Oncologic Emergencies UCSF HO 2014.ppt Inpatient Care for Children and “High Risk” Adult ......
13
1 It’s Not A Tumor! Oncologic Emergencies Diane M. Birnbaumer, M.D., FACEP Professor of Medicine University of California, Los Angeles Senior Clinical Educator Department of Emergency Medicine Harbor-UCLA Medical Center Oncologic Emergencies n Increasing incidence of cancer n Improved survival n Patients with malignancies may present to EDs and general medical offices n Oncologic emergencies n Those resulting from the disease itself n Those resulting from cancer therapy Oncologic Emergencies: General Categories n Metabolic Emergencies n Hypercalcemia n Tumor Lysis Syndrome n Neurologic Emergencies n Malignant spinal cord compression n Brain metastases and increased ICP n Infectious Complications n Neutropenic fever Oncologic Emergencies: General Categories n Cardiovascular Emergencies n Malignant pericardial effusion n Superior vena cava syndrome n Hematologic Emergencies n Hyperviscosity due to dysproteinemia n Hyperleukocytosis and leukostasis
Transcript of Oncologic Emergencies UCSF HO 2014.ppt Inpatient Care for Children and “High Risk” Adult ......

1
It’s Not A Tumor! Oncologic Emergencies
Diane M. Birnbaumer, M.D., FACEP
Professor of Medicine
University of California, Los Angeles
Senior Clinical Educator
Department of Emergency Medicine
Harbor-UCLA Medical Center
Oncologic Emergencies
n Increasing incidence of cancer
n Improved survival
n Patients with malignancies may present to EDs and general medical offices
n Oncologic emergencies
n Those resulting from the disease itself
n Those resulting from cancer therapy
Oncologic Emergencies: General Categories
n Metabolic Emergencies
n Hypercalcemia
n Tumor Lysis Syndrome
n Neurologic Emergencies
n Malignant spinal cord compression
n Brain metastases and increased ICP
n Infectious Complications
n Neutropenic fever
Oncologic Emergencies: General Categories
n Cardiovascular Emergencies
n Malignant pericardial effusion
n Superior vena cava syndrome
n Hematologic Emergencies
n Hyperviscosity due to dysproteinemia
n Hyperleukocytosis and leukostasis

2
Oncologic EmergenciesNeutropenic Fever
n Fever
n Single oral temperature > 38.3C (101.3F)
n Sustained temperature > 38C (100.4F) for > 1 hour
n Neutropenia
n Absolute neutrophil count < 1,000
n Severe neutropenia
n Absolute neutrophil count < 500
Oncologic EmergenciesNeutropenic Fever
n Most commonly seen after chemotherapyn Also seen in myelogenous cancers
n Risk of infection depends on…n Depth of neutropenia
n Duration of neutropenia
n Comorbid conditions (e.g. mucositis)
n Nadir usually 5-10 days after last chemo dosen Recovers 5 days after nadir (usually)
Oncologic EmergenciesNeutropenic Fever
n Organisms
n Multiple organisms implicated
n Enteric gram negatives
n Gram positives
n Frequently no organism recovered
Oncologic EmergenciesNeutropenic Fever
n Presentation
n Fever usually only symptom
n May range from fever only to severe sepsis
n Neutropenia leads to atypical presentation with common infections
n E.g. pneumonia patients may have no infiltrate; UTI patients may have no pyruia

3
Oncologic EmergenciesNeutropenic Fever
n Presentation
n Careful physical examination crucial
n Particular attention to skin, oral cavity, sites of indwelling catheters, perianal area
n Rectal examination discouraged
Oncologic EmergenciesNeutropenic Fever
n Evaluation
n Blood cultures
n Peripheral vein AND any indwelling catheters
n Urine cultures
n Sputum cultures
n Stool, CSF cultures if indicated
Oncologic EmergenciesNeutropenic Fever
n Evaluation
n CXR may be normal
n Consider CT for higher resolution
Oncologic EmergenciesNeutropenic Fever
n Treatment
n All febrile neutropenic patients should receive antibiotics ASAP
n Afebrile neutropenic patients with high suspicion of infection also should get rx
n Broad spectrum to start; narrow later

4
Oncologic EmergenciesNeutropenic Fever
n Treatment
n Most patients should be admitted
n Highly selected patients MAY be treated as outpatients
n Very close follow-up necessary
n Must have ready access to health care
n Assess personal / social situation
Oncologic EmergenciesNeutropenic Fever
n Multinational Association Scoring Systemn No or mild symptoms 5
n No hypotension 5
n No COPD 4
n Solid tumor or no previous fungal infxn 4
n No dehydration 3
n Moderate symptoms 3
n Outpatient status 3
n Age < 60 years 2
Score • 21 low risk for serious medical complications
Neutropenic FeverAntibiotic Strategies
n Broad empiric coverage + coverage for any suspected/ known infections
n Gram-negative coverage for all patients
n Gram-positive coverage for selected patients per IDSA recommendations
n Use bactericidal antibiotics administered through alternate ports to indwelling lines
Neutropenic Fever Treatment
n Clinical Practice Guidelines
n Clinical Infectious Diseases CID 2011:52 (15 February)

