Oncology, lymphology and beyond engels
10
INTRODUCTION 1
Transcript of Oncology, lymphology and beyond engels

INTRODUCTION1

14 ONCOLOGY, LYMPHOLOGY AND BEYOND
1.1 WHY DID WE WRITE THIS BOOK?
Thefieldofoncologyandlymphologyisconstantlyexpandinginknowledge.According-ly,evidenceonthephysiotherapeuticmodalitiesusedisevolvingaswell:• duringorafterthetreatmentofcancer;• inoncologicalrehabilitation;• inthetreatmentofchronicedemaandbreastedema;• inthemanagementofsurgicalscars.
However,thereisagapbetweentheevidencefromscientificstudiesandtheimple-mentationofthesenewinsightsandevidenceinclinicalpractice,oftenbecauseofareluctancetoletgoofoldbeliefs.Therefore,thisbookwaswrittentoinformthereaderofthecurrentevidencefromaphysiotherapeuticpointofviewandtoprovideinsightintohowtointegratecurrentevidenceintodailyclinicalpractice.
1.2 WHAT WILL THIS BOOK BE ABOUT?
This textbookcombinesscientificevidenceandclinicalknowledgeconcerningphysi-caltherapiesduringorafteroncologicaltreatments,edematherapyandthetherapiesusedtotreatsurgicalscars.Thereisaclearrelationshipbetweendifferentpartsofthistextbook.Manyoncological treatments rely on surgery,which leaves surgical scars.Manypatientssufferfromfatigue,increasedordecreasedweight,lossofmusclemassandmusclestrengthanddecreasedphysicalenduranceorlymphedemaafterthetreat-mentofcancer.Needlesstosay,thesecomplicationshamperActivityofDailyLiving(ADL)activitiesandaffectapatient’squalityoflife.
Theaimofthistextbookistoprovidebasicknowledgeconcerningoncologicalrehabili-tation,thetreatmentofscarsandburnsandthetreatmentofchronicedemaonbehalfofimprovingpatient-centredcare.

15INTROdUCTION
1.3 FOR WHOM DID WE WRITE THIS BOOK?
Although this textbook iswrittenbya teamofauthorswitha strongconnection tophysiotherapyfrombothascientificandclinicalperspective,otherhealth-careprofes-sionalswillfindtheinformationinthistextbookuseful.Physicianswillgainmorein-sightintotheconservativeapproachestotreatingthesideeffectsofoncologicaltreat-ment,thetreatmentofchronicedemaincludingbreastedemaandthemanagementofsurgicalscarsbeforeredoingsurgerytotreatascar.Thetextbookwillalsofamiliarizephysicianswiththedifferenttreatmentmodalities,aswellastheevidencemotivatingtheuseofthesemodalities.Asaresult,physicianswillbeabletoreferpatientsandprescribephysiotherapymoreaccurately.Theinformationcontainedinthisbookwillbeofhelptopatient-centredcareingeneral.
Today’s care for patients, especially for patients suffering from a chronic condition,needstostartfromapatient-centredview.Therefore,theinformationinthistextbookishighlyrelevanttothosehealth-careprofessionals(e.g.,nurses,dietician,psycholo-gists,medicalsuppliers)whoareinvolvedinthecareofoncologicalpatients,patientswithchronicedemaandpatientswithsurgicalscars. Itprovidesthemwith informa-tionaboutthephysiotherapeuticmodalitiesandcandiscussmoreaccuratelyhowandwhenothertypesofinterventionsshouldbeimplementedintheplanofcareforcer-tainpatients.Ouroverallaimistoimprovecareforthesetypesofpatients.
1.4 THE EVIDENCE-BASED APPROACH
Theinformationinthisbookwaswrittenbasedoncarefullycomposedclinicalques-tionsusingthePICOSTmethodology.1Theseclinicalquestionswereansweredinlinewiththescientificandclinicalknowledgeavailableatthemomentofthewritingofthistextbook.Afterobtainingthisinformation,theevidencewastranslatedintotheclinicalrealityofdailypractice.
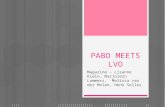
Toobtaintheevidence,severalsystematicreviewswereperformed.AdditionalinformationconcerningthesystematicreviewscanbefoundintheonlineplatformSofia.Apartfromthesystematicreviewsthatwereexecutedbytheteamsofthedifferentauthors,informa-tion/evidencewasappraisedfromotherguidelines,systematicreviewsandmeta-analysisaswellasoriginalresearch;allbasedonthe6Sapproachasdepictedinfigure1.1.
YoucanfindlinkstotheInternationalLymphoedemaFrameworkandtheJournalsattheUniversityofArizonaontheonlinelearningplatformSofia.

