
Operating Room and Burn Unit
91
INFECTION CONTROL IN THE OPERATING AND DELIVERY ROOMS Ma. Laarni D. Canceran, R.N. Department Manager, St. Luke’s Medical Center- Global City
-
Upload
philippine-hospital-infection-contol-nurses-associaton-phicna-inc -
Category
Healthcare
-
view
1.705 -
download
0
Transcript of Operating Room and Burn Unit
INFECTION
CONTROL IN THE
OPERATING AND
DELIVERY ROOMSMa. Laarni D. Canceran, R.N.
Department Manager, St. Luke’s Medical Center- Global City

Basic Principles
Operating Room
Characteristic features:
• Patients are at risk due to exposed wound
• Natural body defenses are depressed
• Most patients are compromised
• Our goal is to decrease Surgical Site Infection
(SSI)
Operating Room
• Room needs to be as
clean as possible
• Houses special
equipments that can
be source of infection
• Set up should take
infection control
principles into account

Operating Room Environment
Operating Room Divisions
Design and Traffic Pattern – 3 zone concept Unrestricted Area which includes the patient reception
area, locker rooms, lounges and offices.
Semi-restricted Areas which include the storage areas for clean and sterile supplies, work areas for storage and processing of instruments and corridors to restricted areas of the suite. Traffic is limited to authorized personnel and patients. Personnel are required to wear gown and hair covering.
Restricted Area includes all areas where personnel are required to wear surgical masks and scrub attire at all times. It includes operating suites, clean core and scrub areas.
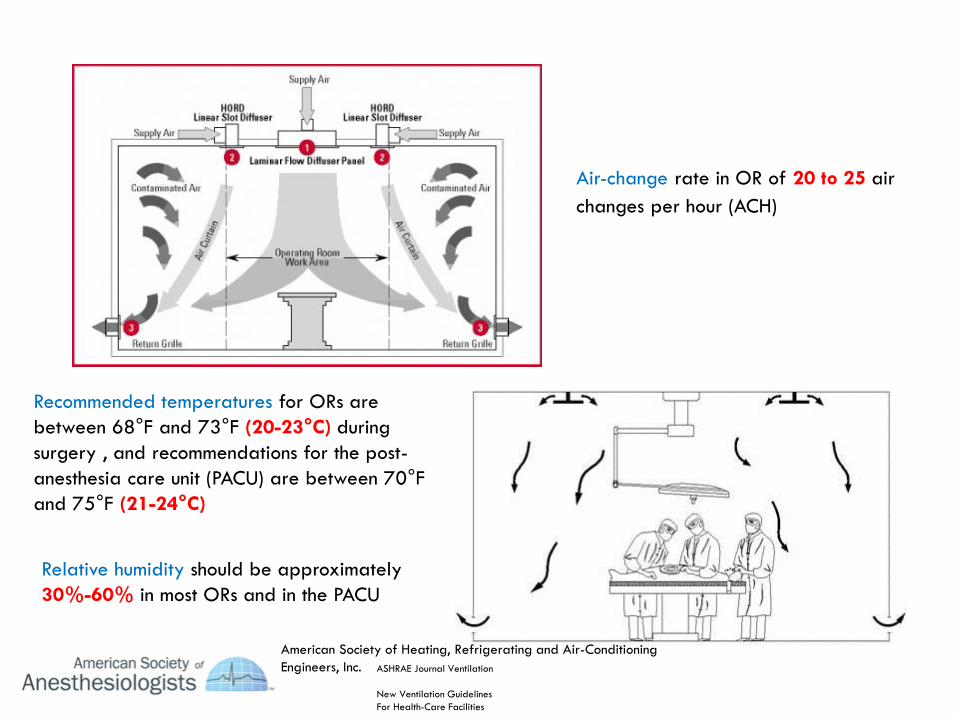
Relative humidity should be approximately
30%-60% in most ORs and in the PACU
Air-change rate in OR of 20 to 25 air
changes per hour (ACH)
Recommended temperatures for ORs are
between 68°F and 73°F (20-23°C) during
surgery , and recommendations for the post-
anesthesia care unit (PACU) are between 70°F
and 75°F (21-24°C)
American Society of Heating, Refrigerating and Air-Conditioning
Engineers, Inc. ASHRAE Journal Ventilation
New Ventilation Guidelines
For Health-Care Facilities
The IC Team should be notified
whenever the air delivery system
for the OT has been shut down
for maintenance or malfunction.
The IC team in conjunction with
facility engineers will assist with
determination of need for any
environmental monitoring needed
once the ventilation system is re-
established. At a minimum
positive pressure, inspection of
filters and air changes per hour
should be verified prior to use of
the affected OT after
interruption. The theatre should
be used only after clearance
from the IC team.