5
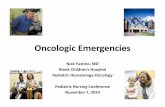
IDSA Management Algorithm
Clin Infect Dis 2002; 34: 730-51.
IDSA RecommendationsOutpatient Treatment
n Suggested Antibiotic Regimen:n Ciprofloxacin 500mg PO q8• PLUS
n Amoxicillin/Clavulanate 500mg PO q8•
n Penicillin-allergic Patients:n Ciprofloxacin 500mg PO q8• PLUS
n Clindamycin
n Note: Outpatient therapy not recommended for the pediatric population.
Clin Infect Dis 2002; 34: 730-51.
IDSA Recommendations Inpatient Treatment
n Inpatient Care for Children and “High Risk” Adult Patientsn Monotherapy: Single, broad-spectrum IV agent
n Cefipime (4th generation cephalosporin)n Ceftazidime (3rd generation cephalosporin)n Carbapenem (Imipenem or Meropenem)
n Combination Therapy:n Aminoglycoside (Gentamicin, Tobramycin, or Amikacin) PLUSn Antipseudomonal beta-lactam (Ticarcillin-clavulanic acid or
Piperacillin-tazobactam), ORn Antipseudomonal cephalosporin (Cefipime or ceftazidime), ORn Carbapenem (Imipenem or Meropenem)
n None of these have been shown to be clearly superior.
Clin Infect Dis 2002; 34: 730-51.
Oncologic EmergenciesSpinal Cord Compression
n Relatively common
n 2.5 to 6% of cancer patients
n Most common: Breast, lung, prostate
n Confers poor prognosis overall
n Urgent need to make diagnosis and treat
n Neuro status at presentation and rapidity of onset predict functional outcome

6
Oncologic EmergenciesSpinal Cord Compression
n Usually results from extension from spinal bony metastases
n Less commonly extends through foramina
n Lymphomas, sarcomas
n Will not see bony destruction
n Most common in thoracic spine
Oncologic EmergenciesSpinal Cord Compression
n Presentation
n 90% have back pain
n 80% have preceding diagnosis of malignancy
n May have several simultaneous lesions
n BACK PAIN + MALIGNANCY = SCC!!
Oncologic EmergenciesSpinal Cord Compression
n Presentation
n Symptoms
n Radicular pain
n Motor weakness
n Gait disturbance
n Bowel or bladder dysfunction
n Imperative to try to diagnose before neurologic dysfunction occurs
Oncologic EmergenciesSpinal Cord Compression
n Evaluation
n MRI is imaging study of choice
n Consider imaging entire spine (+/- C spine)
n CT myelography second choice
n Plain films / nuclear medicine poor choices
n Limited sensitivity and specificity
n Plain films may show bony lesions
n Negative plain films do NOT rule out SCC

7
Oncologic EmergenciesSpinal Cord Compression
n Treatment
n Start as soon as possible; need tissue diagnosis
n Glucocorticoids
n Dexamethasone 10-16 mg IV, then 4 mg every 6 hours
n Radiation
n Mainstay of therapy (?)
n Surgery may also be indicated (or preferable)
Oncologic EmergenciesMalignant Pericardial Effusion
n Common in advanced cancer
n Frequently asymptomatic
n Poor prognosis
n Most patients die within one year
Oncologic EmergenciesMalignant Pericardial Effusion
n Presentation
n Symptoms depend on rapidity of onset
n May see dyspnea, cough, chest pain, dysphasia, hiccups, hoarseness
n May find tachycardia, distant heart sounds, JVD, UE and LE edema, pulsus paradoxus
n Tamponade = hypotension/shock with tachycardia, JVD
Oncologic EmergenciesMalignant Pericardial Effusion
n EKG
n Low voltages
n Electrical alternans

8
Oncologic EmergenciesMalignant Pericardial Effusion
Oncologic EmergenciesMalignant Pericardial Effusion
n Evaluation
n Echo preferred test
n Presence of fluid
n “Tamponade physiology”
n CT and MRI also useful
n Treatment
n Pericardiocentesis
Oncologic EmergenciesSuperior Vena Cava Syndrome
n Usually caused by compression of SVC
n Benign and malignant causes
n Lung cancer, lymphoma most common malignancies
n May also be caused by intraluminal thrombus
n Often due to indwelling catheters
Oncologic EmergenciesSuperior Vena Cava Syndrome
n Presentation
n Onset usually insidious; may be rapid
n Dyspnea, facial swelling, cough
n Cough may aggravated by leaning forward, stooping
n Exam
n Distended neck / chest wall veins
n Facial edema
n Upper extremity edema