16 ONCOLOGY, LYMPHOLOGY AND BEYOND
SystemsIntegra�ng informa�on from the lower levels of the hierarchy withindividual pa�ent records, systems represent the ideal source of evidencefor clinical decision-making.
SummariesSummaries are regularly updated clinical guidelines or textbooks thatintegrate evidence-based informa�on about specific clinical problems.
Single studies with excellent methodologyUnique research conducted to answer specific clinical ques�ons.
Synopses of synthesesSummarize the informa�on found in systema�c reviews. By drawingconclusions from evidence at lower levels of the pyramid, these synopseso�en provide sufficient informa�on to support clinical ac�on.
SynthesesCommonly referred to as a systema�c review, a synthesis is a comprehensivesummary of all the evidence surrounding a specific research ques�on(meta-analyses).
Synopses of single studiesSummarize evidence from high-quality studies. The following evidence-basedabstract journals are the best place to find this type of informa�on CAT
Figure 1.1 The 6S pyramid for pre-appraised evidence.2
Theclinicalquestionsthatformedthebasisforretrievingtheevidenceusedforthistextbookwere:• Whatarethesideeffects(bothshort-termandlong-term)ofanoncologicaltreat-
mentandhowcanaphysicaltreatmentprovidereliefforthesesideeffects?• Whatarethecommonaspectsofanoncologicalrehabilitation?• Doweneedtotakemetabolismintoaccountwhensettingupanoncologicalreha-
bilitationprogramme?• What are common arm and shoulder complaints that warrant a physical treatment
duringoraftertheoncologicaltreatmentofbreastcancerpatientsinparticular?• Canpreventativeactionbetakentoavoidchronicedemaformationafteroncological
treatments?• What is the physical treatment of a chronic edema from a primary and secondary
aetiology?• Whatisthetreatmentofchoicefortreatingachronicedemaintheintensivephase
and maintenance phase?• Whatisthecurrentphysiotherapeuticmanagementofbreastedema?• Whatisthecurrentphysiotherapeuticmanagementofsurgicalscars?

17INTROdUCTION
1.5 THE ICF MODEL AND PATIENT-CENTRED CARE
ThistextbookiswrittenfromaperspectivethatincorporatestheInternationalClassifi-cationofFunctioning,DisabilityandHealth(ICF)3andpatient-centredcare.4
Fortunately,formostpeople,functioningindailylifeissomethingtheytakeforgranted.Theycan–withinlimits–dowhattheywant.Yetinourcaresettingsorinpatientpop-ulations,therearepeoplewithphysicalandpsychologicalproblemsthataresoseverethattheyaffectdaily lifeorevenmakeit impossible.Pain,associatedwithoncologic(orother)conditions,cancausesuffererstoreducetheiractivitylevelsignificantly.Re-strictionsinmobilitysometimesleadtonotparticipatinginsportingactivities.Environ-mental factors,suchaspoor familysupport,colleagueswhosmokeoranunsuitableworkplace,canadverselyaffecttheworksituation.
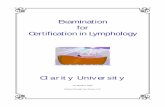
TheICFmodel(figure1.2)wascreatedbytheWorldHealthOrganizationinMay2001tocreateacommonlanguageforFunctioning,DisabilityandHealth.3
You can find a link to the International Classification of Functioning, Disability andHealthontheonlinelearningplatformSofia.
TheadvantageoftheICFmodelisthatitlooksathealthasacontinuumanditappliesto everyone. The ICF as a biopsychosocial model addresses factors at both the indi-vidualandthesocial level.Additionally, the ICFmodel focusesonbothpositiveandnegativeaspectsofhealth.3
Contextual factors
Health condi�on
Environmental factors Personal factors
Ac�vity Par�cipa�onBody Func�ons &Structures
(Disorder or disease)
(Impairments) (Limita�ons) (Restric�ons)
Figure 1.2 TheICFframeworkasdescribedbytheWHO.3

