Rabakir 25 mg, 50 mg, 75 mg, 100 mg, 150 mg, 200 mg, 300 mg ...

Patient Name:Pain Diagnosis:Date of Onset:
Overdose Risk
Item (circle all that apply)
1. Family History of Substance Abuse:
Alcohol Illegal Drugs Prescription Drugs
2. Personal History of Substance Abuse:
Alcohol Illegal Drugs Prescription Drugs
3. Age (mark box if 16-45)4. History of Preadolescent
Sexual Abuse5. Psychological Disease
Attention Deficit Disorder,Obsessive-Compulsive Disorder,or Bipolar, SchizophreniaDepression
Total Total Score Risk Category:
Low Risk: 0 to 3, Moderate Risk: 4 to 7, High Risk: 8 and above
124
3451
3
2
1
334
3451
0
2
1
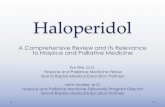
Opioid Risk ToolBy Lynn R. Webster MD
Item scoreif female
Item scoreif male
Initiation Trial ChartDateOpioid prescribed Daily dose Daily morphine equivalent
More than 200Less than 200
Goals achieved Yes, No, PartiallyPain intensity Functional status Improved, No Change, WorsenedAdverse effects Nausea
ConstipationDrowsinessDizziness/VertigoDry skin/PruritisVomitingOther?
Complications? (Reviewed: Y/N)Aberrant Behaviour (Reviewed: Y/N)Urine Drug Screening (Y/N)Other Medications
Initiation ChecklistAre opioids indicated for this pain condition
Explained potential benefits
Explained adverse effects
Explained risks
Patient given information sheet
Signed treatment agreement (as needed)
Urine drug screening (as needed)
Y N Date
0 = None 1 = Limits ADLs
2 = Prevents ADLs
Provider Factors- Incomplete assessments- Rapid titration- Combining opioids and
sedating drugs- Failure to monitor dosing- Insufficient information
given to patient and/or relatives
Mild-to-Moderate PainFirst- line: codeine or tramadol
Second-line: morphine, oxycodone or hydromorphone
Severe Pain
First-line: morphine, oxycodone or hydromorphone
Second-line: fentanylThird-line: methadone
Stepped Approach to Opioid Selection Patient Factors
- Elderly- On benzodiazepines- Renal impairment- Hepatic impairment- COPD- Sleep apnea- Sleep disorders- Cognitive impairment
The Opioid Manager is designed to be used as a point of care tool for providers prescribing opioids for chronic non cancer pain. It condenses key elements from the Canadian Opioid Guideline and can be used as a chart insert.
Goals decided with patient:
Watchful Dose > than 200
To access the Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-cancer Pain and to download the Opioid Manager visit http://nationalpaincentre.mcmaster.ca/opioid/
Opioid Factors
- Codeine & Tramadol - lower risk - CR formulations - higher doses than IR
Prevention- Assess for Risk Factors- Educate patients /families about risks
& prevention
- Start low, titrate gradually, monitor frequently
- Careful with benzodiazepines- Higher risk of overdose - reduce initial
dose by 50%; titrate gradually- Avoid parenteral routes- Adolescents; elderly - may need
consultation- Watch for Misuse
OPIOID MANAGEROPIOID MANAGER
Before You Write the First ScriptA
Initiation TrialB A closely monitored trial of opioid therapy is recommended before deciding whether a patient is prescribed opioids for long term use.
Opioid
Codeine (alone or incombination withacetaminophen or ASA)
CR Codeine
Tramadol (37.5 mg) +acetaminophen (325 mg)
CR Tramadol
IR Morphine
CR Morphine
IR Oxycodone
CR Oxycodone
IR Hydromorphone
CR Hydromorphone
Initial dose
15-30 mg q.4 h. as required
50 mg q.12 h.
1 tablet q.4-6 h. as needed up to 4/day
a) Zytram XL®: 150 mg q. 24 h.b) Tridural™: 100 mg q. 24 h.c) Ralivia™: 100 mg q. 24 h.
5-10 mg q. 4 h. as neededmaximum 40 mg/day10-30 mg q.12 h.Kadian®: q.24 h. Kadian® should not be started inopioid-naïve patients
5-10 mg q. 6 h. as neededmaximum 30 mg/day10-20 mg q.12 h.maximum 30 mg/day1-2 mg q. 4-6 h. as neededmaximum 8 mg/day3 mg q. 12 h.maximum 9 mg/day
Minimum time interval for increase7 days
2 days
7 days
a) 7 daysb) 2 daysc) 5 days
7 days
Minimum 2 days,recommended: 14 days
7 days
Minimum 2 days,recommended: 14 days
7 days
Minimum 2 days,recommended: 14 days
Suggesteddose increase
15-30 mg/day up to maximum of 600 mg/day (acetaminophen doseshould not exceed 3.2 grams/day)
50 mg/day up to maximum of 300 mg q.12 h.
1-2 tab q. 4-6 h. as needed up to maximum 8 tablets/day
Maximum doses:a) 400 mg/dayb) 300 mg/dayc) 300 mg/day
5-10 mg/day
5-10 mg/day
5 mg/day
10 mg/day
1-2 mg/day
2-4 mg/day
Minimum daily dosebefore converting IR to CR
100 mg
NA
3 tablets
NA
20-30 mg
NA
20 mg
NA
6 mg
NA
Suggested Initial Dose and Titration (Modified from Weaver M., 2007 and the e-CPS, 2008) Notes: The table is based on oral dosing for CNCP.Brand names are shown if there are some distinct features about specific formulations. Reference to brand names as examples does not imply endorsement ofany of these products. CR = controlled release, IR = immediate release, NA = not applicable, ASA: Acetylsalicylic Acid D / M / Y D / M / Y D / M / Y D / M / Y
Feb 2011

