Open Access Protocol Telmisartan and Insulin Resistance in ...
12
Telmisartan and Insulin Resistance in HIV (TAILoR): protocol for a dose- ranging phase II randomised open- labelled trial of telmisartan as a strategy for the reduction of insulin resistance in HIV-positive individuals on combination antiretroviral therapy Sudeep P Pushpakom, 1,2,3 Claire Taylor, 4 Ruwanthi Kolamunnage-Dona, 4,5 Catherine Spowart, 4 Jiten Vora, 6 Marta García-Fiñana, 5 Graham J Kemp, 7 John Whitehead, 8 Thomas Jaki, 8 Saye Khoo, 3 Paula Williamson, 4,5 Munir Pirmohamed 1,2,3 To cite: Pushpakom SP, Taylor C, Kolamunnage- Dona R, et al. Telmisartan and Insulin Resistance in HIV (TAILoR): protocol for a dose-ranging phase II randomised open-labelled trial of telmisartan as a strategy for the reduction of insulin resistance in HIV- positive individuals on combination antiretroviral therapy. BMJ Open 2015;5: e009566. doi:10.1136/ bmjopen-2015-009566 ▸ Prepublication history for this paper is available online. To view these files please visit the journal online (http://dx.doi.org/10.1136/ bmjopen-2015-009566). Received 29 July 2015 Revised 17 August 2015 Accepted 28 August 2015 For numbered affiliations see end of article. Correspondence to Professor Munir Pirmohamed; [email protected] ABSTRACT Introduction: Telmisartan, an angiotensin receptor blocker, has beneficial effects on insulin resistance and cardiovascular health in non-HIV populations. This trial will evaluate whether telmisartan can reduce insulin resistance in HIV-positive individuals on combination antiretroviral therapy. Methods and analysis: This is a phase II, multicentre, randomised, open-labelled, dose-ranging trial of telmisartan in 336 HIV-positive individuals over a period of 48 weeks. The trial will use an adaptive design to inform the optimal dose of telmisartan. Patients will be randomised initially 1:1:1:1 to receive one of the three doses of telmisartan (20, 40 and 80 mg) or no intervention (control). An interim analysis will be performed when half of the planned maximum of 336 patients have been followed up for at least 24 weeks. The second stage of the study will depend on the results of interim analysis. The primary outcome measure is a reduction in insulin resistance (as measured by Homeostatic Model Assessment— Insulin Resistance (HOMA-IR)) in telmisartan treated arm(s) after 24 weeks of treatment in comparison with the non-intervention arm. The secondary outcome measures include changes in lipid profile; body fat redistribution (as measured by MRI); plasma and urinary levels of various biomarkers of cardiometabolic and renal health at 12, 24 and 48 weeks. Serious adverse events will be compared between different telmisartan treated dose arm(s) and the control arm. Ethics and dissemination: The study, this protocol and related documents have been approved by the National Research Ethics Service Committee North West—Liverpool Central (Ref: 12/NW/0214). On successful completion, study data will be shared with academic collaborators. The findings from TAILoR will be disseminated through peer-reviewed publications, at scientific conferences, the media and through patient and public involvement. Trial registration numbers: 04196/0024/001-0001; EUDRACT: 2012-000935-18; ISRCTN: 51069819. BACKGROUND AND RATIONALE Combination antiretroviral therapy (cART) is the mainstay for treatment of HIV and has dramatically improved the morbidity and mortality associated with HIV, turning it into a chronic disease. However, cART, together Strengths and limitations of this study ▪ This clinical trial will evaluate whether telmisar- tan can reduce insulin resistance in HIV-positive individuals on combination antiretroviral therapy; this may lead to the repositioning of telmisartan to treat metabolic disease. ▪ The trial will use an adaptive design to inform the optimal dose of telmisartan for reduction of insulin resistance. This design also allows stop- ping of the trial midway if none of the doses show a statistically significant effect after the interim analysis, thereby reducing the duration of trial and related costs. ▪ The trial is assessing a surrogate marker (insulin resistance) as an outcome measure in this trial. Despite the fact that there is a good relationship between insulin resistance and cardiovascular health, this represents a limitation of the trial. Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566 1 Open Access Protocol on March 21, 2022 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-009566 on 15 October 2015. Downloaded from
Transcript of Open Access Protocol Telmisartan and Insulin Resistance in ...

Telmisartan and Insulin Resistance inHIV (TAILoR): protocol for a dose-ranging phase II randomised open-labelled trial of telmisartan as a strategyfor the reduction of insulin resistancein HIV-positive individuals oncombination antiretroviral therapy
Sudeep P Pushpakom,1,2,3 Claire Taylor,4 Ruwanthi Kolamunnage-Dona,4,5
Catherine Spowart,4 Jiten Vora,6 Marta García-Fiñana,5 Graham J Kemp,7
John Whitehead,8 Thomas Jaki,8 Saye Khoo,3 Paula Williamson,4,5
Munir Pirmohamed1,2,3
To cite: Pushpakom SP,Taylor C, Kolamunnage-Dona R, et al. Telmisartanand Insulin Resistance in HIV(TAILoR): protocol for adose-ranging phase IIrandomised open-labelledtrial of telmisartan as astrategy for the reduction ofinsulin resistance in HIV-positive individuals oncombination antiretroviraltherapy. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566
▸ Prepublication history forthis paper is available online.To view these files pleasevisit the journal online(http://dx.doi.org/10.1136/bmjopen-2015-009566).
Received 29 July 2015Revised 17 August 2015Accepted 28 August 2015
For numbered affiliations seeend of article.
Correspondence toProfessor MunirPirmohamed;[email protected]
ABSTRACTIntroduction: Telmisartan, an angiotensin receptorblocker, has beneficial effects on insulin resistance andcardiovascular health in non-HIV populations. This trialwill evaluate whether telmisartan can reduce insulinresistance in HIV-positive individuals on combinationantiretroviral therapy.Methods and analysis: This is a phase II,multicentre, randomised, open-labelled, dose-rangingtrial of telmisartan in 336 HIV-positive individuals overa period of 48 weeks. The trial will use an adaptivedesign to inform the optimal dose of telmisartan.Patients will be randomised initially 1:1:1:1 to receiveone of the three doses of telmisartan (20, 40 and80 mg) or no intervention (control). An interimanalysis will be performed when half of the plannedmaximum of 336 patients have been followed up for atleast 24 weeks. The second stage of the study willdepend on the results of interim analysis. The primaryoutcome measure is a reduction in insulin resistance(as measured by Homeostatic Model Assessment—Insulin Resistance (HOMA-IR)) in telmisartan treatedarm(s) after 24 weeks of treatment in comparison withthe non-intervention arm. The secondary outcomemeasures include changes in lipid profile; body fatredistribution (as measured by MRI); plasma andurinary levels of various biomarkers of cardiometabolicand renal health at 12, 24 and 48 weeks. Seriousadverse events will be compared between differenttelmisartan treated dose arm(s) and the control arm.Ethics and dissemination: The study, this protocoland related documents have been approved by theNational Research Ethics Service Committee NorthWest—Liverpool Central (Ref: 12/NW/0214). Onsuccessful completion, study data will be shared withacademic collaborators. The findings from TAILoR will
be disseminated through peer-reviewed publications, atscientific conferences, the media and through patientand public involvement.Trial registration numbers: 04196/0024/001-0001;EUDRACT: 2012-000935-18; ISRCTN: 51069819.
BACKGROUND AND RATIONALECombination antiretroviral therapy (cART) isthe mainstay for treatment of HIV and hasdramatically improved the morbidity andmortality associated with HIV, turning it intoa chronic disease. However, cART, together
Strengths and limitations of this study
▪ This clinical trial will evaluate whether telmisar-tan can reduce insulin resistance in HIV-positiveindividuals on combination antiretroviral therapy;this may lead to the repositioning of telmisartanto treat metabolic disease.
▪ The trial will use an adaptive design to informthe optimal dose of telmisartan for reduction ofinsulin resistance. This design also allows stop-ping of the trial midway if none of the dosesshow a statistically significant effect after theinterim analysis, thereby reducing the duration oftrial and related costs.
▪ The trial is assessing a surrogate marker (insulinresistance) as an outcome measure in this trial.Despite the fact that there is a good relationshipbetween insulin resistance and cardiovascularhealth, this represents a limitation of the trial.
Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566 1
Open Access Protocol
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from

with the virus itself, can result in various metabolic com-plications, including metabolic syndrome, type 2 dia-betes (T2DM) and an increased risk of cardiovasculardisease (CVD).1 These metabolic complications asso-ciated with cART also occur with HIV lipodystrophy(also known as the fat redistribution syndrome), a clus-tering of morphological and metabolic abnormalitiescomprising peripheral fat loss (lipoatrophy), viscerallipid hypertrophy, insulin resistance and dyslipidaemia,2
which also increases the risk of CVD.3
The prevalence of metabolic syndrome is high incART treated HIV-infected patients (ranges from 11.2–45.4% in different HIV populations);4 the HIV DADcohort (n=33 347) found the prevalence of metabolicsyndrome to increase from 19.4% to 41.6% over a 6-yearperiod with patients having metabolic syndrome showinga fourfold increase in the incidence of T2DM and atwofold to threefold increased risk of developing CVD.5
These results have been confirmed by the MulticenterAIDS Cohort Study (n=1278)6 and a more recent ana-lysis of the DAD cohort.7 Cumulative exposure to cARTalso results in an increased risk of myocardial infarctionwith both protease inhibitors8 (PIs) and nucleosidereverse transcriptase inhibitors9 (NRTIs), as well as inintima-media thickness and an increase in the preva-lence of carotid lesions.10
Insulin resistance, a key feature of HIV lipodystrophyand metabolic syndrome, has been described as centralto cardiometabolic disease and is considered to be animportant link between features of metabolic syndrome,obesity, dyslipidaemia, T2DM and CVD.11 In vitrostudies12 and single drug studies in healthy individuals13
and HIV-infected patients14 15 have shown that PIs andNRTIs cause insulin resistance. The prevalence ofinsulin resistance in cART-treated HIV-infected patientsranges from 10 to 37%,14–16 indicating a significant rolefor cART in its development. Several mechanisms havebeen suggested to be responsible for cART-inducedinsulin resistance; these include cART-induced inhib-ition of adipocyte differentiation,17 increased secretionof adipokines such as interleukin 6 (IL-6) and tumournecrosis factor α (TNF-α),18 and impairment of theinsulin signalling pathway.12
Clinical intervention to arrest or reverse cART-associatedinsulin resistance has been suggested as a strategy toreduce the incidence of T2DM and CVD in HIV-positivepatients. Insulin sensitisers such as thiazolidinediones andmetformin have been trialled but results from randomisedclinical trials in HIV patients have shown mixedresults.19 20 Moreover, the associated adverse effects maylimit their use in HIV-infected patients.21 22 Therefore,there is a need for novel clinical interventions with provensafety profile that can reduce cART-induced insulin resist-ance in HIV-infected individuals.Some angiotensin receptor blockers (ARBs) have a
beneficial effect on insulin resistance and T2DM, owingto their action on the renin-angiotensin system andpartial agonist activity at PPARγ, an important regulator
of adipocyte function. Telmisartan shows maximalpotency on PPARγ when compared to other ARBs andhas been reported to reduce insulin resistance in severalin vitro,23 24 animal25 26 and clinical studies.27–30
Telmisartan also improves adiponectin levels, an import-ant metabolic marker of insulin resistance and athero-sclerotic disease, lipid control, and has favourable effectson fasting serum insulin and high sensitivity C reactiveprotein27 (high-sensitivity C reactive protein (hs-CRP); amarker of CVD). Telmisartan has also been shown toreduce visceral, but not subcutaneous, fat accumulationin patients with metabolic syndrome.31 32 Importantly,telmisartan already has a license for cardiovascular pro-tection in a broad group of at-risk patients (ONTARGETtrial; 120 000 patient-years of follow-up).33
In contrast to the non-HIV population, the effect oftelmisartan on insulin resistance in cART-treatedHIV-positive patients has not been assessed. Using invitro adipocyte models, we (Pushpakom, unpublished)and others34 have shown that telmisartan partiallyreverses the antiadipogenic effects of antiretrovirals. Ourtrial has therefore been designed to address this.Furthermore, although the dose-response relationship oftelmisartan in hypertension is well known, whether thiswould also be similar in reducing insulin resistance isunclear. Our in vitro study in fact suggested that theremight be a non-monotone (bell shaped) relationship oftelmisartan on markers of adipocyte health. We havetherefore utilised an adaptive trial design during theinitial stage of the study to carefully assess the dose–response relationship of telmisartan in vivo.
OBJECTIVESThe primary objective of the trial is to determine theeffect of telmisartan on insulin resistance in HIV-positiveindividuals on cART using Homeostatic ModelAssessment—Insulin Resistance (HOMA-IR). HOMA-IRis a measurable, validated surrogate marker of insulinresistance.35
The secondary objectives include assessing the optimaldose of telmisartan that can significantly reduce insulinresistance, evaluation of tolerability of telmisartan inHIV patients and mechanistic evaluation of the meta-bolic effects of telmisartan. The mechanistic evaluationof telmisartan will explore longitudinal changes inplasma markers that are important indicators of cardio-metabolic health (adiponectin, IL-6, resistin, TNFα,hs-CRP and lipids) at different time points; it will alsoutilise MRI and 1H MR spectroscopy (MRS) to assess theeffect of telmisartan on total body fat and intrahepaticand intramyocellular triglyceride content, respectively.The MRI/MRS evaluation will be limited to a subset ofparticipants who are recruited locally.Telmisartan is known to possess renoprotective
effects;36 37 in addition to the above objectives, the studywill also assess its effects on the kidney using urinarymarkers of renal injury (conventional markers such as
2 Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from

creatinine, urea, total protein and novel biomarkerssuch as KIM-1, NGAL and RBP).
TRIAL DESIGNThis study is a phase II, multicentre, randomised, open-labelled, dose-ranging trial of telmisartan in HIV-positiveindividuals over a period of 48 weeks. The sample sizefor the study is 336 (see Sample size calculation), but atotal of 370 patients will be recruited to participate inthis study to account for patient withdrawals (estimatedto be 10%).The optimal dose of telmisartan that elicits the
desired response is not known; hence, an adaptivedesign is utilised for this study. The first stage of thestudy will be dose-ranging where patients will be rando-mised 1:1:1:1 to receive one of three doses of telmisartan(20, 40 and 80 mg) or no intervention (control). Aninterim analysis will be performed when half of theplanned maximum of 336 patients have been followedup for at least 24 weeks. The second stage of the studywill depend on the results of interim analysis, whichcould be one of the three outcomes listed below:1. One or more active dose groups are substantially
more effective than control; this will lead to a stop-ping of the study and the corresponding dose(s) willbe taken directly into phase III.
2. No dose shows sufficient promise at the interim ana-lysis; this will also lead to a stopping of the study.
3. At least one of the doses shows some improvementover control at interim analysis; this will lead to asecond stage where that/these dose(s) will be fol-lowed up along with the control for a further24 weeks (total: 48 weeks). Additional patients willalso be recruited to these dose(s) and control. If atthe final analysis a large enough reduction in24 week HOMA-IR score is found, the correspondingactive dose will be recommended for phase III.In the telmisartan 40 and 80 mg arms, dose titration
will be undertaken over 2−4 weeks in order to step up tothe allocated dose (as per the Summary of ProductCharacteristics; SPC), or else the maximum tolerateddose if the target is not achieved. All assessments will becarried out at baseline and at weeks 12, 24 and 48 post-treatment with telmisartan, as well as in the control arm.For those who participate in the MRI/MRS substudy,assessment will be at baseline and 24 weeks. The studyflow diagram is given in figure 1.The Clinical Trials Research Centre (CTRC),
University of Liverpool, is the coordinating centre forthis study (http://www.liv.ac.uk/translational-medicine/research/ctrc/about/).
PATIENT RECRUITMENTIdentification of eligible patientsPatients who are eligible for inclusion into the trial willbe identified and recruited through HIV specialtycentres located in the UK that have agreed to participate
in the study. These HIV specialty centres are part of thesecondary care system and are mostly based in an urbansetting. Participants will be identified by the clinical teamat each centre via a search of the patient database(s)either electronically or manually or a clinic list review tofind potentially eligible patients. The inclusion andexclusion criteria are detailed in box 1.
Consent procedureAt the routine clinic visit, eligible patients are informedof the study by a member of the clinical team orresearch staff. A Patient Information Sheet and instruc-tions on how to proceed if they are interested in takingpart will be provided by the research nurse. All patientswill be provided with a full explanation of the trial andgiven sufficient time to consider their decision beforeobtaining informed written consent. In consenting tothe trial, patients are consenting to trial treatment,follow-up and data collection. Patients are free to with-draw consent at any time without providing a reason.Follow-up of these patients will be continued throughthe trial research nurses and the lead investigator ateach centre unless the participant explicitly also with-draws consent for follow-up.
Baseline assessmentsOnce informed consent has been obtained from thepatient, they will be booked in for a baseline assessmentvisit within 30 days of giving consent. The patient willbe advised to arrive fasting when reporting for the base-line assessment. The research team will conduct thebaseline assessments and complete the eligibility andbaseline case report form (CRF) during the baselineassessment visit. The baseline assessments include fulfil-ment of eligibility criteria; recording demographicdetails; full medical and drug history; body weight andvital signs; and waist/thigh circumference. A urine preg-nancy test is offered for females of childbearing poten-tial since telmisartan is not recommended during thefirst trimester of pregnancy and is contraindicatedduring the second and third trimesters of pregnancydue to its teratogenic potential. However, a refusal toundertake a pregnancy test will not preclude trial entry.Blood samples (for plasma, serum and DNA) and urinewill also be collected from each patient at the time ofbaseline screening. Table 1 details the schedule of studyassessments conducted.