18 ONCOLOGY, LYMPHOLOGY AND BEYOND
TheICFisaframeworkusedaroundtheworldtodescribeahealthconditionofapa-tientinabroadbiopsychosocialcontext.Itappliestoeveryone,notjusttopeoplewithfunctionalproblems.Everyone’sfunctionalhealthconditioncanbedescribedusingtheICF.Itisnowwidelyused,forinstancetomeasurehealthstatusatthepopulationlev-el, inclinicalandepidemiologicalsettingstoclassify functionalstatusassessmentattheindividuallevel,andtoidentifygoalsettings,treatmentplanningandmonitoringaswellasoutcomemeasurement.TheICFdescribesdifferentdomainsoffunctioningfromabody,individualandsocietalperspective.Itscorestructureconsistsoftwoparts:• functioninganddisability;• contextual factors.
1.5.1 Functioning and disabilityWithinfunctioninganddisabilitytwosubcategoriesarerecognized:• bodyfunctionsandbodystructures;• activitiesandparticipation.
The body perspectiveisfurtherdividedintotwocomponents:• Thefirstisbody functionsandlistsallphysiologicalfunctionsofbodysystems.• Thesecond,body structures,listsallanatomicalpartsofthebody.
The individual and societal perspectives areelaborated in the componentactivities and participation.
1.5.2 Contextual factorsBoth environmental and personal factors comprise the contextual factors category.
The contextual factors(environmentalorpersonalfactors)mayaffect(facilitateorin-hibit)allcomponentsoffunctioninganddisability.Environmentalfactorsincludethephysical,socialandattitudinalenvironment(e.g.,profession,livingenvironment,socialsupport)andpersonalfactorsrefertoone’sattributes(e.g.,age,gender,copingstrate-gies)orinternalinfluencesonfunctioning.5
• Definitionofbodyfunctions:physiologicalandmental(psychological)proper-ties/functionsofthehumanorganism/bodysystems.
• Definitionofbodystructures:anatomicalpartsofthebodysuchasorgans,limbsandtheircomponentsorposition,presence,shapeandcontinuityofparts of the human body.

