Operative Technique for Converting a Failed Vertical Banded Gastroplasty to Roux-en-Y Gastric Bypass
9
Operative Technique for Converting a Failed Vertical Banded Gastroplasty to Roux-en-Y Gastric Bypass Rodrigo Gonzalez, MD, Scott F Gallagher, MD, Krista Haines, BA, Michel M Murr, MD, FACS BACKGROUND: Bariatric surgeons are increasingly encountering patients with failed weight-loss operations. Conversion from vertical banded gastroplasty (VBG) to Roux-en-Y gastric bypass (RYGB) is the most common revisional operation in our practice. We reviewed our experience in convert- ing from VBG to RYGB using a basic five-step surgical technique. STUDY DESIGN: We reviewed data on all patients undergoing revisional surgery for failed VBG, defined as patients with body mass index 35 kg/m 2 , weight gain, poor control of comorbidities, staple- line dehiscence, or band-specific complications. The five basic steps include identification of the band, delineation of the extent of the pouch, division of the stomach, preparation of the Roux limb, and completion of the cardiojejunostomy. RESULTS: We have undertaken 28 conversions from VBG to RYGB. Median age was 51 years (range 27 to 65 years), preoperative body mass index was 40 kg/m 2 (range 20 to 58 kg/m 2 ), and 25 patients (89%) were women. Indications for revision were band-related complications (13 patients), staple-line disruption (9 patients), and inadequate weight loss (6 patients). Median operative time was 185 minutes (range 105 to 465 minutes), estimated blood loss was 450 mL (range 100 to 2,500 mL), postoperative complications occurred in 6 patients (21%), and length of hospitalization was 5 days (range 3 to 69 days). Median postoperative body mass index was 32 kg/m 2 (range 20 to 41 kg/m 2 ) at a followup time of 16 months (range 1 to 32 months). CONCLUSIONS: The technique described facilitates the operative approach to patients with failed VBG, pro- viding guidelines for safe dissection and division of the gastric pouch for conversion to RYGB. Revisional bariatric operations are technically difficult and are associated with relatively higher complication rates than those reported for primary operations. (J Am Coll Surg 2005;201: 366–374. © 2005 by the American College of Surgeons) Bariatric surgery offers sustainable weight loss, with amelioration of obesity and its related comorbidities. The 1991 National Institutes of Health Consensus Con- ference recognized the vertical banded gastroplasty (VBG) and Roux-en-Y gastric bypass (RYGB) as the 2 operations proved to effectively induce longterm weight loss and improve or completely resolve obesity-related comorbidities. 1 The technical ease and fewer complica- tions made VBG the procedure of choice for many bari- atric surgeons in the 1980s. But because of suboptimal, longterm weight loss, the majority of bariatric surgeons have abandoned the VBG in favor of the RYGB. 2-4 It has been reported that 5% to 36% of patients require revi- sional surgery for failed VBG, 4-6 and approximately 56% of patients are projected to require revisional surgery after VBG over a 12-year period. 7 Conversion of a failed or complicated VBG to RYGB will eliminate the untoward effects (ie, band erosion, stomal stenosis, gastroesophageal reflux disease [GERD] symptoms, and maladaptive eating behavior) while in- ducing durable weight loss. 7-14 Nevertheless, knowledge of the operative technique for converting failed VBG is important to ensure satisfactory outcomes given the technical difficulty of this procedure. 7-14 Most series of revisional surgery in the literature include a wide variety of failed bariatric operations and lack a detailed descrip- tion of the operative technique for conversion to RYGB. The aim of this article is to review our experience and to describe a standardized surgical technique for convert- Competing Interests Declared: None. Received November 4, 2004; Revised March 9, 2005; Accepted April 7, 2005. From the Interdisciplinary Obesity Treatment Group, Department of Sur- gery, University of South Florida College of Medicine,Tampa, FL. Correspondence address: Michel M Murr, MD, FACS, University of South Florida College of Medicine, c/o Tampa General Hospital, PO Box 1289, Tampa, FL 33601. 366 © 2005 by the American College of Surgeons ISSN 1072-7515/05/$30.00 Published by Elsevier Inc. doi:10.1016/j.jamcollsurg.2005.04.022
-
Upload
rodrigo-gonzalez -
Category
Documents
-
view
216 -
download
1
Transcript of Operative Technique for Converting a Failed Vertical Banded Gastroplasty to Roux-en-Y Gastric Bypass

OB
R
BaTf(olctal
C
R2FgCFT
©P
perative Technique for Converting a Failed Verticalanded Gastroplasty to Roux-en-Y Gastric Bypass
odrigo Gonzalez, MD, Scott F Gallagher, MD, Krista Haines, BA, Michel M Murr, MD, FACS
BACKGROUND: Bariatric surgeons are increasingly encountering patients with failed weight-loss operations.Conversion from vertical banded gastroplasty (VBG) to Roux-en-Y gastric bypass (RYGB) isthe most common revisional operation in our practice. We reviewed our experience in convert-ing from VBG to RYGB using a basic five-step surgical technique.