Handling of Infectious Patients
A room may be designated for "precaution cases"(infectious/communicable)” of an infectious patient.
If possible the room at the farthest corner of the area shall be assigned for the case, OR it will be scheduled last for
the day, provided it is not a stat case.

Environmental Cleaning

• The inanimate theatre environment should, under normal circumstances, have
a negligible contribution to the incidence of SSI.
• Floors and walls will never be sterile nor is there any point in trying to
achieve that level of cleaning. Floors are rapidly re-contaminated after
cleaning and disinfection and that they should be cleaned at the end of
each session/case. Disinfectant may not be required, except when cleaning
body fluid spillage.
Walls and ceilings are rarely heavily contaminated, cleaning them once a month is reasonable.
Correct site decontamination of blood and other potentially infectious materials should be in compliance with the standards.
Brooms of whatever materials and vacuum cleaners are not to be used; wet mops shall be used instead.

http://www.ems.org.eg/esic_home/data/giued_part2/Operating%20Theatre.pdf

http://www.ems.org.eg/esic_home/data/giued_part2/Operating%20Theatre.pdf
Environmental Microbiologic sampling
Routine microbiologic sampling of the OT air or surfaces is not recommended
because the results obtained are only valid for the time period and for the
location sampled. Instead, such studies should be limited to recommendations
from the IC-Team, investigations of clusters or outbreaks of infection, or to
validate changes in the ventilation system (e.g. installation of new AHU).
http://www.ems.org.eg/esic_home/data/giued_part2/Operating%20Theatre.pdf
Environmental Decontamination
• Aerosolized Hydrogen Peroxide is a new
method of surface area decontamination that is recommended recently by Infection Control experts as an adjunct to our usual manual cleaning. This method eliminates the deficiencies and inconsistencies inherent in manual cleaning contributed by the human factor.
• UV light no-touch environmental disinfection using ultra violet technology

Staff
MOBILITY
The number of persons present during an operation must be as small as possible
Walking in and out during an operation must be kept to a minimum. People are the most important source of microorganisms in the OR. It is also certain that the number of microorganisms in the air increases as the numberof people and movements in OR increase. Walking in and out disturbs the flow of air, causing unwanted temperature fluctuations.

OR ATTIRE
• hair covering
• mask
• foot wear
• gloves
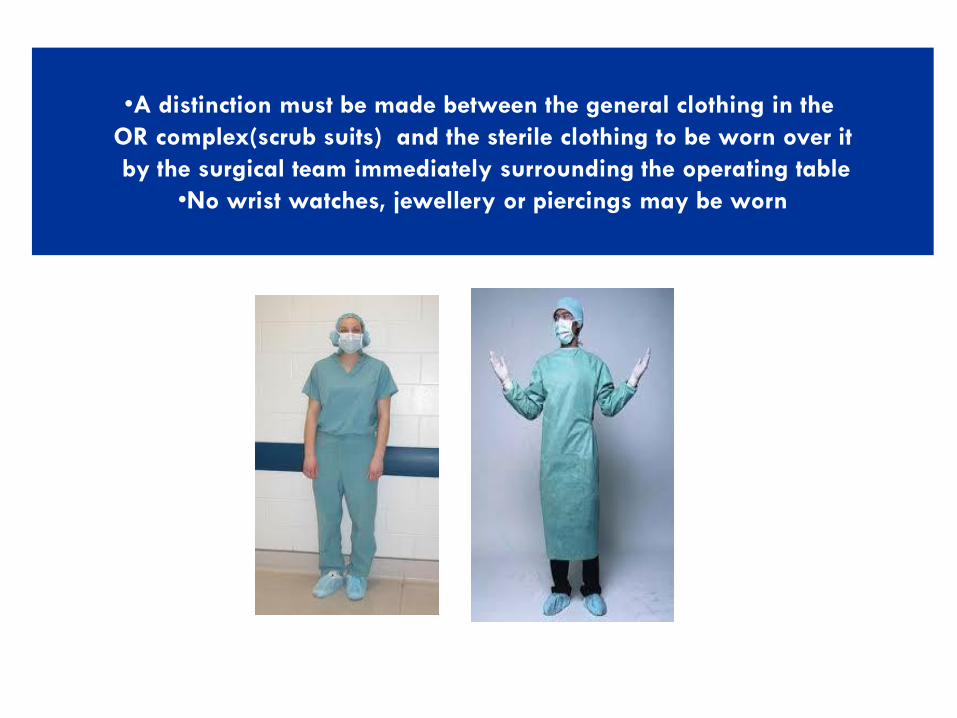
•A distinction must be made between the general clothing in the
OR complex(scrub suits) and the sterile clothing to be worn over it
by the surgical team immediately surrounding the operating table
•No wrist watches, jewellery or piercings may be worn
•In the OR complex, operating room clothing is worn. This clothing is not worn outside
the OR.
•In order to maintain the zone system in practice, it is important that everyone complies
with it.
•When someone has to leave the OR complex for a short time, for instance for brief
administrative activities, a white coat or other item of protective clothing be worn over
the scrub suit. This does not apply when examination or treatment of a patient must
take place in the ward.
•Between operations, clothing is changed when it becomes dirty or wet
•Clean operating room clothing must be put on each day
Double Gloving
• The transmission of HBV and HCV from surgeon to patient and vice versa has occurred in the absence of breaks in techniqueand with apparently intact gloves (Davis 2001). Even the best quality, new latex rubber surgical gloves may leak up to 4% of the time.
• Single gloves had a blood-hand contact rate of 14% while surgeons wearing double gloves had only a rate of 5% (Tokarset al 1995; Tokars et al 1992)
Guidelines for Double Gloving
• The procedure involves coming in contact with large amounts of blood or other body fluids (e.g., vaginal deliveries and cesarean sections).
• Orthopedic procedures in which sharp bone fragments, wire sutures and other sharps are likely to be encountered.
• Surgical gloves are reused. (The possibility of inapparent holes or perforations in any type of reprocessed glove is higher than with new gloves.)