Opioid
MorphineCodeineOxycodoneHydromorphoneMeperidineMethadone & Tramadol
Transdermal fentanyl
Equivalent Doses (mg)
30200206
300
Conversionto MEQ
10.151.55
0.1
Switching Opioids:
Aberrant Drug Related Behaviour (Modified by Passik,Kirsh et al 2002).
Maintenance & Monitoring Chart
DateOpioid prescribed Daily dose Daily morphine equivalent
More than 200Less than 200
Goals achieved Yes, No, PartiallyPain intensity Functional status Improved, No Change, WorsenedAdverse effects Nausea
ConstipationDrowsinessDizziness/VertigoDry skin/PruritisVomitingOther?
Complications? (Reviewed: Y/N)Aberrant Behaviour (Reviewed: Y/N)Urine Drug Screening (Y/N)Other Medications
Morphine Equivalence Table
Dose Equivalents unreliable
60 – 134 mg morphine = 25 mcg/h135 – 179 mg = 37 mcg/h180 – 224 mg = 50 mcg/h225 – 269 mg = 62 mcg/h270 – 314 mg = 75 mcg/h315 – 359 mg = 87 mcg/h360 – 404 mg = 100 mcg/h
0 = None 1 = Limits ADLs
2 = Prevents ADLs
If previous opioiddose was:
Then, SUGGESTEDnew opioid dose is:
High
Moderate or low
50% or less of previous opioid (converted to morphine equivalent)
60-75% of the previous opioid (converted to morphine equivalent)
Maintenance & MonitoringC
When is it time to Decrease the dose or Stop the Opioid completely?D
To access the Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-cancer Pain and to download the Opioid Manager visit http://nationalpaincentre.mcmaster.ca/opioid/
Watchful Dose > than 200
* = behaviours more indicative of addiction than the others.
How to Stop – the essentialsHow do I stop? The opioid should be tapered rather than abruptly discontinued.
How long will it take to stop the opioid? Tapers can usually be completed between 2 weeks to 4 months.
When do I need to be more cautiouswhen tapering? Pregnancy:Severe, acute opioid withdrawal has been associated with premature labour and spontaneous abortion.
How do I decrease the dose?Decrease the dose by no more than 10% ofthe total daily dose every 1-2 weeks. Onceone-third of the original dose is reached, decrease by 5% every 2-4 weeks. Avoid sedative-hypnotic drugs, especially benzodiazepines, during the taper.
When to stop opioids
Pain Condition Resolved
Risks Outweighs Benefits
Adverse Effects Outweighs Benefits
Medical Complications
Opioid Not Effective
Examples and Considerations
Patient receives definitive treatment for condition. A trial of tapering is warranted to determine if the original pain condition has resolved.
Overdose risk has increased.Clear evidence of diversion.Aberrant drug related behaviours have become apparent.
Adverse effects impairs functioning below baseline level.Patient does not tolerate adverse effects.
Medical complications have arisen (e.g. hypogonadism, sleep apnea, opioid induced hyperalgesia)
Opioid effectiveness = improved function or at least 30% reduction in pain intensityPain and function remains unresponsive.Opioid being used to regulate mood rather than pain control.Periodic dose tapering or cessation of therapy should be considered to confirm opioid therapy effectiveness.
Indicator*Altering the route of delivery*Accessing opioids from other sources
Unsanctioned use
Drug seeking
Repeated withdrawal symptoms
Accompanying conditions
Social features
Views on the opioidmedication
Examples• Injecting, biting or crushing oral formulations• Taking the drug from friends or relatives• Purchasing the drug from the “street”• Double-doctoring• Multiple unauthorized dose escalations• Binge rather than scheduled use• Recurrent prescription losses• Aggressive complaining about the need for higher doses• Harassing staff for faxed scripts or fit-in appointments• Nothing else “works”
• Marked dysphoria, myalgias, GI symptoms, craving
• Currently addicted to alcohol, cocaine, cannabis or other drugs• Underlying mood or anxiety disorders not responsive to treatment• Deteriorating or poor social function• Concern expressed by family members
• Sometimes acknowledges being addicted• Strong resistance to tapering or switching opioids• May admit to mood-leveling effect• May acknowledge distressing withdrawal symptoms
D / M / Y D / M / Y D / M / Y D / M / Y D / M / Y D / M / Y
National Opioid Use Guideline Group (NOUGG)