9
Oncologic EmergenciesSuperior Vena Cava Syndrome
n Evaluation
n CT with contrast
n MRI also useful
n Treatment
n Unless respiratory compromise, not a true emergency
n Radiation, stenting, chemo, steroids as indicated
Oncologic EmergenciesTumor Lysis Syndrome
n Seen in aggressive hematologic malignanciesn High grade lymphoma, acute leukemia
n Seen after treatment of treatment of active solid tumors
n Massive release of intracellular contents after tumor deathn Can cause severe metabolic derangements
n May be life threatening
Oncologic EmergenciesTumor Lysis Syndrome
n Hyperuricemia
n Crystallize in renal tubules
n Can lead to acute renal failure
n Hyperkalemia
n Life-threatening arrhythmias
n Hyperphosphatemia
n Leads to hypocalcemia, tetany, seizures, arrhythmias
Oncologic EmergenciesTumor Lysis Syndrome
n Presentationn Rare to see; usually prevented during
treatment
n Suspect in patients with aggressive hematologic malignancies or solid tumorsn Especially with recent chemotherapy
n Seizures
n Arrhythmias
n Decreased urine output / volume overload

10
Oncologic EmergenciesTumor Lysis Syndrome
n Presentation
n Send uric acid, phosphorus, potassium, LDH, calcium
n Check EKG as well
n Grading systems define degree of illness
Oncologic EmergenciesTumor Lysis Syndrome
n Treatment
n Prophylaxis best
n Allopurinol 2-3 days before chemo
n Maintain good hydration
n If TLS present
n Admit ICU / monitor
n Maintain hydration n Want urine output 100-200 mL/hr
n Take care if renal failure
n Treat electrolyte disturbances
Oncologic Emergencies: Hypercalcemia
n Occurs in 10-30% of cancer patients
n Usually seen in patients with known cancer
n Carries a poor prognosis
n Most commonly seen in
n Breast cancer
n Lung cancer
n Multiple myeloma
Oncologic Emergencies: Hypercalcemia
n 3 types
n Humoral hypercalcemia of malignancy
n Via PTHrP (parathyroid related hormone)
n Most common mechanism (33-88%)
n Local bone destruction
n Tumor production of vitamin D analogues

11
Oncologic Emergencies: Hypercalcemia
n Presentation
n Multiple, nonspecific symptoms
n Lethargy, confusion
n Anorexia, nausea
n Constipation
n Polyuria, polydipsia
n Some correlation with rapidity of onset and degree of hypercalcemia
Oncologic Emergencies: Hypercalcemia
n Physical exam usually unhelpfuln May see lethargy
n May see dehydration
n Laboratory
n Must correct total serum calcium for albuminn Measured total Ca + [0.8 x (4.0-albumin)]
n Also check creatinine, other electrolytes, alkaline phosphatase
n Low serum chloride suggestive of hypercalcemia of malignancy
Oncologic Emergencies: Hypercalcemia
n Treatment
n Consider the big picture; comfort measures only may be appropriate
n Hydration with normal saline first step
n Patients often very volume depleted
n Avoid loop diuretics until euvolemic
Oncologic Emergencies: Hypercalcemia
n Treatment
n Bisphosphonates
n Pamidronate, zoledronic acid
n Doses adjusted based on renal function
n Block osteoclastic bone resorption
n SubQ or IM calcitonin (not nasal)
n Quickly lowers serum calcium levels
n Short-lived effect

12
Oncologic Emergencies: Hypercalcemia
n Treatment
n Corticosteroids
n Most effective in hematologic malignanciesn (Elevated levels of vitamin D)
n Dialysisn Patients with renal or heart failure
n Avoid oral phosphate
n Effective treatment of underlying cancer may be useful
Oncologic Emergencies: Hypercalcemia
n Treatment
n Mithramycin
n Multiple side effects limit use
n Gallium nitrate
n Slow infusion rate
n Both have fallen out of favor since introduction of biphosphonates
Oncologic EmergenciesCase Presentation
n Patient received IV NS
n Calcium came down to 10.2 with fluids only
n Workup showed multiple bony metastases throughout
n Follow-up with oncologist; long term care plan discussed with patient
Oncologic EmergenciesBrain Metastases / Increased ICP
n Seen in up to 25% of terminal cancer patients
n Lung, breast, melanoma most common
n Brain edema from tumor expansion causes increased ICP

13
Oncologic EmergenciesBrain Metastases / Increased ICP
n Presentation
n History of cancer in most cases
n Symptoms range from focal to generalized
n Symptoms often subtle, gradual in onset
n Only 50% have headaches
n May see seizures, symptoms of increased ICP
n Confers very poor prognosis
Oncologic EmergenciesBrain Metastases / Increased ICP
n Evaluation
n MRI preferred study
n CT may miss posterior fossa lesions
n Treatment
n May want to consider palliative treatment only
n Steroids for symptom management
n Antiepileptics as needed
n Whole brain irradiation may be indicated
A personal note…
n Discussions regarding end of life care crucial in terminal diseases
n Hospice care, especially home hospice care, provides comfort and addresses quality of life
n Goal is to help the patients live comfortably on their own terms and choose how they want to live the rest of their lives
Thank You For Your Attention!!
Any Questions?