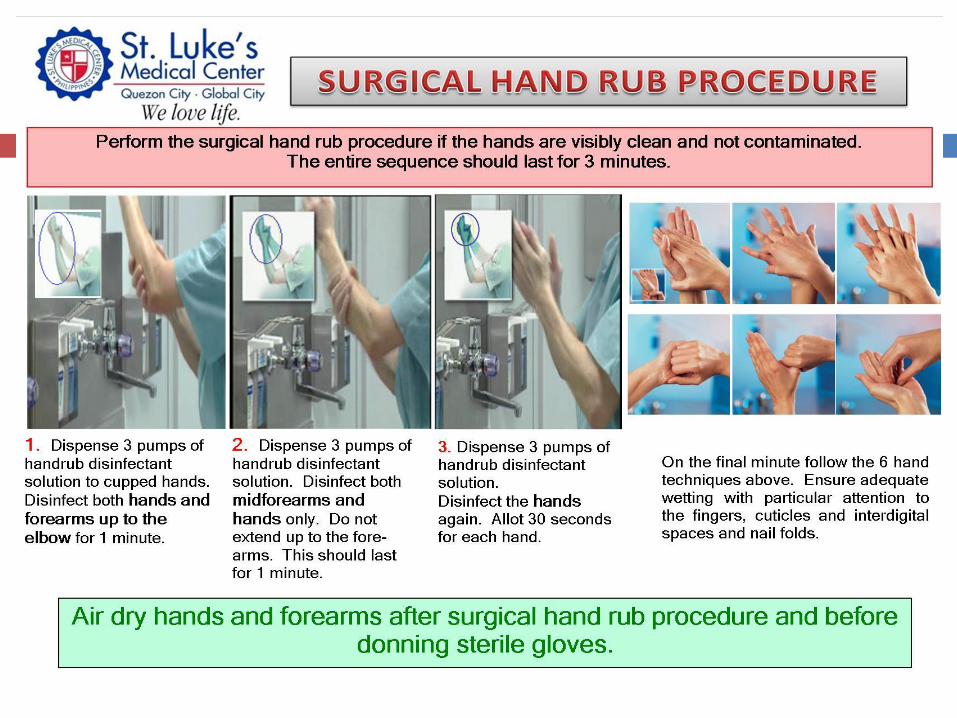
Surgical handwash or surgical handrub must be
performed preoperatively by surgical personnel
to eliminate transient and reduce resident hand
flora.
Pre-operative Hand Hygiene

