Ophthalmic USG
104
Pabita Dhungel B.Optometry 3 rd year ULTRASONOGRAPHY PRINCIPLE, METHODS AND INTERPRETATION
-
Upload
pabita-dhungel -
Category
Health & Medicine
-
view
311 -
download
6
Transcript of Ophthalmic USG

Pabita DhungelB.Optometry3rd year
ULTRASONOGRAPHY PRINCIPLE, METHODS AND INTERPRETATION

PRESENTATION LAYOUT
• Introduction• History• A- scan• B- scan• Methods for special purposes• Clinical pictures• Summary

References
• Clinical Procedure in Optometry• Optometry: science, techniques and Clinical
managements• Ophthalmic ultrasonography• Borish Clinical Refraction

Introduction
• Ultrasound is an acoustic wave (above audible frequency) that consists of oscillations of particles within a medium, frequencies greater than 20kHz(20,000 oscillations/s)
• Diagnostic ophthalmic Ultrasound– Frequency 8-10 MHz (Sandra Frazer et. Al)
• 8-25 MHz for Posterior segment & Orbit (Jager’s Duane Oph.)
• 50 MHz for imaging Anterior segment (Jager’s Duane Oph.)
– Produce short wavelength = 0.2 mm– Good resolution of ocular structures – Less
Penetration

Contd…
• Examination of larger structures e.g abdominal or obstetric ultrasound requires frequencies in the range of 1 to 5 MHz
• Such wavelengths produced by these lower frequencies enable these instruments to penetrate deeper into the body decreasing their resolution capability

Contd…
• Ultrasound is transmitted as a longitudinal wave so its speed is dependent upon the density of the medium it is passing through e.g air sound travels at 340m/s whereas in water its speed is much faster at approx 1480m/s.
• Fluid contact is essential betn the transducer and eye so normal saline is used in open eye or water soluble gel is used if reading taken through eyelids

Sound Wave Velocities Through Various Media
Medium Velocity (m/sec) Water 1,480
Aqueous/ Vitreous 1,532
Silicon Lens 1,486
Crystalline Lens 1,641
PMMA Lens 2,718
Silicon Oil 986
Soft Tissue 1,550
Bone 3,500

History
• In 1956, • First time: Mundt and Hughes, American Oph.
• A-scan (Time Amplitude ) to demonstrate various ocular disease
• Oksala et. Al in Finland• Ultrasound Basic Principle (Pulse-Echo Technique)• Studied reflective properties of globe
• In 1958, Baum and Greenwood • Developed the first two-dimensional(immersion) (B-scan)
ultrasound instrument for ophthalmology.• In the early 1960s, Jansson and associates, in Sweden,
• used ultrasound to measure the distances between structures in the eye.

Contd…
• In the 1960s, Ossoinig, an Austrian ophthalmologist– first emphasized the importance of standardizing
instrumentation and technique.– developed standardized A-scan.
• In 1972, Coleman and associates made– first commercially available immersion B -scan instrument – Refined techniques for measuring Axial length, AC depth,
Lens thickness
• Bronson in 1974 made contact B scan machine.

Advantages of USG
• Easy to use.• No ionizing radiation• Excellent tissue differentiation• Cost effectiveness
Primary uses in ophthalmology:– Posterior segment evaluation in Hazy media / Orbit
• Structural integrity of eye but no functional integrity – Detection and differentiation of intraocular and orbital
lesions – Tissue thickness measurements.– Location of Intra Ocular Foreign Body– Ocular Biometry for IOL power calculations

Principle
Average velocity in Eye = 1500 m/sec– Takes about 33 microseconds to travel & return
back from the posterior part of eye•Principle
– Pulse- Echo System • Emission of multiple short pulses of ultrasound
waves with brief interval to –Detect, process and display the turning
Echoes

• Piezoelectric crystal (Quartz & Ceramic Crystal) – Present in Probe tip
• Application of Pulse of Voltage electric energy – Mechanical Vibration Rapid vibration
» Generate short pulse Ultrasound energy (Transducer)
• Longitudinal ultrasound wave propagate through medium (Eye) – Echoes come back from different Acoustic Interfaces
– A pause of Several Milliseconds for receiving echoes • Creates mechanical vibration as it strikes the probe tip
and the piezoelectric crystals – Produce electric energy
– Transmitted to receiver and in a Cathode ray Tube to display Ultra sonogram