North Kingston Community Health Centre
Family Medicine Clinic
Subject: POLICY FOR THE MANAGEMENT OF PAIN WITH OPIOID ANALGESICS
Date: April 2011
Opioid analgesia for chronic pain must take into consideration of the risks and benefits. Universal precautions are recommended when using these medications for pain management. There is a high risk of diversion and addiction with narcotic medication. From a population perspective, these medications need to be prescribed in a controlled manner.
Chronic pain and mental health issues may also overlap. Appropriate mental health care can be an essential component of chronic pain management. A focus on pain issues may divert attention from management of underlying mental health issues.
1. Prior to initiation of narcotics:
Diagnosis is confirmed and a full physical exam, past medical history, social history,
psychiatric history and substance abuse history has been completed.
A careful screen for liver disease, renal disease, COPD, sleep apnea, other sleep
disorders and cognitive disorders has been conducted.
Less addictive medications have been tried first as per WHO ladder.
An opiate risk assessment screening tool has been completed (see appendix 1).
A treatment agreement has been signed with the prescribing physician (see appendix 2).
A single pharmacy has been appointed by the patient and all prescriptions will be faxed
directly there.
Written and verbal information has been given to the patient re all side effects of
narcotics and reasons for narcotic discontinuation.
A pain assessment tool has been filled out by patient to more objectively track whether
improvement has occurred with the opioid trial ; goal being 30% reduction of symptoms
or 30% improvement in function (see appendix 3).
The terms of opioid therapy have been clarified with patient (ie an opioid trial to aid
with chronic pain symptoms or a short-term treatment agreement for an acute
problem).
Consider tapering benzodiazepines before initiating opioids (especially in elderly).
Active polysubstance abuse is a contraindication to prescribing opioids.
Urine toxicology must be free of polysubstance abuse * 3 prior to assessment by
physician for consideration of opioid analgesics.
Patients have been told to avoid driving when first initiating opioid therapy or after a
dose increase and that they should not have alcohol, benzodiazepines, or other sedating
medications.

2. Choice of opiods:
Weaker opioids such as codeine and tramadol will be first line. (Tramadol is associated
with seizures in patients at high seizure risk. Codeine taken by breast-feeding women
has been associated with fatal opioid toxicity in neonates). *Note Tramadol is not
covered by ODB.
For chronic pain, long-acting formulations are preferred.
In light of the increasing evidence of addiction, diversion risk, and morbidity with
oxycontin, oxycontin will not be prescribed at North Kingston Community Health Centre.
All patients currently on oxycontin will be switched to morphine if there is no history of
renal dysfunction. The morphine equivalent dose will be calculated and reduced by 50%
due to incomplete cross tolerance between opioids. (See appendix 5 and 6).
In patients with renal dysfunction for whom a physician wishes to prescribe a strong
opioid, hydromorphone will be utilized. Use with caution in patients at higher risk of
opioid misuse as it has a higher abuse potential than morphine.
Fentanyl can also be considered if a patient has been on 60-90 mg morphine a day
equivalence for 14 days. Do not use in patient with pre-existing respiratory disease.
Demerol will not be prescribed for CNCP.
For patients with non-cancer chronic pain (NCCP) who are addicted to opioids, they will
be offered methadone or buprenorphine treatment.
If addiction history is remote and an opioid trial is warranted, do not prescribe the same
opioid they were previously addicted to.
3. Monitoring of patients on opioids:
Repeat pain assessment tools will be utilized.
Follow-up will be every 1-2 weeks when initiating opioids and patients on stable doses
will be assessed at a minimum of every 3 months.
There are no early refills and fax refill requests will be denied.
Increases in doses occur with patient visits only.
Aberrant drug-seeking behaviour witnessed by any staff should be documented and the
prescribing physician should be notified (ie unauthorized dose escalation, lost
prescriptions, harassing staff for fit-in appointments or faxed scripts or early refills,
admission of buying from street or altering form of delivery).
Patients will be advised to bring in medication at each visit so that pill counts may be
done.
No patient with NCCP will be above 200 mg/day of morphine equivalent without chronic
pain specialist input.
Urine drugs are performed periodically (immunoassay detects drugs for longer period of
time: 5-7 days while chromatography can specifically identify the medication being

