One way to prepare
62
Transcript of One way to prepare

• Requires some basic knowledge of clinical examinations
• Clinical examination station (OSCE)• One way to prepare: ‘Retrospective approach’• Cardiovascular examination: 2 cases• Respiratory examination: 2 cases
• Duration: 70 mins• Slides and recordings: www.bitemedicine.com/watch
• Other common OSCE cases available in previous and upcoming webinars• Aim of the week is to cover most of the common scenarios
2
Aims and Objectives

3
Clinical examination station: how to prepare?
EXAMINATION ROUTINE
PRESENTATION
VIVA
• Perform each step of the routine confidently
• Pick up on signs
• Present findings systematically
• List appropriate differentials based on findings
• Answer questions systematically
• Explain your thinking
‘Retrospective approach’1. Formulate an OSCE Cases List
2. Prepare your ‘VIVA’ for those cases• Positive signs of diagnosis• ‘Typical’ findings presentation• Risk factors• Signs of decompensation• List of differentials• Complications• How would you investigate this patient?• How would you manage this patient?

4
Clinical examination station: how to prepare?‘Retrospective approach’3. Finalise your examination routine
• Each step of the routine• Signs you are looking for• Your speech
4. Practice your examination routineon friends
5. Go to the wards/clinics looking foryour cases
EXAMINATION ROUTINE
PRESENTATION
VIVA
• Perform each step of the routine confidently
• Pick up on signs
• Present findings systematically
• List appropriate differentials based on findings
• Answer questions systematically
• Explain your thinking

What cases could come up?1. Mitral regurgitation2. Aortic stenosis3. Prosthetic heart valves: aortic, mitral or both4. Stable chronic heart failure5. Ischaemic heart disease: CABG scars
This is not a definitive list• But by preparing for these you will be better at:
• Your exam routine• Looking out for important signs• Formulating your findings systematically• Tackling the VIVA
5
Cardiovascular examination: OSCE Cases list

I performed a cardiovascular examination on this patient• Who has signs suggestive of mitral regurgitation
My main positive findings are:1. XXX2. YYY
My relevant negative findings are:1. XXX (Risk factors)2. YYY (Signs of decompensation)3. ZZZ (POSSIBLE associated features)
Overall, this points towards a diagnosis of mitral regurgitation withno signs of decompensation
6
How to present your findings?
If you have an idea, then back yourself from the start. It gets the examiner listening
RELEVANT negatives
99% of the time your patient will be STABLE

Peripheral
Pulse• Irregularly irregular
7
Cardiovascular examination: Case 1
Central
Auscultation• Pansystolic murmur
• Loudest at the mitral region• Exacerbated on patient lying on
their L side and on held expiration• Radiation to axilla

8
Question 1

9
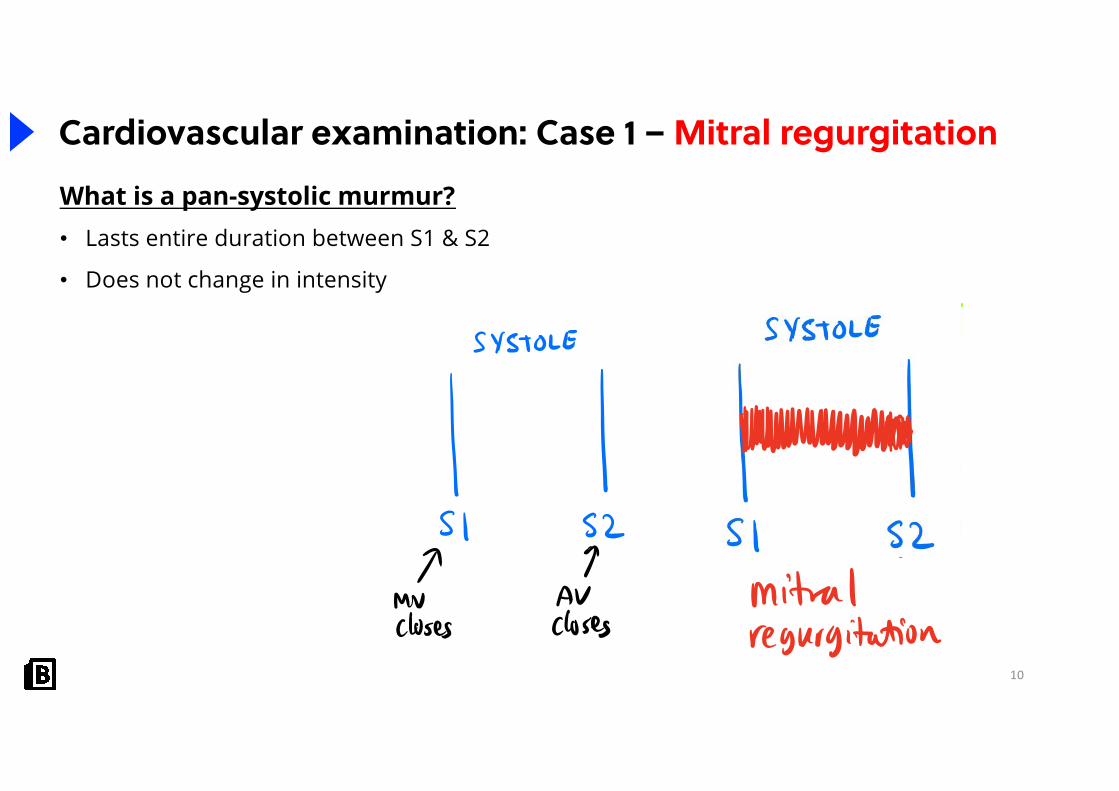
Cardiovascular examination: Case 1 – Mitral regurgitationWhat is a pan-systolic murmur?• Lasts entire duration between S1 & S2
• Does not change in intensity
10
Cardiovascular examination: Case 1 – Mitral regurgitationWhat is a pan-systolic murmur?• Lasts entire duration between S1 & S2
• Does not change in intensity