19INTROdUCTION
• Definitionofactivities:theexecutionofataskoractionbyanindividual/com-ponentsofanindividual’sactions.
• Definitionofparticipation:aperson’sparticipationinsocietyorinvolvementinalifesituation.
• Definitionofexternalfactors:one’sphysicalandsocialenvironmentinwhichpeople live and conduct their life.
• Definitionofpersonalfactors:aperson’sindividualbackground.
1.5.3 Human (dys)functioningAnindividual’sfunctioningconsistsofaninteractionbetweenthedifferentcomponentsandICFdomains.ThereisadynamicrelationshipbetweentheICFdomains,andthein-teractionsworkintwodirections,asillustratedinthefigure.Thesecomponentsofhu-manfunctioningandtheirproblemscanberepresentedintwoways.Ontheonehand,theycanbeusedtoindicatenon-problematicaspectsofhumanfunctioning,usingtheumbrellatermhumanfunctioning.Ontheotherhand,theycanbeusedtodescribedis-abilityandindicateproblems,suchasimpairmentsinbodyfunction/structure,activitylimitationsandparticipationrestrictions,usingtheumbrellatermdisability.
YoucanfindalinktoapracticalmanualonhowtousetheICFontheonlinelearningplatformSofia.
• Definitionofimpairments:abnormalitiesinorlossoffunctionsoranatomicalfeatures.
• Definitionoflimitations:difficultyapersonhasinperformingdailyactivities.• Definitionofparticipationrestrictions:problemsapersonexperienceswith
participatinginsociallife.
Disabilityinvolvesdysfunctionatoneormoreoftheselevels:impairmentsinbodyfunc-tionorstructures,activitylimitationsandparticipationrestrictions.Patientsencounter-ingdevastatingmedicalconditionsmaybeconfrontedwithlong-termimpairmentsinbodystructures(e.g.,scars,edema)andbodyfunctioning(e.g.,pain,limitedmobility),activitylimitations(e.g.,inabilitytowrite)andparticipationrestrictions(e.g.,inabilitytogotoschoolorwork)duringtheirrehabilitation.Theinteractionbetweenallaspectsoffunctioninghasadynamiccharacter:interventionsononeaspectorfactorcanbringaboutchangesinotherrelatedaspectsandfactors.Theinteractionsarespecificanddonothaveapredictableone-to-one relationship.As statedearlier, the interaction

20 ONCOLOGY, LYMPHOLOGY AND BEYOND
takesplace inbothdirections;thepresenceoffunctioningproblemscaninfluenceadisorder or disease. It is important in the care process to collect data on these con-structsindependentlyandthentoinvestigatepossiblerelationshipsandcausal links.Foracompletedescriptionof(dys)functioning,allcomponentsareimportant.Externalandpersonalfactorsalsoinfluenceaperson’sstateofhealthandleveloffunctioning.Theycaneachseparatelyortogetherinfluencefunctioningproblemsateverylevel.
Thepositiveaspectsandstrengthswithinfunctioningcanalsobehighlighted.Thebio-psychosocialvisionoftheICFmaymaketheverycomplexconsequencesofoncologicpathologiesmorecomprehensible.Theoverallgoalforeveryhealth-carepractitioneristorecoverthepatientstothepre-injurystateandtostriveforanoptimalfunctioningandreintegrationintosocietywithunalteredpotential.
1.6 PATIENT-CENTRED CARE
Patientorclient-centredcare(PCC)isdefinedbytheInstituteofMedicineasfol-lows: “Providing care that is respectfulof and responsive to individualpatientpreferences,needsandvalues,andensuringthatpatientvaluesguideallclinicaldecisions”.
Intheiroften-citedliteraturereview,MeadandBowerdescribePCCasencompassingfiveconceptualdimensions:6
• the biopsychosocial perspective, i.e. beyond the disease state and including thepsychologicalandsocialdomains;
• the‘patient-as-person’;• understandinganindividual’sparticularillnessexperiencewithinhisorherunique
lifecontext;• sharingpowerandresponsibility(anequalcaregiver-patientrelationship);• thetherapeuticalliance(care-giver-patient),withempathy,congruenceanduncon-
ditionalpositiveregard.
Ifweimplementpatient-centredcarewithinthecaregiverprocess,theuseofpatient-re-portedoutcomemeasures (PROMs) seems imperative.PROMsare thegold standardforpatient-centredcaretoefficientlyevaluatethepatient’sfeelings,thoughtsandcom-plaintsaboutaclinicalinterventionordisease.CliniciansusePROMstoguideandauditroutinecareandsupportPCC.Manyquestionnairesarealreadypartofstandardintake