STUDY DESIGN: We reviewed data on all patients undergoing revisional surgery for failed VBG, defined aspatients with body mass index �35 kg/m2, weight gain, poor control of comorbidities, staple-line dehiscence, or band-specific complications.The five basic steps include identification of theband, delineation of the extent of the pouch, division of the stomach, preparation of the Rouxlimb, and completion of the cardiojejunostomy.
RESULTS: We have undertaken 28 conversions from VBG to RYGB. Median age was 51 years (range 27to 65 years), preoperative body mass index was 40 kg/m2 (range 20 to 58 kg/m2), and 25patients (89%) were women. Indications for revision were band-related complications (13patients), staple-line disruption (9 patients), and inadequate weight loss (6 patients). Medianoperative time was 185 minutes (range 105 to 465 minutes), estimated blood loss was 450 mL(range 100 to 2,500 mL), postoperative complications occurred in 6 patients (21%), and lengthof hospitalization was 5 days (range 3 to 69 days). Median postoperative body mass index was32 kg/m2 (range 20 to 41 kg/m2) at a followup time of 16 months (range 1 to 32 months).
CONCLUSIONS: The technique described facilitates the operative approach to patients with failed VBG, pro-viding guidelines for safe dissection and division of the gastric pouch for conversion to RYGB.Revisional bariatric operations are technically difficult and are associated with relatively highercomplication rates than those reported for primary operations. ( J Am Coll Surg 2005;201:
366–374. © 2005 by the American College of Surgeons)hbsoa
wssdoitrotT
ariatric surgery offers sustainable weight loss, withmelioration of obesity and its related comorbidities.he 1991 National Institutes of Health Consensus Con-
erence recognized the vertical banded gastroplastyVBG) and Roux-en-Y gastric bypass (RYGB) as the 2perations proved to effectively induce longterm weightoss and improve or completely resolve obesity-relatedomorbidities.1 The technical ease and fewer complica-ions made VBG the procedure of choice for many bari-tric surgeons in the 1980s. But because of suboptimal,ongterm weight loss, the majority of bariatric surgeons
ompeting Interests Declared: None.
eceived November 4, 2004; Revised March 9, 2005; Accepted April 7,005.rom the Interdisciplinary Obesity Treatment Group, Department of Sur-ery, University of South Florida College of Medicine, Tampa, FL.orrespondence address: Michel M Murr, MD, FACS, University of Southlorida College of Medicine, c/o Tampa General Hospital, PO Box 1289,
dampa, FL 33601.
3662005 by the American College of Surgeons
ublished by Elsevier Inc.
ave abandoned the VBG in favor of the RYGB.2-4 It haseen reported that 5% to 36% of patients require revi-ional surgery for failed VBG,4-6 and approximately 56%f patients are projected to require revisional surgeryfter VBG over a 12-year period.7
Conversion of a failed or complicated VBG to RYGBill eliminate the untoward effects (ie, band erosion,
tomal stenosis, gastroesophageal reflux disease [GERD]ymptoms, and maladaptive eating behavior) while in-ucing durable weight loss.7-14 Nevertheless, knowledgef the operative technique for converting failed VBG ismportant to ensure satisfactory outcomes given theechnical difficulty of this procedure.7-14 Most series ofevisional surgery in the literature include a wide varietyf failed bariatric operations and lack a detailed descrip-ion of the operative technique for conversion to RYGB.he aim of this article is to review our experience and to
escribe a standardized surgical technique for convert-ISSN 1072-7515/05/$30.00doi:10.1016/j.jamcollsurg.2005.04.022

iss
MTBouww�tetmlR
qwgfRgus
gsbbp
OVfetc
IrTttt1ifgtfdltpba
DTttpmaiug(
DIaTdtwptopgltctp
367Vol. 201, No. 3, September 2005 Gonzalez et al Technique for Revisional Bariatric Surgery
ng VBG to RYGB. Our technique consists of five basicteps, which we have found useful in approaching revi-ional procedures.