11
Cardiovascular examination: Case 1 – Mitral regurgitationWhy is mitral regurgitation associated with an irregularly irregular pulse?• Mitral regurgitation = MV valve doesn't close
properly
(1)
12
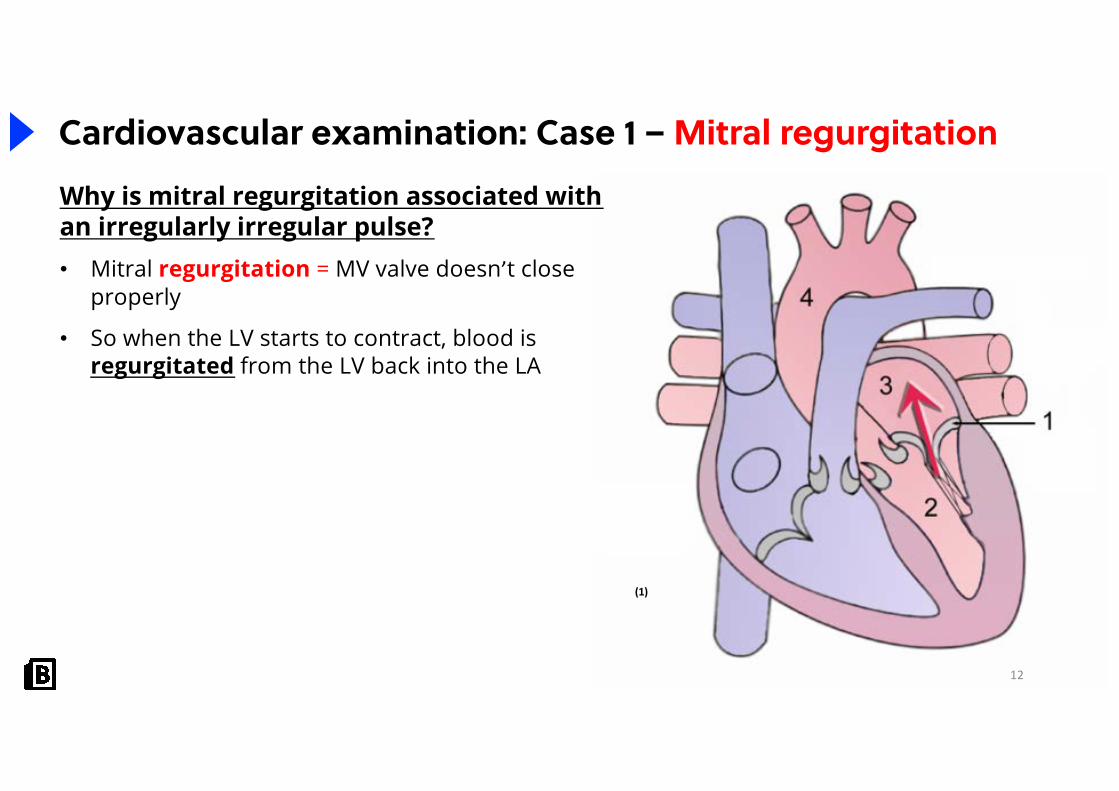
Cardiovascular examination: Case 1 – Mitral regurgitationWhy is mitral regurgitation associated with an irregularly irregular pulse?• Mitral regurgitation = MV valve doesn’t close
properly
• So when the LV starts to contract, blood is regurgitated from the LV back into the LA
(1)

