OPG and Extraoral radiography
74
Click here to load reader
-
Upload
neha-sharma -
Category
Health & Medicine
-
view
220 -
download
20
description
Thorough knowledge of the indications of various extra oral techniques allows accurate and timely diagnosis of various maxillofacial pathologies. Further, we can arrive at a diagnosis with minimum number of x-rays there by reducing patient exposure to radiation.
Transcript of OPG and Extraoral radiography

63A7.tmp635E.tmp635E.tmp

Radiographs
(Part 2)Presented byDr. Neha SharmaPG II YR

3
CONTENTS
PANORAMIC IMAGING EXTRAORAL RADIOGRAPHS CEPHALOMETRIC LANDMARKS LATERAL SKULL PROJECTION SUBMENTOVERTEX PROJECTION PA WATERS PROJECTION REVERSE TOWNES PROJECTION TMJ IMAGING CONCLUSION

HISTORY OF -EXTRAORAL RADIOGRAPHIC TECHNIQUES

EXTRA-ORAL SOURCE
Discovered by
Dr. Hisatugu Numata of Japan,
1933

Father of Panoramic Radiography
• 1949, extra-oral films
• X-ray source - stationary
Dr Yrjo Veli Paatero

What is panoramic imaging /pantomography???
A technique for producing a single
tomographic image of the facial structures
that includes both the maxillary and
mandibular dental arches and their supporting
structures.

‘Panorama’ ‘Tomography’
An unobstructed
view of a region in
every direction
An X-ray technique for making
radiographs of layers of tissue in depth without the
interference of tissues above and below the level
PANTOMOGRAPHY

Equipment
1. Panoramic X-ray unit

2. Screen film

3. Intensifying screens

4. Cassette

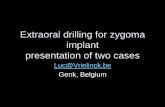
BONY LANDMARKS IN MANDIBLE
14
1
1. Condylar head 2. Sigmoid notch 3. Coronoid process 4. External oblique ridge5. Mandibular canal
23
4
5
6. Post. Border of Ramus 8. Lower border7. Gonial Angle
6
7
9. Mental ridge 11. Mental foramen 10. Genial tubercle13. Lingula
12. External Oblique Ridge14. Hyoid bone
8
9
1011
1213
14

BONY LANDMARKS IN MAXILLA
15
15
15. Glenoid fossa19. Floor of Max.Sinus
17. Zygomatic Arch16. Articular eminence 18.Post. wall max. sinus20. Zygomatic process of max. forming innominate line
21. Hard palate 22. Floor of the orbit 23. Nasal septum 24. Incisive foramen25. Inferior choncha 26. Meatus 27. Frontal process of Z.bone
1617
18
19
2021
22 2329
25
24
26
28.Pterygo max. fissure30. Maxillary tuberosity29.Spine of the sphenoid bone 31. Lateral pterygoid plate
3130
2827

OTHER STRUCTURES
16
32
32. External acoustic meatus 34. Shadow of ear lobe33. Styloid process35. nose 36. Shadow of Cervical spine
33
34
35
36 37
37. Cervical vertebrae
38
38. Nasopharyngeal space 39. Shadow of uvula
40
39
40 Submandibular fossa

A panoramic film is not as useful as periapical radiography for detecting small carious lesions, periodontal diseases, or periapical lesions.
It should not be used as a substitute for intraoral films.

Impacted teeth and its relation with the mandibular canal.

To evaluate eruption patterns

To detect diseases, lesions, conditions of the jawsand the extent of large lesions.

to evaluate trauma

Retained teeth or root tips in edentulous patients

Post-operative examination and patient education.

Implants

ROTATION CENTER
The pivotal point or axis, around which the cassette carrier and X-ray tubehead rotate, is termed a ROTATION CENTER.

Double center of rotation

Three stationary centers of rotation

Continously moving center of rotation


During the exposure cycle, the machine shifts to one or more additional rotation centers.
This rotational change allows the image layer to conform to the shape of the dental arches.
The location and no. of rotational centers influence the size and shape of the focal trough.