RANDOMISATIONParticipants will be randomised to receive telmisartan20, 40, 80 or control (no intervention) in a 1:1:1:1 ratioonce (A) eligibility criteria have been fulfilled; (B) fullyinformed written consent has been obtained; and (C)baseline assessments have been completed. Participantswill be randomised using a bespoke secure (24 h) webbased randomisation programme controlled centrally bythe CTRC, University of Liverpool. For each recruiting
Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566 3
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from
centre, randomisation will be stratified by ethnicity(African-American and non-African-American) whereethnicity is determined by self-categorisation using theNHS ethnicity codes. Centres will be provided withemergency back-up randomisation envelopes to be usedin the event of a system failure or when a system failurecannot be resolved in a reasonable time frame. Patientsmay only be randomised into the study by an authorisedmember of staff at the study site as detailed on the dele-gation log. Participants may only be randomised into thestudy once.
TRIAL INTERVENTIONSTelmisartan is an angiotensin receptor antagonist indi-cated for clinical use as an antihypertensive agent. It isalso used to reduce cardiovascular events in patientswho are at risk. However, the current trial uses telmisar-tan outside its licensed indications.At the onset of the trial, telmisartan was under patent
(Boehringer Ingelheim GmBH; Micardis); however,during the course of the trial, the patent expired andseveral manufacturers started marketing generic
telmisartan, which was then also used in the trial, butthe trial will continue to use Micardis SPC as the refer-ence SPC. Telmisartan used in this trial is sourced viausual local NHS procurement arrangements.Telmisartan tablets are available in 20, 40 or 80 mg
doses and therefore fit in with the dose range to beused in the trial prior to interim analysis. In most cases,the participant is provided their required dose in onetablet. Telmisartan tablets are for once-daily oral admin-istration and should be taken with liquid, with orwithout food. The CRFs will be used to record whichbrand has been dispensed to the participant.Telmisartan is stored as per the manufacturer’s SPC.For each randomised patient, treatment is for a
maximum period of 48 weeks. The principal investigatoror delegated other will issue a prescription based on thepatient’s randomisation status and the trial treatmentcan start immediately after randomisation. For the threetreatment arms, treatments will be dispensed at theappropriate doses at baseline, at 12 weeks and then at24 weeks, unless interruption or discontinuation is war-ranted. Wherever titration of dose is required, the treat-ment starts with 20 mg and is then titrated upwards over
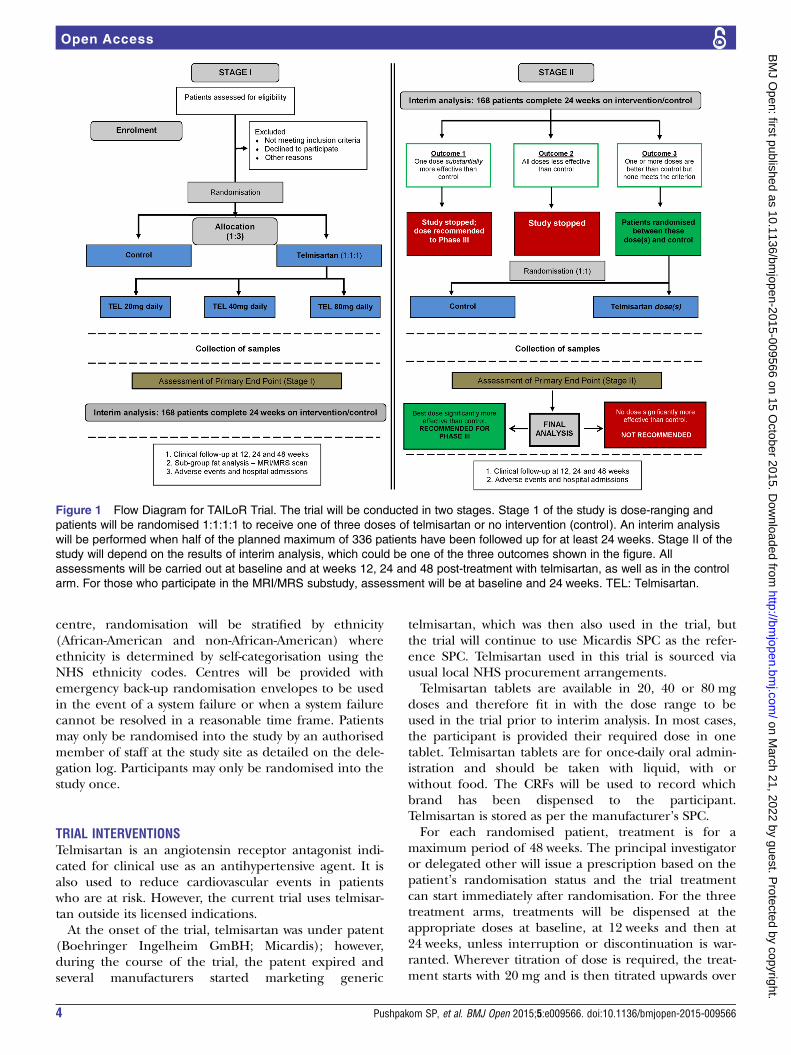
Figure 1 Flow Diagram for TAILoR Trial. The trial will be conducted in two stages. Stage 1 of the study is dose-ranging and
patients will be randomised 1:1:1:1 to receive one of three doses of telmisartan or no intervention (control). An interim analysis
will be performed when half of the planned maximum of 336 patients have been followed up for at least 24 weeks. Stage II of the
study will depend on the results of interim analysis, which could be one of the three outcomes shown in the figure. All
assessments will be carried out at baseline and at weeks 12, 24 and 48 post-treatment with telmisartan, as well as in the control
arm. For those who participate in the MRI/MRS substudy, assessment will be at baseline and 24 weeks. TEL: Telmisartan.
4 Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from
a period of 2 weeks (for a 40 mg dose) or 4 weeks (foran 80 mg dose). At 48 weeks, administration of trialtreatments will be stopped and any unused medications
will be returned to pharmacy for disposal via their localprocedures. There is a 2 week attendance window oneither side of each of the follow-up visits and a 4 daywindow on either side of the titration visits.Since the results of the interim analysis decide the
design of stage II of the trial, those patients who are on adose that is not taken forward to stage II will be asked tostop taking the medication completely. These patientswill continue to be monitored for any adverse events for aperiod of 7 days (washout period for telmisartan) afterwhich they will no longer be part of the trial and willreturn to routine care. For those who are on trial armswhose dose(s) are taken forward to stage II, they will beasked to continue on the same dose for a further24 weeks. Since treatment is not stopped between stages Iand II, some participants may receive up to a maximumof 48 weeks trial treatment before the results of theinterim analysis are known. For patients recruited afterthe results of interim analysis are known, they will be ran-domised equally to the non-intervention (control) armand the remaining telmisartan dose arm(s).Dose modifications will be allowed in those who are
randomised to a particular dose arm but do not toleratethat dose. The patient will be allowed to continue onthe nearest dose tolerated. Those who show adverseeffects as a result of the trial intervention or due to theHIV therapy may be withdrawn from the trial treatment.The decision to interrupt or discontinue trial therapy isat the discretion of the treating physician using theirinformed clinical opinion. Any changes will be docu-mented in the CRF along with the justification for thosechanges. Patients who withdraw from study treatmentwill be asked to allow continuation of scheduled evalua-tions, complete an end-of-study evaluation if appropriateand be given appropriate care under medical supervi-sion until the symptoms of any adverse event resolve orthe patient’s condition becomes stable. Follow-up ofthese patients will be continued through the trialresearch nurses and the lead investigator at each centreunless the participant explicitly also withdraws consentfor follow-up. Data up to the time of withdrawal will beincluded in the analyses unless the patient explicitlystates that this is not their wish.
PATIENT FOLLOW-UPApart from the dose-titration visits for participants in the40 and 80 mg arms, follow-up visits will be designed tofit with routine hospital visits where possible. The studywill also allow a 2 week window on either side of thescheduled follow-up visit date to ensure flexibility.Individual patients will be sent reminders aboutfollow-up visits by the research nurses provided theyhave agreed to receive them. If any of the trial patientsare lost to follow-up, contact will be attempted throughthe research nurse and lead investigator at each centre.Wherever possible, information on the reason for loss tofollow-up will be recorded.