13
Cardiovascular examination: Case 1 – Mitral regurgitationWhy is mitral regurgitation associated with an irregularly irregular pulse?• Mitral regurgitation = MV valve doesn’t close
properly
• So when the LV starts to contract, some blood is regurgitated from the LV back into the LA
• Over time, LA becomes dilated
(1)
14
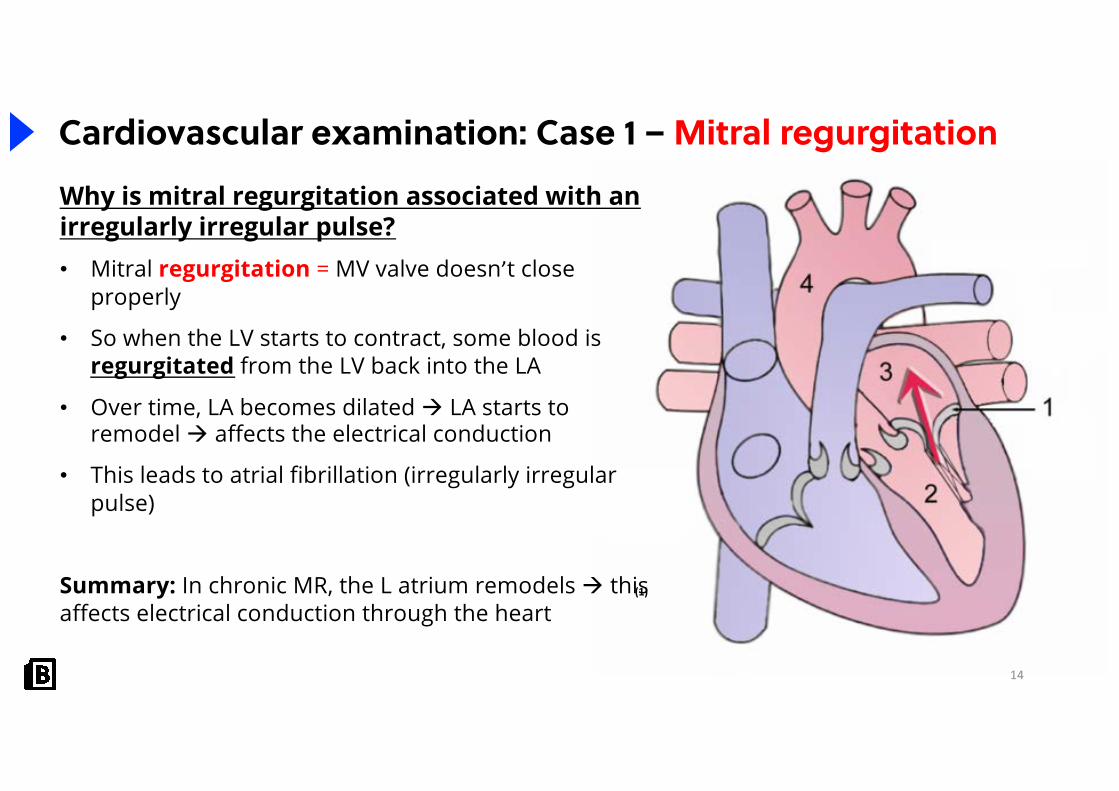
Cardiovascular examination: Case 1 – Mitral regurgitationWhy is mitral regurgitation associated with an irregularly irregular pulse?• Mitral regurgitation = MV valve doesn’t close
properly
• So when the LV starts to contract, some blood is regurgitated from the LV back into the LA
• Over time, LA becomes dilated à LA starts to remodel à affects the electrical conduction
• This leads to atrial fibrillation (irregularly irregular pulse)
Summary: In chronic MR, the L atrium remodels à this affects electrical conduction through the heart
(1)

15
Cardiovascular examination: Case 1 – Mitral regurgitationPlease present your findings?
I performed a cardiovascular examination on this patient who has signs suggestive of MITRAL REGURIGTATION
My main positive findings are:
• I palpated an irregularly, irregular pulse, suggestive of atrial fibrillation
• On auscultation, I could hear normal 1st & 2nd heart sounds with a systolic murmur between S1 & S2
• The systolic murmur was:
• Character: pansystolic
• Region: loudest over the mitral region
• Augmentation: end-expiration with the patient lying on their left side
• Radiation: axilla
16
Cardiovascular examination: Case 1 – Mitral regurgitationPlease present your findings?
My relevant negative findings are:
• No signs of vascular risk factors e.g. tar staining, tendon xanthomata
• No peripheral stigmata of infective endocarditis
• No scars to suggest coronary artery bypass graft or valve replacement
• No signs of decompensation e.g. pulmonary or peripheral oedema
This points towards a diagnosis of grade 3 mitral regurgitation complicated by atrial fibrillation