prescribed.) prescribed.) *Routine urine drug screen does not screen for oxycodone,
this must be specifically requested. 25 ml at minimun is needed for urine drug screen
(see appendix 4).
If suspect tampering of urine, check urine sample immediately afterwards to see if it is warm and a urine creatinine can be ordered (less than 2-3 mmol per L suggests dilution). *As well, there are temperature strips that can be purchased and stuck on urine bottles to ensure appropriate urine temperature at 4 mins post-collection.
Carefully assess for any aberrant drug-seeking behaviors.
4. Ending an opioid prescription:
Patient experiences insufficient analgesia after 2-3 dose increases (less than 30% goal)
Patient has unacceptable adverse events (nausea, constipation, drowsiness, dizziness or
vertigo, dry skin, pruitus , vomiting, etc) or medical complications.
There is evidence of clinical or functional instability: missed appointments, failure to
follow through with specialist appointments, failure to comply with required
investigations, urine toxicology indicative of polysubstance abuse or treatment contract
parameters have been breached.
References:
1. `` Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain``,
NOUGG, April 30, 2010.
2. ``Universal Precautions Revisited: Managing the Inherited Pain Patient``, Gourlay et al., Pain
Medicine, Volume 10 S2, 2009.

Appendix 1: Opiate Risk Assessment Tool
Item Mark each box
that applies
Item score if
female
Item score
if male
1. Family History of Substance Abuse:
Alcohol [ ] 1 3
Illegal Drugs [ ] 2 3
Prescription Drugs [ ] 4 4
2. Personal History of Substance Abuse:
Alcohol [ ] 3 3
Illegal Drugs [ ] 4 4
Prescription Drugs [ ] 5 5
3. Age (mark box if 16-45) [ ] 1 1
4. History of Preadolescent Sexual Abuse [ ] 3 0
5. Psychological Disease
Attention Deficit Disorder, Obsessive-Compulsive Disorder, or Bipolar, Schizophrenia
[ ] 2 2
Depression [ ] 1 1
Total ____ ____
Total Score Risk Category: Low Risk: 0 to 3 Moderate Risk: 4 to 7 High Risk: 8 and above
— Attribution: By Lynn R. Webster, MD; Medical Director of Lifetree Medical, Inc., Salt Lake
City, UT 84106

Appendix 2: Sample Opioid Treatment Contract
TREATMENT AGREEMENT FOR THE MANAGEMENT OF PAIN WITH THE OPIOD ANALGESICS:
I understand I am receiving my opioid medication from Dr. _____________ to treat my pain condition. This medication works to relieve pain and improve sleep disturbances caused by pain. There is a high potential for abuse and therefore this substance is regulated. To insure my safety and minimize abuse potential I agree to the following conditions:
I understand the significant side effects of opioids which include but are not limited to nausea, vomiting, constipation, impaired judgment, decreased libido, respiratory depression and death if used improperly or combined with other medications/illicit drugs or alcohol.
I understand drowsiness may occur when starting opioid therapy or when increasing the dosage. I agree to refrain from operating a vehicle or machinery until such drowsiness disappears.
I understand the use of any mood-altering substance, like tranquilizers, sleeping pills, alcohol, illicit drugs (marijuana, cocaine, heroin or hallucinogens), may have serious negative side effects and may interfere with opioid therapy.
I understand using any amount of alcohol or illicit drugs while on opioid medications may result in serious harm to myself, including death.
I understand I am receiving opioid medication from only Dr._________________ to treat my pain condition.
I understand the treatment goal is not to eliminate pain but to improve my ability to function and my overall quality of life.
I will not seek pain medications from another physician. Only Dr. __________ will prescribe opioids for me.
I consent to open communication between my doctor and any other health professionals involved in my pain management, including pharmacists, other physicians, emergency departments, etc.
I agree to attend all appointments, treatments and consultations as requested by my physician. If I am unable to comply with these requests and miss

appointments I understand my physician may cease to prescribe opioids to me.
I will not give away or sell my medication to anyone else, including family members; nor will I accept any medication from anyone else.
I will not take opioid medications in larger amounts or more frequently than prescribed by my physician.
I agree to be responsible for the secure storage of my medication at all times.
I will not use over the counter opioid medications (Tylenol #1, 222’s etc).
I understand if my prescription runs out early for ANY reason (for example, the medications are lost, stolen or taken more often than prescribed) Dr. ________________________ will NOT prescribe extra medications for me or renew my prescription early. I will have to wait until my next prescription is due.
I understand I will be required to leave weekly or random urine samples for toxicology screening and if not left my opioid prescription may not be renewed.
I understand any illicit substance found in my urine is a breach of this contract and my prescription for opioids may be stopped because using illicit drugs or alcohol in combination with opioids is potentially lethal.
I understand that I may be required to pick up my medication daily/weekly.
I understand that I will need to bring my medications to appointments for pill counting.
I understand if I break these conditions, Dr. ____________________ may cease writing opioid prescriptions for me.
Patient’s Signature: _______________________________________
Physician Signature: _______________________________________
Date: _________________________