Brushless Surgical Hand Scrub

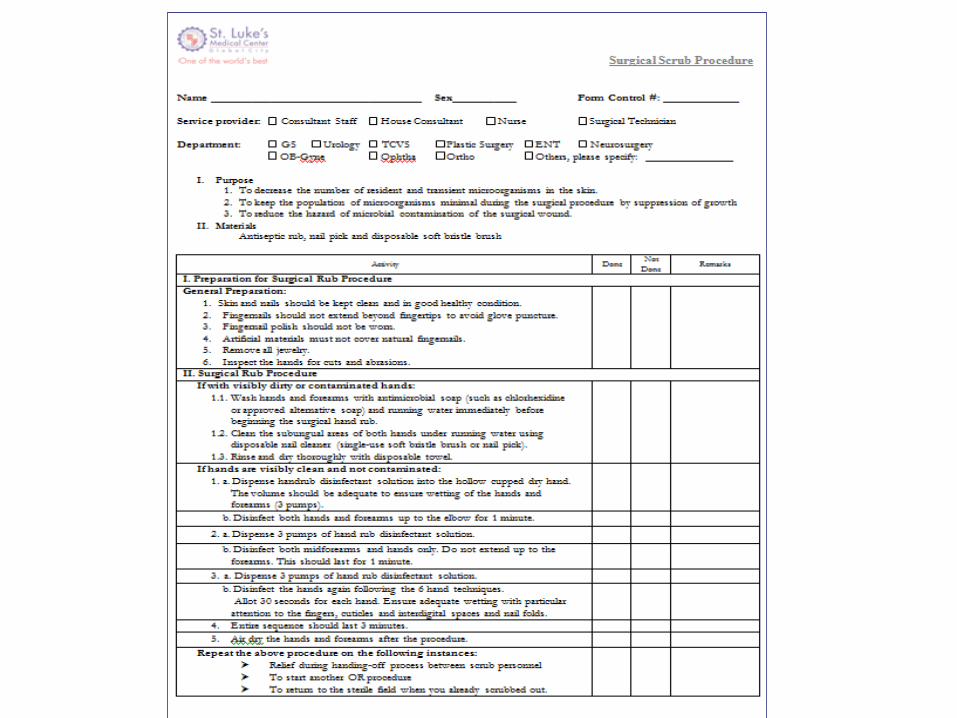
Name ___________________________ Sex_______ Form Control #: _____________Service provider : Consultant/ Surgeon Resident Nurse Intern Surgical Technician
Department : GS Ortho ENT Uro Others, please specify: ____________________•Purpose
•To decrease the number of resident and transient microorganisms in the skin.•To keep the population of microorganisms minimal during the surgical procedure by suppression of growth•To reduce the hazard of microbial contamination of the surgical wound •Materials
Antiseptic rub, face mask, cap, eye goggles and nail pick
Surgical Scrub Procedure
Activity Done Not Done Remarks
I. Preparation for Surgical Rub Procedure
General Preparation:
•Skin and nails should be kept clean and in good healthy condition.
•Fingernails should not extend beyond fingertips to avoid glove puncture.
•Fingernail polish should not be worn.
•Artificial materials must not cover natural fingernails.
•Remove all jewelry.
II. Preparation Immediately before Surgical Rub
• Inspect the hands for cuts and abrasions.
• Be sure all hair is covered by headgear/bouffant cap.
• Adjust disposable mask snugly and comfortably over nose and mouth.
• Wear eye goggles if needed.
III. Surgical Rub Procedure
1Wash hands and forearms with antimicrobial soap (such as chlorhexidine or approved alternative soap) and running water
immediately before beginning the surgical hand scrub.
2 Clean the subungual areas of both hands under running water using disposable nail cleaner
3aApply 2-3 ml (6 drops) of antiseptic soap from the dispenser to the hands. (or follow manufacturer’s recommendation)
3b
Wash the hands and forearms for 3 – 6 minutes including at least 30 strokes each hand. Pay particular attention to the fingers,
cuticles and interdigital spaces and working the antimicrobial soap to four sides of the forearm. Avoid splashing your surgical attire.
4
Rinse thoroughly hands and forearms under running water, holding hands higher than elbows and away from surgical attire,
allowing water to drip from flexed elbows.
5Dry hands and arms with sterile linen before donning sterile gloves and gown. (Double glove if with cuts or abrasions.)
6
Repeat the above procedure on the following instances:
Relief during handing-off process between scrub personnel.
To start another OR procedure.
To return to the sterile field when you already scrubbed out.
Waterless Surgical Hand Scrub
Visitors

• Visitors to the operating room include visiting doctors from other wards, parents of young children while thay are brought to the OR, partners who attend Cesarean, and technicians
• The number of persons present during an operation must be kept to a minimum. Everyone must be aware of the risks of infections and must maintain the necessary discipline.
• The number of movements must be kept to a minimum.
• Visitors who are present during the operation must wear the standard surgical clothing. For a brief visit (less than or equal to 15mins) overalls with cuffs around the arms and ankles will suffice. In addition, disposable masks and hair covers are worn.
For longer visits (more than 15mins) visitors must follow the clothes changing procedure for the staff

