Oncologic Emergencies - psons.orgpsons.org/.../10/Section-22-Oncologic-Emergencies... · Oncologic...
24
1 Oncologic Emergencies Juanita Madison, RN, MN, AOCN Franciscan Health System Oncologic Emergencies Life-threatening medical emergencies caused by: Malignancy Treatment of malignancy When do they occur? Initial manifestations of malignancy or Late in disease process Oncologic Emergencies Metabolic Oncologic Emergencies Tumor Lysis Syndrome (TLS) Sepsis & Septic Shock Disseminated Intravascular Coagulation (DIC) Hypercalcemia Inappropriate Antidiuretic Hormone Secretion (SIADH) Anaphylaxis Structural Oncologic Emergencies Spinal Cord Compression Superior Vena Cava Syndrome Increased Intracranial Pressure (ICP) Cardiac Tamponade Tumor Lysis Syndrome (TLS) Metabolic imbalance Caused by breakdown of malignant cells (spontaneous, or induced by chemotherapy, biotherapy, or radiation therapy) Large number of rapidly proliferating cells killed Cell lysis, rupture of tumor cell membranes Intracellular components released into blood stream Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies: A resource for nurses .Oncology Nursing Society, Pittsburgh, PA. pp: 433-459.
Transcript of Oncologic Emergencies - psons.orgpsons.org/.../10/Section-22-Oncologic-Emergencies... · Oncologic...

1
Oncologic Emergencies
Juanita Madison, RN, MN, AOCN
Franciscan Health System
Oncologic Emergencies
Life-threatening medical emergencies caused by:
Malignancy
Treatment of malignancy
When do they occur?
Initial manifestations of malignancy
or
Late in disease process
Oncologic Emergencies
Metabolic Oncologic Emergencies Tumor Lysis Syndrome (TLS)
Sepsis & Septic Shock
Disseminated Intravascular Coagulation (DIC)
Hypercalcemia
Inappropriate Antidiuretic Hormone Secretion (SIADH)
Anaphylaxis
Structural Oncologic Emergencies Spinal Cord Compression
Superior Vena Cava Syndrome
Increased Intracranial Pressure (ICP)
Cardiac Tamponade
Tumor Lysis Syndrome (TLS)
Metabolic imbalance
Caused by breakdown of malignant cells (spontaneous, or induced by chemotherapy, biotherapy, or radiation therapy)
Large number of rapidly proliferating cells killed
Cell lysis, rupture of tumor cell membranes
Intracellular components released into blood
stream
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing
oncologic emergencies: A resource for nurses .Oncology Nursing Society, Pittsburgh, PA. pp: 433-459.

2
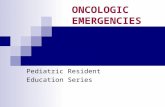
TLS: Pathophysiology
Intracellular components Potassium
Phosphorous
Nucleic acids (DNA, RNA)
Cell killed (lysed), cell membrane ruptures
Nucleic acids released into blood stream
Potassium & Phosphorous released into blood stream
Results in: Hyperuricemia
Hyperkalemia
Hyperphosphatemia
Hypocalcemia
K+
PO4- PO4
-
Nucleic Acids
K+ K+
K+ PO4-
K+
Nucleic
Acids
Hypoxanthine
Xanthine
Uric Acid
Urine
PO4- K+ K+ PO4
- PO4-
Ca++ Ca++ Ca++ Xanthine
Oxidase
(Liver)
Tumor Lysis Syndrome: Who’s At Risk?
Most common in: Patients with large tumor burden that is highly responsive to antineoplastic therapy (resulting in rapid cell kill)
Risk Factors: Tumor-related
High-grade lymphomas
Hematologic malignancies (acute or chronic leukemia's with WBC)
Tumors with high growth fractions (anticipated to be responsive to treatment)
Patient-related Large tumor burden/bulky tumors
Elevated LDH
Pre-existing renal dysfunction
Treatment-related Chemotherapy & biologic agents
Radiation therapy
Tumor Lysis Syndrome: Onset, Duration, Incidence
Onset:
Usually within 24-48 hrs after initiation of antineoplastic therapy
Duration:
May persist for 5-7 days post-therapy
Incidence:
Exact incidence unknown
Occurs mostly in patients with
Hematologic malignancies with large proliferative growth fractions
Large bulky disease (acute leukemia's, high-grade lymphomas)
Clinical Manifestations Often asymptomatic initially
Detected initial via abnormalities in blood chemistries
Signs & symptoms patients exhibit depend on extent of metabolic abnormalities
Hyperkalemia
Hyperuricemia
Hyperphosphatemia
Hypocalcemia