ETHODShis study was approved by the Institutional Reviewoard (IRB) of the University of South Florida Collegef Medicine. Prospectively collected data on all patientsndergoing revisional bariatric surgery for failed VBGere reviewed. Failure to achieve adequate weight lossas defined as patients with a body mass index (BMI)35 kg/m2, weight gain, or poor control of comorbidi-
ies. Comorbidities were described as obesity-related dis-ases that improve or resolve with weight loss. Resolu-ion of comorbidities was defined as discontinuingedications to control a specific disease after weight
oss. All operations consisted of converting from VBG toYGB.Patients with anatomically intact VBG and inade-
uate weight loss (less than 50% of the excess bodyeight), patients with band-specific complications re-ardless of their weight loss, and patients with staple-lineailure were also considered candidates for conversion toYGB. Band-specific complications that prompted sur-ical revision included stenosis, band erosion, stomallcers, intractable bleeding, and refractory GERDymptoms.
All patients underwent at least an endoscopy, upperastrointestinal contrast study, or an abdominal CTcan before operation and a comprehensive evaluationy our multidisciplinary bariatric team, including aariatrician, nutritionist, psychologist, cardiologist, andulmonologist.
perative techniqueBG is converted to a vertical disconnected RYGB in
ive steps: identification of the band; delineation of thextent of the pouch; division of the stomach; prepara-ion of the Roux limb; and completion of the
Abbreviations and Acronyms
BMI � body mass indexEBWL � excess body weight lossGERD � gastroesophageal reflux diseaseRYGB � Roux-en-Y gastric bypassVBG � vertical banded gastroplasty
ardiojejunostomy. s
dentification of the band or the silicone elastomeringhis is facilitated by inserting a large-caliber orogastric
ube to delineate the VBG pouch. We start by dissectinghe left lobe of the liver, which is usually firmly adheredo the band and the anterior surface of the stomach (Fig.). At the time of the original gastroplasty, the omentums often interposed between the band and the undersur-ace of the left lobe of the liver, making it hard to distin-uish between the gastrocolic and gastrohepatic omen-um. Identifying the location of the band may beacilitated by entering the lesser sac. The band can beissected circumferentially and removed at this stage, or
ater with a partial gastrectomy if it is densely adhered tohe stomach. Alternatively, provided that the VBGouch drains freely into the excluded stomach, intactands (nonobstructive or eroded) can be left in placefter division of the proximal gastric pouch.
elineation of the extent of the pouchhe extent of the VBG pouch is delineated by dissecting
he overhang in a dilated pouch and localizing the ver-ical staple line. A gastrotomy at the distal end of theouch might be necessary to introduce a blunt instru-ent that identifies the extent of the dilated VBG pouch
t the angle of His and to determine if there is disruptionn the vertical staple line. This gastrotomy will later besed to insert the anvil of the circular stapler in a retro-rade fashion in preparation for the cardiojejunostomyFig. 2).
ivision of the stomachn preparation for this step, the angle of His is dissectednd a retrogastric passage to the lesser curvature is made.he neurovascular bundle is identified, preserved, andissected from the lesser curvature distal to the left gas-ric artery but proximal to the band to create a smallindow that will admit two linear staplers. A suture islaced at the angle of His to mark the proximal end ofhe VBG vertical staple line and to guide the positioningf the linear staplers used to divide the proximal gastricouch of the RYGB. A red rubber catheter is used touide the linear staplers between the window in theesser curvature and the angle of His (Fig. 2). This ana-omically directed dissection of the VBG pouch andardia preserves the left gastric artery and its branches tohe cardia while avoiding unnecessary dissection of thehrenoesophageal ligament, preserving adequate blood
upply to the RYGB pouch.
tlapsdsgpaislssl
POsptjlRkmk
CTtrgtasar
Fltlgct
368 Gonzalez et al Technique for Revisional Bariatric Surgery J Am Coll Surg
The pouch of the RYGB is constructed by positioninghe 90-mm linear stapler proximal to the vertical stapleine of the VBG, as guided by the marking suture placedt the angle of His. The distal portion of the VBGouch, including its stoma, is distal to this second lineartapler, allowing the distal part of the VBG pouch torain into the distal stomach (Fig. 3). When the stoma istenotic and the VBG vertical staple line is intact, aastrogastrostomy will guarantee drainage of the distalart of the pouch to the distal and now excluded stom-ch. Alternatively, when the proximal pouch of the VBGs small or the band has eroded into the stomach, theecond linear stapler is applied distal to the first stapleine, but in such manner as to include the entire verticaltaple line of the VBG between the two staplers and thetoma. The remaining stomach between the two stapleines is then resected, creating a disconnected RYGB.
