Oncology Care Model (OCM) WSMOS presentation Final Care Model (OCM) WSMOS...
41
Oncology Care Model (OCM) Carol Vanevenhoven, Pharm.D, MBA Mark Nelson, Pharm.D
Transcript of Oncology Care Model (OCM) WSMOS presentation Final Care Model (OCM) WSMOS...

Oncology Care Model (OCM)
Carol Vanevenhoven, Pharm.D, MBAMark Nelson, Pharm.D

Today’s Focus1. Factors and legislation driving payment reform
2. Overview of Oncology Care Model
3. Implementation Challenges
4. Where is all this headed?

Background1. U.S. healthcare is fragmented, inefficient, inaccessible &
expensive
2. Move from “volume-‐based” care to “value-‐based” care
3. Catalyzed in large part by federal health reform
4. Cancer care is a high cost service with high variability
5. CMMI’s new Oncology Care Model (OCM) is the latest alternative payment model (APM)

Cancer Care Costs Rising Faster than Overall Healthcare

MACRA Law 2015• Eliminates SGR Formula• Transition from “buy and bill” to Value Based Care• Value = quality/cost
• 4 year implementation (2019)• Choose Alternative Payment Model (APM) or MIPS


Not subject to MIPS
What are my Options Under MACRA?Am I in an APM?
Yes NO Is this my first year in Medicare OR am I below the low-‐
volume threshold?
Yes NO
Am I in an Advanced APM?
Yes NO
Do I have enough payments or patients through my
advanced APM?
Yes NO Subject to MIPS
Qualifying APM Participant (QP)Excluded from MIPS5% lump sum bonus payment (2019 – 2024),
higher fee schedule updates (2026+)APM specific rewards
Favorable MIPS scoring & APM specific rewards
There will be financial incentives for participating in an APM even if you don’t
become a QP
Slide courtesy of the Centers of Medicare and Medicaid Services


MedicareAlternative Payment ModelOncology Care Model (OCM)
MedicareMerit-‐based Incentive Payment System

OCM vs MIPS

OCM Overview• New payment and delivery model• 5 yr program testing episode based payment incentives
• 6-‐month episodes• Goal to align financial incentive to improve – Care coordination– Appropriateness of care– Access for chemotherapy patients

6 Practice Transformation Elements1. Provide core functions of patient navigation2. Documented 13 point care plan 3. 24/7 access to an appropriate clinician who
has real time access to the patient’s EMR4. Use and ONC-‐certified EMR and attest to MU5. Follow national guidelines (NCCN, ASCO)6. Utilize data for continuous quality
improvement

Participation• Nationally 195 practices & 19 payers• Washington State 3 practices

Practice CharacteristicsNumber of Medicare Beneficiaries
CMS-‐HCC Risk Scores
OCM practices All practices
25th Percentile 260 48
50th Percentile 446 86
75th Percentile 918 204
OCM practices All practices
25th Percentile 0.992 0.968
50th Percentile 2.275 2.058
75th Percentile 3.879 3.739

Washington State
• Northwest Medical Specialties– Tacoma, WA
• North Star Lodge Cancer Center– Yakima, WA
• Northwest Cancer Specialists PC– Vancouver, WA

North Star Lodge (NSL)
• Comprehensive Cancer Center– 6 medical oncologists, 2 mid-‐levels– 3 radiation oncologists– 22 infusion chairs – Outreach to Ellensburg and Sunnyside
• Around 850 new analytic cases annually• Medicare primary payer

Northwest Medical Specialties -‐NWMS
• Ten Oncologists, seven mid-‐levels• 6 clinics• 3,500 new patients annually• Well-‐develop research program• OCM participant• Two commercial VBC programs• 65% of all patient currently eligible for VBC

Two New Sources of Revenue
•$160PMPM•Care management and compliance
MEOS Payments
• Percent of savings• Percent depends on quality measures
Performance-‐Based
Payments (PBP)

Performance Based Payment (PBP)
• PBP = the difference between risk adjusted benchmark price and cost
• Discount from “benchmark Price”: 4% 1-‐sided risk; 2.75% 2-‐sided risk
• Each 6-‐month episode• Adjusted based on quality scores


Risk Adjustment and Price
• Complex patients cost more• Intent is to financially credit groups for managing complex patients
• Risk is adjusted PRIOR to first chemo claim

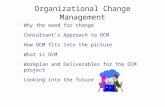
Episode Costs Vary Dramatically

Implications
Predicting patient costs will be very difficult
Averages don’t tell us very much
We also know that OCM prices don’t
work well
Variability = Opportunity
We need to examine what makes high cost
episodes more expensive
Patients with a cancer type are highly variable
Will lead to volatility in performance-‐based payments

