
One Halton and General Practice Strategy Presenter NHS Halton CCG 27/03/15.
15
One Halton and General Practice Strategy Presenter NHS Halton CCG 27/03/15
-
Upload
gervais-jason-cummings -
Category
Documents
-
view
222 -
download
2
Transcript of One Halton and General Practice Strategy Presenter NHS Halton CCG 27/03/15.

One Halton and General Practice Strategy
PresenterNHS Halton CCG
27/03/15

ONE HALTON
Key strategic issues• Five Year Forward View
– New models of care– A new deal for primary care
• Dalton review• Care Act 2015• JSNA/BCF• Co-Commissioning
– Full delegation
• Collaborative commissioning• 2015/16 tariff & PMS review• A Call to Action• Prime Ministers Challenge Fund 2015

General Practice Strategy for Halton
• Population of 128,500• 17 practices (8 in Runcorn, 9 in Widnes)• 74 GPs (headcount)• 52 nurses• Registered list sizes at practices range from over
14,000 to 2,000
• A blueprint for co-commissioning general practice services from April 2015.
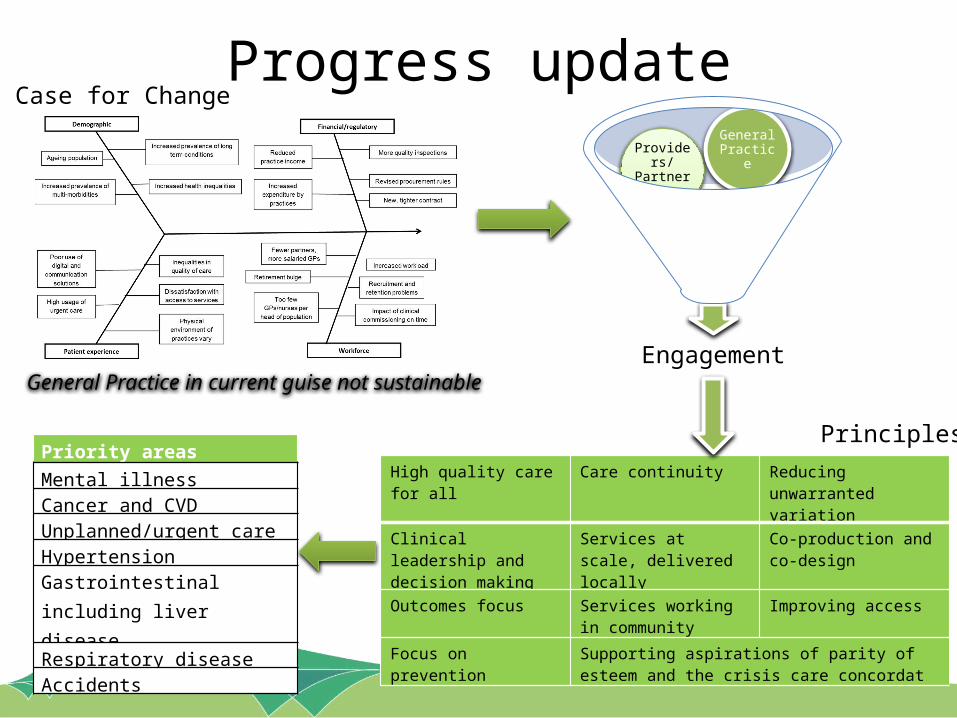
Progress updateCase for Change
Engagement
Public
Providers/ Partners
General Practice
High quality care for all Care continuity Reducing unwarranted variation
Clinical leadership and decision making
Services at scale, delivered locally
Co-production and co-design
Outcomes focus Services working in community
Improving access
Focus on prevention Supporting aspirations of parity of esteem and the crisis care concordat
General Practice in current guise not sustainable
PrinciplesPriority areas
Mental illnessCancer and CVDUnplanned/urgent care HypertensionGastrointestinal including liver disease
Respiratory diseaseAccidents
Emerging Care Model – Multi-Specialty Community Provision Key features
• Driving concept is to strengthen services in the community, wrapping them around local people, ensuring needs are met through integrated health and social care services
• Practices working together
• A focus on areas/conditions where we can have a greater impact
• Innovative solutions and alternative funding approaches
• Embracing the role, skills and insight of the local Voluntary/Community sector
• Creation of Community Hubs – co-location of services
• Multispecialty Community Provider (MCP) model
• Prime Minister Challenge Fund 2015

Partners and providers (not exhaustive)Community nursing Voluntary groups District nursing
Community midwives Community groups Social care services
Mental health teams Urgent care centres Elective pathways
Well being services Children’s services Health improvement teams
Family nursing Out of Hours provider Promotion, prevention and screening
Community pharmacy Outpatient services Diagnostic services
School nursing Health visiting Sexual health services

Proposed engagement approachPhase Approach Timescale
One Insight work – understanding behaviours, thoughts and views On-going *
Two Informing/warming up – mass publicity of work and engagement events
8 weeks(April – May)
Three Engaging and co-producing – designing care pathways with public/patients, General Practice and providers/partners
16 weeks(June – Sept)
Four Consultation – formally consulting on changes 12 weeks(Oct - Dec)
Five Implementation Business As Usual (Jan 16…)
‘* Run in parallel with phases two and three
• Clear objectives for each phase• Element of flexibility

So what’s next?

Well it could mean……..• Right person, right service, right time, right
place with best possible outcomes and experience?
• Tell your story once, get seen quicker, stay well longer?
• One assessment, One set of tests and One treatment plan?
• Plan together, Care together?
ONE HALTON

What we don’t want is….
• Rigid old ways of working• No more “like it or lump it” • One Size fits all• We don’t want centralised conformity, we want
what is right for our population. • Numerous hand offs and no diagnosis• Long Waits to get better (treatment)• Top down approach – we want to harness a
collective energy.

What we want is….
• A health and social care service to be proud of• Services fit for the populations needs• A multi speciality community model• Everyone working together• Improved care delivery• Better outcomes• Reduced inequalities• Joint planning

What we want is Ideas
We could see….. • GP surgeries set up in hospitals/Urgent Care Centres• Out patient clinics & diagnostics (x ray/blood tests)
in the community• Community services in different buildings (settings)• Different services in the same buildings• Specialist doctors and nurses in the community• Non clinical models supporting services and people• New creative (alternative) ideas

RehabilitationEnd of LifeChildren
Self CarePlanned CareUrgent Care
Prevention
Gen
eral
Pra
ctice
Soci
al c
are
Com
mun
ity
Men
tal H
ealth
Acut
e
Volu
ntar
y se
ctor
Publ
ic h
ealth
One Halton
Wel
l bei
ng
Phar
mac
y
Lear
ning
Dis
abili
ty
Trust
Communication
Culture
Commitment
Resource
Integration
Enablers – Resources, IM&T, Workforce, Estates, Communications & Engagement
Co production
Next steps• One Halton – direction of travel – have we got it right?• General Practice Strategy - Co produced – co
commissioned – Working Together• Engagement and communication- clinical and beyond• Commitment to deliver (this is what Halton does well) • Alignment of work plans and priorities• Multi agency / disciplinary teams• BUT HOW?


