reparation of the Roux limbnce the stomach is divided between the two linear
taplers, the subsequent steps are similar to those of arimary RYGB. The Roux limb is prepared by dividinghe proximal jejunum at a point of maximal mobility. Aejunojejunostomy is completed with a 100-cm Rouximb in patients with BMI� 49 kg/m2 and a 150-cmoux limb in patients with BMI between 50 and 59g/m2. We perform a jejunoileostomy at 100 cm proxi-al to the ileocecal valve for patients whose BMI is� 60
g/m2.15
ompletion of the cardiojejunostomyhe last step is to complete a side-to-side cardiojejunos-
omy using a 21-mm circular stapler. The anvil has al-eady been introduced into the VBG pouch through aastrotomy and exteriorized through the anterior wall ofhe cardia. The Roux limb is brought up to the upperbdomen in an antecolic position. The 21-mm circulartapler is introduced from the open end of the Roux limbnd is mated with the anvil. The circular staple line isoutinely reinforced with interrupted sutures.
A gastrostomy tube is routinely placed in the excluded
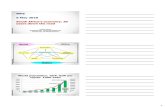
igure 1. Once the band is located (lower arrow), the vertical stapleine (upper arrow), which forms a crease that extends from the bando the angle of His, can be easily identified. The band and the stapleine delineate the borders of the pouch of the vertical bandedastroplasty. Exposure of these elements may sometimes be diffi-ult because of dense adhesions to adjacent structures, especially
he left lobe of the liver.
dpcaurg
RWoRmtdhba
p14(hmc
si(qftpTVljA
FiSwclHp
369Vol. 201, No. 3, September 2005 Gonzalez et al Technique for Revisional Bariatric Surgery
istal stomach to prevent gastric dilation during theostoperative period. Additionally, we routinely placelosed suction drains around the cardiojejunostomy. Asprecaution in these patients, we perform the routinepper gastrointestinal series 48 hours postoperatively,ather than on postoperative day 1, as in patients under-oing primary bariatric surgery.
ESULTSe have undertaken a total of 52 revisional bariatric
perations, including 28 conversions from VBG toYGB. These 28 patients had undergone VBG at aean of 12 years before the revisional operation (range 1
o 23 years). Two patients had an earlier bariatric proce-ure that had been converted to a VBG: the first patientad an earlier jejunoileal bypass converted to a VBGecause of oxalate nephropathy; the second patient hadn earlier horizontal gastroplasty converted to a VBG.
Median age was 51 years (range 27 to 65 years), 25atients (89%) were women, preoperative weight was10 kg (range 58 to 182 kg), and preoperative BMI was0 kg/m2 (range 20 to 58 kg/m2). Fourteen patients50%) were older than 50 years and 10 patients (36%)ad a BMI greater than 35 kg/m2. Obesity-related co-orbidities were present in 19 patients (68%), the most
ommon being GERD, as listed in Table 1.The preoperative diagnoses that prompted conver-
ion of VBG to RYGB were: band-related complicationsn 13 patients (46%), staple-line dehiscence in 9 patients32%), and an anatomically intact VBG with inade-uate weight loss in 6 patients (21%). Intraoperativeindings in the 22 patients with VBG-related complica-ions were staple-line disruption,10 followed by enlargedouch,9 stenosis,8 band erosion,3 and marginal ulcer.2
able 2 summarizes the intraoperative findings of theBG-related complications. In patients with an en-
arged pouch, the distance between the esophagogastricunction and the band was between 8 cm and 20 cm.ll patients with an enlarged pouch reported GERD
igure 2. Once the extent of the pouch is delineated, a gastrotomys done to introduce the anvil of the circular stapler (lower arrow).taple line dehiscence can be verified by exploring the staple lineith a blunt instrument through the gastrostomy. Two red rubberatheters are passed through a retrogastric tunnel between theesser curvature (inferior to the left gastric artery) and the angle ofis to guide the introduction of the staplers used to divide the
roximal gastric pouch of the gastric bypass (upper arrow).
se
41ceiibwai(l(ias
tattanedcettst
k3
Fppastrtoge
370 Gonzalez et al Technique for Revisional Bariatric Surgery J Am Coll Surg
ymptoms; no patient was diagnosed with Barrett’ssophagus.