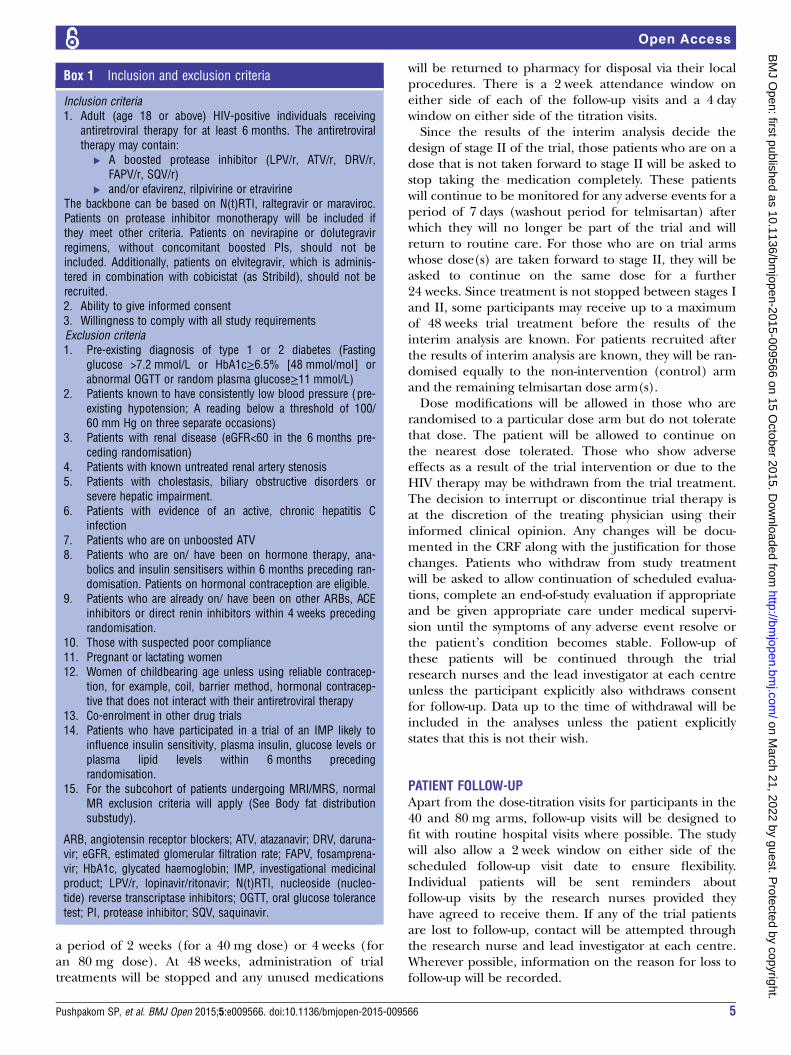
Box 1 Inclusion and exclusion criteria
Inclusion criteria1. Adult (age 18 or above) HIV-positive individuals receiving
antiretroviral therapy for at least 6 months. The antiretroviraltherapy may contain:
▸ A boosted protease inhibitor (LPV/r, ATV/r, DRV/r,FAPV/r, SQV/r)
▸ and/or efavirenz, rilpivirine or etravirineThe backbone can be based on N(t)RTI, raltegravir or maraviroc.Patients on protease inhibitor monotherapy will be included ifthey meet other criteria. Patients on nevirapine or dolutegravirregimens, without concomitant boosted PIs, should not beincluded. Additionally, patients on elvitegravir, which is adminis-tered in combination with cobicistat (as Stribild), should not berecruited.2. Ability to give informed consent3. Willingness to comply with all study requirementsExclusion criteria1. Pre-existing diagnosis of type 1 or 2 diabetes (Fasting
glucose >7.2 mmol/L or HbA1c≥6.5% [48 mmol/mol] orabnormal OGTT or random plasma glucose≥11 mmol/L)
2. Patients known to have consistently low blood pressure (pre-existing hypotension; A reading below a threshold of 100/60 mm Hg on three separate occasions)
3. Patients with renal disease (eGFR<60 in the 6 months pre-ceding randomisation)
4. Patients with known untreated renal artery stenosis5. Patients with cholestasis, biliary obstructive disorders or
severe hepatic impairment.6. Patients with evidence of an active, chronic hepatitis C
infection7. Patients who are on unboosted ATV8. Patients who are on/ have been on hormone therapy, ana-
bolics and insulin sensitisers within 6 months preceding ran-domisation. Patients on hormonal contraception are eligible.
9. Patients who are already on/ have been on other ARBs, ACEinhibitors or direct renin inhibitors within 4 weeks precedingrandomisation.
10. Those with suspected poor compliance11. Pregnant or lactating women12. Women of childbearing age unless using reliable contracep-
tion, for example, coil, barrier method, hormonal contracep-tive that does not interact with their antiretroviral therapy
13. Co-enrolment in other drug trials14. Patients who have participated in a trial of an IMP likely to
influence insulin sensitivity, plasma insulin, glucose levels orplasma lipid levels within 6 months precedingrandomisation.
15. For the subcohort of patients undergoing MRI/MRS, normalMR exclusion criteria will apply (See Body fat distributionsubstudy).
ARB, angiotensin receptor blockers; ATV, atazanavir; DRV, daruna-vir; eGFR, estimated glomerular filtration rate; FAPV, fosamprena-vir; HbA1c, glycated haemoglobin; IMP, investigational medicinalproduct; LPV/r, lopinavir/ritonavir; N(t)RTI, nucleoside (nucleo-tide) reverse transcriptase inhibitors; OGTT, oral glucose tolerancetest; PI, protease inhibitor; SQV, saquinavir.
Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566 5
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from
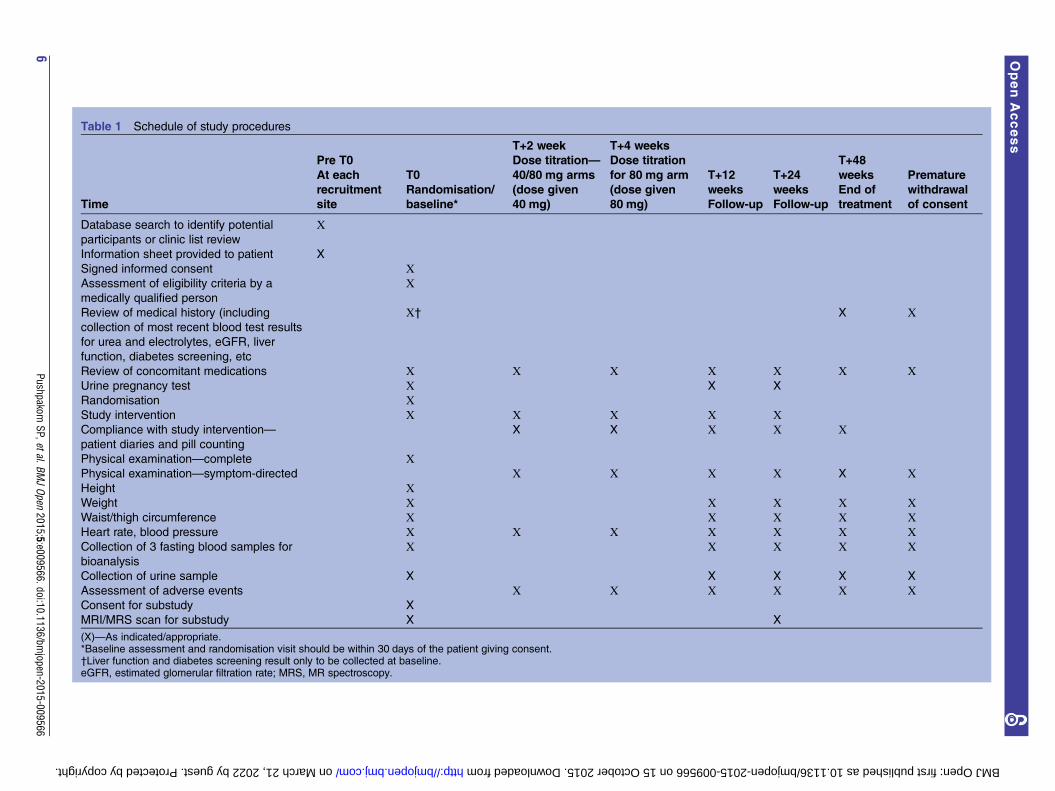
Table 1 Schedule of study procedures
T+2 week T+4 weeks
Time
Pre T0
At each
recruitment
site
T0
Randomisation/
baseline*
Dose titration—
40/80 mg arms
(dose given
40 mg)
Dose titration
for 80 mg arm
(dose given
80 mg)
T+12
weeks
Follow-up
T+24
weeks
Follow-up
T+48
weeks
End of
treatment
Premature
withdrawal
of consent
Database search to identify potential
participants or clinic list review
Х
Information sheet provided to patient X
Signed informed consent ХAssessment of eligibility criteria by a
medically qualified person
Х
Review of medical history (including
collection of most recent blood test results
for urea and electrolytes, eGFR, liver
function, diabetes screening, etc
Х† X Х
Review of concomitant medications Х Х Х Х Х Х ХUrine pregnancy test Х X X
Randomisation ХStudy intervention Х Х Х Х ХCompliance with study intervention—
patient diaries and pill counting
X X Х Х Х
Physical examination—complete ХPhysical examination—symptom-directed Х Х Х Х X ХHeight ХWeight Х Х Х Х ХWaist/thigh circumference Х Х Х Х ХHeart rate, blood pressure Х Х Х Х Х Х ХCollection of 3 fasting blood samples for
bioanalysis
Х Х Х Х Х
Collection of urine sample X X X X X
Assessment of adverse events Х Х Х Х Х ХConsent for substudy X
MRI/MRS scan for substudy X X
(X)—As indicated/appropriate.*Baseline assessment and randomisation visit should be within 30 days of the patient giving consent.†Liver function and diabetes screening result only to be collected at baseline.eGFR, estimated glomerular filtration rate; MRS, MR spectroscopy.