Appendix 3: Sample Pain Assessment Scale

Appendix 4: Immunoassay versus Chromatography for Detection of Opioid Use
Immunoassay Chromatography
Does not differentiate between various opioids Differentiates: codeine, morphine, oxycodone, hydrocodone,
hydromorphone, heroin (monoacetylmorphine).
Will show false positives: Poppy seeds, quinolone
antibiotics.
Does not react to poppy seeds.
Often misses semi-synthetic and synthetic opioids, e.g.,
oxycodone, methadone, fentanyl.
More accurate for semi-synthetic and synthetic opioids.
Drug Number of days drug is detectable
Immunoassay Chromatography
Benzodiazepines
(regular use)
20+ days for regular diazepam use. Immunoassay does not distinguish different
benzodiazepines. Intermediate-acting benzodiazepines such as
clonazepam are often undetected.
Not usually used for benzodiazepines.
Cannabis 20+ Not used for cannabis.
Cocaine + metabolite 3–7 1–2
Codeine 2–5 1–2 (Codeine metabolized to
morphine.)
Hydrocodone 2–5 1–2
Hydromorphone 2–5 1–2
Meperidine 1 (often missed) 1
Morphine 2–5 1–2: Morphine can be metabolized to
hydromorphone

— Source: Adapted from Brands 1998
Oxycodone Often missed 1–2

Appendix 5: Oral Opioid Analgesic Conversion Table
The table is based on oral dosing for chronic non-cancer pain.
The figures are based on the Compendium of Pharmaceutical & Specialties (Canadian
Pharmacists Association 2008) and a systematic review by Pereira (2001). Wide ranges
have been reported in the literature.
These equivalences refer to analgesic strength of oral opioids, and not psychoactive
effects or effectiveness in relieving withdrawal symptoms.
1. Equivalence to oral morphine 30 mg:
Table B Appendix 8.1 Oral Opioid Analgesic Conversion Table
Equivalence to oral
morphine 30 mg:
To convert to oral
morphine equivalent,
multiply by:
To convert from
oralmorphine,
multiply by:
Morphine 30 mg 1 1
Codeine 200 mg 0.15 6.67
Oxycodone 20 mg 1.5 0.667
Hydromorphone 6 mg 5 0.2
Meperidine 300 mg 0.1 10
Methadone and tramadol Morphine dose equivalence not reliably established.
2. Equivalence between oral morphine and transdermal fentanyl:
Transdermal fentanyl* 60–134 mg morphine = 25mcg/h
135–179 mg = 37 mcg/h
180–224 mg = 50 mcg/h
225–269 mg = 62 mcg/h
270–314 mg = 75 mcg/h
315–359 mg = 87 mcg/h
360–404 mg = 100 mcg/h
* Formulations include 12, 25, 50, 75 and 100 ucg/hour patches, but the 12 ucg/hour patch is generally used for dose adjustment rather than initiation of fentanyl treatment.

Appendix 6: Opioid Tapering
Precautions for Outpatient Opioid Tapering
o Pregnancy: Severe, acute opioid withdrawal has been associated with
premature labour and spontaneous abortion.
o Unstable medical and psychiatric conditions that can be worsened by
anxiety: While opioid withdrawal does not have serious medical consequences, it can cause
significant anxiety and insomnia.
o Addiction to opioids obtained from multiple doctors or “the
street:” Outpatient tapering is unlikely to be successful if the patient regularly accesses
opioids from other sources; such patients are usually best managed in an opioid agonist
treatment program (methadone or buprenorphine).
o Concurrent medications: Avoid sedative-hypnotic drugs, especially
benzodiazepines, during the taper.
2. Opioid Tapering Protocol
o Before Initiation
Emphasize that the goal of tapering is to make the patient feel better:
to reduce pain intensity and to improve, mood and function.
Have a detailed treatment agreement.
Be prepared to provide frequent follow-up visits and supportive
counselling.
o Type of Opioid, Schedule, Dispensing Interval
Use controlled-release morphine if feasible (see 2.3 below).
Prescribe scheduled doses (not p.r.n.).
Prescribe at frequent dispensing intervals (daily, alternate days,
weekly, depending on patient’s degree of control over opioid use). Do not refill if patient
runs out.
Keep daily schedule the same for as long as possible (e.g., t.i.d.).
o Rate of the Taper
The rate of the taper can vary from 10% of the total daily dose every
day, to 10% of the total daily dose every 1–2 weeks.
Slower tapers are recommended for patients who are anxious about
tapering, may be psychologically dependent on opioids, have co-morbid cardio-respiratory
conditions, or express a preference for a slow taper.
Once one-third of the original dose is reached, slow the taper to one-
half or less of the previous rate.
Hold the dose when appropriate: The dose should be held or increased
if the patient experiences severe withdrawal symptoms, a significant worsening of pain or
mood, or reduced function during the taper.
o Switching to Morphine
Consider switching patients to morphine if the patient might be
dependent on oxycodone or hydromorphone.
Calculate equivalent dose of morphine (see Appendix B-8: Oral Opioid
Analgesic Conversion Table).
Start patient on one-half this dose (tolerance to one opioid is not fully
transferred to another opioid).
Adjust dose up or down as necessary to relieve withdrawal symptoms
without inducing sedation.
o Monitoring during the Taper
Schedule frequent visits during the taper (e.g. weekly).
At each visit, ask about pain status, withdrawal symptoms and
possible benefits of the taper: reduced pain and improved mood, energy level and alertness.
Use urine drug screening to assess compliance.

