic μ-opioid agonist remifentanil.
Methods: Children (8 to 14 yr) with or without obstructive sleep apnea were administered a 15-min, fixed-rate remifentanil infusion (0.05, 0.1, or 0.15 μg · kg-1 · min-1). Each dose group had five patients with and five without obstructive sleep apnea. Plasma remifentanil concentrations were measured by tandem liquid chromatography mass spectrometry. Remifentanil effects were measured via miosis, respiratory rate, and end-expired carbon dioxide. Remifentanil pharmacodynamics (miosis vs. plasma concentration) were compared in children with or without obstructive sleep apnea.
results: Remifentanil administration resulted in miosis in both non- obstructive sleep apnea and obstructive sleep apnea patients. No differ-ences in the relationship between remifentanil concentration and miosis were seen between the two groups at any of the doses administered. The administered dose of remifentanil did not affect respiratory rate or end- expired carbon dioxide in either group.
conclusions: No differences in the remifentanil concentration–miosis relation were seen in children with or without obstructive sleep apnea. The dose and duration of remifentanil administered did not alter ventilatory param-eters in either group.
(ANESTHESIOLOGY 2019; 130:00–00)
Opioid Sensitivity in Children with and without Obstructive Sleep ApneaMichael C. Montana, M.D., Ph.D., Lindsay Juriga, B.S., Anshuman Sharma, M.D., Evan D. Kharasch, M.D., Ph.D.
Anesthesiology 2019; 130:00–00
Submitted for publication April 17, 2018. Accepted for publication January 28, 2019. From the Department of Anesthesiology, Washington University in St. Louis, School of Medicine, St. Louis, Missouri (M.C.M., L.J., A.S., E.D.K.); and the Department of Anesthesiology, Duke University School of Medicine, Durham, North Carolina (E.D.K.).
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. All Rights Reserved. Anesthesiology 2019; 130:00–00
Michael M. Todd, M.D., served as Handling Editor for this article. A preliminary version of this study entitled “Remifentanil in Children with and without Obstructive Sleep Apnea” was presented at the Society for Pediatric Anesthesiology Annual Meeting in Colorado Springs, Colorado, April 1–3, 2016.
editor’S PerSPective
What We Already Know about This Topic
• Children with obstructive sleep apnea are at greater risk for post-operative hypoxia and other respiratory events as compared with children without this disorder
• There is some reason to believe that children with obstructive sleep apnea may be at greater risk for opioid-induced respiratory depres-sion due to increased sensitivity to the drugs
What This Article Tells Us That Is New
• The authors hypothesized that children with obstructive sleep apnea would be more sensitive to the effects of an opioid (remifentanil) on pupil size—a very good indicator of opioid effects
• While remifentanil did reduce pupil size in the expected dose- related fashion, there were no differences between children with obstructive sleep apnea and those without
• While the authors did not observe any differences in the effect of remifentanil on respiration, the study was not designed to examine this factor in detail
2019
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.<zdoi;10.1097/ALN.0000000000002664>Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

2 Anesthesiology 2019; 130:00–00 Montana et al.
PerioPerative Medicine
the opioid dose of patients undergoing tonsillectomy for a diagnosis of obstructive sleep apnea; published guidelines recommend decreasing opioid doses in all patients with sleep apnea, for fear of respiratory depression.13
Despite the widespread belief that obstructive sleep apnea increases opioid sensitivity, evidence to support this claim comes largely from either animal studies, or from human studies that are limited by their reliance on behavioral scores, rather than using objective markers of opioid sen-sitivity.6,9,14–17 There is an unmet need to quantify whether there is opioid sensitivity in children with obstructive sleep apnea as compared to children without obstructive sleep apnea. The purpose of this study was to evaluate opioid pharmacodynamics in pediatric patients with and without obstructive sleep apnea, using remifentanil as the prototype opioid. We tested the hypothesis that children with obstruc-tive sleep apnea have increased pharmacodynamic sensitiv-ity to remifentanil, compared to those without obstructive sleep apnea. Pupil constriction (miosis) is the most sensitive measure of opioid effects at subanesthetic drug concentra-tions, and was used as an objective measure of opioid effect. Sensitivity to remifentanil was assessed using pupillometry, and also respiratory rate and end-expired carbon dioxide in pediatric patients with and without obstructive sleep apnea.
Materials and Methods
Patients and Clinical Protocol
This study was approved by the Washington University in St. Louis Institutional Review Board. Eligible subjects were children, 8 to 14 yr of age, undergoing an elective
procedure requiring general anesthesia. Exclusion criteria were an inability to cooperate with study requirements (e.g., IV placement, sitting quietly, or pupillometry). Patients’ par-ents or legal guardian provided written informed consent and patients provided written assent. Two cohorts of chil-dren were studied: those with obstructive sleep apnea and those without obstructive sleep apnea. Children were con-sidered to have obstructive sleep apnea based on their chief complaint, history, and rationale for surgery as documented in the operative surgeon’s preoperative note which stated the indication for surgery as obstructive sleep apnea. Within this group, 9 out of 15 children (60%) presenting for tonsil-lectomy for obstructive sleep apnea had an overnight sleep laboratory polysomnogram, and all confirmed the diagnosis of obstructive sleep apnea. The remaining six children had at least two of the following: snoring, witnessed breathing pauses or gasping for breath, restless sleep, or daytime som-nolence (table 1). In addition, all children with obstruc-tive sleep apnea carried the International Classification of Diseases, Tenth Revision (ICD10) billing codes for Sleep Apnea, Unspecified (G47.30) or Obstructive Sleep Apnea (G47.33) in their medical record.