21INTROdUCTION
procedureswithin oncologic rehabilitation. At the patient level, data can be used tomonitorindividualprogress,investigatetheeffectsofmedicalandsurgicalinterventionsandimprovecommunicationbetweenpatientsandcaregivers.7FunctionaloutcomeisoftenmeasuredusingPROMs.Expertconsensusexistsonusingbothgenericanddis-ease-specificQualityofLife(QoL)questionnairestocapturethefullimpactofahealthcondition.8
The conceptofHealthRelatedQualityof Life (HRQOL)overlapswith thatofhealthandQualityofLife (QoL).Differentdefinitionsof thesethreeconceptsexist.9 In this manuscriptwemakenoexplicitdistinctionbetweenthedifferentconceptsandusethetermQoLasanall-encompassingtermtotalkaboutHRQOLandQoLmeasuresforthereaders’ convenience.
AccordingtotheWHOQOLgroup(1995),QoLisdefinedas:“Anindividual’sper-ceptionsoftheirpositioninlifeinthecontextofthecultureandvaluesystemsinwhichtheyliveandinrelationtotheirgoals,expectations,standardsandcon-cerns. It isabroadrangingconceptaffected inacomplexwaybytheperson’sphysicalhealth,psychological state, levelof independence, social relationshipsandtheirrelationshiptosalientfeaturesoftheirenvironment.”10
Weencourageallhealth-careworkerstoapproachpatientsinaholisticbiopsychosocialwayandinapatient-centredway.Thesearenotemptyconceptsbutrequirecommit-ment,interactionandeffortfromallpartiesinvolved.Atregularintervalsinthecareprocess,thefollowingquestionsseemimportanttous:• Whatismypatient’swish?• Whatismypatient’sidea,opinionorfeeling?• Howhashisorherbiopsychosocialfunctioningchanged?• HowcanIempowerthepatientaspartofthe(multidisciplinary)team?
Clear
Jointdecision
making
Info
rma�
on e
xcha
nge
Communica�on
Empo
wer
men
t
Collabora�onSharedaccountability
Goodexperience Sh
ared
power
Sharedresponsibility
voice Figure 1.3 Importantaspectsofpatient-centredcare.

22 ONCOlOgy, lympHOlOgy ANd bEyONd
1.7 REFERENCES1. GebruersN,MeeusM.Health Science Literacy. From research to review. Acco;2021.2. DiCensoA,BayleyL,HaynesRB.ACPJournalClub.Editorial:Accessingpreappraisedevidence:
fine-tuningthe5Smodelintoa6Smodel.AnnInternMed.2009;151(6):Jc3-2,jc3-3.3. WorldHealthO.Internationalclassificationoffunctioning,disabilityandhealth:ICF.In.Geneva:
WorldHealthOrganization;2001.4. BarryMJ,Edgman-LevitanS.Shareddecisionmaking--pinnacleofpatient-centeredcare.NEngl
JMed.2012;366(9):780-781.5. PetersonDB.InternationalClassificationofFunctioning,DisabilityandHealth:AnIntroduction
forRehabilitationPsychologists.Rehabilitationpsychology.2005;50(2):105-112.6. MeadN,BowerP. Patient-centredness: a conceptual framework and reviewof the empirical
literature.SocSciMed.2000;51(7):1087-1110.7. MeirteJ,HellemansN,AnthonissenM,etal.BenefitsandDisadvantagesofElectronicPatient-re-
portedOutcomeMeasures:SystematicReview.JMIRPerioperMed.2020;3(1):e15588.8. VanBeeckEF,LarsenCF,LyonsRA,MeerdingWJ,MulderS,Essink-BotML.Guidelinesforthecon-
ductionoffollow-upstudiesmeasuringinjury-relateddisability.JTrauma.2007;62(2):534-550.9. KarimiM,BrazierJ.Health,Health-RelatedQualityofLife,andQualityofLife:WhatistheDiffer-
ence?Pharmacoeconomics.2016;34(7):645-649.10. TheWorldHealthOrganizationQualityofLifeassessment(WHOQOL):positionpaperfromthe
WorldHealthOrganization.SocSciMed.1995;41(10):1403-1409.