Terms
PROBE – Consists of piezoelectric transducer. – A piezoelectric transducer consist of small ceramic plates
• which converts electricity into sound waves and sound waves into electric signals to be displayed on the screen.
– Damping material (metal powder with plastic or epoxy) • Help to produce shorter Pulse – Better for Axial
resolution• Axial resolution
– The minimum distance between two interfaces (Echo Sources) along the direction of the sound beam

Contd…
• Shape of the Crystal: – Planer crystal
• Produce relatively parallel sound beam (A- Scan)
– Acoustic lens – Produce focused sound beam (B-scan)• Improves lateral resolution
–Minimum separation between two interfaces perpendicular to the direction of sound beam

Contd…
• RECEIVER (computer unit) – Receives returning echoes
• Produces electrical signal that undergoes complex processing
–Amplification, Compensation, Compression, Demodulation and Rejection

Contd…
• RESOLUTION – – Ability to discern two interfaces close to each
other.– Higher the frequency of ultrasound
• Shorter the wavelength & better the resolution.
• Echoes- – Reflected portion of the wave.

• GAIN – – Relative units of Ultrasound intensity
• Expressed in Decibel (db)• Adjust of gain doesn't change the amount of energy
emitted by transducer – but chance in intensity of the returning echoes for
display – Electric Amplification of the echo signals received by the
transducer • Higher the gain – Greater the sensitivity of the
Instrument in displaying weaker echoes (i.e Vitreous opacities)
• Lower the gain – Weaker the depth of sound penetration
– only stronger echoes are displayed (i.e Retina / Sclera)

Gain contd…
• Stronger echoes are located in the centre of the returning sound wave – Lowering gain effectively narrows the sound beam
• Improves both axial and lateral Resolution
• When the gain is Increased – A-scan gets taller and B-scan echoes gets brighter
conversely • When the gain is turned down the echoes get
shorter and dimmer.

Displaying the Ultrasound
1. A-Mode Display
2. B-Mode Display
3. M-Mode Display

A - scan
• ‘A’ for amplitude provides one dimensional display of returning echoes in the form of vertical spikes of various heights and distances from the initial signal
• Echoes from the structures deeper within the eye take longer to return to the transducer for conversion back to electric signal, so appear further along the time baseline

Contd…
• Two fundamental data obtained are
i) distance of echo source from the probe face
- forms the basis of biometry
ii) amplitude of echo signal (spike) which partly depends on the nature of reflecting interface
- forms the basis of quantitative echography

Standardization of A scan
• Credited to Dr. Karl Ossoinig
1.Unique sound Amplification :
S-shaped amplifier with flat upper and lower curves and a steep mid segment and a dynamic range of 36dB
This amplification enhances the difference between normal and abnormal signals

A-Mode DisplayA-Mode Display• Sound velocity should be adjusted
– Time Dimension calculated according to the speed at which sound travels via a given medium
– Phakic Eye – Average Sound Velocity : 1,550 m/sec
Average Velocity Adjustment for Eye Length measurement
Ocular Media Velocity (m/sec)
Aphakia (Aqueous/ Vitreous) 1,532
Phakia 1,550
Pseudophakia PMMA Implant Silicone Implant
1,532 + 0.2 mm or 1,5501,486
Silicon oil 986
Note: Average Velocity : Average of Sound Velocities for the Aqueous + Vitreous + Lens

Examination steps
• Patient is positioned with head near oscilloscope
• Topical anaesthetic drops are placed in the eye
• Probe is firmly placed on the globe without coupling jelly as tear acts as coupling agent
• Eight meridians are scanned, postero-anteriorly, by shifting and tilting the probe in a single, smooth arc movement from limbus to fornix

Contd…
• In cases of traumatized or infected eyes, or soon after intraocular surgery, examination through the closed eyelids is safer
• At the end of procedure, the eye is irrigated with sterile saline, and the probe tip is cleaned with alcohol wipe or other suitable disinfectant

Orientation and labelling of scan
• The labelling of sections is determined by the projection of the beam and not the probe location
• E.g a section labelled 12 equator (12E) is produced by placing the probe at 6 0’clock and mid distance betn limbus and fornix, a section labelled 6 anterior (6 A) is produced by placing the probe at 12 0’clock fornix