Median operative time was 185 minutes (range 105 to65 minutes), estimated blood loss was 450 mL (range00 to 2,500 mL), and transfusion of packed red bloodells was required in 3 patients (11%) because of periop-rative bleeding. Intraoperative complications includedncidental enterotomies in 2 patients (7%) and a splenicnjury requiring splenectomy in 1 patient (4%). Theand was completely removed in all but two patients inhom extensive adhesions to the posterior wall hinderedsafe dissection. A partial gastrectomy was undertaken
n 2 patients (7%) for band erosion and in 2 patients7%) for resection of undrained stomach between stapleines. A gastrostomy tube was placed in 26 patients93%). Additional surgical procedures were carried outn 11 patients (39%), including cholecystectomy (21%)nd incisional hernia repair (14%). Median length oftay was 5 days (range 3 to 69 days).
Early postoperative complications (within 30 days af-er operation) occurred in 9 patients (32%), includingn anastomotic leak in 5 patients (18%), wound infec-ion in 2 patients (7%), and deep venous thrombosis inhe right internal jugular and subclavian vein requiringnticoagulation and postoperative upper gastrointesti-al bleeding requiring blood transfusions in 1 patientach (4%). One patient had CT-guided percutaneousrainage of an abscess after developing a leak from theardiojejunostomy. One of the leaks originated from thexcluded stomach in a patient who underwent a splenec-omy with her VBG; a gastrostomy tube was inserted athe time of conversion but the leak developed at thetaple line; this patient developed sepsis followed by mul-iorgan failure and died 3 months postoperatively.
Postoperative BMI was 32 kg/m2 (range 20 to 41g/m2) at a median followup of 16 months (range 1 to6 months).This corresponds to an overall percentage of
igure 3. The proximal gastric pouch of the Roux-en-Y gastric by-ass (RYGB) (arrow) is divided using two linear staplers placedroximal to the staple line of the vertical banded gastroplasty (VBG),llowing the distal part of the VBG pouch to drain into the distaltomach. Blood supply to the RYGB pouch is assured by preservinghe neurovascular bundle and the left gastric artery (identified by theight angle instrument). The band is usually dissected circumferen-ially and removed. In case of extensive adhesions, nonobstructiver noneroded bands can be left in place after division of the proximalastric pouch provided that the VBG pouch drains freely into the
xcluded stomach.
ePl3p6awoBf2mbRTm
toitdf
tvwvpoip(sAs
DTporscnratieiwvVqi
swcG
T
O
GOHDDD 11
TGUpV
SEBBBBBBB
V
371Vol. 201, No. 3, September 2005 Gonzalez et al Technique for Revisional Bariatric Surgery
xcess body weight loss (%EBWL) of 48% (3% to 71%).atients undergoing operation for inadequate weight
oss after VBG had a median %EBWL of 59% (range0% to 71%); patients undergoing operation for com-lications had a median %EBWL of 39% (range 3% to3%). Two patients who had a history of food intoler-nce, prolonged vomiting, and excessive weight lossere operated on for severe VBG outlet obstruction sec-ndary to band stenosis. One patient had a preoperativeMI of 20 kg/m2 and had lost 2 pounds at the 3-month
ollowup. The second patient had a preoperative BMI of4 kg/m2 and had lost 14 pounds at her last visit 9onths postoperatively. Since then, these patients have
een able to eat properly and their weight loss stabilized.esolution of obesity-related comorbidities is listed inable 1; hypertension was the comorbidity most com-only resolved.Additionally, 4 patients (14%) required readmission
o the hospital because of complications within 4 weeksf the operation. Three patients reported nausea, vom-ting, and abdominal pain. One patient had a stenosis athe cardiojejunostomy requiring multiple endoscopicilations. Extensive evaluation in the other two patientsailed to demonstrate any abnormality requiring specific
able 1. Preoperative Incidence and Resolution of Obesity-R
besity-related comorbidityPreoperative
n
astroesophageal reflux disease 14bstructive sleep apnea 8ypertension 8iabetes mellitus 7egenerative joint disease 4yslipidemia 3
able 2. Intraoperative Findings of 32 Vertical Bandedastroplasty-Related Complications Found in 22 Patientsndergoing Conversion from Failed Vertical Banded Gastro-lasty to Roux-en-Y Gastric BypassBG-related complication n %
taple-line disruption 7 32nlarged pouch 5 23and stenosis 3 14and stenosis � enlarged pouch 3 14and stenosis � marginal ulcer 2 9and stenosis � staple-line disruption 2 9and erosion 1 5and erosion � enlarged pouch 1 5and erosion � staple-line disruption 1 5
gBG, vertical banded gastroplasty.
reatment. The fourth patient was readmitted for deepenous thrombosis and pulmonary embolism, whichere treated with anticoagulation; subsequently, she de-eloped lower gastrointestinal bleeding and requiredlacement of an inferior vena cava filter. Other late post-perative complications occurred in 7 patients (25%),ncluding stenosis requiring endoscopic dilations in 3atients (11%), incisional hernia in three patients11%), and small bowel obstruction secondary to adhe-ions requiring surgical treatment in 1 patient (4%).dditionally, 6 patients (21%) reported longterm foul-
melling diarrhea.