Children were classified as non–obstructive sleep apnea if they presented for tonsillectomy with or with-out adenoidectomy with a preoperative diagnosis of Acute Recurrent, or Chronic Tonsillitis (ICD10 codes J03.91 and J35.01), but not obstructive sleep apnea, or if they presented for a procedure requiring general anesthesia and did not have any medical history of obstructive sleep apnea. The medical record of non–obstructive sleep apnea children was assessed for sleep studies and signs and symptoms of
table 1. Data Supporting the Diagnosis of Obstructive Sleep Apnea.
Patient no.SleepStudy
aHi (episodes
per Hr)SPo2
nadir (%)oSa
Severity Snoring
Breathing Pause or Gasping
restlessSleep
Poorlyrested
daytime Somnolence
nocturnal eneuresis
Behavioral issues
1 X X Unk Unk Unk Unk Unk2 X 8.1 90 Moderate X X Unk Unk Unk Unk Unk3 X 34.9 74 Severe X Unk Unk Unk X X Unk4 X No X X Unk Unk No5 X 46.9 81 Severe X Unk Unk X X Unk X6 X X Unk X X Unk Unk7 X X Unk Unk Unk No Unk8 X 3.5 90 Mild X X Unk Unk Unk Unk Unk9 X 4.8 94 Mild X X Unk Unk X Unk Unk10 X X Unk Unk Unk Unk Unk11 X 6.3 84 Moderate X X X Unk X X Unk12 X No X X X Unk No13 X 22.1 92 Severe X X X X Unk Unk Unk14 X 10.5 90 Severe X X X Unk X No No15 X 14.0 84 Severe X X X X X X XTotal 9 15 9 5 6 7 2 2% 60% 100% 60% 33% 40% 47% 13% 13%
The AHI is reported to 0.1 episodes per hr, and severity is based on the AHI as mild (1 to 5), moderate (6 to 10), and severe (≥11). “No” indicates patient was queried and the request was denied by patient and/or family; “X” indicates yes; “Unk” indicates that the patient was not queried.AHI, apnea-hypopnea index; OSA, obstructive sleep apnea.
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

Anesthesiology 2019; 130:00–00 3
Opioid-induced Miosis Is Unaltered by Obstructive Sleep Apnea
Montana et al.
obstructive sleep apnea. One child in the non–obstructive sleep apnea group did exhibit snoring, however this child also had received a sleep study that indicated the absence of obstructive sleep apnea with an Apnea–Hypopnea Index of 0. None of the other children in the non–obstructive sleep apnea group had snoring, witnessed breathing pauses or gasping for breath, restless sleep, or daytime somnolence described as symptoms in their operative surgeon’s preop-erative note.
The study was conducted in the patient’s preoperative holding room prior to surgery. Anesthesia and surgical care were not altered for this study, except that a second 20-gauge preoperative IV catheter was placed in the ante-cubital fossa for venous blood sampling (one preoperative IV catheter is standard of care for this age group at our insti-tution). Following IV placement, heart rate, pulse oximetry, blood pressure, and nasal cannula end-expired carbon diox-ide monitors were placed. Patients breathed room air.
A remifentanil infusion was started and maintained for 15 min at a continuous rate of either 0.05, 0.1, or 0.15 μg · kg-1 · min-1. These doses were chosen to target remifentanil plasma concentrations 0.1 to 3 ng/ml, because pupil con-striction is maximum at plasma concentrations greater than 3 ng/ml.18 Remifentanil was administered based on ideal body weight.19 Ideal body weight was calculated as ([2.3 kg × height (inches) > 60] + 45.5 kg [females] or 50 kg [males]). Patients’ actual weight was used if they were less than the calculated ideal body weight. A cycled, dose escalation par-adigm was used. The first patient in each group received 0.05 μg · kg-1 · min-1, the second: 0.1 μg · kg-1 · min-1, the third: 0.15 μg · kg-1 · min-1, then the dose escalation repeated (i.e., patient four received 0.05 μg · kg-1 · min-1). Each dose group consisted of five patients with obstruc-tive sleep apnea and five patients without obstructive sleep apnea for a total of 15 patients each in the obstructive sleep apnea and non–obstructive sleep apnea groups.