o Completing the Taper
Tapers can usually be completed between 2–3 weeks and 3–4 months.
Appendix 7:
SAMPLE Termination of Controlled-Substances Agreement:
Dr._______________________ has told me that my trial of opioid therapy has failed to reach
previously agreed upon treatment goats and so must be discontinued. Although every effort will
be made to reduce the risk of withdrawl symptoms from occurring, which may include a
temporary increase in my pain level, I understand this may be possible. Although
uncomfortable, I am aware that these withdrawl symptoms are not life-threatening and will go
away over time.
A. For this reason, the doctor has indicated that over the next month my dose of ______ will
be reduced and stopped.
Initials:__________
B. Or, at my request, I will try to find my own provider.
Initials:______________

RxFiles: Q&A Summary www.RxFiles.ca - March 2011
Urine Drug Screening (UDS) - Frequently Asked Questions (FAQ) “I do this routinely for all my patients when prescribing opioids for chronic pain.”
A) Why bother with urine drug screening (UDS)? • To improve patient care and communication by managing the misuse and diversion risks associated with select medications. • To help verify self-report of medication history. Is a prescribed drug present? Is anything else unexpectedly present? • To encourage or reinforce healthy behavioral change, sometimes as a requirement of continued treatment. UDS is commonly
included in a treatment agreement outlining both patient’s and health care professional’s responsibilities for safe medication use.
B) How often should we monitor for compliance using UDS?1 • Consider risk for opioid misuse or addiction, aberrant drug-related behaviours & availability. [See ORT tool.2] Monitor more frequently
in those at higher risk or exhibiting behavioural issues (e.g. q2-4wks); others less frequently (e.g. random, 1-4 times per year). • Random testing (for high risk): select dates & have receptionist call patient on date; allow ≤ 24hrs for patient to come in.
C) What are the types of UDS?1,3
Types of UDS When to test? Benefits Limitations & Comments Point-of-care (POC) Testing Enzyme Immunoassay (EIA) (e.g. ELISA, EMIT)
o When immediate results are desired (not too commonly done as relatively non-specific for drug class only)
o Urine sample collected & tested at the physician’s office/clinic
o Results are immediate for a drug class (e.g. opiate)
o Portable o Identify illicit drug use in a
timely fashion
o Cost of POC test kits & dipsticks o Less sensitive & specific than laboratory tests o Will not identify specific drug or metabolites o Subjective nature of the qualitative assays o Lacks adequate quality assurance & control (e.g. integrity
of the test reagents following transportation & storage) o Data management issues. Limited menu of drugs offered o POC devices lack evidence to improve patient outcomes
Laboratory Testing – Immunoassay
o Useful for initial screening (rapid & inexpensive)
o Detects drugs for a longer time than chromatography (5-7 days vs 1-2 days for chromatography)
o Does not distinguish between different types of opioids o Often misses semi-synthetic/synthetic opioids e.g. fentanyl,
hydromorphone, oxycodone, meperidine & methadone o Shows false positives (poppy seeds, quinolone antibiotics)
Lab. Testing –
Chroma-tography or Mass spectrometry (MS) see comment on right
o To specifically confirm presence of a given drug