Macular screening
1) Axial section• easier of the two approaches•Probe is placed on cornea and directed axially•Suitable for measurement but not sensitive in detecting early macular thickening or in differentiation of its lesions because of strong sound attenuation by the lens

Contd…
• Posterior section• In the RE this is 9P position and in the LE the
3P position• Produced by directing the patient’s gaze
temporally and placing the probe at the nasal limbus and aiming it posteriorly thus avoiding the lensand achieving better resolution

Examination of fundus periphery
• Patient’s gaze is directed maximally towards the meridian to be scanned and probe is placed at the opposite fornix the beam being aimed across the globe towards the opposite periphery
• Useful for detecting peripheral retinal cysts/retino-schisis, choroidal detachments and ciliary body lesions

B - Scan
• B for brightness produces two dimensional slice of tissue images, composed of coalescing dots of varying degrees of brightness , depending on the reflectivity of the echo source
• Probe emits a focused sound beam at the frequency of 10 MHz , eye dedicated scanners produce a sound beam whose focal zone coincides with the posterior globe wall and anterior orbit

Contd…
• Marker at the probe tip indicates the beam orientation and the top of the echogram as it displays on the screen
• Coupling jelly is applied to the probe tip to ensure adequate sound transmission
• Probe sterilized with alcohol, impregnating B-probe in sterilizing soln isn’t recommended as it damages the transducer

Fundamental objectives for high quality B- scan
• Lesions must be placed in the center of the scanning beam
• Beam must be directed perpendicularly to interfaces at the area of interest
• Lowest possible decibel gain that is consistent with the maintenance of adequate intensity should be used to optimize resolution of the images

B- scan sections: orientation and labelling
• 1) Axial section• Easiest to perform and interpret• Probe is placed on the cornea and directed
axially• Posterior lens surface and optic nerve head
are placed in the center of the echogram• Optic nerve head is used as an echographic
centre

Contd…
• Depending on the clock hour location of the probe marker, a vertical axial section (marker at 12 0’clock) horizontal axial scan (marker at 3 0’clock RE and 9 0’clock LE) and sections of all other clock hours can be performed
• Easy orientation and demonstration of posterior pole lesions and attachments of membranes to optic nerve head

Contd…
• Because of scatter and strong sound attenuation created by the lens higher decibel gain levels are needed to show structures at the posterior segment
• In pseudophakia strong artefacts created by the lens implant will hamper the adequate visualization

Contd…
2) Transverse section•Probe is placed on the limbus and directed posteriorly •Echograms are labelled according to clock hour at the center of the beam and also to the beam’s anteroposterior location•E.g section labelled 12 posterior (12P) is produced by a probe located at 6 0’clock limbus, a 6 0’clock (6E) by probe located at 12 0’clock

Contd…
3) Longitudinal section•Section produces an antero-posterior slice of the ocular wall along one meridian only; from the optic nerve (lower portion of echogram) to the ciliary body (upper portion of the echogram)•Probe is located on sclera with marker at its limbal side

Contd…
• Echograms are labelled after the clock-hour location of the beam
• E.g L-3 is a section produced by a probe at 9 0’clock limbus and L-12 by a probe at 6 0’ clock limbus

Steps for ocular screening
1) Transverse 12:
Patient directs gaze superiorly
Probe is placed at the 6 0’clock limbus with its marker nasally
Shifting and rotating the probe from limbus to fornix scans the superior retina postero-anteriorly

Contd…
2) Transverse 3:•The patient gazes at 3 0’ clock and the probe is placed at 9 0’clock with its marker up•Probe is manoeuvred from the limbus to fornix, scanning the nasal retina in the RE and temporal retina in the LE

Contd…
3) Transverse 6:•The patient looks downwards and the probe is positioned at 12 0’clock with the marker nasally and swept from limbus to fornix to scan inferior retina
4) Transverse 9:•The patient gazes at 9 0’clock and the probe is manoeuvred at 3 0’clock with its marker kept up, section scans the temporal retina in the RE and nasal retina in the LE

Contd…
• Four additional transverse scans of the oblique quadrants i.e 1:30 , 4:30, 7:30 and 10:30 0’ clock hours may be performed in a similar fashion if abnormalities in the oblique periphery are suspected