Patients
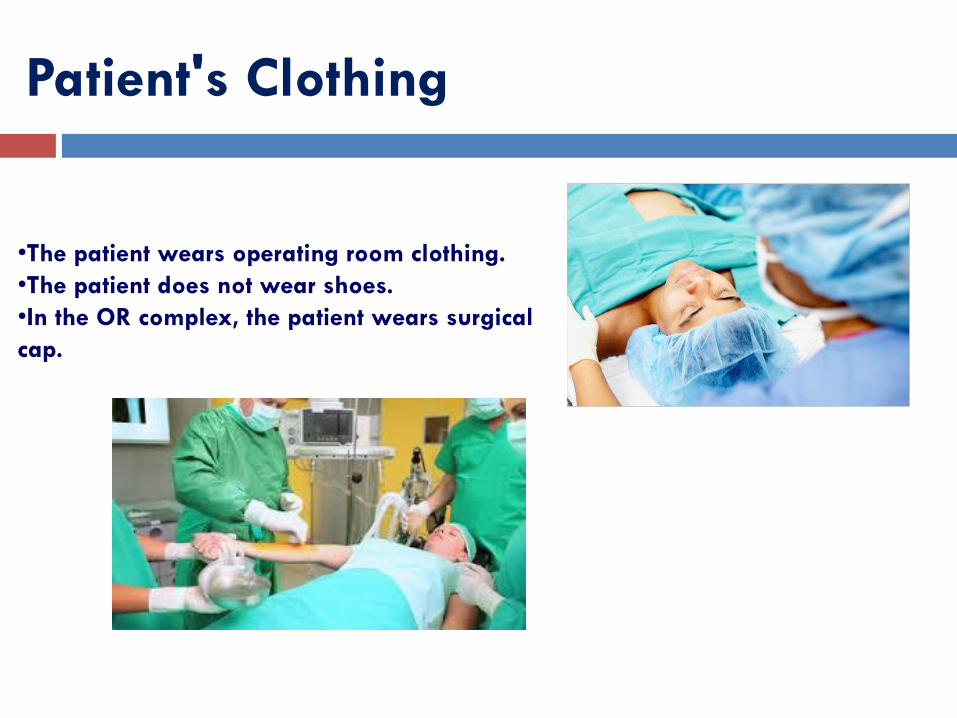
Patient's Clothing
•The patient wears operating room clothing.
•The patient does not wear shoes.
•In the OR complex, the patient wears surgical
cap.
Transport to and across the transfer area
Transport of the patient to operating room can take place in three ways:
1. On the day of the operation, either in the ward or at the boundary of
the operating area, the patient is lifted onto a clean bed with clean
bedding, which is wheeled next to the operating table. After the
operation, this bed is used again to transport the patient to the recovery
room or the nursing ward.
2. The patient is wheeled to the boundary of the operating room area in
his/her own bed. There, the patient is lifted onto an operating surface on
wheels or a mobilift, after which it is wheeled into the operating room.
After the operation the patient is lifted from this system onto a bed with
clean bedding in the recovery room

Transport to and across the transfer area
3. If it is not possible to lift the patient onto a clean bed or an
operating surface on wheels outside the operating room(for
example if the patient is in a traction bed), an exception can
be made and the patient can be wheeled to the operating
table on his/her own "dirty" bed from the nursing ward. In
that case, the bed must be made up with clean bedding in the
nursing ward and domestically cleaned insofar as possible.
•The risk of infection is the same in every part of the transfer
area. No link has been demonstrated between one of the
above-mentioned systems of transport and the chance of
infection. The choice between these three methods can be
based on practical and economic considerations.
•The bed a patient was lying in his/her ward may only be
wheeled to the operating table in exceptional cases.