ISCUSSIONhe increasing demand for bariatric surgery has beenaralleled by a rise in the frequency of revisional bariatricperations. We recommend converting all failed bariat-ic operations to RYGB because it induces durable andustainable weight loss and corrects most of the compli-ations after these operations (ie, gastroplasty and jeju-oileal bypass).7,8,10,13,14,16 Nevertheless, revisional bariat-ic surgery may be extremely challenging and has beenssociated with higher early and longterm morbidityhan primary RYGB. So it is advisable that surgeonsnvolved in treating clinically significant obesity becomexperienced in primary bariatric surgery before attempt-ng revisional procedures in patients with failed previouseight-loss operations. We describe here the steps in-olved in the conversion from failed or complicatedBG to RYGB. We believe that using a standard se-uence of steps facilitates the procedure and may reducentraoperative complications and improve outcomes.
VBG was the operation of choice for many bariatricurgeons during the 1980s. But reports of unsatisfactoryeight loss and a relatively high incidence of longterm
omplications (ie, emesis, maladaptive eating syndrome,ERD, and band-related complications) prompted sur-
ed Comorbidities in 19 PatientsPostoperative
Resolution, nn %
2 7 863 11 631 4 882 7 712 7 501 4 67
elat
%
5029292515
eons to abandon the VBG in favor of the RYGB. Re-

vumsaVtwv
tVl5eVglpla
adsaaItpccphrs
umnsLcprss
aromod
cwVwatrfco
vhe3RBpRVr
tmsvtpRbstslaldwr
372 Gonzalez et al Technique for Revisional Bariatric Surgery J Am Coll Surg
ising the VBG by restapling or tightening the band fornsatisfactory weight loss produced dismal results. Asany as 56% of patients with VBG will require revi-
ional surgery over a 12-year period compared with nonefter conversion to RYGB.7 Converting from failedBG to RYGB has been reported to be more effective
han revising the VBG. Consequently, many patientsith failed VBG undergo conversion to RYGB as a sal-age operation.
Similar to what has been described in the litera-ure,12,17 the most common indication for revision ofBG in our series was dehiscence of the vertical staple
ine. Staple-line dehiscence has been reported in up to0% of patients and is the most common cause of inad-quate weight loss in patients requiring revision of theBG, because it eliminates the restrictive nature of theastroplasty.4 Staple-line disruption or gastric pouch di-atation has been treated by restapling the stomachouch. But a high incidence of complications such as
eaks and ischemia has been reported after thispproach.7,8,10
Symptoms of GERD are reported in 40% of patientsfter VBG. These symptoms can occur from postpran-ial esophageal loading or true reflux from the distaltomach. Staple-line disruption may allow passage ofcid into the pouch and into the esophagus. Addition-lly, large pouches may include acid-secreting mucosa.n patients with an intact VBG undergoing conversiono RYGB because of severe GERD symptoms, it is re-orted that 96% of patients have a complete or near-omplete resolution of heartburn symptoms, 88% dis-ontinue antireflux medications, and all patients withreoperative endoscopically documented esophagitisave complete resolution without progression to Bar-ett’s esophagus.14 In our cohort, GERD symptoms re-olved in 86% of patients.
Stomal stenosis has been reported in 5% of patientsndergoing VBG.9,18-20 Its pathogenesis is unclear, but itight result from ulceration of the stomal canal or ste-
osis from a fibrotic reaction to the band. Patients withtomal stenosis report vomiting, rapid satiety, or GERD.ong-standing stenosis can lead to lack of propulsiveontractile activity in a chronically enlarged, atonic,roximal pouch. In addition, associated vomiting couldesult in severe malnutrition. Endoscopic dilations oftenotic stomas offer only temporary relief, so conver-ion to RYGB is warranted.
The incidence of band erosion is between 1% and 7% r
t 3 years after VBG.4,18,20,21 Erosion of the band canesult in bleeding, nonhealing ulceration, mechanicalbstruction, and, rarely, perforation. Endoscopic re-oval of eroded bands has been successful in small series
f patients,22 but it does not address the underlyingense scarring, which may require a revisional operation.In patients with anatomically intact VBG, excessive
aloric intake may be the primary cause for inadequateeight loss. Brolin and colleagues16 reported that theBG adversely alters postoperative eating behavior to-ard soft, high-calorie foods. Similarly, Sugerman and
ssociates2 attributed inconsistent weight loss after VBGo abuse of sweets. It is important to keep in mind thatevisional bariatric procedures undertaken exclusivelyor inadequate weight loss might have inferior resultsompared with primary operations because of the previ-usly mentioned maladaptive eating behavior.