Dark adapted infrared pupillometry was performed using binocular infrared pupilometers mounted in light occlusive goggles sampling at 100 Hz. The goggles were paired to a digital eye tracking system that fixates on the pupils (I-Portal, Neuro Kinetics, Inc., USA). Pupil area in pixels was continuously recorded during the study, and later averaged into 10-s bins. Data from both eyes were averaged. Baseline pupil size was defined as the average of the first 30 s of recording. Time-specific pupil size was the average area in the 30 s preceding each blood draw. Fractional pupil size was the time-specific area divided by the baseline pupil area. To measure plasma concentrations of remifentanil, 3 ml blood were drawn at 0, 1, 2, 4, 6, 10, and 15 min following the beginning of the remifentanil infusion.
Respiratory monitoring was performed using nasal cannula and end-expired carbon dioxide monitoring via a Capnostream 20 Bedside Monitor (Medtronic, USA). End-expired carbon dioxide and respiratory rate were recorded before, and 1, 2, 4, 6, 10, and 15 min after starting the
remifentanil infusion. Respiratory depression was defined as a respiratory rate less than 8, or oxygen saturation less than 90%. Data regarding altered mental status (e.g., confusion, disorientation, or hallucinations), excessive sedation (failure of the patient to respond to their name called loudly), and any need for external airway support (e.g., jaw thrust, oral or nasal airway insertion, mask ventilation, or intubation) were also collected. Following the 15-min assessment period, the remifentanil infusion was stopped. The patient then pro-ceeded with the planned surgery.
Analytical
To prevent ex vivo remifentanil metabolism, blood was immediately injected into potassium EDTA vacutainers (BD Vacutainer, USA) and plasma separation, acidification, and −80°C storage were performed within an hour of blood draw.20 Samples were centrifuged at 3,000 rotations per minute at 4°C for 5 min to separate plasma. Plasma (500 μl) was acidified with 3 μl of a nearly saturated 1 g/ml citric acid solution and stored at −80°C until analysis. All samples were analyzed within 3 months of collection.
Venous plasma remifentanil concentrations were deter-mined by liquid chromatography-tandem mass spectrom-etry, using a modification of a previous method.20 Protein precipitation was used to prepare samples. An aliquot of 100 μl of thawed patient plasma, calibrator, or quality control plasma was pipetted into discrete wells of a 96-well 2.2-ml polypropylene plate. Fentanyl internal standard (10 μl of 25 ng/ml; Cerilliant, USA), and 300 μl of methanol was added to each sample. The plate was capped and samples were mixed on a plate shaker for 1 min. The plate was then centrifuged at 6,100 rotations per minute for 15 min at 4°C in a Beckman Coulter Ultracentrifuge using a JS-13 rotor. After centrifugation, 200 μl of supernatant was transferred to a new 96-well 0.45-ml polypropylene plate.
Analysis was performed on a triple-quadrupole mass spec-trometer (6,500, AB Sciex, Ontario, Canada) equipped with a Turbo Ion Spray ionization source using positive polar-ity and multiple reaction monitoring. The chromatography system was a Shimadzu (USA) Prominence HPLC system consisting of two LC-20AD XR pumps with a CTO-20AC oven, a SIL-20AC XR auto-sampler, a DGU-20A
5R degas-
ser, and a CBM-20A controller. Chromatographic separa-tion was performed using a Gemini C-18 analytical column (50 × 2.0 mm, 3µm) with a Gemini C-18 SecurityGuard column (4 × 2.0 mm; Phenomenex, USA). The injection volume was 5 μl and the oven temperature was 25°C. Before each injection the needle was washed with metha-nol. Mobile phase (0.5 ml/min) was (A) 0.1% formic acid in water and (B) 0.1% formic acid in acetonitrile. The gradient used was 10% B held for 0.5 min and then increased lin-early to 80% during the next 2.5 min. B was then immedi-ately re-equilibrated back to 10%. Under these conditions, retention time for remifentanil and fentanyl were 2.2 and 2.5 min respectively. Both Q1 and Q3 quadrupoles were
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

4 Anesthesiology 2019; 130:00–00 Montana et al.
PerioPerative Medicine
optimized to unit mass resolution. Instrument parameters were: curtain gas, 20; ion spray voltage, 5,000 V; source tem-perature, 450°C; gas 1/nebulizer gas, 40; gas 2, 40; collision gas, 9 V, and entrance potential, 10 V. For remifentanil col-lision cell exit potential was 4 V, declustering potential 61 V, and collision energy 21 V. For fentanyl collision cell exit potential was 2 V, declustering potential 91 V, and collision energy 31 V. Multiple reaction monitoring transitions were m/z 377.2 is greater than 317.1 for remifentanil and 337.2 is greater than 188.1 for fentanyl with 150-ms dwell times. Remifentanil plasma calibration standards were 0.25, 0.5, 0.75, 1, 2.5, 5, 10, and 20 ng/ml. Remifentanil plasma qual-ity control samples were 0.5, 2.5, and 10 ng/ml. Interday coefficients of variation were 9, 6, and 7% for 0.5, 2.5, and 10 ng/ml remifentanil.