o To identify drugs not included in an immunoassay test, when result contested
o More accurate for semi-synthetic & synthetic opioids.
o Differentiates: codeine, morphine, oxycodone, hydrocodone, hydromorphone, heroin (monoacetylmorphine), etc.
o Doesn’t react to poppy seeds
o More expensive & may take longer to get results o Requires caution in interpretation: e.g. codeine
metabolized to morphine
Strips Temperature-test o Detects tampering/dilution o Must be read within minutes; sample cools quickly. Costly. Urine Creatinine level: Detects sample dilution (urine creatinine < 2-3 mmol/L is non-physiologic & suggests dilution) ELISA=enzyme linked immunosorbent assay EMIT=enzyme multiplied immunoassay GC=gas chromatography LC=liquid chromatography MS=mass spectrometry POC=point of care
D) What are the detection times for immunoassay and chromatography?1,3 for most drugs: 1 to 3 days • Long-term use of lipid soluble drugs {eg. marijuana, diazepam, ketamine, or phenycyclidine (PCP)} may extend detection to a week or more • Immunoassay’s ability to detect drugs will vary according to the drug’s concentration in urine & the assay’s cutoff concentration
Drug Immunoassay (days detected) GC, LC or MS Amphetamines Up to 3 days {caution with false positives from interfering agents; see “G”.} Benzodiazepines (regular use)
20+ days for regular diazepam use. Does not distinguish between different benzo’s. Intermediate-acting benzodiazepines (eg clonazepam) often undetected.
Varies; identifies specific agents
Cannabis/THC (depends on grade & frequency of use)
Single use – 1-3 days. Chronic use – up to 30 days. Nabilone (Cesamet®) does not contain THC & never detected in urine. Dronabinol (Marinol®), & Sativex® will produce positive results.
Varies
Cocaine + metabolite 3-7 days (metabolite=benzoylecgonine) {Note: no structural similarity to other “caine”s} 1-2 days Gabapentin - 1-2+ days if used in high doses
Heroin & 6-MAM monoacetylmorphine
Heroin rarely detected (half-life =3-5 minutes). {Heroin 6-MAM morphine} 6-MAM difficult to detect (half-life=25-30 min) –detection within a few hours.
Meperidine 1 day; but often missed; (can be specifically requested) 1 day Methadone & EDDP Often missed. Up to 3 days. {Up to 6 days with EDDP (methadone metabolite)} Opioids, various 2-5 days: codeine, hydrocodone, hydromorphone, morphine
Often missed: fentanyl, oxycodone (can be specifically requested), methadone 1-2 days. ♣
♣ Metabolism note: codeine will be metabolized to both morphine & ~ hydrocodone/hydromorphone. Morphine high dose may be partly metabolized to hydromorphone. ROUTINE TESTS - RUN BY SK PROVINCIAL LAB (Regina): Alprazolam & mets, Amphetamine, Benzoylecgonine, Clonazepam & mets, Cocaine, Codeine, Diazepam, Diphenhydramine, EDDP, Fentanyl & mets, Flunitrazepam,
Flurazepam & mets, Gabapentin, Hydrocodone, Hydromorphone, Ketamine, Lorazepam, MDA, MDEA, MDMA, Meperidine & mets,Methadone ,Methamphetamine, Methylphenidate, Morphine, Oxazepam, Oxycodone, PCP, Pseudoephedrine, Ritalinic acid, Temazepam, THC, Triazolam. NOT TESTED UNLESS SPECIFICALLY ORDERED: barbiturates, buprenorphine & mets, cocaethylene, bromazepam, ethanol, GHB gammahydroxybutyrate. Other: chloral hydrate.
Mass spectrometry (used at SK Provincial Lab) gives better specificity as opposed to chromatography. Combination & tandem testing also used when more specific detection & quantification needed [e.g. gas or liquid chromatography + mass spectrometry (GC-MS, LC-MS); or tandem MS].