SSI Prevention
Bundles of Care in SSI
Pre-Operative Showers
• 4% Chlorhexidine
solution used,
preferred night before
and morning of
surgery
• Cochrane review,
showed no clear
evidence or advantage
• Pre-operative shower
reduces SSIs
Re-use of Single use Items
• Big issue
• Little available evidence of harm from reuse, FDA says oversight is warranted
• Problems involved- thousands of equipment and supplies, re-processing differs, need for authority, issue of efficacy
• Single-use equipment
Reuse of disposable/ single-use equipment is not recommended. Chemical disinfection and sterilization processes may damage or weaken the integrity of single-use items and make them unsafe for use.
Centralized Sterilization Area
• Training

INFECTION CONTROL IN THE
BURN UNITMa. Laarni D. Canceran, R.N.
Department Manager, St. Luke’s Medical Center- Global City
Burn Wound Patient
• Among patients at highest risk for hospital-
acquired infections
• Have lost a portion of their integument that
would ordinarily be a strong barrier to
invasion of microorganisms
• Necrotic tissue in the burn eschar– combined
with the presence of serum CHON, provides
a rich culture for MOs

Infections
• Most common cause of death in burn patients
• Most common site of infection are the burn wound
and lungs
• May also initiate a septic response accompanied
by multi-organ failure
Types of Burns
• Majority of Burns– caused by thermal injury
• Adults– flame burns
• Children– scalding and flames
• Others– chemical, electrical, fire cracker injuries




Epidemiology of Burn Wounds
The development of infection depends on the
presence of three conditions:
• Source of organisms-
• A. Burn wound of patient
• B. Environment
• C. Endogenous flora
• Mode of transmission
• Susceptibility of the patient.

Sites of Environmental Contamination in
Burn Care Facilities
Site Microorganism
Hydrotherapy equipment P. Aeruginosa, E. Cloacae
Sink faucets P. Aeruginosa
Faucet handles P. Aeruginosa
Bars of soap P. Aeruginosa
Towel racks P. Aeruginosa
Sink basins P. Aeruginosa
Transportation equipment P. Aeruginosa
Water supply P. Aeruginosa
Sink drains P. Aeruginosa
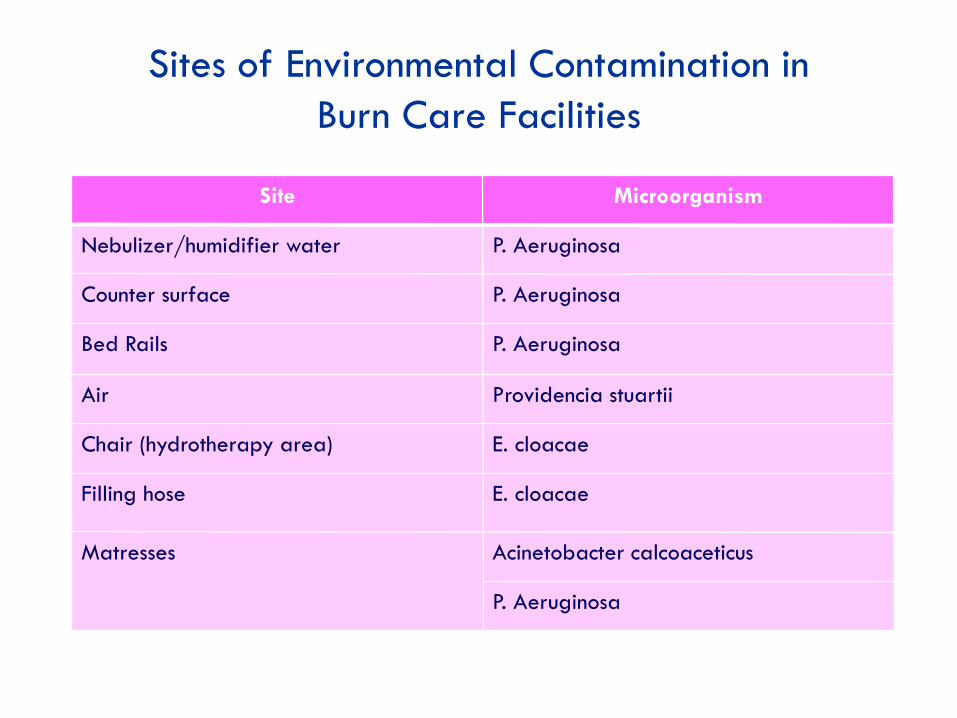
Sites of Environmental Contamination in
Burn Care Facilities
Site Microorganism
Nebulizer/humidifier water P. Aeruginosa
Counter surface P. Aeruginosa
Bed Rails P. Aeruginosa
Air Providencia stuartii
Chair (hydrotherapy area) E. cloacae
Filling hose E. cloacae
Matresses Acinetobacter calcoaceticus
P. Aeruginosa
Mode of Transmission
• Contact-- either via the hands of the
personnel caring for the patient or from
contact with inappropriately decontaminated
equipment.
• Droplet spread.
• Airborne spread.
In general, the larger the burn injury, the greater the
volume of organisms that will be dispersed into the
environment from the patient.
Patient Susceptibility
What Lowers Physical Defenses:
• Invasive devices, such as endotracheal tubes,
• Intravascular catheters and urinary catheters,
Bypass the body’s normal defense mechanisms..