Remifentanil-miosis Concentration-effect Relationship
Miotic effect as a fractional change from baseline versus remifentanil concentration was analyzed using nonlin-ear regression with global curve fitting (SigmaPlot; Systat Software, USA). A three-parameter sigmoid inhibitory-E
Max
logistic function was used:
E(r) = EMax
×(1–(rγ/(rγ+EC50γ))
where E(r) is the effect at remifentanil concentration r; E
Max is the maximum pupillary constriction produced by
remifentanil; r is the remifentanil concentration in ng/ml; and γ is the shape parameter that determines the steepness of the concentration effect relationship.
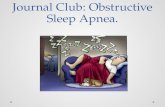
resultsBetween September 1, 2015, and October 31, 2017, 507 records of patients aged 8 to 14 yr were assessed for eligibil-ity. Of these, 87 met screening criteria and were approached for participation. Details of screening and enrollment are shown in figure 1. Thirty-three patients agreed to par-ticipate. Blood draw failed in three patients; a total of 30 patients underwent a remifentanil infusion and assessment.
Patient demographics are shown in table 2. The obstruc-tive sleep apnea cohort consisted exclusively of children undergoing tonsillectomy (with or without adenoidec-tomy) for obstructive sleep apnea. The non–obstructive sleep apnea cohort consisted of children undergoing ade-notonsillectomy for chronic tonsillitis (four subjects), an interval appendectomy (one subject), circumcision (two subjects), excision of a preauricular cyst (one subject), inguinal hernia repair (two subjects), orchiopexy (two sub-jects), palatoplasty (one subject), and tympanoplasty (two subjects). No patient had been admitted to the hospital in the past 30 days and no patient was currently taking opioids.
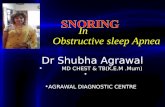
Measured remifentanil venous plasma concentrations through time are shown in figure 2. Pupillometry results are expressed as a fraction of baseline pupil area, and are shown in figure 3 as a function of time following the start of the remifentanil infusion. Remifentanil induced miosis occurred
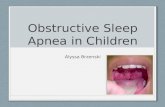
at all doses in both groups of patients. Fractional pupillary constriction as a function of remifentanil concentration from all dosing paradigms were pooled, and miosis was plotted as a function of measured remifentanil plasma concentration (fig. 4). The 95% CI generated from dose-response curves for both non–obstructive sleep apnea and obstructive sleep apnea patients were found to overlap (fig. 4).
Neither respiratory rate (fig. 5A), nor end-expired car-bon dioxide (fig. 5B) was appreciably altered in any of the patients during the 15-min remifentanil infusion. There were no serious adverse events. Table 3 summarizes the incidence of respiratory depression, low oxygen saturation, nausea, emesis, altered mental status, excessive sedation, and patients requiring airway support. The incidence of adverse events was not different between patients with and those without obstructive sleep apnea. One patient in the obstructive sleep apnea group that was administered 0.15 μg · kg-1 · min-1 remifentanil did have a respiratory rate of 7 breaths per minute at 10 min, however, their respiratory rate at 15 min was 11 breaths per minute.
discussionThis study tested the hypothesis that children with obstructive sleep apnea have an increased sensitivity to the miotic and respiratory depressant effects of the μ-opi-oid agonist remifentanil as compared to those without obstructive sleep apnea. When miosis was measured using dark adapted pupillometry, there was no difference in the remifentanil miosis concentration-effect curves between patients diagnosed with obstructive sleep apnea and those without obstructive sleep apnea. No differences in ven-tilatory parameters (end-expiratory carbon dioxide and respiratory rate) were seen between the groups, although it is likely that the infusion dose, duration, and resultant effect-site remifentanil concentrations, were insufficient to perturb ventilation. We chose to examine pupillary miosis because it is objectively quantifiable, is the most sensitive measure of opioid effect, and occurs at lower plasma concentrations than required for analgesia or respi-ratory depression.22 In addition, remifentanil miosis dose response curves have been shown to parallel respiratory depression dose response curves and inversely parallel arterial carbon dioxide dose–response curves.22 Studying μ-opioid induced miosis also allowed for the evaluation of the opioid dose-response relationship in children with and without obstructive sleep apnea, prior to any con-founding by sedative-hypnotics often administered before or coincident with general anesthesia. While remifentanil has unique pharmacokinetic properties, including rapid metabolism by endogenous blood and tissues esterases, it is a prototype μ-opioid agonist and results from our study should be generalizable to other opioids. Our results did not demonstrate any difference in the miotic effect of remifentanil in children either with or without sleep apnea. The doses and duration of remifentanil administered did
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

Anesthesiology 2019; 130:00–00 5
Opioid-induced Miosis Is Unaltered by Obstructive Sleep Apnea
Montana et al.
not perturb ventilatory parameters sufficiently to make clear conclusions regarding any differences between the two groups regarding sensitivity to opioid induced respi-ratory depression.