E) Prior to doing a UDS
• Inform the patient of the routine nature of test (e.g. “I do this routinely for all of my patients on opioids…”) • Take a careful history of medication use in the past week. May ask “what should I expect to see in the results?” • Collect the sample in the physician office & ensure proper labeling. Consider who will be using the information.
F) How do we interpret unexpected results and what can we do?1,4,5
CAUTION: Goal is to improve communication and not to police! Remember result could be false. Give opportunity for patient to address the report & suggest a repeat UDS if results are plausibly false. Clinician must be willing to change treatment plan if an abuse/diversion issue arises. This could include: 1) tightening boundaries with ↑ emphasis on holisitic, non-drug treatment; 2) referral to addiction services; 3) discontinue drug with or without a taper. Seek confirmatory testing if necessary. Detox services help & introduce recovery processes & services.
Results Possible explanation Actions for the Physician or Allied Health Professional UDS negative for prescribed opioid
• False negative • Non-compliance (e.g. if patient
binging on opioid, then running out) • Diversion (suspect especially if
repeatedly negative)
• Repeat test using chromatography; specify the drug of interest (e.g. oxycodone, fentanyl, methadone often missed by immunoassay)
• Take a detailed history of medication use for the preceding 7 days (e.g. could learn that patient ran out several days prior)
• Ask patient if they have given the drug to others • Monitor compliance with pill counts • Review/revise treatment agreement (tighten boundaries)
UDS positive for non-prescribed opioid or benzodiazepines
• False positive (e.g. poppy seeds) • Patient acquired opioids from other
sources (double-doctoring, “street”)
• Repeat UDS regularly • Ask the patient if they accessed opioids from other sources • Assess for opioid misuse/addiction; may refer to addiction tx program • Review/revise treatment agreement (tighten boundaries)
UDS positive for illicit drugs (e.g. cocaine, cannabis/THC)
• False positive • Patient occasionally using or
addicted to the illicit drug • Cannabis is positive for patients
taking dronabinol (Marinol®), THC:CBD (Sativex®) or using medical marijuana
• Repeat UDS regularly • Assess for abuse/addiction and refer to addiction treatment program as
appropriate • Ask about medical prescription of dronabinol, THC:CBD or medical
marijuana access program
Urine creatine is <2-3 mmol/L suggesting dilution
• Patient added water to sample • Patient added an acid to sample
(may detect by ordering pH)
• Repeat UDS (Note, some labs can test for common adulterants if suspected) • Consider supervised collection or temperature testing • Take a detailed history of medication use for the preceding 7 days • Review/revise treatment agreement (tighten boundaries)
Urine sample is cold
• Delay in handling sample (urine cools within minutes)
• Patient added water to sample
• Repeat UDS, consider supervised collection or temperature testing • Take a detailed history of the patient’s med use for the preceding 7 days • Review/revise treatment agreement (tighten boundaries)
G) What are some examples of cross-reacting compounds for certain immunoassays? 2, 6 Interfering agent Immunoassay affected Interfering agent Immunoassay affected
Codeine {codeine metabolizes to morphine; will produce a morphine:codeine ratio of <2:1. a ratio >2:1 suggests non-codeine source (e.g. heroin, morphine; also poppy seeds if low morphine level but high ratio}
Codeine, morphine, hydrocodone (NOT likely hydromorphone)
Morphine Morphine, Hydromorphone
Diet pills (e.g. clobenzorex, fenproporex) Amphetamine Pantoprazole possibly other PPI? THC Efavirenz THC Poppy Seeds c Morphine -will produce high ratio (>19:1) of
morphine:codeine with very small amounts of morphine (<2000ng/ml)
Ephedrine, pseudoephedrine Amphetamine Promethazine Amphetamine Hydrocodone Hydromorphone Quetiapine Methadone l-methamphetamine (Vicks® Inhaler in USA only) Amphetamine Sertraline Benzodiazepine Levofloxacin & some other fluoroquinolones Opiates Trazodone Fentanyl Selegiline Amphetamine Venlafaxine Phencyclidine NOTES: a Cocaine is very reliable and has low cross-reactivity with other agents. b A minor metabolite should not be in excess of its parent. Clarify any unexplained test results with someone with expertise in the area. Quantitative testing (GC & MS) may be performed in some cases for confirmatory testing. c Poppy seed & heroin EIAs can be very similar (very high morphine:codeine ratio > 2:1) but absolute levels of morphine & codeine are typically lower with poppy seed. To distinguish, avoid poppy seed ingestion; alternately if test for 6-MAM is positive, this proves hx of heroin use (but short t ½ of 6-MAM makes difficult to get +’ve test).
Acknowledgements: We would like to thank those who contributed to the development, review for this chart: M. Markentin, Dr. L. Lanoie, Dr. P. Butt, Dr. B. Fern, Jeff Eichorst (SK Provincial Lab). Prepared by: Margaret Jin PharmD, L Regier BSP.
DISCLAIMER: The content of this newsletter represents the research, experience and opinions of the authors and not those of the Board or Administration of Saskatoon Health Region (SHR). Neither the authors nor Saskatoon Health Region nor any other party who has been involved in the preparation or publication of this work warrants or represents that the information contained herein is accurate or complete, and they are not responsible for any errors or omissions or for the result obtained from the use of such information. Any use of the newsletter will imply acknowledgment of this disclaimer and release any responsibility of SHR, its employees, servants or agents. Readers are encouraged to confirm the information contained herein with other sources. Additional information and references online at www.RxFiles.ca Copyright 2011 – RxFiles, Saskatoon Health Region (SHR) www.RxFiles.ca References
1 National Opioid Use Guideline Group (NOUGG). Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non‐Cancer Pain. Part B: Recommendations for Practice. April 30, 2010.
Version 5.6. http://nationalpaincentre.mcmaster.ca/opioid/ 2 Opioid Risk Tool: http://nationalpaincentre.mcmaster.ca/opioid/cgop_b_app_b02.html 3 Gourlay DL, Heit, Caplan YH. Urine Drug Testing in Clinical Practice. The art and science of patient care. Edition 4. May 31, 2010 4 Gourlay DL, Heit HA. Universal precautions revisited: managing the inherited pain patient. Pain Med. 2009 Jul;10 Suppl 2:S115‐23. 5 Regier L. Substance Abuse / Addiction Chart in RxFiles Drug Comparison Charts –8th Ed. Accessed on line at: http://www.rxfiles.ca/rxfiles/uploads/documents/CHT‐Substance‐Abuse.pdf 6 Tenore PL. Advanced urine toxicology testing. J Addict Dis. 2010. Oct;29(4):436‐48.
Remember, it’s OK to say “no”.
Clonazepam & lorazepam may test negative in benzodiazepine EIAs!