operative dentisitry

of 12
Transcript of operative dentisitry
-
8/18/2019 operative dentisitry
1/12
ABSTRACT
This article describes the properties, advances and shortcomings of glass-ionomer cementas a restorative material. The adhesion of glass-ionomer to tooth structure is less techniquesensitive than composite resins and its quality increases with time. Therefore glass-ionomer
might turn out to the more reliable restorative material in minimal invasive dentistry basedon adhesive techniques.
Uniterms: Glass ionomer cements adhesion; Minimum intervention; Sealant restorations.
RESUMO
ste artigo descreve as propriedades, avan!os tecnol"gicos e limita!#es dos cimentos deion$mero de vidro como material restaurador. % ades&o dos cimentos ionom'ricos (estrutura dental ' menos sens)vel (s varia!#es t'cnicas do que o mecanismo de ades&o das
resinas compostas e a qualidade do cimento se aprimora com o uso cl)nico. *ortanto ocimento de ion$mero de vidro torna-se o material restaurador mais confi+vel emprocedimentos restauradores minimamente invasivos baseados em t'cnicas adesivas.
Unitermos: imentos de ion$mero de vidro, ades&o; Minima interven!&o; Selantes.
INTRODUCTION
There is a continuous urge for novelties in dentistry originating from changing professionalperceptions, changing demands from the patient and progress in industrial possibilities. Thealtering professional perceptions come along with raising consciousness that cariestreatment is not merely technique, but requires a bio-medical approach, that less-invasivetechniques are possible, that bio-compatibility requires increased interest, that there arechallenging new possibilities and that there eist new marets/.
The patient has changed as they demand more esthetics, established bio-compatibility andlower costs. 0n top of that industry contributed substantially in progressive possibilities,
such as computeri1ed systems, %23%M, optical reading and cutting, chemical reading andcutting, physico-chemical bonding and new materials.
Today4s dentistry can be characteri1ed by a move away from metal towards non-metalrestorations. Motivation is mainly based on concern for esthetics and biocompatibility.5ndirect restorative dentistry this means a shift from amalgam to composites. 6or directrestorations, three essentially different materials are at our disposal7 amalgam, resin-basedcomposites and glass-ionomers. 0f all direct dental restorations in the 8etherlands9:, in9
-
8/18/2019 operative dentisitry
2/12
was /:= and in ?::? this number was >:=@ Aestoring in tooth colored materials isnowadays the first option in the teaching programs at the dental schools in the 8etherlands.
Amalgam
%malgam ecellently served dentistry for almost ?:: years@ Bhy changing a winning horseC
The reluctance for amalgam originates from its composition and structure. Dasicallyamalgam is a mercury alloy and in our case a silver-mercury alloy. The reaction of onlysilver powder with mercury into a solid silver-mercury component proceeds too slow forrestorative application, which necessitated additional more reactive metals. 0ften we sawand see that attempts to improve turns out to compromise other characteristics. 5n case ofdental amalgam the increase in setting time was at the cost of strength and corrosionresistance. The chemical reaction of dental silver amalgam can roughly be described by7
The Gree letter γ EgammaF denotes the crystallographic identification of the variouscomponents. The stannous-mercury component SnHg or γ ? forms the wea lin in the set
composite structure. %s can be seen from Table 9 the γ ?-phase is substantially weaer than
the other ones, but what is worse, its corrosion potential is far negative. Bhen two metalswith unequal corrosion potential are in electrical contact within an electrolyte Ewater orsalivaF, the less noble metal will dissolve by releasing ions. 5t is very liely that the reactivemercury ions immediately will react with the remaining γ component in the restoration,
whilst the harmless tin ions will disappear. Iet, the result of this corrosion is that thesurface, and later the bul of the restoration becomes porous, which does not contribute tothe esthetics and strength of the restoration. The γ ?-phase is the %chilles heel of dental
amalgam and suppression of this component could be achieved by adding small quantitiesof copper to the alloy. The copper-containing, so-called non-γ ? amalgams indeed showed
less corrosion. %ddition of copper to silver amalgam suppresses the formation of the γ ? Jphase SnHg, which improves the alloy considerably9?. Bhether the use of amalgam indentistry should be limited or avoided for biological reasons is still open for discussion. 5nthe 8etherlands, the official standpoint is that there is no scientific evidence that amalgamis a serious ha1ard for the patient, whilst the dental team can be at ris of mercurypoisoning, if no adequate hygienic measures are taen99.
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#tab1http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#tab1
-
8/18/2019 operative dentisitry
3/12
%part from the above arguments, amalgam holds another serious problem. Decause of itsbrittleness the restoration should be as buly as possible, and by absence of adhesion,cavity preparation is based on macro-mechanical retention. Doth measures imply thatplacement of amalgam is usually associated with sacrifice of sound tooth structure. Today,the opinion holds that, if prevention has failed, the dentist should only minimally sacrificesound tooth structure when restoring the tooth. Bithin this concept, adhesion is essential.There are at the present two classes of materials which allow direct restorations withadhesive techniques. These are resin-based composites and glass-ionomer cements.