Given the previous reports that anesthetized children with obstructive sleep apnea are more likely to develop central apnea following a 0.5 μg/kg IV dose of fen-tanyl,23 and that recurrent hypoxemia is associated with an increased sensitivity to morphine,9,24 we expected to find an increased pharmacodynamic sensitivity to the miotic effect of remifentanil in children with obstructive sleep apnea. The miotic effect of remifentanil as a function of infusion duration for three different fixed-dose remifentanil infusions (0.05, 0.1, or 0.15 μg · kg-1 · min-1) demonstrated similar μ-opioid induced miosis in both obstructive sleep apnea and non–obstructive sleep apnea patients.
Simply evaluating remifentanil effect versus time curves shows earlier onset of miosis in obstructive sleep apnea patients, and might be interpreted as a greater opioid sen-sitivity. However, the measurement of remifentanil plasma concentrations enabled a pharmacodynamic analysis. This demonstrated indistinguishable miotic opioid dose-re-sponse relationships between obstructive sleep apnea and non–obstructive sleep apnea patients, and adds nuance to any conclusions that would be reached by viewing effect versus time alone. This illustrates the importance of mea-suring actual drug concentrations when performing drug- response studies.25
Measured remifentanil concentrations were higher and more variable in patients with obstructive sleep apnea. It is not immediately apparent why. The obstructive sleep apnea group in our study weighed more than the non–obstructive
Fig. 1. Participant flow diagram. OSA, obstructive sleep apnea.
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

6 Anesthesiology 2019; 130:00–00 Montana et al.
PerioPerative Medicine
sleep apnea group (66.1 kg vs. 48.3 kg). This is consistent with a previous study of nearly 500 children with obstructive sleep apnea presenting for adenotonsillectomy, which found that almost half of participants were overweight or obese.26 Due to obesity, we explicitly chose to dose based on ideal body weight. Remifentanil pharmacokinetics are similar in obese versus lean adults, and we expected pharmacokinet-ics to be similar in children.19 Nevertheless, inter-individual variability can lead to several-fold differences in predicted versus measured plasma drug concentrations, especially for short duration, non–steady state infusions.27,28 In addition,
recent evidence suggests that the Minto model21,29 used in our simulation may not be optimal for children.30 The rel-evant consideration is that discordance between expected versus measured remifentanil concentrations again illustrates
table 2. Demographic Characteristics
total(n = 30)
remifentanil
non-oSa(n = 15)
oSa(n = 15)
Age Mean ± SD 11 ± 2 11 ± 2 11 ± 2 Range 8–14 8–14 8–13Weight (kg) Mean ± SD 57.2 ± 24.9 48.3 ± 22.4 66.1 ± 24.8 Range 24.9–119.4 24.9–113.9 29.2–119.4Sex Female 10 (33.3%) 4 (26.7%) 6 (40.0%) Male 20 (66.7%) 11 (73.3%) 9 (60.0%)Race Caucasian 23 (76.7%) 12 (80.0%) 11 (73.3%) Black 6 (20.0%) 3 (20.0%) 3 (20.0%) Native American 1 (6.7%) 0 (0%) 1 (6.7%)
Values are n (%) unless otherwise noted. OSA, obstructive sleep apnea.
Fig. 2. Measured remifentanil plasma concentrations during a 15-min fixed dose infusion (0.05, 0.1, or 0.15 μg · kg-1 · min-1) in patients with obstructive sleep apnea (red symbols) and without obstructive sleep apnea (black symbols). Time is relative to the start of the remifentanil infusion. Results are show as the mean ± SD (n = 5 for each group).
Fig. 3. Remifentanil effects on dark-adapted pupil area and the influence of obstructive sleep apnea. Times are relative to the start of the remifentanil infusion. Pupil diameter (pixels) is shown relative to baseline area. Results are shown from a continuous dose infusion of either (A) 0.05, (B) 0.1, or (C), 0.15 μg · kg-1 · min-1. Black circles represent non–obstructive sleep apnea patients and red triangles represent obstructive sleep apnea patients. Results are presented as mean ± SD (n = 5 per group).
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

Anesthesiology 2019; 130:00–00 7
Opioid-induced Miosis Is Unaltered by Obstructive Sleep Apnea
Montana et al.
the importance of measuring actual drug concentrations when performing drug-response studies, lest observed clinical differences be misattributed as pharmacodynamic differences.25
There are several possible explanations for why no dif-ference was seen in remifentanil-induced miosis between obstructive sleep apnea and non–obstructive sleep apnea patients. Previous studies that suggest a difference in opioid sensitivity between children with and without obstructive sleep apnea have assumed similar pharmacokinetics with-out measuring actual opioid plasma concentrations.9,23,24 It is possible that pharmacokinetic rather than pharmacody-namic differences between the groups could account for the apparent difference in opioid sensitivity between children with and without obstructive sleep apnea. Another prob-able explanation is that different outcomes were used in this versus previous studies. We focused on miosis, the most sensitive measure of opioid effect, while others focused on respiratory depression. While miosis occurred at all three remifentanil doses administered, and venous plasma con-centrations less than 1 ng/ml, we did not see an appreciable change in either end-expired carbon dioxide or respiratory rate. The remifentanil dose range and duration, selected to avoid loss of consciousness or apnea, did not alter ven-tilatory parameters or induce sedation. However, during the concomitant administration of general anesthesia, chil-dren with obstructive sleep apnea had a higher incidence of apnea following a 0.5 µg/kg fentanyl bolus compared with non–obstructive sleep apnea children.23 Reduced
Fig. 4. Remifentanil effects on miosis. Measured remifentanil concentrations are presented on a log scale. Black circles repre-sent non–obstructive sleep apnea patients and red triangles rep-resent obstructive sleep apnea patients. The sigmoid inhibitory - EMax logistic function is plotted as a solid line for non–obstruc-tive sleep apnea patients and a dashed line for non–obstructive sleep apnea patients. Values below the lower limit of quantifica-tion are not shown. 95% confidence bands for each group are also plotted (grey for non–obstructive sleep apnea and red for obstructive sleep apnea).