6Pushpakom
SP,etal.BMJOpen
2015;5:e009566.doi:10.1136/bmjopen-2015-009566
OpenAccess
on March 21, 2022 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-009566 on 15 October 2015. Downloaded from

OUTCOMES AND ASSESSMENTSEfficacy of trial treatments will be assessed throughoutthe period of the study. The primary outcome measureis a reduction in insulin resistance (as measured byHOMA-IR) in telmisartan treated arm(s) after 24 weeksof treatment in comparison with the non-interventionarm. Fasting plasma and serum samples will be collectedfrom each participant at baseline and at follow-up visits(weeks 12, 24 and 48) and stored under appropriateconditions locally. Biochemical analyses will be carriedout centrally in an accredited clinical laboratory. Fastingplasma glucose will be measured by standard clinicalmethods and serum insulin will be measured by an elec-trochemiluminescence immunoassay using a Cobas CAnalyser (Roche Diagnostics, Switzerland). HOMA-IRwill be calculated using the equation: (fasting seruminsulin (mU/L)×fasting plasma glucose (mmol/L))/22.5. The secondary outcome measures are detailed inbox 2. Serum and urine biomarker analyses and DNAextraction will be performed centrally using HumanMultiplex ELISA (Millipore) on a BioPlex 200 System(BioRad) and Chemagic Magnetic Separation Module I(MSM I), respectively.
Assessment of compliance with study treatment/sAll participants on intervention arms are given a treat-ment diary to record their daily treatment compliance.Compliance with the study treatment will be ascertainedon the basis of what is recorded in the treatment diaryand by recording the number of pills remaining in thepacks.
Body fat redistribution substudyA substudy will be undertaken only for patients recruitedfrom the North West of UK to assess whether telmisartan
results in any changes in the total body adipose contentand intrahepatic and intramyocellular lipid content. Thiswill be assessed at baseline and at 24 weeks by MRI and1H MRS in an on-site MRI research facility. Patientsrecruited will be given a separate patient informationsheet and consent form containing information on thesubstudy and requirements for MRI/MRS. Participantswill be allowed to withdraw from the substudy anytimebut remain in the main study. Only patients who consentto take part in the main study and satisfy the normal MRexclusion criteria (normal MR exclusion criteria includepatients using pacemakers, cochlear implants, piercings,metal in the head or elsewhere in the body, and thosewho suffer from claustrophobia) will be included in thesubstudy. MRI of the total body adipose content will beundertaken on a Siemens 1.5 T Symphony scanner(Siemens, Erlangen Germany) using well-establishedmethods.38 MRI will be analysed to obtain volume esti-mates of total body subcutaneous, total internal, subcuta-neous abdominal and intra-abdominal adipose tissue. Inthe same subcohort of patients, liver and skeletal muscle1H MR spectra will be acquired using the Siemens bodycoil and Siemens CP extremity coil, respectively, usingestablished methods.39 Analysis of all imaging data will beconducted centrally.
SAMPLE SIZE CALCULATIONThe primary response from each patient is the differ-ence between the baseline HOMA-IR score and theirHOMA-IR score at 24 weeks. The design has been con-structed under the assumption that for all patients thisresponse is normally distributed with a common SD, σ.The sample size calculation is based on a one-sided
type I error of 5% and a power of 90%. If there is no dif-ference between the mean response on any treatmentand that on control, then a probability of 0.05 is set forthe risk of erroneously ending the study with a recom-mendation that any treatment be tested further. For thepower, we adopt a generalisation of this power require-ment to multiple active treatments due to Dunnett.40
Effect sizes are specified as the percentage chance of apatient on active treatment achieving a greater reductionin HOMA-IR score than a patient on control as this spe-cification does not require knowledge of the commonSD, σ. The requirement is that, if a patient on the bestactive dose has a 65% chance of a better response thana patient on control, while patients on the other twoactive treatments have a 55% chance of showing a betterresponse than a patient on control, then the best activedose should be recommended for further testing withprobability 1−β=0.90. A 55% chance of achieving abetter response on active dose relative to control corre-sponds to a reduction in mean HOMA-IR score of abouta sixth of an SD (0.178σ), while the clinically relevanteffect of 65% corresponds to a reduction of about halfan SD (0.545σ). The critical values for recommendingthat a treatment is taken to further testing at the interim
Box 2 Secondary outcome measures
1. Change in lipid profile (total cholesterol, triglycerides, LDL-cand HDL-c) at weeks 12, 24 and 48 between telmisartantreated arm(s) and the control arm.
2. Change in body fat redistribution as measured by MRI/MRS at24 weeks between telmisartan treated arm(s) and control arm(See substudy).
3. Change in plasma concentrations of biomarkers (adiponectin,lipin1, IL-6, TNF-α, resistin and hs-CRP) at 12, 24 and48 weeks between telmisartan treated arm(s) and control arm.
4. Change in insulin resistance, measured longitudinally at weeks12 and 48, in telmisartan treated arm(s) in comparison withthe control arm.
5. Change in urinary biomarker levels at 12, 24 and 48 weeksbetween telmisartan treated arm(s) and the control arm.
6. Difference in expected and unexpected serious adverse eventsbetween different telmisartan treated dose arm(s) and thecontrol arm over the study follow-up.
HDL-c, high density lipoprotein-cholesterol; hs-CRP, high sensi-tive, C reactive protein; IL-6, interleukin-6; LDL-c, low densitylipoprotein-cholesterol; TNF-α, tumour necrosis factor-α.
Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566 7
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from
and final analyses (2.782 and 2.086) have been chosento guarantee these properties using a method describedby Magirr et al,41 generalising the approach ofWhitehead and Jaki.42
The maximum sample size of this study is 336 evalu-able patients, although the use of the interim analysismay change the required sample size. The study willrecruit additional patients to account for an anticipated10% dropout rate.
Interim monitoring and analysesAn interim analysis will take place once the primary endpoint is available for at least 42 patients on each arm (ie,half of the planned maximum of 336 patients). Thesample SD pooled across all four arms is used to con-struct test statistics expressing the advantage of each ofthe three active treatments over control. The analysis willbe proceeding as follows:1. If the largest test statistic exceeds 2.782, the study will
be stopped and the corresponding dose will berecommended for further testing.
2. If any active dose shows no improvement over control(ie, has a negative test statistic), that active dose willbe dropped.
3. If no active dose shows an improvement over control,the study will be stopped and no significant improve-ment over control will be claimed.
4. If some improvement over control is detected for atleast one dose (ie, at least one test statistic is between 0and 2.782), the study will progress to the second stage.At the interim analysis, doses may be dropped from
the trial, or the trial may be stopped altogether.Consequently, the required sample size when the deci-sion is reached could be smaller than the maximumstated number of 336 patients. The values 168 (if thestudy is stopped following interim analysis), 252 (if oneactive dose arm is promoted to the second stage), 294(if two active dose arms are promoted to the secondstage) and 336 (if all three active dose arms are pro-moted to the second stage) are possible. The reducedsample sizes refer to the numbers of patients with24 week HOMA-IR scores which are included in the ana-lysis. Evaluation of the patient withdrawal rate will becarried out and the sample size will be adjusted accord-ingly. There will be additional patients who have beenrecruited during the 24 weeks prior to extracting thedata for interim analysis and their number will dependon the recruitment rate achieved. A decision to discon-tinue recruitment, in all patients or in selected sub-groups, will be made on the basis of results from theinterim analysis by the Independent Data and SafetyMonitoring Committee (IDSMC).
STATISTICAL ANALYSISPrimary outcome analysisThree different doses of the intervention will be evalu-ated against the control in stage 1 of the study and an
interim analysis will take place that will allow ineffectivedoses to be eliminated quickly while a dose showing apositive effect can be taken forward. An ANCOVA modelwill be fitted for a 24 week HOMA-IR score adjusting forthe stratification factor (African-American and non-African-American), and the corresponding t—values willbe used to construct test statistics expressing the advan-tage of each of the active treatments over control. Thelargest of these test statistics will be compared to theinterim critical value (2.782) and proceed as discussedabove at the interim analysis. At the final analysis, if thelargest comparative test statistic exceeds the final criticalvalue (2.086), then this dose would be recommendedfor further study. Adjustments can be made to allow forany discrepancies between target and actual sample sizeswhile still preserving the one-sided type I error rate at0.05.
