OPEN ACCESS Case Report A Case ... - ECronicon Open Access“A Case Report of Double Penetrating...
4
Cronicon OPEN ACCESS EC OPHTHALMOLOGY EC OPHTHALMOLOGY Case Report A Case Report of Double Penetrating Ocular Injury Marsida Krasniqi* Department of Medicine, University Aleksander Moisiu, Durres, Albania Citation: Marsida Krasniqi. “A Case Report of Double Penetrating Ocular Injury”. EC Ophthalmology 11.5 (2020): 47-50. *Corresponding Author: Marsida Krasniqi, Department of Medicine, University Aleksander Moisiu, Durres, Albania. Received: March 29, 2020; Published: April 24, 2020 Abstract Keywords: Double-Penetrating Eye Injury; Open Globe; Foreign Bodies; Vitrectomy Ocular trauma with open globe injury is the most common ophthalmic emergency. Patients with open globe injury and with an intraorbital foreign body, make the prognosis poor for visual acuity. This is a case report of a 38 years old male with a double pen- etrating ocular injury with a shotgun. The scleral wound was repaired in another clinic, 8 hours after the trauma. The patient came to our clinic, 7 days after the trauma. The skull roentgenograms demonstrated multiple metallic fragments in the subcutaneous tissue of the face and orbits. CT scan shows a 0.4 mm metallic foreign body on the nasal lower orbit. A double penetrating eye injury was impressed, and the patient was vitrectomized immediately. The exit wound was at the corresponding location of the entrance wound, compatible with the diagnosis of perforating globe injury. During vitrectomy, iatrogenic posterior vitreous detachment was induced from disc margin and the adherent cortical vitreous was carefully separated from the exit wound. Intraocular laser photocoagulation around the retinal hole at the exit wound and cryopexy over the entrance wound were applied. The patient’s BCVA recovered to 2/10 three weeks postoperatively, and 3/10 at 10- month follow-up. Introduction One of the most causes of blindness and visual loss is ocular trauma with open globe and intraocular foreign body [1,2]. According to the US Eye Injury Database and pellet guns account for nearly 6% of all ocular injuries and they still remain the most frequent gun injuries in the emergency setting [3]. Other articles have reported the severity of trauma in the visual outcome after the eye repair [2,4,5]. The poor prognosis depends on the time of foreign body removal and by the surgical techniques [6,7]. In our case report we report the visual outcome of a double penetrating eye injury with intraocular foreign body. Case Report Mr. Alban was first examined at International eye clinic on 11/03/2019 with chief complaint of loss of vision in the right eye following injury with a shotgun 7 days back. Emergent treatment and primary sclera wound repair were done elsewhere about 8 hours after trauma. On examination here, his best-corrected visual acuity was perception of light with accurate projection of rays in the right eye and 10/10 in the left eye. Intraocular pressure with applanation tonometer was 07 mmHg in the right eye and 15 mmHg in the left eye. Exami- nation of the anterior segment was done with slit lamp. In the slit lamp the right eye showed repaired sclera wound at 7o clock position about 2 mm posterior to the limbus. In the anterior chamber a 2 mm hyphemia and an early sunflower cataract was notice.
Transcript of OPEN ACCESS Case Report A Case ... - ECronicon Open Access“A Case Report of Double Penetrating...

CroniconO P E N A C C E S S EC OPHTHALMOLOGYEC OPHTHALMOLOGY
Case Report
A Case Report of Double Penetrating Ocular Injury
Marsida Krasniqi*
Department of Medicine, University Aleksander Moisiu, Durres, Albania
Citation: Marsida Krasniqi. “A Case Report of Double Penetrating Ocular Injury”. EC Ophthalmology 11.5 (2020): 47-50.
*Corresponding Author: Marsida Krasniqi, Department of Medicine, University Aleksander Moisiu, Durres, Albania.