Macular screening
1) horizontal axial • an axial section with the marker nasally will display the macular area and adjcent optic nerve head
2) Vertical macula•Probe is tilted temporally without losing the posterior lens echoes •Vertical beam is shifted from optic nerve to the macular area, lens acts as a reference point for accurate placement and future reference

Contd…
3) Transverse 9:00 RE and 3:00 LE•The probe is placed on the corresponding nasal limbus with its marker up, and the patient gazes temporally•Avoiding the lens allows better visualization of the vertical extent of macular masses

Contd…
• 4) Longitudinal 9:00 RE and 3:00 LE• Patient’s gaze is directed temporally• Probe is placed on the nasal side of the globe
with the marker at the limbus• Macular area will appear at the centre of the
echogram with the optic nerve at the bottom and ciliary body at the top
• Lateral extension of lesion is studied in this section

M- Mode Display
• Motion Mode & Time-Motion Mode • Used to monitor Integrity of Blood Vessels/ Lens
Accommodation Dynamic • Aka Color Doppler Imaging (CDI), the technique
provides information about the ocular vascular supply superimposed on a B-scan image

Contd…
• This modality gives approx flow velocity of the principal vessels in the eye and orbit, by providing a color doppler display for pulse doppler examination (Lieb et al 1991; Giovagnorio et al 1993)
• CDI scans of the eye and orbit are performed with patient lying in supine position with their eye closed using an ultrasound frequency > 7 MHz and a Doppler frequency >5 MHz (Tranquart et al 2003)

Contd…
• The transducer or probe is applied to closed eyelid using a thick layer of conducting gel
• Care must be taken not to exert any pressure on the globe as this might result in a decrease in blood flow velocity, thus increasing the RI with no diagnostic significance

FACTOR INFLUENCING HEIGHT IN A-SCAN AND BRIGHTNESS IN B-SCANFACTOR INFLUENCING HEIGHT IN A-SCAN AND BRIGHTNESS IN B-SCAN
1. Angle of the sound beam
1. Interface
2. Size and shape of interfaces

• When the sound beam is directed perpendicularly to a structure
– Maximum amount of sound will be reflected back to the probe.
The farther away from the ideal angle , the lower the amplitude.
1. ANGLE OF INCIDENCE

• Depends upon the difference between Acoustic Impedance
– Greater the diff. AI stronger the Reflected Echoes
• EG:
– Anterior lens surface produce strong echo when bordered by Aqueous than by Blood
– Interface between vitreous and fresh blood is very slight resulting in small echo.
– The difference between a detached retina and the vitreous is great producing a large echo
2. INTERFACE

Smooth surface like retina will give strong reflection.
Smooth and rounded surface scatter the beam.
Coarse surface like ciliary body or membrane with folds tend to scatter the beam without any single strong reflection.
Small interface produces scattering of reflection.
3. TEXTURE AND SIZE OF INTERFACE

Indications for Intraocular Examination
Opaque Ocular MediaAnterior Segment
Corneal opacificationHyphema /hypopyonCataractPupillary or
retrolenticular membrane
Posterior Segment Vitreous hemorrhage or
inflammation
Clear Ocular Media
Anterior segment
Iris lesions
Ciliary body lesionsPosterior segment
Tumors
Choroidal detachment
Retinal detachment
Optic disc abnormalities-Intraocular foreign bodies
•
BiometryBiometry

� Indications-Signs & Symptoms-• Unilateral or Bilateral
Exophthalmos• Enophthalmos• Globe Displacement• Lid Abnormalities - Ptosis,
Retraction, Swelling, Ecchymosis• Palpable or Visible Masses• Chemosis• Motility Disturbances;
Diplopia• Pain
Additional Indications-
• Tissue Differentiation of Mass Lesions
• Clarification of CT or MRI Findings
• Assessment of blood flow within lesions
• Follow-up studies
Intraorbital ExaminationIntraorbital Examination

Examination Techniques For The Globe:
• Positioning the patient
• Topical anesthesia
• Techniques
– Contact Technique• Probe - placed directly on the globe
– Immersion Technique
• Methylcellulose - a coupling medium (B-Scan)

Contact Technique• The Probe Placed
– Directly on the cornea (A-Scan) or over closed lids (B- Scan)
– To evaluate the posterior segment only (B Scan)
Small solid probe fits in the Tonometer holder for A-scan biometry.
Small solid probe fits in the Tonometer holder for A-scan biometry.