Secondary outcome analysisLinear mixed effect models will be used to analyse sec-ondary and mechanistic outcomes. The evaluation ofbeneficial and adverse biomarkers in relation to insulinresistance will be examined using the joint modellingapproach43 44 accounting for informative loss tofollow-up or censoring. Structural equation models45 willbe used to assess the inter-relationship between multiplebiomarkers over effect of treatment while accounting fortime-varying confounders. Mechanistic outcomes such aschange in body fat, liver and muscle fat distribution willbe analysed using a multiple linear regression model.Differences will be considered significant at p<0.05.Differences between the groups will be estimated with95% CIs.
SAFETY REPORTINGThe CTRC will be notified of all serious adverse reac-tions (SAR), serious adverse events (SAE) and suspectedunexpected serious adverse reactions (SUSARs) within24 h of the local site becoming aware of the event. TheCTRC will notify the MHRA and main Research EthicsCommittee (REC) of all SUSARs occurring during thestudy on behalf of the chief investigator according to thefollowing timelines: fatal and life-threatening within7 days of notification and non-life threatening within15 days. It will also submit an annual report of all SAEsto the sponsor, MHRA and the main REC and providethe IDSMC with listings of all SAEs on an ongoing basis.The study may be prematurely discontinued on the basisof new safety information, or for other reasons given bythe IDSMC and/or Trial Steering Committee (TSC),sponsor or REC concerned. All investigators will beinformed of all SUSARs occurring throughout the study.The assignment of the severity/grading of adverseevents will be made by the investigator responsible forthe care of the participant using the Division of AIDSTable for Grading the Severity of Adult and PaediatricAdverse Events V.1.0 (2009) definitions.46 The CTRC
8 Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from

will monitor SAE and ADR reporting rates across sitesduring the course of the trial and if any inconsistenciesare noted, they will be investigated and additional train-ing provided.
Reporting of pregnancyFemale study participants of childbearing potential willbe offered a pregnancy test as part of the trial screeningprocess and at weeks 12 and 24. Any pregnancy whichoccurs during the study will be reported as an SAE tothe CTRC within 24 h of the site becoming aware of itsoccurrence and the participant will be instructed imme-diately to stop taking study drugs. All pregnancies thatoccur during treatment need to be followed up untilafter the outcome. The investigator will discuss the risksof continuing with the pregnancy and the possible effectto the fetus with the participant.
ETHICAL CONSIDERATIONSThe conduct of this study will be in accordance with theDeclaration of Helsinki, 1964 and later revisions.The main ethical issue is the potential allocation of
participants to less effective treatment arms. In stage 1of the trial, a quarter of the patients will be allocated tothe non-intervention control arm; it is also likely thatsome of the intervention arms could be found to be lesseffective during the interim analysis and hence bedropped. However, these comparator arms are necessaryfor the identification of a positive drug effect in thetreatment arm(s) and its optimal dose. This does nothave any impact on the control of HIV infection sincethe intended use of telmisartan in this patient popula-tion is only as an adjuvant drug and not as the primarydrug to treat HIV infection.Telmisartan is an antihypertensive drug, and thus
there is a possibility that some of the participants rando-mised to the higher doses may experience hypotension.The eligibility criteria aim to exclude those who consist-ently show hypotension; moreover, the prevalence oftelmisartan-induced hypotension in normotensive indivi-duals has been found to be rare in previous studies.47 48
However, the trial will take adequate precautions such asroutine blood pressure monitoring to address this issue.There will be a minor increase in the pill burden to theparticipants of this trial; however, this is not a majorissue since the intervention is available as a single tabletthat needs to be taken only once daily.Other ethical issues include contraception for all
women of childbearing age during the course of thetrial and additional clinic visits required for baselineassessments and dose titration (limited to only 40 and80 mg arms). For a subset of patients recruited to under-take the substudy, it may involve additional patient timeto undertake MRI/MRS scans. In the event that thestudy is discontinued, participants will be treated accord-ing to standard clinical care.
Ethical and regulatory approvalsThe study, this protocol and related documents havebeen approved by the National Research Ethics ServiceCommittee North West—Liverpool Central (Ref: 12/NW/0214).This study falls within the remit of the EU Directive
2001/20/EC, transposed into UK law as the UKStatutory Instrument 2004 No 1031: Medicines forHuman Use (Clinical Trials) Regulations 2004 asamended. This trial has been registered with theMedicines and Healthcare Products Regulatory Agency(MHRA) and granted a Clinical Trial Authorisation(04196/0024/001-0001). The EUDRACT number is2012-000935-18.
DATA COLLECTION AND TRIAL MONITORINGData collectionData management procedures for the trial will be devel-oped and overseen by the CTRC, University ofLiverpool. The CTRC will provide training, essentialdocumentation and user support to the study centres,and monitoring, if triggered by an incident or whereappropriate. All primary data will be entered into thestudy CRF for this study. Each participant will beassigned a unique screening number at the start of theassessment, which will be recorded on the consent formand the baseline assessment CRF and on all other docu-ments used to record participant data. All original CRFswill be returned to the CTRC. For the participant treat-ment diaries, the participant initials and randomisationnumber will be clearly labelled on all documents. Thelaboratory read-outs will be obtained for blood, urinesamples and for the body fat distribution substudy fromautomated equipment. These will be uploaded securelyto the central trial database.
Trial monitoringTrial monitoring procedures for this study are based ona risk assessment conducted by the CTRC, University ofLiverpool. Guidance issued by the MRC, Department ofHealth and the MHRA on risk-adapted approaches tothe management of CTIMPs proposes a three-level cat-egorisation for the potential risk associated with anIMP.49 In this study, telmisartan is used outside the man-ufacturer’s indication; therefore, the IMP here is cate-gorised as Type B: ‘somewhat higher than that of standardmedical care’. This level of risk will inform the risk assess-ment, regulatory requirements, nature and extent of themonitoring, and the management processes used in thetrial.
Central monitoringData stored at the CTRC will be checked for missing orunusual values and for consistency within participantsover time. Any suspect data will be returned to the sitein the form of data queries and sites are expected torespond to these queries with an explanation/resolution
Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566 9
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from
to the discrepancies. There are a number of monitoringfeatures in place at the CTRC to ensure reliability andvalidity of the trial data.
Clinical site monitoringThe CTRC personnel may need direct access to primarydata such as patient records and laboratory reports; sincethis affects the patient’s confidentiality, this fact isincluded on the patient information sheet. Individualparticipant medical information obtained as a result ofthis study is considered confidential and disclosure tothird parties is prohibited. Medical information may begiven to the participant’s medical team and all appropri-ate medical personnel responsible for the participant’swelfare. The only identifiable data transferred is theconsent form and this is disclosed in the patient informa-tion sheet and consent form. The CTRC will preserve theconfidentiality of participants taking part in the study andThe University of Liverpool is registered as a DataController with the Information Commissioners Office.
Trial management and oversightTrial Management GroupThe Trial Management Group (TMG) will be respon-sible for the day-to-day running and management of thetrial and will meet, as a minimum, approximately 10times a year. The TMG will comprise the ChiefInvestigator, other lead investigators (clinical and non-clinical) and members of the trial coordinating centre(CTRC).
Trial Steering CommitteeThe TSC will meet at least once annually and willprovide overall supervision for the trial and provideadvice through its independent Chairperson. The ultim-ate decision for the continuation of the trial lies withthe TSC. The TSC will consist of an independent chair-person (with clinical expertise in HIV), two independ-ent statisticians with expertise in adaptive trial designand medical statistics, a user representative, the investiga-tors, representatives of the research networks, sponsorsand principal investigators.
Independent Data and Safety Monitoring CommitteeThe IDSMC will meet at least once annually and will beresponsible for reviewing and assessing recruitment,interim monitoring of safety and effectiveness, trialconduct and external data. It will provide a recommen-dation to the TSC concerning the continuation of thestudy. The IDSMC will consist of an independent chair-person (with clinical expertise in HIV) and two inde-pendent members: one who is an expert in the field ofHIV lipodystrophy, and one who is an expert in medicalstatistics and adaptive trial design. Terms of referencefor the TMG and TSC and Charter for the IDSMC areavailable on request from the CTRC, University ofLiverpool.
NOTIFICATION OF AMENDMENTSAny amendments made to the study including protocolamendments will be communicated to the appropriateagencies for approval prior to implementation. All sub-stantial amendments made will be reviewed by thesponsor prior to submission to the REC and the MHRAfor their approval; substantial amendments will also benotified to all participating research sites. All substantialand non-substantial amendments as well as respectiveregulatory approvals will be provided electronically viathe Integrated Research Application System (IRAS) tothe Clinical Research Network North West Coast whowill notify the Research and Development Departmentat individual participating sites for local approval andimplementation.