Received: March 29, 2020; Published: April 24, 2020
Abstract
Keywords: Double-Penetrating Eye Injury; Open Globe; Foreign Bodies; Vitrectomy
Ocular trauma with open globe injury is the most common ophthalmic emergency. Patients with open globe injury and with an intraorbital foreign body, make the prognosis poor for visual acuity. This is a case report of a 38 years old male with a double pen-etrating ocular injury with a shotgun. The scleral wound was repaired in another clinic, 8 hours after the trauma. The patient came to our clinic, 7 days after the trauma. The skull roentgenograms demonstrated multiple metallic fragments in the subcutaneous tissue of the face and orbits. CT scan shows a 0.4 mm metallic foreign body on the nasal lower orbit. A double penetrating eye injury was impressed, and the patient was vitrectomized immediately. The exit wound was at the corresponding location of the entrance wound, compatible with the diagnosis of perforating globe injury. During vitrectomy, iatrogenic posterior vitreous detachment was induced from disc margin and the adherent cortical vitreous was carefully separated from the exit wound. Intraocular laser photocoagulation around the retinal hole at the exit wound and cryopexy over the entrance wound were applied. The patient’s BCVA recovered to 2/10 three weeks postoperatively, and 3/10 at 10- month follow-up.
Introduction
One of the most causes of blindness and visual loss is ocular trauma with open globe and intraocular foreign body [1,2]. According to the US Eye Injury Database and pellet guns account for nearly 6% of all ocular injuries and they still remain the most frequent gun injuries in the emergency setting [3]. Other articles have reported the severity of trauma in the visual outcome after the eye repair [2,4,5]. The poor prognosis depends on the time of foreign body removal and by the surgical techniques [6,7]. In our case report we report the visual outcome of a double penetrating eye injury with intraocular foreign body.
Case Report
Mr. Alban was first examined at International eye clinic on 11/03/2019 with chief complaint of loss of vision in the right eye following injury with a shotgun 7 days back. Emergent treatment and primary sclera wound repair were done elsewhere about 8 hours after trauma.
On examination here, his best-corrected visual acuity was perception of light with accurate projection of rays in the right eye and 10/10 in the left eye. Intraocular pressure with applanation tonometer was 07 mmHg in the right eye and 15 mmHg in the left eye. Exami-nation of the anterior segment was done with slit lamp. In the slit lamp the right eye showed repaired sclera wound at 7o clock position about 2 mm posterior to the limbus. In the anterior chamber a 2 mm hyphemia and an early sunflower cataract was notice.

48
Citation: Marsida Krasniqi. “A Case Report of Double Penetrating Ocular Injury”. EC Ophthalmology 11.5 (2020): 47-50.
A Case Report of Double Penetrating Ocular Injury
The posterior segment was exanimated with indirect ophthalmoscope, which revealed hazy media in the right eye due to vitreous hemorrhage. Fundus examination for the left eye revealed normal optic nerve head and normal macular region.
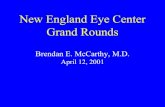
Skull roentgenograms demonstrated multiple metallic fragments in the subcutaneous tissue of the face and orbits (Figure 1).
Figure 1
Orbital computed tomography (CT) scan revealed high-density foreign body on the posterior nasal upper orbit (Figure 2). Skull X-ray confirmed one 0.4 mm metallic foreign body on the nasal lower orbit.
Figure 2

49
Citation: Marsida Krasniqi. “A Case Report of Double Penetrating Ocular Injury”. EC Ophthalmology 11.5 (2020): 47-50.
A Case Report of Double Penetrating Ocular Injury
B-scan sonography revealed several high-density signals (vitreous opacity) without acoustic shadow in the right eye.
Double penetrating ocular injury with retained intraorbital foreign body in the right eye was impressed and immediate vitrectomy was performed.
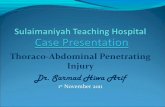
Intra-operatively, there was dense vitreous and pre-retinal hemorrhage (Figure 3).