Sources of Cost SavingsSource % Cost Reduction
Drugpathways compliance 1.0% to 3.0%
Avoidable ER utilization 0.6% to 1.1%
Avoidablehospital admissions 4.0% to 7.0%
Diagnostics (imaging, lab) 0.2% to 0.5%
End-‐of-‐life caremanagement 0.9% to 1.9%
Total potential savings 6.7% to 13.5%
(1) John D. Sprandio, MD, Consultants in Medical Oncology & Hematology. Oncology Patient Centered Medical Home ® Analysis of OPCMH savings conducted by third party actuary 2010. (2) How Oncologists are Bending the Cost Curve. Oncology Times. January 10, 2013. (3) Changing Physician Incentives for Affordable, Quality Cancer Care: Results of an Episode Payment Model. Newcomer et. Al. Journal Oncology Practice. July 8, 2014.

7 Sections for AnalysisPricing Analysis
Understanding Episode Costs
Physician Comparative Performance
Hospital Utilization (Admits and ER Visits)
Drug Regimens
End-‐of-‐life Care
Volatility and Risk

Clinical Data and Quality MeasuresNQS domains
1. Communication and care coordination
2. Person and caregiver caregiver-‐centered experience and outcomes
3. Clinical quality of care4. Patient safety
Data sources1. Medicare claims-‐
based2. Patient-‐reported
experience (surveys)3. Practice-‐reported
data

Key Tactics for OCM• Form patient navigation department– Nurse navigators, social workers, financial advocates
• Part time survivorship nurse practitioner• Part time palliative care nurse practitioner• Standardize electronic screening tools for depression and psychosocial distress
• Develop/document/deliver care plans

Transformation Plan Vignettes
Provide core functions of patient navigation

Patient Navigation

Transformation Plan Vignettes
Documented 13 point care plan

IOM Care Management Plan

Sample: 13 Point Care Plan

Estimated Out of Pocket Costs

Team StatsScheduler QueueClinical Team Tool
Survivorship Resource Coordination DatabaseCarol Vanevenhoven, PharmD, MBA; Amanda Geerhart, CTR; Laura Fernandez, CTR
Tracking Time
Average Time (Minutes)
Non-‐Scheduled Follow Up

Advanced Care Planning
Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep OctNumber of Records Uploaded to HIE n/a 0 0 62 29 36 32 22 34 32 29 41Number of New Oncology Patients Seen at NSL in the prior month n/a 92 102 94 86 110 111 94 114 179 140 109Per Month % of records uploaded to HIE 0% 0% 66% 34% 33% 33% 24% 30% 18% 23% 38%YTD % of patients uploaded to HIE 0% 0% 22% 24% 26% 27% 26% 27% 25% 25% 26%

Transformation Plan Vignettes
Cost Savings Targets

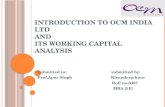
Understanding ED Admissions
0
10
20
30
40
50
60
Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Frequency
YVMH ED Visits by Day of the WeekAnnual Average Between 2013 -‐ 2015

Understanding ED Admissions
0
5
10
15
20
25
30
12:00A
M
1:00
AM
2:00
AM
3:00
AM
4:00
AM
5:00
AM
6:00
AM
7:00
AM
8:00
AM
9:00
AM
10:00A
M
11:00A
M
12:00P
M
1:00
PM
2:00
PM
3:00
PM
4:00
PM
5:00
PM
6:00
PM
7:00
PM
8:00
PM
9:00
PM
10:00P
M
11:00P
M
YVMH ED Visits by Time of DayAnnual Average Between 2013 -‐ 2015

Understanding ED Admissions
4
101
169
31
20
20
40
60
80
100
120
140
160
180
LVL1 LVL2 LVL3 LVL4 LVL5
Frequency
Acuity Level
YVMH ED Acuity Levels OCMAnnual Average 2013-‐2015

• CMS will learn from OCM and will likely encourage assumption of 2-‐sided risk in OCM year 3 (2019). OCM 2-‐sided risk likely to be a MACRA APM
• Will likely enable the shift of financial risk to providers. In oncology, risk shift most likely to be to bundled/episodic pricing
• Timeframe: ability to engage in and influence the outcome next 12-‐18 months; the rest plays out over the subsequent 3-‐5 years. There will be “winners” and there will be “losers.”
Where is all this Headed?

FAMILY TREE OF ALTERNATIVE PAYMENT IN ONCOLOGY
Oncology Medical Home (OCM is an OMH Model)
Shared Savings -‐ two sided risk
Bundles -‐Procedure Specific
Bundles -‐Cancer Type Specific
Capitation
Fee-‐for-‐Service
Care Management
Fees
Pathways Compliance
Shared Savings –one sided risk
Increasing Level of Risk
Oncology Medical Home (OCM is an OMH Model)
Bundles -‐Procedure Specific
Pathways Compliance