Focal troughThe focal trough (also known as the Image layer) is defined as a 3-D curved zone in which structures are clearly demonstrated on a panoramic radiograph.

Advantages
1. Field size
2. Minimal exposure
3. Simplicity
4. Patient cooperation
5. Useful in patients with trismus & gagging
6. Valuable visual aid for patient education

Disadvantages
1. Cannot be used in detection of caries and periodontal disease.
2. Overlapping of teeth in premolar region
3. Focal trough limitations
4. Shadow of cervical spine in the lower anterior region.
5. Ghost images
6. Equipment cost

34
COMMON ERRORS

PATIENT POSITIONING
ERRORS

Positioning of lips and tongue

Positioning of Frankfort plane upward

Positioning of Frankfort plane downward

Positioning of teeth anterior to focal trough

Positioning of teeth posterior to focal trough

Positioning of midsagittal plane

Patient movement

Positioning of spine

Processing Errors
Underexposed, light, washed out imageVery dark film, Overexposed
Film Fog
Improper filter in daylight loader

Panoramic Image= Right lateral image+PA image+Left Lateral image

04/07/2023 46
EXTRAORAL RADIOGRAPHI
C TECHNIQUES

LATERAL CEPHALOMETRIC PROJECTIONFilm position - cassette is placed perpendicular to the floor with long axis of the cassette placed vertically.
Position of patient - left side of the face is positioned against the cassette. Mid sagittal plane is perpendicular to the floor and parallel to film.
Central ray - perpendicular to the film.

Exposure parametersKVp= 84mAs= 13Seconds =1.6

INDICATIONS• To evaluate fac ia l growth and
development, t rauma, d isease and developmental anomal ies.
• Demonstrates the bones of the face, skul l as wel l as the soft t i ssue profile of the face.

Film position - cassette is perpendicular to the floor with long axis of the cassette placed vertically.
Position of patient –The film is adjusted so that the upper circumference of the skull is .5 inch below the lower border of the cassette.
Central ray - perpendicular to the film towards the E.A.M.
TRUE LATERAL SKULL

51
LATERAL SKULL PROJECTION
Exposure parameters KVp= 65 mAs= 10 Seconds =.5-2 sec

To survey skull and facial bone for trauma or pathology.
Nasopharangeal soft tissue, paranasal sinus and hard palate.
Condition affecting sella turcica, such as tumour of pitutary gland in acromegaly.
Indications

5304/07/2023
PA WATERS PROJECTIONFilm position - cassette is perpendicular to the floor with long axis of the cassette placed vertically.
Position of patient - mid sagittal plane perpendicular to the floor and parallel to film.Head is extended so that only the chin touches the casette.The tip of nose is .5 to 1.5 cm away from the cassette
Central ray- perpendicular and to the midpoint of the film.

54
Exposure parameters• KVp= 65 • mAs= 10 • Seconds =2-3 sec

55
INDICATIONS
• Demonstrate the maxillary , frontal and ethmoidal sinuses.
• The orbit, frontozygomatic suture, nasal cavity, coronoid process of the mandible and the zygomatic arch are also seen.

56
Film position- cassette is placed perpendicular to the floor with long axis of the cassette placed horizontally.Position of patient- head is centered on the cassette (Head and neck tipped back).Vertex of the skull touches the cassette.Central raY- perpendicular to the film. It enters via between angle of mandible and in a coronal plane ¾ inches anterior to the external auditory meatus.
SUBMENTOVERTEX (BASE) PROJECTION

57
SUBMENTOVERTEX (BASE) PROJECTION
Exposure parameters
KVp= 50 mAs= 20 Seconds =.4

58
INDICATIONS
Help to study destruct ive les ion affect ing the palate, pterygoid region or base of the skul l , sphenoidal s inus.
Fractures of zygomatic arches ( JUG HANDLE).