Figure 3
The full-thickness scleral exit wound surrounded by avulsed retina hole margin superior and nasal to the optic disc was also noted. The exit wound was at the corresponding location of the entrance wound, compatible with the diagnosis of perforating globe injury. Dur-ing vitrectomy, iatrogenic posterior vitreous detachment was induced from disc margin and the adherent cortical vitreous was carefully separated from the exit wound. Intraocular laser photocoagulation around the retinal hole at the exit wound (Figure 4) and cryopexy over the entrance wound were applied. Intravitreal injection of antibiotics (vancomycin 1 mg/0.1 mL and ceftazidime 2 mg/0.1 mL) was performed after collecting vitreous specimens for microorganism culture.
Figure 4
The patient’s BCVA recovered to 2/10 three weeks postoperatively, and 3/10 at 10- month follow-up.

50
Citation: Marsida Krasniqi. “A Case Report of Double Penetrating Ocular Injury”. EC Ophthalmology 11.5 (2020): 47-50.
A Case Report of Double Penetrating Ocular Injury
Discussion
We present a case of intraorbital foreign body in a double penetrating eye injury. The prognosis was poor due to time removal of the foreign body.
Vitrectomy in a case of intraorbital foreign body with double penetrating globe injury is complicated due to associated high risk of orbital inflammation and complication [8]. Metallic foreign body can be detected by orbital CT. Location, size, chemical structure, and the complications caused by foreign body influence the decision to remove it [9]. Different articles has shown the use of transcranial approach in removing an intraorbital foreign body [10] but this calls for neurosurgical competence and increases risk of intracranial complications. In our case, we performed a transconjuctival approach to removal the intraorbital foreign body. The conjunctiva was incised along limbus. The patient’s BCVA recovered to 2/10 three weeks postoperatively, and 3/10 at 10- month follow-up. The patient had a good cosmetic appearance, normal IOP.
Conclusion
As a conclusion we can say that the time of removal of foreign body and the surgical approach influence in visual acuity. In our case we use a transconjuctival approach to remove the intraorbital foreign body. The patient’s best correction visual acuity was 3/10 at 10-month follow-up.
Bibliography
1. Odebode TO., et al. “Ocular and visual complications of head injury”. Eye 19.5 (2005): 561-566.
2. Rahman I., et al. “Open globe injuries: Factors predictive of poor outcome”. Eye 20.12 (2006): 1336-1341.
3. Kuhn F., et al. “Epidemiology of blinding trauma in the United States Eye Injury Registry”. Ophthalmic Epidemiology 13.3 (2006): 209-216.
4. Ben Simon GJ., et al. “Gunshot wound to the eye and orbit: A descriptive case series and literature review”. Journal of Trauma - Injury, Infection and Critical Care 71.3 (2011): 771-778.
5. Isaac DLC., et al. “Prognostic factors in open globe injuries”. Ophthalmologica 217.6 (2003): 431-435.
6. Schmidt GW., et al. “Vision Survival after Open Globe Injury Predicted by Classification and Regression Tree Analysis”. Ophthalmology 115.1 (2008): 202-209.
7. Fujikawa A., et al. “Visual outcomes and prognostic factors in open-globe injuries”. BMC Ophthalmology 18.1 (2018): 138.
8. Page RD., et al. “Risk factors for poor outcomes in patients with open-globe injuries”. Clinical Ophthalmology 10 (2016): 1461-1466.
9. Pinto A., et al. “Role of Computed Tomography in the Assessment of Intraorbital Foreign Bodies”. Seminars in Ultrasound, CT and MRI 33.5 (2012): 392-395.
10. Yeh S., et al. “Current trends in the management of intraocular foreign bodies”. Current Opinion in Ophthalmology 19.3 (2008): 225-233.
Volume 11 Issue 5 May 2020© All rights reserved by Marsida Krasniqi.