Fig. 5. Remifentanil effects on (A) respiratory rate and (B) end-expired CO2. Measured remifentanil concentrations are pre-sented on a log scale. Black circles represent non-OSA patients and red triangles represent OSA patients. Data for all three doses were pooled and are presented for every measured remifentanil concentration. Values below the lower limit of quantification are not shown. 95% confidence bands for each group are also plot-ted (grey for non–obstructive sleep apnea and red for obstructive sleep apnea).
table 3. Adverse Events during Remifentanil Infusion
non-oSa (n = 15)
oSa (n = 15)
Respiratory rate < 8 0 1O2 < 90% 0 0Heart rate < 60/min 2 2Excessive sedation 1 0Altered mental state 0 0Re-intubation 0 0
OSA, obstructive sleep apnea.
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

8 Anesthesiology 2019; 130:00–00 Montana et al.
PerioPerative Medicine
posttonsillectomy morphine requirements have also been reported in children with severe obstructive sleep apnea.24 It is conceivable that altered opioid sensitivity in obstructive sleep apnea patients only occurs at the higher plasma con-centrations required for respiratory depression and seda-tion. Higher doses were not pursued in this study due to safety considerations. A third possibility is that greater sen-sitivity to opioids in obstructive sleep apnea occurs only in the presence of sedative-hypnotics, which was deliberately avoided in this opioid-specific protocol. Finally, a fourth possibility is a recognized limitation of this study, namely, the reliance on surgeon diagnosis to classify whether patients have obstructive sleep apnea, rather than formal polysomnography. Nonetheless, while our non–obstructive sleep apnea patients did not receive polysomnography, 60% of our obstructive sleep apnea patients did receive formal polysomnography demonstrating obstructive sleep apnea. Furthermore, a majority of children presenting for surgery have only a clinical diagnosis of obstructive sleep apnea, not one based on polysomnography, so these are the data available on which clinical decision are made. In this study, and inherent in the conduct of clinical pharmacology stud-ies in children, is difficulty with recruitment, and for prag-matic reasons, we did not universally use polysomnography for research purposes to diagnose the children in this study. Therefore, we did not categorize the severity of disease for all individuals in either cohort. Indeed, in our study a documented polysomnogram was only available for nine subjects and thus polysomnography incompletely informs our results. Lastly, it is possible that our obstructive sleep apnea patients simply did not have a severe enough disease phenotype to engender altered opioid sensitivity. Both ani-mal and human studies have implicated chronic intermit-tent hypoxemia as the driver for altered opioid sensitivity.31 Thus, perhaps only the most severe obstructive sleep apnea patients, i.e., those with nighttime hypoxemia, will experi-ence altered opioid sensitivity.
There are recognized limitations to this investigation. We intentionally did not perform polysomnography on all chil-dren and relied on surgeon practices, to simulate real world clinical practice for children with obstructive sleep apnea. Polysomnography is time consuming and expensive. Less than 10% of patients diagnosed with obstructive sleep apnea undergo polysomnography prior to surgery, even for tonsil-lectomy.32,33 Another limitation is that while opioid effects were studied in isolation, to specifically test the opioid– obstructive sleep apnea hypothesis, it is possible that postop-erative sensitivities may differ, due either to higher opioid doses or opioid interactions with anesthetics and sedative hypnotics. These possibilities merit further evaluation.
Given the high prevalence of obstructive sleep apnea, many children with obstructive sleep apnea will undergo surgical procedures that require opioid analgesia, includ-ing tonsillectomy. Tonsillectomy, while seemingly a minor procedure, is exquisitely painful. Therefore, opioid
analgesia is the mainstay of treatment for moderate to severe posttonsillectomy pain. Despite the perioperative use of opioids and other analgesic adjuncts, moderate to severe pain following tonsillectomy is common and can last for days.16 Treatment for posttonsillectomy pain is often insufficient or ineffective as evidenced by a recent survey where more than 40% of patients experience severe pain as defined as greater than or equal to 7 out of 10 on a numeric rating scale.34
The primary focus of this study was neither pain relief nor respiratory depression, but rather the miosis–remifen-tanil concentration effect relationship in children with and without obstructive sleep apnea. Indeed, it is not possible to extrapolate pupillometry as an explicit and perfect marker for either of these critical clinical end-points. In addition, our reliance on a nasal cannula for exhaled carbon dioxide concentrations may have limited our ability to quantify significant respiratory depression. Nevertheless, this study questions the notion that all chil-dren with a clinical diagnosis of obstructive sleep apnea are more sensitive to opioids.12,13 Further studies designed to directly test sensitivity to opioid-induced respiratory depression in this high-volume, vulnerable population, are clearly needed. In conclusion, we did not identify a difference in sensitivity to opioid induced miosis in chil-dren with and without a clinical diagnosis of obstructive sleep apnea.