LATERAL OBLIQUEFilm position - flat against the patient cheeks and is centered over the body of the mandible.Position of patient - ala tragus line is parallel to the floor. Inferior border of the cassette should be parallel to the lower border of the mandible and below it.Central ray - directed 2cm behind the angle of the mandible and beam is directed -10° to -15°

Exposure parameters
KVp= 65-70 mAs= 10 Seconds =.8

61
Lateral Oblique Views - Largely replaced by panoramic views
Indications: • Impacted third molars • fractures of the ramus, condyle or body of
the mandible.

62

63
TRANSCRANIAL VIEWFilm position - cassette is
placed flat against the patient ear and centred over the TMJ of interest.
Position of patient - head is adjusted so that the saggital plane is vertical.
The ala tragus is parallel to floor.
Central ray - is ½ inch behind and 2 inch above the auditory meatus

64
Exposure parameters
KVp= 70 mAs= .7 Seconds =1.5
Indications
• Arthritic changes on the articular surface.• To evaluate the joint’s bony relationship.

65
TRANSPHARYNGEAL VIEWFilm position - cassette is placed flat against the patient ear and is centered to a point ½’” anterior to ext. auditory meatus, over the TMJ of interest.
Position of patient - head is adjusted so that the saggital plane is vertical.The ala tragus is parallel to floor.
Central ray - from the opposite side cranially at an angle -5° to -10°.

66
INDICATIONS• Fracture of condylar head and neck of the mandible
Exposure parameters
KVp= 70 mAs= 7 Seconds =1.5

67
TRANSORBITAL/ZIMMER VIEWFilm position - cassette is placed behind the patient’s head at an angle of 45° to the saggital plane.
Position of patient - head is adjusted so that the saggital plane is vertical. The canthomeatal line is parallel to floor. The mouth should be wide open.
Central ray - from the opposite side cranially at an angle -5° to -10°.

68
INDICATIONS The anterior view of the temporomandibular joint Medial displacement of fractured condyle Fracture of neck of condyle. There is minimum superimposition.
Exposure parameters
KVp= 70 mAs= 7 Seconds =.8

69
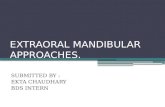
REVERSE-TOWNE PROJECTION(OPEN MOUTH)
Film position - cassette is placed perpendicular to the floor with long axis of the cassette placed horizontally.
Position of patient- Pt. forehead and tip of the nose should touch the film and is asked to keep his mouth wide open
Central ray- directed via mid saggital plane at the level of the mandible and is perpendicular to the film.

70
Exposure parameters
KVp = 65 mAs = 10 Seconds = 2-3
INDICATIONS:
• Suspected fracture of the condylar neck.
• Intracapsular fracture of the TMJ
• Shows posterolateral wall of maxillary sinus

71
DRAWBACKS OF EXTRA ORAL TECHNIQUES
Magnification occurs due to the greater object to film distance used.
Details are not well defined.Contrast is reduced as the secondary
radiation produced by the soft tissues is more.
It is a 2- D image of 3- D structure.

CONCLUSION Thorough knowledge of the indications
of various extra oral techniques allows accurate and timely diagnosis of various maxillofacial pathologies. Further, we can arrive at a diagnosis with minimum number of x-rays there by reducing patient exposure to radiation.

• White SC, Pharoah MJ.Oral Radiology Principles And Interpretations.6 thelsevier:: Missouri; 2009
• Mac Donald,Avery.Dentistry For The Child And Adolscent.9th.elsevier: Missouri; 2011
• Langland and Langlais.. Principles Of Dental Imaging.7thed.elsevier: Muir; 2005
• Freny R,Karjodkar.Textbook Of Dental And Maxillofacial Radiology.6thed.elsevier: Reed; 2000
• Dental radiography, Principles and Techniques; Haring, Howerton;Third edition.

DR ANKIT GOEL, SUBHARTI.