3
TLS: Signs & Symptoms Hyperkalemia Serum K+ >6.5 mEq/L
Early cardiac:
• Tachycardia
• EKG Changes: Prolonged QT and ST segment, lowering and inversion of T wave
Late cardiac:
• Bradycardia
• EKG Changes: Shortened QT, elevated T wave, wide QRS
• Ventricular tachycardia, ventricular fibrillation, cardiac arrest
• Nausea/vomiting
• Diarrhea
• Increased bowel sounds
• Twitching
• Muscle cramps
• Weakness
• Paresthesias
• Lethargy
• Syncope
Hyperuricemia Serum uric acid >10 mg/dl
Severe = >20 mg/dl
• Oliguria, anuria, azotemia
• Edema, hypertension
• Acute renal failure
• Chronic renal failure
• Malaise, weakness, fatigue
• Nausea, vomiting
• Flank pain, gout
• Pruritus
Gobel, B. H. (2013). In M. Kaplan (Ed.), Understanding an managing oncologic emergencies: A resource for nurses
2nd Edition (pp. 433 - 459). Pittsburgh, PA: ONS
TLS: Signs & Symptoms Hyperphosphatemia Serum PO4 >5 mg/dl
• Anuria
• Oliguria
• Azotemia
• Edema
• Hypertension
• Acute renal failure
Secondary
Hypocalcemia Serum Ca++ < 8.7 mg/dl
Neurological/Neuromuscular
•Twitching, paresthesias
• Restlessness
• Muscle cramps & weakness
• Anxiety, depression
• Carpopedal spasms
• Seizures
• Confusion
• Hallucinations
Cardiac
• Tetany
• Ventricular arrhythmias
• Prolonged QT interval, inverted T wave
• Heart block
• Cardiac arrest
Gobel, B. H. (2013). In M. Kaplan (Ed.), Understanding an managing oncologic emergencies: A resource for nurses
2nd Edition (pp. 433 - 459). Pittsburgh, PA: ONS
Prevention TLS
Hydration IV Normal saline or 5% dextrose
Begin 24 – 48 hours prior to therapy
Ensure urine output >150 – 200 ml/hr
Diuresis If urine output no maintained by hydration alone
Loop diuretics or osmotic diuretics
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 433-459; McGraw, B. (2008). CJON 12 (4); 563-565.
Prevention TLS
Allopurinol (Oral or IV) Begin 24 hour prior to therapy
Blocks uric acid production by inhibiting xanthine oxidase (liver enzyme)
Prevents uric acid precursors from converting to uric acid, ↓ risk uric acid crystallization
Rasburicase IV Converts uric acid into allantoin → very soluble compound, excreted by kidneys
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 433-459; McGraw, B. (2008). CJON 12 (4); 563-565.