17
Cardiovascular examination: Case 1 – Mitral regurgitationWhat are your differentials?1. Mitral regurgitation
2. Aortic stenosis • Ejection systolic murmur with radiation to carotids
3. Tricuspid regurgitation• Pansystolic murmur
• Heard loudest over lower L sternal edge• Augmented on held INSPIRATION• No radiation • Rarer
Acute ChronicInfective endocarditis Ischaemic injury to L ventricle à dilated MV
annulus
Rupture of papillary muscle (e.g. post MI) Calcification of MV annulus
Rheumatic heart disease

18
Cardiovascular examination: Case 1 – Mitral RegurgitationWhat are possible complications of mitral regurgitation
Complications from the valve• Infective endocarditis
Complications from impaired outflow• Left ventricular failure • Atrial fibrillation

19
Cardiovascular examination: Case 1 – Mitral regurgitationHow would you investigate this patient?
Bedside• Basics observations: HR, BP, RR, SpO2• Urine dip: glycosuria for diabetes• ECG:
• AF• P-mitrale (broad, notched P waves): sign of dilated LA
Bloods• Inflammatory markers: CRP and ESR for infective
endocarditis• BNP: raised if associated heart failure
(2)

20
Cardiovascular examination: Case 1 – Mitral regurgitationHow would you investigate this patient?
Imaging• CXR
• L atrial enlargement• Signs of heart failure (ABCDE)
• ECHO: gold standard test to diagnose & assess severity• Severe: Jet width > 0.7cm, regurgitant volume >
60mls
Special• Coronary angiography: measure gradient across valve
and assess for concomitant coronary artery disease(3)

21
Cardiovascular examination: Case 1 – Mitral regurgitationHow would you manage this patient?
Conservative• Improve cardiovascular risk factors e.g. smoking cessation
Medical
• Anticoagulation for AF
• Manage heart failure if present
• ACEi, beta-blockers, diuretics
Surgical
• Valve repair or replacement indicated if:
• Symptomatic
• Severe LV dilation
• Significantly reduced LVEF
• New-onset AF
22
Grading murmursFreeman & Levine Grading for heart murmurs
• Grade 1: Faintest murmur• Grade 2: Faint murmur• Grade 3: Loud murmur, no thrill• Grade 4: Loud murmur + palpable thrill• Grade 5: Murmur heard with stethoscope partially on chest + thrill• Grade 6: Murmur heard with stethoscope held off chest
Peripheral
23
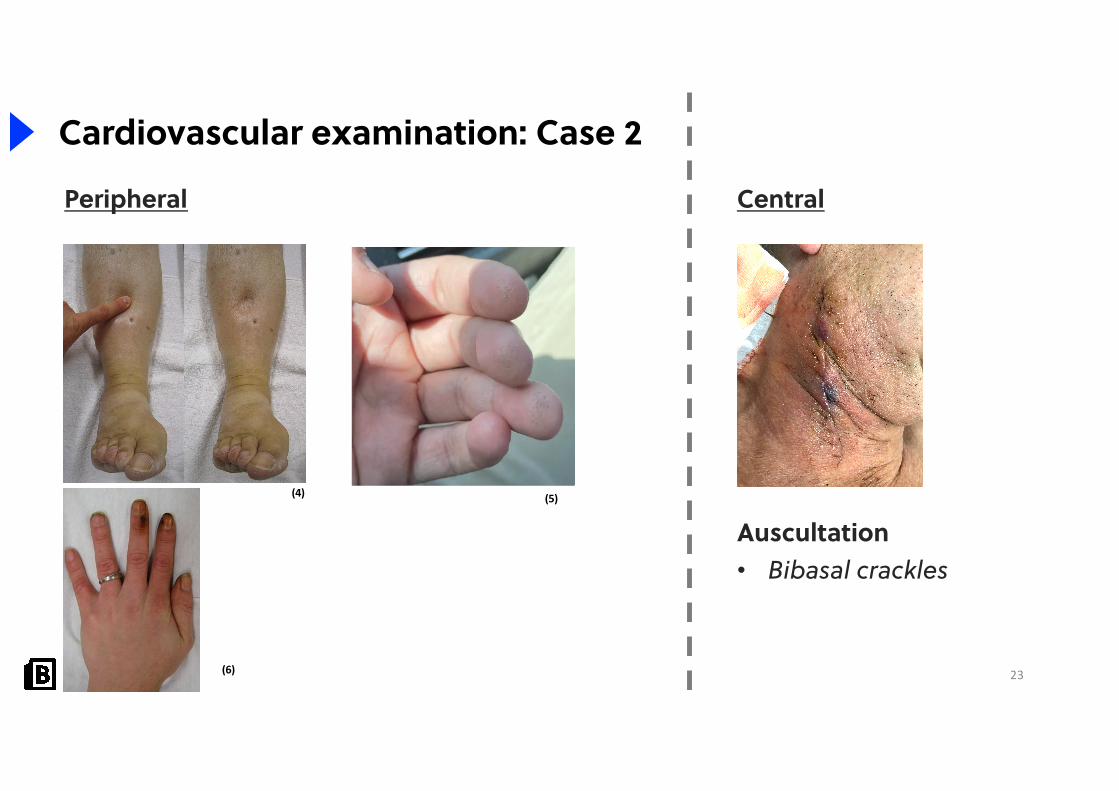
Cardiovascular examination: Case 2
Central
Auscultation• Bibasal crackles
(4) (5)
(6)
24
Question 2