Composites
5t goes beyond the scope of this paper to cover structure and properties of resin-basedcomposites, but some essentials will be discussed. 5n mechanical sense, the stronger resin-based composites can compete with dental amalgam ETable ?F.
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#tab2http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#tab2
-
8/18/2019 operative dentisitry
4/12
5n contrast to the superior esthetics of resin-based composites stands their great handicap,which is that their hardening is associated with polymeri1ation shrinage. 5t taes mostconscientious understanding and technical sill to avoid leaage notwithstandingsophisticated bonding systems. 5t has to be appreciated that leaage is the most common
reason for secondary caries and replacement of the restoration. 2ue to failing adhesion andpremature fracturing and wear, the lifetime of a resin-based composite restoration is limited.The longevity of a restoration depends not only on the material, but also on the cavity si1eand location as well as on the dentist and the patient.
The longevity of a posterior amalgam restoration runs up to 9:-9K years, whilst resin-basedcomposites have to be replaced after K-> years9. This means that the longevity of acomposite restoration is only half that of an amalgam restoration. 5n addition it taesapproimately ?- K times more time to mae a composite than an amalgam restoration.onsequently resin-based composite restorations are epensive and cost much chair time.%n amalgam restoration is usually better and a composite restoration is often worse than itloos. %s a matter of fact, it taes a good dentist to mae a good composite and a bad one
to mae a bad amalgam. 5f a plenty silled dentists are available, resin-based compositesmay contribute to very satisfying dentistry, but problems arise if there eists a shortage.
Table
-
8/18/2019 operative dentisitry
5/12
There eists consensus on the fact that the Lthree step bondingL ends up to the best results.5n practice these three steps consist of many more. 6or proper application of the bestestablished bonding systems one consecutively has perform the following steps7 etching,rinsing, drying, miing of primer, priming agitation, air blowing of primer, additional priming,application of adhesive, impregnation of adhesive, spreading of adhesive, light curing andadditional curing. These total > J 9? steps taes at least ? - < minutes chair time. *roper
bonding requires deep nowledge and great sill; more than before, the quality of therestoration is determined by the dentist factor. The latest bonding generations became moreoperator friendly, but their clinical durability is reduced. 0n top of this premature in situdegradation of bonding and composite limit the lifetime of these inds of restorations?9.
The conclusion so far might be that resin-based composites are highly aesthetic alternativesfor amalgam that can be used with minimal invasive treatment, but that particularly thebonding procedure is too demanding for wide-scale dentistry.
-
8/18/2019 operative dentisitry
6/12
Glass-ionomers
6ully in contrast with resin-based composites is application and bond formation with glass-ionomers. 5t is true, the bond strength reaches only ?/= of that can be obtained with resinbonding systems9
-
8/18/2019 operative dentisitry
7/12
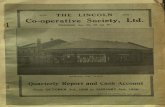
8ote that the vertical ais in 6igure ?b is twice as high as that of 6igure ?a, which implies
that wear of the resin-modified types wear considerably faster than the conventional ones.5n 6igure
-
8/18/2019 operative dentisitry
8/12
6or direct restorative dentistry, the slow setting of conventional glass-ionomers is felt as aninconvenience. %part from the irritant of waiting for finishing the restoration, a drawbac ofthe slow setting is that the water content of the freshly placed cement can easily be altered
-
8/18/2019 operative dentisitry
9/12
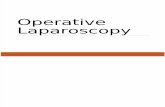
either by dehydration or water uptae from the saliva. 5f the immature restoration is notprotected by a varnish, the surface might be damaged as is shown in 6ig.Ka where evenafter some days the surface of normally set and unprotected glass-ionomer is dyeinfiltrated.
The loosely bound water may have a negative effect on initial solidity of glass-ionomer, butis at the same time responsible for positive characteristics such as curing shrinage relieveand continuing chemistry throughout the bul material, which reinforces the material andfacilitates fluoride release.
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#fig4ahttp://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#fig4a
-
8/18/2019 operative dentisitry
10/12
%, yet not fully established technique, by which the cements hardening is substantiallyaccelerated with ultrasonic or heat treatment may solve many problems related to the slowsetting of glass-ionomers. 6igure Kb shows that accelerated hardening prevents the glass-ionomer for dye penetration. Mechanical properties are also significantly enhanced by heator ultra-sound treatment. 6or this reason no specific values for glass-ionomer are given inTable ?.