On the other hand, sustained weight loss after con-ersion to RYGB because of VBG-related complicationsas also been well documented. Sugerman and cowork-rs13 reported an increase in excess body weight loss from6% to 67% 1 year after conversion from VBG toYGB. Westling and colleagues17 reported a decrease inMI from 35 kg/m2 to 28 kg/m2 after conversion ofreviously unsuccessful gastric restrictive procedures toYGB. Patients undergoing conversion of an intactBG to RYGB because of severe GERD symptoms are
eported to increase the %EBWL from 59% to 83%.14
Revisional bariatric surgery is associated with rela-ively increased complication rates compared with pri-ary bariatric surgery, especially anastomotic failures
uch as strictures and leaks.9,13,14,17,18,23 Scarring from pre-ious inflammatory reaction to the foreign material (inhis case, the band) may provide inadequate tissue toerform the anastomosis. When converting a VBG toYGB, division of the stomach is done well above theand and above the portion of the stomach previouslytapled to create the VBG pouch. So the cardiojejunos-omy of the RYGB is performed in a previously unusedegment of the stomach. Nevertheless, the incidence ofeaks in revisional surgery is higher than in primary bari-tric surgery. We have a low threshold for diagnosis of aeak based on radiologic findings or change in surgicalrain output. By the same token, two of the patientsho developed leaks were treated nonoperatively and
equired no further intervention.Two recently published analyses found revisional bariat-
ic surgery to be among the most influential factors predic-

tiips
tCmfspsalt
sRaotmtmssdvtptt
ASAADCS
R
1
1
1
1
1
1
1
1
1
1
2
2
2
373Vol. 201, No. 3, September 2005 Gonzalez et al Technique for Revisional Bariatric Surgery
ive of leaks after RYGB.24,25 This high complication ratellustrates the high complexity of these patients, the signif-cance of describing a detailed operative approach to theseatients, and the importance of only experienced bariatricurgeons undertaking these challenging operations.
The longterm safety and efficacy of converting VBGo RYGB have been previously documented.7,8,10,13,14,16
onversion of restrictive procedures to other purelyalabsorptive procedures has not been undertaken as
requently, so longterm data are lacking. Csepel and as-ociates26 reported satisfactory results after convertingatients with failed LapBand to biliopancreatic diver-ion. Their experience was with only two patients, with
short followup. Further experience and longer fol-owup would be desirable before recommending theseypes of revisional bariatric operations.
In summary, we describe here five basic steps of atandardized technique for converting failed VBG toYGB based on anatomically directed dissection. Usingcombination of preoperative studies and simple intra-perative maneuvers, the size of the VBG pouch is de-ermined. Dissection of the pouch is undertaken in aanner to preserve blood supply to the cardia through
he left gastric artery. Partial resection of the stomachay be necessary to remove bands that eroded into the
tomach and eliminate any undrained segments of thetomach. Similarly, avoiding tension and excessiveevascularization of the Roux limb is essential in pre-enting anastomotic failures. Placement of a gastros-omy tube helps to decompress the excluded stomach inatients who develop delayed gastric emptying. Usinghese techniques has minimized postoperative complica-ions to the level of complications after primary RYGB.
uthor Contributionstudy conception and design: Gonzalezcquisition of data: Hainesnalysis and interpretation of data: Gonzalezrafting of manuscript: Gonzalezritical revision: Gallagherupervision: Murr
EFERENCES
1. NIH Consensus Conference. Gastrointestinal surgery for severeobesity. Consensus Development Conference Panel. Ann InternMed 1991;115:956–961.
2. Sugerman HJ, Starkey JV, Birkenhauer A. A randomized pro-
spective trial of gastric bypass versus vertical banded gastroplastyfor morbid obesity and their effects on sweets versus non-sweetseaters. Ann Surg 1987;205:613–624.
3. Hall JC, Watts JM, O’Biren PE, et al. Gastric surgery for morbidobesity. The Adelaide study. Ann Surg 1990;211:419–427.
4. MacLean LD, Rhode BM, Sampalis J, Forse RA. Results of thesurgical treatment of obesity. Am J Surg 1993;165:155–160.
5. MacLean LD, Rhode BM, Forse RA. Late results of vertical bandedgastroplasty for morbid obesity. Surgery 1990;107:20–27.