25
Cardiovascular examination: Case 2 – Congestive cardiac failurePlease present your findings?
I performed a cardiovascular examination on this patient who has signs suggestive of CHRONIC HEART FAILURE
My main positive findings are:
• Tar staining • Finger prick marks suggesting blood glucose monitoring• Peripheral oedema up to knees• I also noticed a vertical 6cm scar on the neck along the distribution of the carotid artery
suggestive of a carotid endarterectomy scar• On auscultation of the lung bases: bibasal crackles

26
Cardiovascular examination: Case 2 – Congestive cardiac failurePlease present your findings?
My relevant negative findings are:• No scars to suggest coronary artery bypass graft or valve replacement• Normal heart sounds, with no added sounds or murmurs• No peripheral stigmata of infective endocarditis
This points towards congestive cardiac failure• The presence of both pulmonary and peripheral oedema suggests an element of
decompensation

27
Cardiovascular examination: Case 2 – Congestive cardiac failureWhat are the possible causes of heart failure?
• Heart failure is defined as inadequate cardiac output for the body’s requirements
• Can be classified as L or R sided heart failure
Left sided Right sided Ischaemic heart disease Left sided heart failure
Valvular disease• Mitral• Aortic
Valvular disease• Tricuspid• Pulmonary
Cor pulmonale • COPD• Fibrosis • PE• Obstructive sleep apnoea
28
Cardiovascular examination: Case 2 – Congestive cardiac failureHow would you investigate this patient?
Bedside• Basics observations: HR, BP, RR, SpO2• ECG: L ventricular strain (LBBB and large amplitude QRS) or R ventricular
strain (RBBB and right axis)
Bloods• FBC: anaemia (causes or exacerbates heart failure)• BNP or NT-pro BNP• U&Es: renal function can be deranged in heart failure (cardiorenal
syndrome)• Screen for risk factors: diabetes, lipids

29
Cardiovascular examination: Case 2 – Congestive cardiac failureHow would you investigate this patient?
Imaging• CXR
• ABCDE signs of heart failure• ECHO: gold standard test to diagnose & assess severity
• Assess left ventricular ejection fraction
(3)

30
Cardiovascular examination: Case 2 – Congestive cardiac failureHow would manage CCF? MDT approach: GP, heart failure team (cardiologist, specialist nurses), occupational therpaist
Conservative• Stop smoking and diabetes control • Healthy diet and consider fluid restriction • Regular exercise
Medical• 1st line: Beta blocker and ACEi
• Add furosemide if evidence of fluid overload, as is the case here • 2nd line: add in aldosterone antagonist • 3rd line: consider cardiac resynchronisation therapy or implantable cardiac defibrillator
Surgery• Heart transplant • Left ventricular assist device
• Given to patients unlikely to survive until heart donor becomes available

31
Cardiovascular examination: Case 2 – Congestive cardiac failureNew York Classification of heart failure
Grading SymptomsGrade 1 No SOB
Grade 2 SOB with exertion• Slight limitation of physical activity
Grade 3 SOB with exertion• Marked limitation of physical activity • Mild activity causes symptoms
Grade 4 SOB at rest

What cases could come up?
1. Surgical: Lobectomy/Pneumonectomy
2. Pulmonary fibrosis
3. Bronchiectasis
4. COPD
5. Pleural effusion
6. Lung malignancy
32
Respiratory examination: OSCE Cases list

Peripheral
33
Respiratory examination: Case 1
Central
End of the bed:• Audible wet cough from the end of
the bed
Auscultation:• Coarse crackles which change on
coughing• Occasional wheeze
(7)
(8)