Sealants
Thans to their applicability under humid conditions and direct bonding to tooth enamel, theinorganic glass-ionomers are practicable alternatives for resin fissure sealings. To someetend, the affirmed low wear resistance, which causes the sealant already to erode aftersome months9K,9, may substantially be reduced by using heavy filled restorative glass-ionomer materials in stead of the thin fissure sealant glass-ionomer varieties. %lthough theglass-ionomer sealant visually disappears soon after placement, its preventive effect wasreported still effective after / years. SM images, obtained by replica techniques from thefissures showed clinically imperceptible, retained material E6igure /F. The presence of thismaterial may be responsible for the prolonged prevention efficacy9,
.Shimoobe?: suggested that under oral conditions, glass-ionomer sealants might graduallychange into a new, more durable structure with high retention. He epected that with helpof the mineralising potential of saliva, glass-ionomers might transform into an enamel-liestructure called Lpseudo enamelL. 5n addition to the satisfaction with glass-ionomer as aneffective way of preventing fissure caries, van 2uinen et al> observed clinically visiblechanges in the glass-ionomer as shown in 6igure / and . These changes referred totranslucency, smoothness and hardness. 5n analogy to the Ere-F mineralising power on toothstructures9, the potential of saliva as a reinforcing agent for restorative materials wassuggested.
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#fig4bhttp://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#tab2http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#fig5http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#fig5http://www.scielo.br/img/revistas/jaos/v14nspe/30830f6.jpghttp://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#fig4bhttp://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#tab2http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#fig5http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1678-77572006000700002#fig5http://www.scielo.br/img/revistas/jaos/v14nspe/30830f6.jpg
-
8/18/2019 operative dentisitry
11/12
The ideal pit and fissure sealant should be a full proof obstruction for the damaging effectsof dental plaque at sites of the tooth that hardly can be cleaned with domestic measures. %tight-adhering, erosion-resistant, impermeable layer covering the tooth fulfills that goal. 5fthe retention and its erosion resistance are guaranteed for a substantial number of years,
there is nothing against the use of the, basically inactive, resin-based materials for thispurpose. However, application of resins requires etensive tooth surface conditioning, whilstthe hydrophobic material is essentially unwelcome in the humid oral environment. 5ncontrast to this, the hydrophilic glass-ionomer requires only minor substrate conditioningand shows a tight adhesion to enamel but unfortunately will erode easily.
MeOare and MOPr9K reported that teeth sealed with resins more frequently develop cariesthan teeth sealed with glass-ionomer. This, in spite of the fact that the bul glass-ionomersealant had visually vanished within a few months, while the maOority of the resin sealantsshowed retention for / years and more. Their findings can be eplained by either anunperceived sealant residuum or a longtime Eafter-F effect of the fluoride release from themeanwhile eroded glass-ionomer. MeOare and MOPr9K eplained their observations by SM-
imaging, which revealed still retained Lglass-ionomerL in the depth of the fissure at sites,where clinically no remnants of the cement were detectable. These remnants may be thesame as the LintermediateL layer as postulated by Bilson et al.? demonstrated that glass-ionomer adOacent to tooth structure and incontact with the oral fluids, frequently altered into a material with unepected cuttingresistance and displaying raised alcium- and *hosphate content. 5t was remarable thatsuch an altered layer was only detectable after a couple of years4 performance, whilst itsthicness increased with time. This indicates that, with time, the echange process
continues and consequently the glass-ionomer restoration gains in quality, starting from theouter surface and the Ounction with tooth structure. 5t appears that, glass-ionomer performsclinically better than from laboratory research may be epected,9>. %s saliva and itsminerals play a crucial role in minerali1ation processes?, it can be understood that onlyunder in vivo circumstances the glass-ionomer surface changed into the new structure.
0ada et al9 showed that glass-ionomer stored in saliva has an improved surface hardnesscompared to samples stored into water. %lso in deeper areas echange processes has beenreported??. Geiger and Beiner demonstrated between dentin and glass-ionomer anintermediate echange layer containing fluoridated carbonate-apatite.
CONCLUSIONS
5n contrast to resin bonding, the adhesion of glass-ionomer to tooth structure is nottechnique sensitive and its quality increases with time. Therefore glass-ionomer might turnout to the more reliable restorative material in minimal invasive dentistry based on adhesivetechniques.
-
8/18/2019 operative dentisitry
12/12
Glass-ionomer is not only bioactive, but has even features of an intelligent material. Glass-ionomer can be called active as it releases fluoride, it can be called intelligent, because itreleases fluoride proportionally to the acidity. To some etend it has a pH buffer capacity.
% persisting concern of conventional glass-ionomers is their brittleness and low wearresistance. The latter is even pH-dependent which means that proper oral hygiene is vital.
9. 6or socio-economical reasons, direct restorative techniques are preferred over indirectones.
?. 5nterest in amalgam is fading.
. Glass-ionomers holds a great potential to become the first choice direct restorativematerial.