Applanation Technique

Contact Technique A Scan – Phakic Eye

Contact Technique A- Scan - Aphakia

Contact Technique
• Sources of Error – Corneal compression
(Shorter Axial length) • 1mm error in Axial length –
2.5 to 3.0 Ds error in IOL Power
– Misalignment of sound beam
– Fluid Miniscus Trapped• Erroneously Long AL

• Correct– ( no compression )
No Fluid meniscus trapped between probe tip and cornea.
A- Scan

Immersion Technique
• Can use in the same instrument – Requires Scleral Cup
• Coupling Agent – Methylcellulose • Probe is not directly placed on the
cornea – immersed into the fluid
• Error – Small air bubbles in the fluid
gives falsely long AL measurement
Prager Scleral Shell

Scleral Shells
The Hansen scleral shells available in 16, 18, 20, 22, and 24 mm
The Hansen scleral shells available in 16, 18, 20, 22, and 24 mm
The Prager Shell The Prager Shell
The Kohn shell The Kohn shell

Immersion Technique
The cup is placed between the lids and methylcellulose 1% is poured into the cup.
The ultrasound probe is immersed in the solution, keeping it 5 to 10 mm away from the cornea.

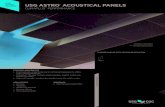
A-Scan (Immersion Biometry)
Initial spike (IS), the anterior (C1) and posterior (C2) corneal surfaces, the anterior (L1) and posterior (L2) lens surfaces, the retina (R), sclera (S), and orbital tissues (O).
Initial spike (IS), the anterior (C1) and posterior (C2) corneal surfaces, the anterior (L1) and posterior (L2) lens surfaces, the retina (R), sclera (S), and orbital tissues (O).

Immersion Technique: Advantages
• Important in patients with shorter axial length < 22.00 mm – no corneal compression
• Where small error in measurement cause significant error in Biometry
• Can examine the cornea, anterior chamber, iris, lens & retrolental space
• Ultrasound Biomicroscopy:– developed by Pavlin & colleagues– uses sound wave of 50 to 100 MHz

Immersion Technique• Should be cautious in eyes with recent intraocular
surgery or penetrating trauma.
• No corneal compression
• No problem of fluid meniscus
• The display of a separate corneal spike makes it easier to determine when the sound beam is properly aligned along the optical axis.

Examination Techniques For The Globe-A scan
• The probe should remain perpendicular to the structure studied– The probe is first adjusted to the Tissue Sensitivity gain setting.
• One dimensional acoustic display-echoes-vertical spikes from baseline
Uses•For IOL calculations (biometry)•For differentiating and monitoring certain ocular conditions • Congenital glaucoma• Progressive Myopia
Uses•For IOL calculations (biometry)•For differentiating and monitoring certain ocular conditions • Congenital glaucoma• Progressive Myopia

Axial Eye Length Measurements
• Two techniques: – The contact method– The immersion method
• In both techniques, the sound beam must be directed along the optical axis of the eye.

B scan
• Different types of Probe • The probe face is Oval
Shaped with the transducer movement in the direction of longest diameter
• The probe contains transducer that moves back and forth near the tip
• Fig of probe face

B scan
• Each probe has a marker – A dot / Line – Indicates the side of
the probe that is represented on the upper portion of B-Scan Display

• Basic Screening Examination– transverse scans of the four major
quadrants at a high gain setting, from limbus to fornix
– first superior portion → nasal portion → inferior portion → temporal portion
Examination Techniques For The Globe:..