4
Prevention TLS
Urinary Alkalinization Sodium bicarbonate added to IV fluid (50-100 meq/liter)
Goal: urine pH level > 7.0
Use is controversial Potential complications associated with alkalinization
Metabolic alkalosis
Calcium phosphate precipitation
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 433-459; McGraw, B. (2008). CJON 12 (4); 563-565.
TLS Preventative Measures
Monitor serial lab values
Serum potassium, phosphorous, calcium, uric acid
Renal function studies – BUN & creatinine
Frequency of monitoring
Prior to initiation of therapy
Every 8 – 12 hours during the first 48 – 72 hours of treatment
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 433-459; McGraw, B. (2008). CJON 12 (4); 563-565.
Mr. J.: 63 Year-Old Male
diagnosed with High-Grade NHL
Past Medical History: Noninsulin-dependent diabetes mellitus, supraventricular arrhythmia
Scheduled to receive 1st cycle CHOP-R chemotherapy in outpatient clinic
Cyclophosphamide (Cytoxan), doxorubicin (Adriamycin), vincristine (Oncovin), prednisone, + Rituximab (Rituxan)
Started on oral allopurinol 300 mg daily
IV hydration pre & post chemotherapy in clinic
Instructed to increase oral intake to 8 glasses fluid per day
Mr. J: Two Days Post 1st Chemo
Mr. J’s wife calls clinic and reports:
Weakness, muscle cramping, numbness & tingling of extremities
Nausea/vomiting
Decreased urine output
Swelling both feet
What could be the cause of Mr. J’s symptoms?
What should we advise Mrs. J. to do?

5
Treatment of TLS Hyperuricemia • Hydration, urinary alkalinization
• Oral allopurinol or IV allopurinol
• Rasburicase
• Hemodialysis for significant renal compromise
Hyperkalemia Mild (Potassium<6.5 mEq/L):
• Sodium polystyrene sulfonate orally or by retention enema
Potassium >6.5 mEq/L or cardiac changes:
• IV calcium gluconate or calcium carbonate
• IV sodium bicarbonate, hypertonic glucose & insulin accompanied by sodium polystyrene sulfonate
• Loop diuretics & aggressive hydration
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 433-459.
Treatment of TLS
Hyperphosphatemia • Phosphate-binding agents
• Aluminum-containing antacids
• Hypertonic glucose plus insulin
• Aggressive hydration
Hypocalcemia • Appropriate management of hyperphosphatemia
• IV calcium gluconate or calcium chloride to treat arrhythmias
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 433-459.
Mr. J’s Labs in ER (2 Days Post CHOP-R Chemotherapy)
Baseline Pre-Chemo Labs
Hgb 11.1 g/dl
Platelets 245,000/mm3
Na++ 136
K+ 4.1
BUN 45 mg/dl
Creatinine 2.2 mg/dl
Uric acid 12.6 mg/dl
ER: 2 days post-chemo
Hgb 11.2 g/dl
Platelets 200,00/mm3
Na++137 mmol/l
K+ 6.5 mmol/l
BUN 100
Creatinine 5.1 mg/dl
Uric acid 25 mg/dl
ED intake interview revealed Mr. J. had not been able to tolerate oral medications after his chemotherapy
Had not taken prescribed allopurinol
Had not taken in recommended 8 glasses fluid per day