34
Question 3

35
Respiratory examination: Case 1 – Bronchiectasis
Please present your findings?
I performed a respiratory examination on this gentleman who has signs of BRONCHIECTASIS
My main positive findings are:• Audible productive cough • Long acting anti-muscarinic inhaler at the bedside• Digital clubbing• On auscultation:
• Coarse crepitation's that altered on coughing

36
Respiratory examination: Case 1 – BronchiectasisPlease present your findings?
My relevant negative findings are:• Reassuringly, not requiring oxygen currently• No CO2 retention flap • No signs of decompensation (e.g. cor pulmonale – raised JVP and peripheral oedema)
This points towards a diagnosis of bronchiectasis
• The patient displayed no evident signs of an underlying cause e.g. rheumatoid arthritis
• The commonest causes of bronchiectasis are idiopathic and post-infection, which I suspect may well be the case in this patient

37
Respiratory examination: Case 1 – Bronchiectasis
(9)

38
Question 4

39
Respiratory examination: Case 1 – Bronchiectasis What are the possible causes of bronchiectasis
Cause ExamplesCongenital Cystic fibrosis
Kartgener’s syndromePrimary ciliary dyskinesia Yellow nail syndrome
Post-infection MeaslesTBAspiration
Immunological dysfunction Rheumatoid arthritis Inflammatory bowel diseaseABPAHypogammaglobulinemia

40
Respiratory examination: Case 1 – BronchiectasisWhat are the differentials?
• Bronchiectasis: think of possible causes• Fibrosis
Bronchiectasis FibrosisProductive cough (Sputum pot) Dry cough
Coarse crackles which change on coughing
Fine end-inspiratory crackles
41
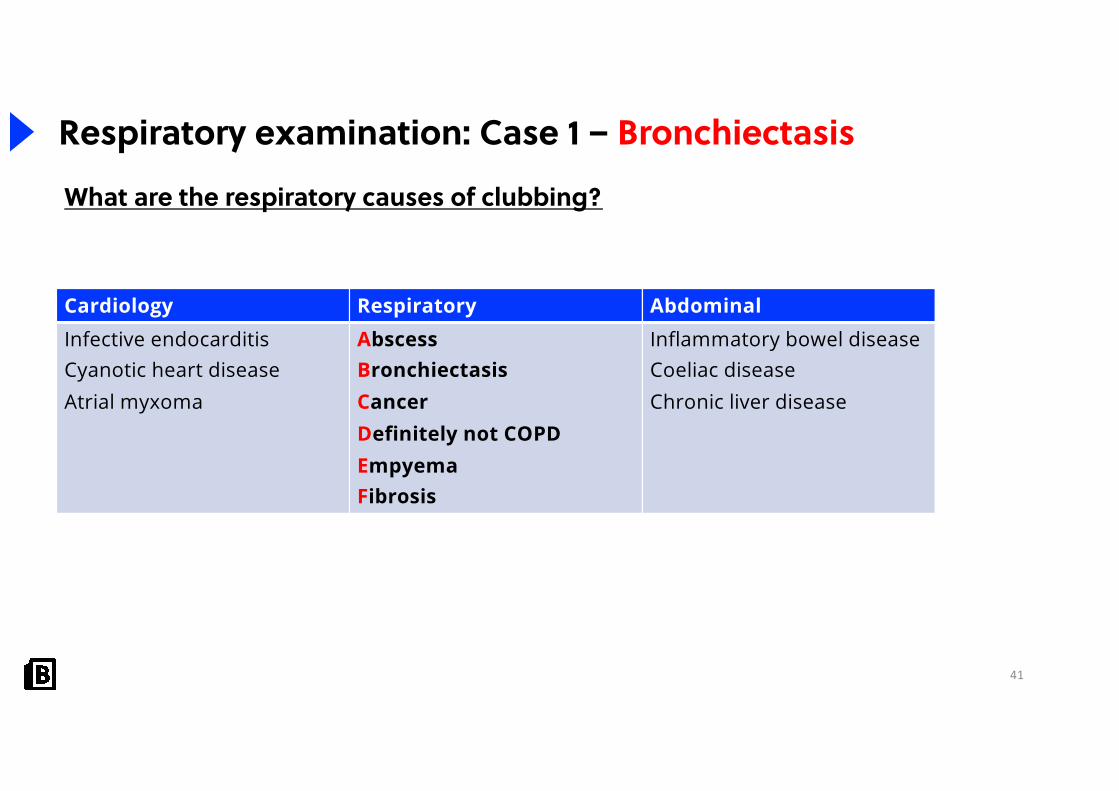
Respiratory examination: Case 1 – Bronchiectasis
Cardiology Respiratory Abdominal Infective endocarditisCyanotic heart diseaseAtrial myxoma
AbscessBronchiectasisCancerDefinitely not COPDEmpyemaFibrosis
Inflammatory bowel diseaseCoeliac diseaseChronic liver disease
What are the respiratory causes of clubbing?