Mode of Transmission Risk Factors
• Duration of hospitalization
• Burn wound size
• Transfusions
• Resistance of microorganisms to topical
antibiotic agents
• Resistance of microorganism to systemically
administered antimicrobial agents
Characteristics of Burn Wound Infection
• Focal gangrene that spreads throughout the wound
• Conversion of a partial-thickness wound to a full-thickness wound
• Hemorrhagic discoloration of sub-eschar tissue
• Focal, multi-focal or generalized dark brown, black or violaceous discoloration
• Changes in the unburned skin at the wound margins char. by edema and violaceousdiscoloration

Burn Wound Infection

Definitions for Burn Wound Infections
Burn infections must meet the following criteria:
Criterion 1: Patient has a change in burn wound
appearance or character, such as dark brown,
black or violaceous discoloration of the eschar,
or edema at wound margin
And Histologic examination of burn biopsy
shows invasion of organisms into adjacent
viable tissue

Definitions for Burn Wound Infections
Burn infections must meet the following criteria:
Criterion 2: Patient has a change in burn wound
appearance or character, such as dark brown,
black or violaceous discoloration of the eschar,
or edema at wound margin
And At least one of the following:
a. Organisms cultured from blood in the absence of other
identifiable infection
b. Isolation of herpes simplex virus in biopsies
Definitions for Burn Wound Infections
Burn infections must meet the following criteria:
Criterion 3: Patient w/ a burn has at least two of the following signs or symptoms with no other recognized cause: fever (>38˚C) or hypothermia (<36 ˚C), hypotension, oliguria (<2oml/hr), hyperglycemia at previously tolerated level of dietary carbohydrate, or mental confusion
And at least one of the following:a. Histo exam of burn biopsy shows invasion of organisms
into adjacent viable tissues
b. Organisms cultured from blood
c. Isolation of herpes simplex virus in biopsies

REMINDERS:
• Purulence alone at the burn wound site is not adequate for the diagnosis of burn infection; such purulence may reflect incomplete wound care.
• Fever alone in a burn patient is not adequate for the diagnosis of a burn infection because fever may be the result of tissue trauma or the patient may have an infection at another site.
Prevention and Control
There is evidence that improvements in the
prevention and control of infections in burn
patients has led to improvements in patient
survival
BURN WOUND INFECTION CONTROL
MEASURES
Goals:
• Control the transfer of endogenous organisms to
the burn sites
• Prevent the transfer of exogenous organisms from
other persons to patients
GENERAL MEASURES
Ward setting
• Burn cases should be accommodated in Burns Unit
• Burns Unit must be physically separated from other areas
• Single rooms should be provided for isolation
Ventilation
• Filtered air at positive pressure into individual rooms,
extracted in the corridor outside each room
• Air from ventilated rooms should be extracted to the
exterior
• No direct airflow between Burns Unit and other areas


GENERAL MEASURES
Environmental hygiene
• Daily mopping of furniture, bedside lamps, door
handles or knobs
• No sharing of wash bowls, or furniture (e.g., beds
and chairs)
• Restrict stuffed toys and items which cannot be
effectively decontaminated
• Minimize linen agitation
GENERAL MEASURES
Visitors and Traffic Control
• Orient all visitors to burn unit infection control
practices ( i.e. Hand washing, gowning and
isolation precautions)
• Limit amount of visitors present at any one time
• Screen visitors for infection and restrict if present
• Monitor visitors for compliance with infection
control practices

GENERAL MEASURES
Hand Washing
• Hand washing should be done before and after
each patient contact with antiseptic .Hand washing
sinks should be conveniently accessed
• Antiseptic hand rub is an alternative for hands
without visible dirt
Prevention and Control
Use of Barrier Techniques
- Used to prevent contact transmission ofmicroorganisms from patient to patient viacontaminated hands and clothing of HCW who providedirect care
• Use of gloves and gown made of impermeablematerial
• Washing of hands before donning of gloves and afterremoval of gloves– need not be sterile for routine non-invasive patient care
• If sink is not directly accessible, alcohol should alwaysbe at bedside (this is a necessity)
On Gowns and Aprons...
• Protective gown or apron is worn to prevent soiling
and in-apparent contamination of personal
uniform
• Should be replaced in-between patients