6. Nightengale ML, Sarr MG, Kelly KA. Prospective evaluation ofvertical banded gastroplasty as the primary operation for morbidobesity. Mayo Clin Proc 1991;66:773–782.
7. van Gemert WG, van Wersch MM, Greve JW, Soeters PB. Re-visional surgery after failed vertical banded gastroplasty: restora-tion of vertical banded gastroplasty or conversion to gastric by-pass. Obes Surg 1998;8:21–28.
8. Behrns KE, Smith CD, Kelly KA, et al. Reoperative bariatricsurgery. Lessons learned to improve patient selection and results.Ann Surg 1993;218:646–653.
9. Cariani S, Nottola D, Grani S, et al. Complications after gastro-plasty and gastric bypass as a primary operation and as a reop-eration. Obes Surg 2001;11:487–490.
0. Jones KB. Revisional bariatric surgery–safe and effective. ObesSurg 2001;11:183–189.
1. Owens BM, Owens ML, Hill CW. Effect of revisional bariatricsurgery on weight loss and frequency of complications. ObesSurg 1996;6:479–484.
2. Vasallo C, Andreoli M, La Manna A, Turpini C. 60 reoperationson 890 patients after gastric restrictive surgery. Obes Surg 2001;11:752–756.
3. Sugerman HJ, Kellum JM Jr, DeMaria EJ, Reines HD. Conver-sion of failed or complicated vertical banded gastroplasty togastric bypass in morbid obesity. Am J Surg 1996;171:263–269.
4. Balsiger BM, Murr MM, Mai J, Sarr MG. Gastroesophagealreflux after intact vertical banded gastroplasty: correction byconversion to Roux-en-Y gastric bypass. J Gastrointest Surg2000;4:276–281.
5. Murr MM, Balsiger BM, Kennedy FP, et al. Malabsorptive pro-cedures for severe obesity: comparison of pancreatico-biliary by-pass and very very long Roux-en-Y gastric bypass. J GastrointestSurg 1999;3:607–612.
6. Brolin RE, Robertson LB, Kenler HA, Cody RP. Weight loss anddietary intake after vertical banded gastroplasty and Roux-en-Ygastric bypass. Ann Surg 1994;220:182–190.
7. Westling A, Öhrvall M, Gustavsson S. Roux-en-Y gastric bypassafter previously unsuccessful gastric restrictive surgery. J Gastro-intest Surg 2002;6:206–211.
8. Kaminski DL. Gastric restrictive procedures to treat obesity:reasons for failure and long-term evaluation of the results ofoperative revision. Int J Surg Investig 2001;2:413–421.
9. Gavert N, Szold A, Abu-Abeid S. Laparoscopic revisional sur-gery for life-threatening stenosis following vertical banded gas-troplasty, together with placement of an adjustable gastric band.Obes Surg 2003;13:399–403.
0. Morino F, Toppino M, Fronda G, et al. Weight loss and complica-tions after vertical banded gastroplasty. Obes Surg 1992;2:69–73.
1. Moreno P, Alastrué A, Rull M, et al. Band erosion in patientswho have undergone vertical banded gastroplasty. Incidence andtechnical solutions. Arch Surg 1998;133:189–193.
2. Subramanyam K, Robbins HT. Erosion of Marlex band andsilastic ring into the stomach after gastroplasty: endoscopic rec-ognition and management. Am J Gastroenterol 1989;84:1319–
1321.
2
2
2
2
374 Gonzalez et al Technique for Revisional Bariatric Surgery J Am Coll Surg
3. Khaitan L, van Sicke K, Gonzalez R, et al. Laparoscopic revisionof bariatric procedures: is it feasible? Am Surg 2005;71:6–12.
4. Fernandez AZ, DeMaria EJ, Tichansky DS, et al. Experiencewith over 3,000 open and laparoscopic bariatric procedures.Multivariate analysis of factors related to leak and resultant mor-tality. Surg Endosc 2004;18:193–197.
5. Livingston EH, Ko CY. Assessing the relative contribution of
individual risk factors on surgical outcome for gastric bypasssurgery: a baseline probability analysis. J Surg Res 2002;105:48–52.
6. Csepel J, Quinn T, Pomp A, Gagner M. Conversion to a lapa-roscopic biliopancreatic diversion with a duodenal switch forfailed laparoscopic adjustable silicone gastric banding. J Lapa-
roendosc Adv Surg Tech 2002;12:237–241.