42
Respiratory examination: Case 1 – BronchiectasisHow would you investigate this patient?
Bedside• Basic obs: HR, BP, RR, SpO2
• Sputum MCS: screen for infection or colonisation
• H.influenzae and P.aeruginosa
Bloods
• FBC and CRP: evidence of infection
• ABG: respiratory failure

43
Respiratory examination: Case 1 – BronchiectasisHow would you investigate this patient?
Imaging • CXR: tramlines and ring shadows
• CT thorax: signet ring sign
Special tests
• Spirometry: obstructive pattern with FEV1/FVC < 0.7
• Screen for underlying aetiology: RF, immunoglobulins, sweat test
Restrictive Obstructive
FEV1 or ↓ ↓
FVC ↓
FEV1/FVC >70% <70%

44
Respiratory examination: Case 1 – Bronchiectasis
(10)

45
Respiratory examination: Case 1 – Bronchiectasis
(11)

46
Respiratory examination: Case 1 – BronchiectasisHow would you treat this patient?MDT approach: respiratory team, GP, occupational therapists
Conservative• Pulmonary rehabilitation
• Immunisations
Medical
• Bronchodilators and/or inhaled corticosteroids
• Long-term antibiotics: azithromycin
• Mucolytics
Surgical
• Lobectomy
• Lung transplantation

Peripheral• Fine tremor
47
Respiratory examination: Case 2
Central
• Reduced cricosternal distance• Hyper-resonant percussion• Global polyphonic wheeze
(9) (4)
48
Question 5

49
Respiratory examination: Case 2 – COPDPlease present your findings?
I performed a respiratory examination on this patient who has signs of chronic obstructive pulmonary disease
My main positive findings are:
• A fine tremor suggesting beta agonist use
• Evidence of tar staining
• A reduced cricosternal distance with hyper-resonant percussion suggesting lung hyperexpansion
• On auscultation, a global polyphonic wheeze
• Pitting peripheral oedema suggesting cor pulmonale

50
Respiratory examination: Case 2 – COPDPlease present your findings?
My relevant negative findings are:
• No signs of mediastinal shift: central trachea, apex beat non-displaced
• No signs of decompensation (no CO2 retention flap)
• No signs of other treatment e.g. no supraclavicular scar (seen for surgery for TB)
This points towards chronic obstructive pulmonary disease• The patient has evidence of a smoking history which is the likely underlying
cause• He also has evidence of cor pulmonale

51
Respiratory examination: Case 2 – COPDWhat are the differentials?
• COPD: think of possible causes• Elderly: smoking• Young: alpha-1-antitrypsin deficiency
• Asthma
COPD Asthma Older patient + Evidence of smoking Younger patient +/- smoking
Beta-agonists Anti-muscarinicInhaled corticosteroids
Beta-agonistsAnti-muscarinics not usedInhaled corticosteroids