6
TLS: Nursing Interventions
Recognize patients at risk Leukemia, lymphoma, small-cell lung cancer
Large tumors with large growth fractions or elevated LDH
Recent chemo or radiation therapy
High LDH, concurrent renal disease
Careful assessment of fluid balance
Patient teaching – strategies to reduce incidence or severity of symptoms
Maintain adequate oral fluid intake
Take Allopurinol as ordered
Signs & symptoms to report to health care team
Written instructions
Holmes Gobel, B. (2013). Tumor Lysis Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 433-459.
.
Mr. J. was treated with: 1 amp D50, 10 units regular insulin
D51/2 NS plus 100 mEq NaHCO3 at 250 cc/hr
Allopurinol 300 mg/day po
IV Lasix 40 mg
Transferred to inpatient telemetry unit with following orders:
Strict I & O Notify MD for urine output < 200 ml/hr
BID weights
Vital signs Q2 hrs
Repeat Laboratory tests in 1 hr, monitor Q4 hrs: Electrolytes, Ca++, PO4-, BUN, Creatinine, Uric Acid
Sepsis & Septic Shock
Septicemia: Invasion of blood by microorganisms
Sepsis: Systemic response to infection (vasodilation, displacement of intravascular volume)
Septic Shock: Vascular collapse caused by vasodilation, leakage intravascular volume into interstitial space
Continuum Septic Shock:
Infection Septicemia Sepsis Septic Shock
Incidence and Mortality
Incidence in cancer patients
Bacteremia or sepsis: 10-20% of patients with febrile neutropenia
Hematologic Malignancies have higher incidence than solid tumors
Hematologic malignancies: 66.4 per 1,000 hospitalized patients
Solid tumors: 7.6 per 1,000 hospitalized patients
Mortality in cancer patients
Approximately 28%, same mortality rates for hematologic malignancies & solid tumors
Courtney, et al (2007). Oncologist, 12, 1019-1026; Shelton, B.K. (2011), in Yarbro et al (eds), Cancer Nursing: Principles and Practice
(7th ed., pp 713-744). Jones & Bartlett.; Williams, et al (2004).Critical Care 8, 291-298.

7
Septic Shock: Pathophysiology Micro-organisms in blood stream release chemical mediators & hormones
Endotoxins – released by gram negative bacteria
Exotoxins – released by gram positive bacteria
Profound systemic vasodilation Hypotension
Tachycardia
Increased vascular permeability Fluid leaks from vascular space to interstitial space
Decreases circulating blood volume
Hypoxic tissues
Metabolic acidosis
Holmes Gobel, et al (2013). Sepsis & septic shock. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 287-335.
Causes of Sepsis
Bacterial organisms (most common cause of sepsis) Gram-negative bacteria (responsible for 50-60% cases of septic shock)
Escherichia coli Klebsiella pneumoniae Pseudomonas aeruginosa
Gram-positive bacteria (increased incidence due to use of vascular access devices)
Streptococcus pneumoniae Staphylococcus aureus Corynebavcterium
Other organisms Invasive fungal infections, viruses
Lewis, et al (2011). CA: A Cancer Journal for Clinicians, 61, 287-314.
Clinical Presentation: Septic Shock
Early Phase Hyperdynamic Phase (Warm)
Hypodynamic Phase (Cold)
• Normal or elevated
temperature
• Chills
• Warm, flushed skin
• Anorexia
• Normal or low BP
• Normal or elevated
temperature
• Chills and rigors
• Changes in LOC
(anxiety, restlessness,
confusion)
• Tachycardia, bounding
pulses, widening pulse
pressure
• Decreased urine output
• Subnormal temperature
• Pale, cool, and clammy
skin
• Disorientation, lethargy
• Tachycardia
• Weak, thready pulse
• Hypotension
• Anuria
Holmes Gobel, et al (2013). Sepsis & septic shock. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 287-335.
Mr. J.: Seven days post-3rd cycle chemotherapy (CHOP-R)
Wife calls outpatient clinic at 5 pm on Friday and reports husband has:
Fever
Dry cough
Discomfort with swallowing

8
Mr. J & Wife arrive in ER at 7:30 pm:
Awake, alert, anxious
Skin warm, appears flushed
↓ breath sounds lower lobes bilaterally with rales in right lung base
Oral cavity without erythema or lesions, skin intact
Dual-lumen Groshong® central venous catheter exit site without redness or drainage; however, c/o slight tenderness to area above catheter exit site
O2 sat 98% room air
Temp 1020F, HR irregular 96, RR 16, BP 126/84
Diagnostic Evaluation
CBC with differential Complete metabolic panel Serum lactate Blood cultures X 2 Cultures of body fluids
Urine, stool, throat, wounds, sputum
Chest X-Ray
Holmes Gobel, et al (2013). Sepsis & septic shock. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 287-335.
Treatment of Sepsis/Septic Shock:
Immediate initiation IV antibiotics (within 1 hour of fever onset) Fluid resuscitation
Goals: CVP: 8-12 mmHg MAP: > 65 mmHg Urine output: > 0.5 mg/kg/hr
Holmes Gobel, et al (2013). Sepsis & septic shock. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 287-335.
Treatment of Sepsis/Septic Shock
Mean arterial pressure (MAP) < 65 Vasopressor and inotropic drugs
Norepinephrine, dopamine (first line)
Phenylephrine, dobutamine, etc (second line)
Oxygen therapy
Antipyretics
Holmes Gobel, et al (2013). Sepsis & septic shock. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 287-335.