TIME FRAME AND TRIAL STATUSTAILoR is currently recruiting from 19 specialist HIVcentres throughout the UK. The study has so farrecruited 293 patients and has been given a no-costextension to continue recruitment till the end of July2015. Each participant is followed up for a total of48 months. The total study period is 56 months.
DISCUSSIONMetabolic disease and insulin resistance continue to bea major problem in HIV-infected individuals; a recentlongitudinal study observed an overall insulin resistanceprevalence of 21% (using a HOMA-IR cut-off >3.8) inHIV patients.50 Given that HIV is now considered achronic disease with an ageing population51 and the factthat ageing further increases the susceptibility toage-related comorbidities such as metabolic and CVD,the magnitude of this problem is likely to become evengreater. This is exemplified by the fact that the preva-lence of insulin resistance in HIV patients increases withage, ranging from 5% in patients <30 years to 30% inpatients over 60 years of age.50 Therefore, there is apressing need to develop or identify newer therapies tocombat metabolic disease in this group of individuals;this trial will potentially address this need and may leadto the repositioning of telmisartan to treat metabolicdisease.Since the start of this trial, two smaller studies have
already reported beneficial metabolic effects of telmisar-tan in cART-treated HIV patients. While one studyobserved a reduction in HOMA-IR with 80 mg telmisar-tan,52 the other did not find a reduction in HOMA-IRbut observed a loss of total and subcutaneous fat with a40 mg dose.53 This clearly underlines the need for awell-powered trial to confirm the efficacy of telmisartanfor reducing insulin resistance and this is met by thecurrent study. The trial also utilises a novel adaptivedesign which will enable identification of the optimaldose of telmisartan, if ultimately it is found to elicit astatistically significant beneficial effect on insulin resist-ance. The adaptive design also allows stopping of the
10 Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from

trial midway if none of the doses show a statistically sig-nificant effect after the interim analysis; this will reducethe duration of the trial and result in cost saving.Of course, we are assessing a surrogate marker
(insulin resistance) as an outcome measure in this trial.Despite the fact that there is a good relationshipbetween insulin resistance and cardiovascularhealth,54 55 this represent a limitation of the trial.However, this is a phase IIb trial, and thus a surrogatemarker as a primary outcome measure is justified,because a trial to show a reduction in cardiovascular endpoints will necessarily need to be large and would bereserved for a follow-on phase III design.
Author affiliations1Department of Molecular and Clinical Pharmacology, The Wolfson Centre forPersonalised Medicine, University of Liverpool, Liverpool, UK2MRC Centre for Drug Safety Science, University of Liverpool, Liverpool, UK3Department of Molecular and Clinical Pharmacology, University of Liverpool,Liverpool, UK4Clinical Trials Research Centre, University of Liverpool, Liverpool, UK5Department of Biostatistics, University of Liverpool, Liverpool, UK6Department of Diabetes and Endocrinology, The Royal Liverpool andBroadgreen University Hospitals NHS Trust, Liverpool, UK7Magnetic Resonance and Image Analysis Research Centre, University ofLiverpool, Liverpool, UK8Department of Mathematics and Statistics, Lancaster University, Lancaster,UK
Acknowledgements The authors thank the Principal Investigators andresearch team of this multicentre study who are ideally suited to conduct thisstudy due to their experience in the field of HIV and its management. Theauthors would also like to thank the members of the TSC and IDSMC for thetrial oversight they provide. Finally, the authors would like to thank all patientswho are part of the study so far for contributing to this study. List ofParticipating Centres: Prof Saye Khoo, The Royal Liverpool and BroadgreenUniversity Hospitals NHS Trust, Liverpool; Prof Margaret Johnson, Royal FreeLondon NHS Foundation Trust, London; Dr Barry Peters, Guy’s and StThomas’ NHS Foundation Trust, London; Dr Frank Post, King’s CollegeHospital NHS Foundation Trust, London; Dr Elbushra Herieka, The RoyalBournemouth and Christchurch Hospitals NHS Foundation Trust, Dorset;Dr Satyajit Das, Coventry and Warwickshire Partnership NHS Trust, Coventry;Dr Jane Minton, St James University Hospital, Leeds; Prof Clifford Leen,Western General Hospital, Edinburgh; Dr Duncan Churchill, Brighton andSussex University Hospitals NHS Trust, Brighton; Dr Fabiola Martin, YorClinic,York; Dr David Chadwick, The James Cook University Hospital,Middlesbrough; Dr Graeme Moyle, Chelsea and Westminster Hospital,St Stephens Aids Trust, London; Dr Fabiola Martin, Harrogate DistrictHospital, Harrogate; Dr Gabriel Schembri, Manchester Royal Infirmary,Manchester; Dr Jonathan Ainsworth, North Middlesex University Hospital NHSTrust, London; Dr Mark Gompels, Southmead Hospital, Bristol; Dr MasChaponda, St Helens Hospital, Merseyside; Dr David Loay, George EliotHospital NHS Trust, Nuneaton; Dr Mayur Chauhan, The Newcastle UponTyne Hospitals NHS Foundation Trust.
Contributors SPP, MP, SK, PW, RK-D, TJ, JW and JV were involved in thedesign of the study and preparation of the funding application. SPP, MP, SK,PW, RKD, TJ, JW, JV, GJK, MGF, CT and CS were involved in thedevelopment of protocol and protocol submission. SPP and MP undertookthe drafting of the manuscript. All authors have read the draft critically tomake contributions and approved the final text.
Funding This project (Ref: 10/60/37) is funded by the Efficacy andMechanism Evaluation (EME) Programme, an MRC and NIHR partnership. SPis funded by the Wellcome Trust Institutional Strategic Support Fund (ISSF).
Competing interests None declared.
Ethics approval The study, this protocol and related documents have beenapproved by the National Research Ethics Service Committee North West—Liverpool Central (Ref: 12/NW/0214).
Provenance and peer review Not commissioned; peer reviewed for ethicaland funding approval prior to submission.
Data sharing statement The findings from TAILoR will be disseminatedthrough peer-reviewed publications, at scientific conferences, the media andthrough patient and public involvement.
Open Access This is an Open Access article distributed in accordance withthe terms of the Creative Commons Attribution (CC BY 4.0) license, whichpermits others to distribute, remix, adapt and build upon this work, forcommercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
REFERENCES1. Lorenzo C, Williams K, Hunt KJ, et al. The National Cholesterol
Education Program—Adult Treatment Panel III, InternationalDiabetes Federation, and World Health Organization definitions ofthe metabolic syndrome as predictors of incident cardiovasculardisease and diabetes. Diabetes Care 2007;30:8–13.
2. Carr A, Emery S, Law M, et al. An objective case definition oflipodystrophy in HIV-infected adults: a case-control study. Lancet2003;361:726–35.
3. Potthoff A, Brockmeyer NH, Gelbrich G, et al. Lipodystrophy—a signfor metabolic syndrome in patients of the HIV-HEART study. J DtschDermatol Ges 2010;8:92–8.
4. Paula AA, Falcão MC, Pacheco AG. Metabolic syndrome inHIV-infected individuals: underlying mechanisms andepidemiological aspects. AIDS Res Ther 2013;10:32.
5. Worm SW, Friis-Møller N, Bruyand M, et al. High prevalence of themetabolic syndrome in HIV-infected patients: impact of differentdefinitions of the metabolic syndrome. AIDS 2010;24:427–35.
6. Brown TT, Cole SR, Li X, et al. Antiretroviral therapy and theprevalence and incidence of diabetes mellitus in the multicenterAIDS cohort study. Arch Intern Med 2005;165:1179–84.
7. De Wit S, Sabin CA, Weber R, et al. Incidence and risk factors fornew-onset diabetes in HIV-infected patients: the Data Collection onAdverse Events of Anti-HIV Drugs (D:A:D) study. Diabetes Care2008;31:1224–9.
8. Friis-Møller N, Reiss P, Sabin CA, et al. Class of antiretroviral drugsand the risk of myocardial infarction. N Engl J Med2007;356:1723–35.
9. Use of nucleoside reverse transcriptase inhibitors and risk ofmyocardial infarction in HIV-infected patients. AIDS 2008;22:F17–24.
10. Lo J, Abbara S, Shturman L, et al. Increased prevalence of subclinicalcoronary atherosclerosis detected by coronary computed tomographyangiography in HIV-infected men. AIDS 2010;24:243–53.
11. Samaras K. Prevalence and pathogenesis of diabetes mellitus inHIV-1 infection treated with combined antiretroviral therapy. J AcquirImmune Defic Syndr 2009;50:499–505.
12. Djedaini M, Peraldi P, Drici MD, et al. Lopinavir co-induces insulinresistance and ER stress in human adipocytes. Biochem BiophysRes Commun 2009;386:96–100.
13. Lee GA, Rao M, Mulligan K, et al. Effects of ritonavir and amprenaviron insulin sensitivity in healthy volunteers. AIDS 2007;21:2183–90.