Research Support
Supported by a Faculty Development Award from the Pharmaceutical Research and Manufacturers of America (PhRMA) Foundation (Washington, DC; to Dr. Montana) and the Washington University in St. Louis Department of Anesthesiology (St. Louis, Missouri).
Competing Interests
The authors declare no competing interests.
Correspondence
Address correspondence to Dr. Montana: Washington University School of Medicine, 660 South Euclid Avenue, Box 8054, St. Louis, Missouri 63110. [email protected]. Information on purchasing reprints may be found at www.anesthesiology.org or on the masthead page at the begin-ning of this issue. Anesthesiology’s articles are made freely accessible to all readers, for personal use only, 6 months from the cover date of the issue.
references
1. Brown KA: Outcome, risk, and error and the child with obstructive sleep apnea. Paediatr Anaesth 2011; 21:771–80
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

Anesthesiology 2019; 130:00–00 9
Opioid-induced Miosis Is Unaltered by Obstructive Sleep Apnea
Montana et al.
2. Marcus CL, Brooks LJ, Draper KA, Gozal D, Halbower AC, Jones J, Schechter MS, Ward SD, Sheldon SH, Shiffman RN, Lehmann C, Spruyt K; American Academy of Pediatrics: Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012; 130:e714–55
3. Bhattacharyya N, Lin HW: Changes and consistencies in the epidemiology of pediatric adenotonsillar sur-gery, 1996-2006. Otolaryngol Head Neck Surg 2010; 143:680–4
4. Friedman M, Wilson M, Lin HC, Chang HW: Updated systematic review of tonsillectomy and adenoidectomy for treatment of pediatric obstructive sleep apnea/hypopnea syndrome. Otolaryngol Head Neck Surg 2009; 140:800–8
5. De Luca Canto G, Pachêco-Pereira C, Aydinoz S, Bhattacharjee R, Tan HL, Kheirandish-Gozal L, Flores-Mir C, Gozal D: Adenotonsillectomy complications: a meta-analysis. Pediatrics 2015; 136:702–18
6. Coté CJ, Posner KL, Domino KB: Death or neurologic injury after tonsillectomy in children with a focus on obstructive sleep apnea: Houston, we have a problem! Anesth Analg 2014; 118:1276–83
7. Leong AC, Davis JP: Morbidity after adenotonsillec-tomy for paediatric obstructive sleep apnoea syndrome: Waking up to a pragmatic approach. J Laryngol Otol 2007; 121:809–17
8. McColley SA, April MM, Carroll JL, Naclerio RM, Loughlin GM: Respiratory compromise after ade-notonsillectomy in children with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg 1992; 118:940–3
9. Brown KA, Laferrière A, Lakheeram I, Moss IR: Recurrent hypoxemia in children is associ-ated with increased analgesic sensitivity to opiates. Anesthesiology 2006; 105:665–9
10. Wilson K, Lakheeram I, Morielli A, Brouillette R, Brown K: Can assessment for obstructive sleep apnea help predict postadenotonsillectomy respiratory com-plications? Anesthesiology 2002; 96:313–22
11. Patino M, Sadhasivam S, Mahmoud M: Obstructive sleep apnoea in children: Perioperative considerations. Br J Anaesth 2013; 111 Suppl 1:i83–95
12. Sadhasivam S, Chidambaran V, Ngamprasertwong P, Esslinger HR, Prows C, Zhang X, Martin LJ, McAuliffe J: Race and unequal burden of perioperative pain and opioid related adverse effects in children. Pediatrics 2012; 129:832–8
13. American Society of Anesthesiologists Task Force on Perioperative Management of Patients with Obstructive Sleep Apnea: Practice guidelines for the perioperative management of patients with obstruc-tive sleep apnea: An updated report by the American Society of Anesthesiologists Task Force on Perioperative Management of Patients with Obstructive Sleep Apnea. Anesthesiology 2014; 120:268–86
14. Kieran S, Gorman C, Kirby A, Oyemwense N, Lander L, Schwartz M, Roberson D: Risk factors for desatu-ration after tonsillectomy: Analysis of 4092 consecutive pediatric cases. Laryngoscope 2013; 123:2554–9
15. Chung SA, Yuan H, Chung F: A systemic review of obstructive sleep apnea and its implications for anes-thesiologists. Anesth Analg 2008; 107:1543–63
16. Schwengel DA, Sterni LM, Tunkel DE, Heitmiller ES: Perioperative management of children with obstruc-tive sleep apnea. Anesth Analg 2009; 109:60–75