On gloving...
• Gloves should be worn when contact withblood, body fluids, secretions and excretions
• Gloves(sterile) should be worn for burnwound dressing
• Gloves should be changed whencontaminated with secretions or excretionsfrom one site prior to contact with another site,even if care of the patient is not completed
• Hand washing after removing gloves
Prevention and Control
Prevention of Cross-Contamination From Inanimate Surfaces and Food
• Each patient should be assigned his or her ownstethoscope, blood pressure cuff, box of cleandisposable gloves and container(s) of topicalantimicrobial agent
• Items of equipment that must be shared betweenpatients should be thoroughly cleaned and disinfectedbetween patients
• Covers on mattresses should be inspected betweenpatients and mattresses with damaged covers shouldnot be used

Prevention and Control
Prevention of Cross-Contamination From
Inanimate Surfaces and Food
• Raw vegetables have been shown to be a
source of P. Aeruginosa microorganisms that
cause burn wound infections. Patients, as
much as possible should not be fed raw fruits
and vegetables
Prevention and Control
Prevention of Cross-Contamination From Convalescent Patients
• Convalescent burn patients may be a reservoir ofmicroorganisms for cross-contamination andinfection of burn patients in the acute phase of care
• They are least likely to become infected but may beignored as reservoir for patients in intensive care
• Ideally, there should be a separate area forconvalescent patients and nursing staff shouldhandle patients without crossover between thesetwo patient care areas

Prevention and Control
Hydrotherapy
• Also considers the use of barrier techniques but is aseparate entity in the prevention and control ofinfection because of its emphasis on cross-contamination
• Hydrotherapy is provided in a common area usingcommon equipment and involves exposure to water
• Effective decontamination of complex equipmentbetween patients in a limited period may be a majorchallenge to burn care personnel
• Always remember that water contacts the entire burnwounds surface

BATHING
AREA

Prevention and Control
Topical Antimicrobial Agents
Daily Wound Care
• Aseptic technique for wound manipulation and
dressing
• All dressing should preferably be done on bedside
• Expose, clean and re-wrap less infected areas first
Prevention and Control
Topical Antimicrobial Agents
• Applied to the burn wound surface to diminishcolonization and multiplication ofmicroorganisms on the surface of the wound
• Most commonly used agents:1. Silver sulfadiazine
2. Cerium-nitrate-silver-sulfadiazine
• Microbial resistance has been reported
• Administer topical antimicrobial agentsaseptically


Prevention and Control
Systemic Antimicrobial Agents
• Extensive use frequently leads to selection of
resistant microorganisms
• Continued use of the same antibiotics provides a
selective advantage for these microorganisms and
are able to proliferate and displace susceptible
microorganisms in and on burn wounds
• Continued colonization may lead to an outbreak
• Appropriate use of antibiotics– use in clearly
indicated situations with appropriate basis
ANTIMICROBIALS AND BURNS
• The burn wound will always be colonized with
organisms until wound closure is achieved and
administration of systemic antimicrobials will
not eliminate this colonization but rather
promote emergence of resistant organisms.
• If antimicrobial therapy is indicated to treat a
specific infection, it should be tailored to the
specific susceptibility patterns of the organisms,

ANTIMICROBIALS AND BURNS
• Empiric antimicrobial therapy to treat fever
should be strongly discouraged because burn
patients often have fever secondary to the
systemic inflammatory response to burn injury.
• Prophylactic antimicrobial therapy is
recommended only for coverage of the
immediate peri-operative period surrounding
excision or grafting of the burn wound. This
should be discontinued within 24 hours.

CULTURING
Why?
• To provide early identification of organisms colonizing the
wound
• To monitor the effectiveness of current wound treatment
• To guide peri-operative or empiric antibiotic therapy
• To detect any cross-colonizations which occur quickly so that
further transmission can be prevented.
When?
• when the patient is admitted and at least weekly until the
wound is closed.
Burn Wound Infection Prevention and Control
Summary of Approaches:
• Use of barrier techniques
• Prevention of cross-contamination from inanimate
surfaces and food
• Prevention of cross-contamination from convalescent
patients
• Hydrotherapy
• Application of topical anti-microbial agents
• Appropriate use of systemically administered
antimicrobial agents
Acknowledgement
Acknowledgement:
Mary Joann Foronda, RN
ICN, Jose Reyes Memorial Medical Center
St. Luke's Medical Center's legacy of excellence surpasses all expectations. For
over a century, St. Luke's superior brand of healthcare service has made it truly
world class.
With astounding success anchored on five pillars of expertise-expert doctors,
state-of-the-art technology, guaranteed patient safety, excellent success rate
and passionate customer service, St Luke's Medical Center is the first hospital in
the country to be accredited by the Joint Commission International(JCI).

Thank you!


