Examination Techniques For The Globe-B scan
• After transverse scan – Eye should be scanned with longitudinal scan at
least in four major quadrants– Helpful in detecting lesions in peripapillary region and macula
• Globe should also be evaluated with vertical and horizontal axial scan

A-scan basic screening examination

Special Examination Techniques
• Topographic– Location– Extension– Shape
• Quantitative– Reflectivity estimate: spike height– Internal structure: histologic architecture– Sound attenuation: absorption, shadowing
• Kinetic– Mobility: after movement– Vascularity: blood flow

Topographic Echography
A. point-like
e.g. fresh V.H
B. membrane-like
e.g. R.D
C. mass-like
e.g. choroidal melanoma

Quantitative Echography
1-Reflectivity estimate:
PVD Vs RD– PVD produces 50%
high spike– RD produces 100%
high spike

Quantitative ..internal structure
• Choroidal melanoma-homogenous histologically-regular internal stucture,low reflectivity
• Choroidal hemangioma-multiple vascular spaces-regular internal structure high reflectivity
• Metastatic carcinoma-irregular arrangement of tumor cells,variable reflectivity

Kinetic Echography• Lesion mobility (after
movement)– Non-solid lesion (e.g.
vitreous membrane, RD) displays after movement.
– Solid lesion (e.g. tumor) does not.
Blurred appearance of spikes

Kinetic…• Vascularity (spontaneous motion)
– Vascularity is a characteristic that is assessed in tumors spontaneous motion (low-amplitude flickering of the internal lesion spikes)

• Three major portions:– orbital soft tissue assessment
– extraocular muscle evaluation
– retrobulbar optic nerve
examination
• Two approaches:– Transocular (through the globe)
• for lesions located within the posterior & mid-aspects of the orbital cavity
– Paraocular (next to the globe)• for lesions located within the lids or anterior orbit
Examination Techniques For The Orbit:

• Basic Screening Examination– Mainly Transocular approach
– Transverse scans of the four major meridians using a medium-high gain setting• From limbus to fornix
– First superior portion → nasal portion → inferior portion → temporal portion
Examination Techniques For The Orbit:…

Clinical Examples:
Order of disappearance with gain reduction : Vitreous Opacities –Blood- Retinal Tissue – Ca++Order of disappearance with gain reduction : Vitreous Opacities –Blood- Retinal Tissue – Ca++

Vitreoretinal Disease
• Mild and extremely dense Asteroid hyalosis• Dense Vitreous hemorrhage

Vitreous Haemorrhage
• US showing hemorrhagic track through vitreous cavity along path of penetrating nail injury

Posterior Scleritis
• High reflective thickening of retinochoroid layer and sclera

RD Vs PVDRD Vs PVD
Choroidal Detachment Choroidal Detachment

Posterior Vitreous Detachment
• Low reflective vitreous opacities and a posterior vitreous detachment as seen with normal aging of the eye.

Tractional RD
• US showing tent shaped tractional RD (Large arrow). Small arrows show vitreous membranes of low reflecting attached to apex of detached retina.

Dislocated Lens:

Choroidal Detachment
B-scan of eye with “kissing” Choroidal detachment & Haemorrhage

Subarachnoid Fluid Around the Optic Nerve
Positive crescent sign.

Ciliary Body Detachment (Immersion Technique)
Ciliary body detachment as seen on high-resolution scan. Note the large cleft in the subciliary space

Choroidal Melanoma:

Thyroid Ophthalmopathy Vs Myositis
• Thickened muscles due to thyroid ophthalmopathy.
• Orbital myositis
Thickened muscle
to be irregular and
medium-high reflective
in thyroid but regular and
low reflective in myositis.

Posterior Staphylomas


.
Positive T-sign at the insertion of the optic nervePositive T-sign at the insertion of the optic nerve
Nodular posterior scleritis with fluid in the Tenon capsuleNodular posterior scleritis with fluid in the Tenon capsule
ScleritisScleritis

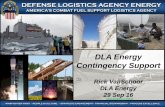
AC – Hyphema (Immersion Technique)
US showing anterior chamber hyphema.
C represents cornea, white arrow - hyphema and L - Lens.

Metallic Foreign Body
• US of eye demonstrated a metal F.B. (arrow) which is highly reflective. This can produce a region that may look like a nerve shadow or even resemble a dehiscence in sclera.

Metallic IOFB
• Thick, very highly reflective spike from foreign body(F) and decreased spike height of sclera and orbital tissue as a result of sound attenuation.
.

Retinoblastoma
• Non-calcified RB• Calcified RB

Extrusion of Lens Material
• B-scan of eye with severe blunt trauma showing extrusion of lens material through small posterior lens rupture (arrow).

S
THANK YOU