52
Respiratory examination: Case 2 – COPDHow would you investigate this patient?
Bedside• Basic obs• Sputum MCS: screen for infection or colonisation
• H.influenzae and S.pneumoninae
• ECG: evidence of right heart failure e.g. RBBB and right axis
Bloods• FBC and CRP: evidence of infection
• ABG: type 2 respiratory failure
• Alpha-1-antitrypsin
53
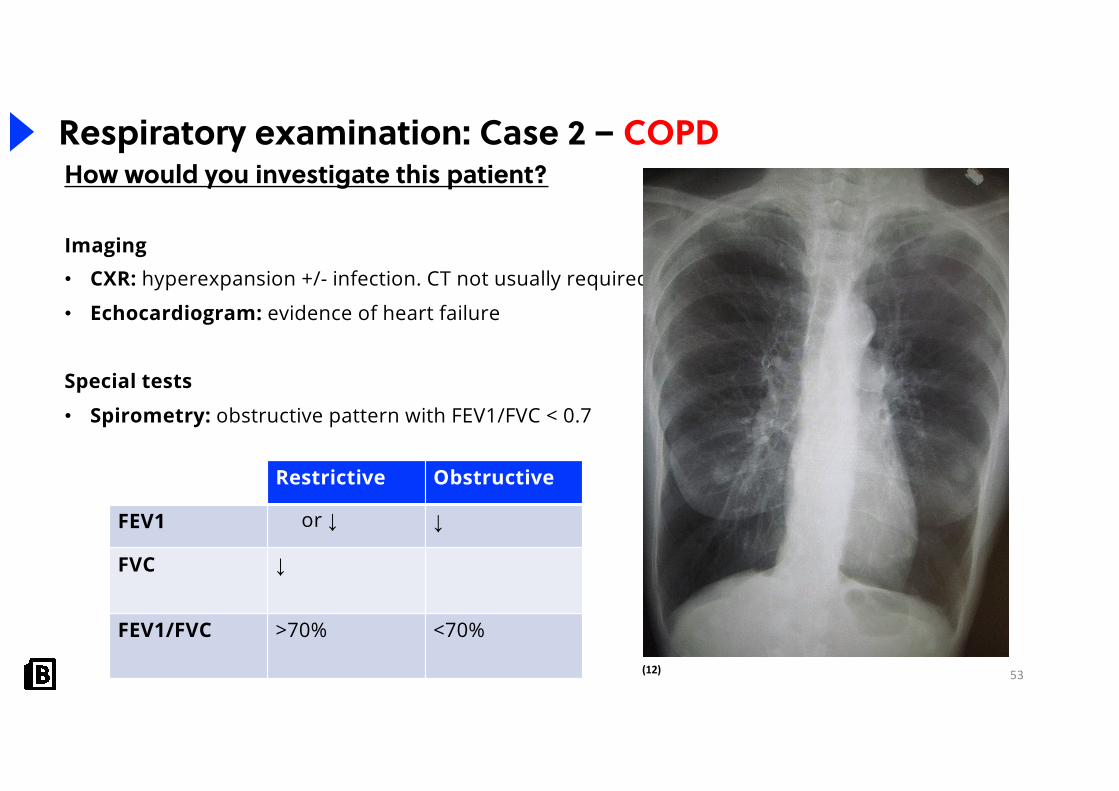
Respiratory examination: Case 2 – COPDHow would you investigate this patient?
Imaging • CXR: hyperexpansion +/- infection. CT not usually required
• Echocardiogram: evidence of heart failure
Special tests
• Spirometry: obstructive pattern with FEV1/FVC < 0.7
Restrictive Obstructive
FEV1 or ↓ ↓
FVC ↓
FEV1/FVC >70% <70%
(12)

54
Question 6

55
Respiratory examination: Case 2 – COPDHow would you treat this patient?MDT approach: respiratory team, GP, occupational therapists
Conservative• Smoking cessation and nicotine replacement
• Pulmonary rehabilitation
• Immunisations
Medical
• Bronchodilators and/or inhaled corticosteroids• Mucolytics
• LTOT
Surgical
• Lung volume reduction
• Lung transplantation

56
Respiratory examination: Case 2 – COPDIndications for LTOT?
LTOT is indicated in non-smokers with:• PaO2 <7.3 kPa OR
PaO2 ≥7.3 and <8 kPa AND 1 of the following:• Secondary polycythaemia• Peripheral oedema• Pulmonary hypertension
57
Top decile question
58
Recap‘Retrospective approach’1. Formulate an OSCE Cases List2. Prepare your ‘VIVA’ for those cases
• Positive signs of diagnosis• ‘Typical’ findings presentation• Risk factors• Signs of decompensation• List of differentials• Complications• How would you investigate this patient?• How would you manage this patient?
3. Finalise your examination routine• Each step of the routine• Signs you are looking for• Your speech
EXAMINATION ROUTINE
PRESENTATION
VIVA
• Perform each step of the routine confidently
• Pick up on signs
• Present findings systematically
• List appropriate differentials based on findings
• Answer questions systematically
• Explain your thinking


61
References
1. Wikicommons. Modified by JHeuser from the modified version by Dake of the original heart diagram by Wapcaplet. uploaded: 15. April 2006 {{cc-by-sa-2.5,2.0,1.0}} {{WikimediaAllLicensing}}
2. Mrug / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)3. Frank Gaillard / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)4. James Heilman, MD / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)5. U/ttriber. https://i.redd.it/ls1p27ofe4i41.jpg6. James Heilman, MD / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)7. Desherinka / CC BY-SA (https://creativecommons.org/licenses/by-sa/4.0)8. Wikicommons. RonEJ. Public domain. 9. National Heart Lung and Blood Institute / Public domain10. Mcgfowler / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)11. Hellerhoff / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)12. James Heilman, MD / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0)
All other images were acquired under the basic license from Shutterstock and not suitable for redistribution

62
Further information
Fill out a feedback form to receive yourCertificate of Attendance!
Stay up-to-date!• Website: www.bitemedicine.com• Facebook: www.facebook.com/biteemedicine• Instagram: @bitemedicine• Email: [email protected]
Presenter’s contact details• Instagram: @arun.kiru• Youtube: Arun Kiru• Twitter: @ArunKirupakaran• Email: [email protected]