17. Laferrière A, Liu JK, Moss IR: Neurokinin-1 versus mu-opioid receptor binding in rat nucleus tractus sol-itarius after single and recurrent intermittent hypoxia. Brain Res Bull 2003; 59:307–13
18. Barvais L, Engelman E, Eba JM, Coussaert E, Cantraine F, Kenny GN: Effect site concentrations of remifentanil and pupil response to noxious stimulation. Br J Anaesth 2003; 91:347–52
19. Egan TD, Huizinga B, Gupta SK, Jaarsma RL, Sperry RJ, Yee JB, Muir KT: Remifentanil pharmacokinetics in obese versus lean patients. Anesthesiology 1998; 89:562–73
20. Koster RA, Vereecke HE, Greijdanus B, Touw DJ, Struys MM, Alffenaar JW: Analysis of remifentanil with liquid chromatography-tandem mass spectrometry and an extensive stability investigation in EDTA whole blood and acidified EDTA plasma. Anesth Analg 2015; 120:1235–41
21. Minto CF, Schnider TW, Egan TD, Youngs E, Lemmens HJ, Gambus PL, Billard V, Hoke JF, Moore KH, Hermann DJ, Muir KT, Mandema JW, Shafer SL: Influence of age and gender on the pharmacokinet-ics and pharmacodynamics of remifentanil. I. Model development. Anesthesiology 1997; 86:10–23
22. Rollins MD, Feiner JR, Lee JM, Shah S, Larson M: Pupillary effects of high-dose opioid quantified with infrared pupillometry. Anesthesiology 2014; 121:1037–44
23. Waters KA, McBrien F, Stewart P, Hinder M, Wharton S: Effects of OSA, inhalational anesthesia, and fen-tanyl on the airway and ventilation of children. J Appl Physiol (1985) 2002; 92:1987–94
24. Brown KA, Laferrière A, Moss IR: Recurrent hypox-emia in young children with obstructive sleep apnea is associated with reduced opioid requirement for anal-gesia. Anesthesiology 2004; 100:806–10; discussion 5A
25. Avram MJ: In reply: presenting data versus predic-tions as basic scientific information: Target-controlled infusions versus microgram per kilogram per minutes. Anesthesiology 2011; 114:723; author reply 721–3
26. Marcus CL, Moore RH, Rosen CL, Giordani B, Garetz SL, Taylor HG, Mitchell RB, Amin R, Katz ES, Arens R, Paruthi S, Muzumdar H, Gozal D, Thomas NH, Ware J, Beebe D, Snyder K, Elden L, Sprecher RC, Willging
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019

10 Anesthesiology 2019; 130:00–00 Montana et al.
PerioPerative Medicine
P, Jones D, Bent JP, Hoban T, Chervin RD, Ellenberg SS, Redline S; Childhood Adenotonsillectomy Trial (CHAT): A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med 2013; 368:2366–76
27. Struys MM, Coppens MJ, De Neve N, Mortier EP, Doufas AG, Van Bocxlaer JF, Shafer SL: Influence of administration rate on propofol plasma-effect site equilibration. Anesthesiology 2007; 107:386–96
28. Fisher DM: Take it to the limit (one more time). Anesthesiology 2007; 107:367–8
29. Minto CF, Schnider TW, Shafer SL: Pharmacokinetics and pharmacodynamics of remifentanil. II. Model application. Anesthesiology 1997; 86:24–33
30. Eleveld DJ, Proost JH, Vereecke H, Absalom AR, Olofsen E, Vuyk J, Struys MMRF: An allome-tric model of remifentanil pharmacokinetics and pharmacodynamics. Anesthesiology 2017; 126:1005–18
31. Lerman J: Unraveling the mysteries of sleep-disor-dered breathing in children. Anesthesiology 2006; 105:645–7
32. Friedman NR, Perkins JN, McNair B, Mitchell RB: Current practice patterns for sleep-disordered breath-ing in children. Laryngoscope 2013; 123:1055–8
33. Roland PS, Rosenfeld RM, Brooks LJ, Friedman NR, Jones J, Kim TW, Kuhar S, Mitchell RB, Seidman MD, Sheldon SH, Jones S, Robertson P; American Academy of Otolaryngology—Head and Neck Surgery Foundation: Clinical practice guideline: Polysomnography for sleep-disordered breathing prior to tonsillectomy in children. Otolaryngol Head Neck Surg 2011; 145(1 Suppl):S1–15
34. Guntinas-Lichius O, Geißler K, Komann M, Schlattmann P, Meissner W: Inter-Hospital variability of postoperative pain after tonsillectomy: Prospective registry-based multicentre cohort study. PLoS One 2016; 11:e0154155
Copyright © 2019, the American Society of Anesthesiologists, Inc. Wolters Kluwer Health, Inc. Unauthorized reproduction of this article is prohibited.Downloaded from anesthesiology.pubs.asahq.org by ASA, Vicki Tedeschi on 03/11/2019