14. Palacios R, Merchante N, Macias J, et al. Incidence of and riskfactors for insulin resistance in treatment-naive HIV-infected patients48 weeks after starting highly active antiretroviral therapy. AntivirTher 2006;11:529–35.
15. Bernal E, Masiá M, Padilla S, et al. Insulin resistance in HIV-infectedpatients receiving long-term therapy with efavirenz, lopinavir/ritonavirand atazanavir. Med Clin 2007;129:252–4.
16. Grunfeld C, Rimland D, Gibert CL, et al. Association of upper trunkand visceral adipose tissue volume with insulin resistance in controland HIV-infected subjects in the FRAM study. J Acquir ImmuneDefic Syndr 2007;46:283–90.
17. Jones SP, Janneh O, Back DJ, et al. Altered adipokine response inmurine 3T3-F442A adipocytes treated with protease inhibitors andnucleoside reverse transcriptase inhibitors. Antivir Ther2005;10:207–13.
18. Lagathu C, Bastard JP, Auclair M, et al. Antiretroviral drugs withadverse effects on adipocyte lipid metabolism and survival alter theexpression and secretion of proinflammatory cytokines andadiponectin in vitro. Antivir Ther 2004;9:911–20.
19. Benavides S, Nahata MC. Pharmacologic therapy for HIV-associatedlipodystrophy. Ann Pharmacother 2004;38:448–57.
Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566 11
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from

20. McGoldrick C, Leen CL. The management of dyslipidaemias inantiretroviral-treated HIV infection: a systematic review. HIV Med2007;8:325–34.
21. Nissen SE, Wolski K. Effect of rosiglitazone on the risk of myocardialinfarction and death from cardiovascular causes. N Engl J Med2007;356:2457–71.
22. Sheth SH, Larson RJ. The efficacy and safety of insulin-sensitizingdrugs in HIV-associated lipodystrophy syndrome: a meta-analysis ofrandomized trials. BMC Infect Dis 2010;10:183.
23. Benndorf RA, Rudolph T, Appel D, et al. Telmisartan improvesinsulin sensitivity in nondiabetic patients with essential hypertension.Metab Clin Exp 2006;55:1159–64.
24. Younis F, Stern N, Limor R, et al. Telmisartan ameliorateshyperglycemia and metabolic profile in nonobese Cohen-Rosenthaldiabetic hypertensive rats via peroxisome proliferator activatorreceptor-gamma activation. Metab Clin Exp 2010;59:1200–9.
25. Foryst-Ludwig A, Hartge M, Clemenz M, et al. PPARgammaactivation attenuates T-lymphocyte-dependent inflammation ofadipose tissue and development of insulin resistance in obese mice.Cardiovas Diabetol 2010;9:64.
26. Souza-Mello V, Gregório BM, Cardoso-de-Lemos FS, et al.Comparative effects of telmisartan, sitagliptin and metformin alone orin combination on obesity, insulin resistance, and liver and pancreasremodelling in C57BL/6 mice fed on a very high-fat diet. Clin Sci2010;119:239–50.
27. Derosa G, Fogari E, D’Angelo A, et al. Metabolic effects oftelmisartan and irbesartan in type 2 diabetic patients with metabolicsyndrome treated with rosiglitazone. J Clin Pharm Ther2007;32:261–8.
28. Makita S, Abiko A, Naganuma Y, et al. Effects of telmisartan onadiponectin levels and body weight in hypertensive patients withglucose intolerance. Metab Clin Exp 2008;57:1473–8.
29. Georgescu EF, Ionescu R, Niculescu M, et al. Angiotensin-receptorblockers as therapy for mild-to-moderate hypertension-associatednon-alcoholic steatohepatitis. World J Gastroenterol2009;15:942–54.
30. Rizos CV, Milionis HJ, Kostapanos MS, et al. Effects of rosuvastatincombined with olmesartan, irbesartan, or telmisartan on indices ofglucose metabolism in Greek adults with impaired fasting glucose,hypertension, and mixed hyperlipidemia: a 24-week, randomized,open-label, prospective study. Clin Ther 2010;32:492–505.
31. Chujo D, Yagi K, Asano A, et al. Telmisartan treatment decreasesvisceral fat accumulation and improves serum levels of adiponectinand vascular inflammation markers in Japanese hypertensivepatients. Hypertens Res 2007;30:1205–10.
32. Shimabukuro M, Tanaka H, Shimabukuro T. Effects of telmisartanon fat distribution in individuals with the metabolic syndrome.J Hypertens 2007;25:841–8.
33. Yusuf S, Teo KK, Pogue J, et al. Telmisartan, ramipril, or both inpatients at high risk for vascular events. N Engl J Med2008;358:1547–59.
34. Boccara F, Auclair M, Cohen A, et al. HIV protease inhibitors activatethe adipocyte renin angiotensin system. Antivir Ther 2010;15:363–75.
35. Singh B, Saxena A. Surrogate markers of insulin resistance:a review. World J Diabetes 2010;1:36–47.
36. Takagi H, Umemoto T. Telmisartan improves insulin sensitivity:a meta-analysis of randomized head-to-head trials. Int J Cardiol2012;156:92–6.
37. Ucciferri C, Falasca K, Mancino P, et al. Microalbuminuria andhypertension in HIV-infected patients: a preliminary study oftelmisartan. Eur Rev Med Pharmacol Sci 2012;16:491–8.
38. Thomas EL, Hamilton G, Patel N, et al. Hepatic triglyceride contentand its relation to body adiposity: a magnetic resonance imaging andproton magnetic resonance spectroscopy study. Gut 2005;54:122–7.
39. Rico-Sanz J, Thomas EL, Jenkinson G, et al. Diversity in levels ofintracellular total creatine and triglycerides in human skeletalmuscles observed by (1)H-MRS. J Appl Physiol 1999;87:2068–72.
40. Dunnett C. Selection of the best treatment in comparison to a controlwith an application to a medical trial. In: Santer T, Tamhane AC,eds. Design of experiments: ranking and selection. New York:Marcel Dekker, 1984:47–66.
41. Magirr D, Jaki T, Whitehead J. A generalized Dunnett test formulti-arm multistage clinical studies with treatment selection.Biometrika 2012;99:494–501.
42. Whitehead J, Jaki T. One- and two-stage design proposals for aphase II trial comparing three active treatments with control using anordered categorical endpoint. Stat Med 2009;28:828–47.
43. Henderson R, Diggle P, Dobson A. Joint modelling of longitudinalmeasurements and event time data. Biostatistics 2000;1:465–80.
44. Williamson PR, Kolamunnage-Dona R, Philipson P, et al. Jointmodelling of longitudinal and competing risks data. Stat Med2008;27:6426–38.
45. Emsley R, Dunn G, White IR. Mediation and moderation of treatmenteffects in randomised controlled trials of complex interventions. StatMethods Med Res 2010;19:237–70.
46. NIH. Division of AIDS Table for Grading the Severity of Adult andPediatric Adverse Events, Version 1.0 December, 2004; ClarificationAugust 2009. 2004.
47. Stangier J, Su CA, Roth W. Pharmacokinetics of orally andintravenously administered telmisartan in healthy young and elderlyvolunteers and in hypertensive patients. J Int Med Res2000;28:149–67.
48. Stangier J, Su CA, Schondorfer G, et al. Pharmacokinetics andsafety of intravenous and oral telmisartan 20 mg and 120 mg insubjects with hepatic impairment compared with healthy volunteers.J Clin Pharmacol 2000;40(12 Pt 1):1355–64.
49. Depart of Health MRC, Medicines and Healthcare ProductsRegulatory Agency Clinical Trials Working Group. 2011. Risk_adapted_approaches_to_the_management_of_clinical_trials_of_investigational_medicinal_products.pdf
50. Araujo S, Bañón S, Machuca I, et al. Prevalence of insulin resistanceand risk of diabetes mellitus in HIV-infected patients receiving currentantiretroviral drugs. Eur J Endocrinol 2014;171:545–54.
51. Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection asa chronic disease. Lancet 2013;382:1525–33.
52. Vecchiet J, Ucciferri C, Falasca K, et al. Antihypertensive andmetabolic effects of telmisartan in hypertensive HIV-positivepatients. Antivir Ther 2011;16:639–45.
53. Lake JE, Tseng CH, Currier JS. A pilot study of telmisartan for visceraladiposity in HIV infection: the metabolic abnormalities, telmisartan, andHIV infection (MATH) trial. PLoS ONE 2013;8:e58135.
54. Ginsberg HN. Insulin resistance and cardiovascular disease. J ClinInvest 2000;106:453–8.
55. Laakso M, Kuusisto J. Insulin resistance and hyperglycaemia incardiovascular disease development. Nat Rev Endocrinol2014;10:293–302.
12 Pushpakom SP, et al. BMJ Open 2015;5:e009566. doi:10.1136/bmjopen-2015-009566
Open Access
on March 21, 2022 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-009566 on 15 O
ctober 2015. Dow
nloaded from