9
ER Orders for Mr. J.:
Stat CBC with differential, CXR, & cultures of blood (peripheral blood and central lines), urine, sputum, stool, CVC exit site
Stat Electrolytes, Blood Glucose, BUN, & Creatinine
Meropenum 1 gm IV stat & Q8h
Vancomycin 1000 mg IV stat & Q12h
Admit to medical unit
Neutropenic precautions
Mr. J’s Labs in ER:
• WBC 1,100/mm3
• ANC 450/mm3
• Hgb 10 g/dl
• Plt 30,000/mm3
• Glucose 201 mg/dl
• Na++ 134 mEq/l
• K+ 3.3 mEq/l
• BUN 12 mg/dl
• Creatinine 0.9 mg/dl
Nursing Assessment on Admission to Inpatient Unit: 9 PM
Extreme restlessness & anxiety
Shaking chills
Skin warm, flushed
Temp 102.40F
HR 120 irregular, bounding
RR 20, oxygen saturation 96% room air
BP 128/60
No urine output since early am
Stat IV antibiotics ordered in ER not yet given
Clinical Presentation: Septic Shock
Early Phase Hyperdynamic Phase (Warm)
Hypodynamic Phase (Cold)
• Normal or elevated
temperature
• Chills
• Warm, flushed skin
• Anorexia
• Normal or low BP
• Normal or elevated
temperature
• Chills and rigors
• Changes in LOC
(anxiety, restlessness,
confusion)
• Tachycardia, bounding
pulses, widening pulse
pressure
• Decreased urine output
• Subnormal temperature
• Pale, cool, and clammy
skin
• Disorientation, lethargy
• Tachycardia
• Weak, thready pulse
• Hypotension
• Anuria
Holmes Gobel, et al (2013). Sepsis & septic shock. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 287-335.

10
Nursing Management Sepsis
Frequent vital signs & assessments
LOC, skin color & temp, lungs
Maintain oxygenation
Oxygen therapy & ventilatory support
Administer IV fluids,
Expand intravascular volume (fluid resuscitation)
Monitor I & O
Antipyretics
Assess for fluid overload
Mr. J: Nursing Assessment 9:45 pm
Disoriented, lethargic
Skin pale, cool
↓ breath sounds lower lobes bilaterally with diffuse bilateral rales, hemoptysis
Abdomen distended, rebound tenderness
No urine output
Oozing blood from venipuncture sites
HR 136 irregular, weak
RR 28 labored, oxygen saturation 88% room air
BP 88/50
Clinical Presentation: Septic Shock
Early Phase Hyperdynamic Phase (Warm)
Hypodynamic Phase (Cold)
• Normal or elevated
temperature
• Chills
• Warm, flushed skin
• Anorexia
• Normal or low BP
• Normal or elevated
temperature
• Chills and rigors
• Changes in LOC
(anxiety, restlessness,
confusion)
• Tachycardia, bounding
pulses, widening pulse
pressure
• Decreased urine output
• Subnormal temperature
• Pale, cool, and clammy
skin
• Disorientation, lethargy
• Tachycardia
• Weak, thready pulse
• Hypotension
• Anuria
Holmes Gobel, et al (2013). Sepsis & septic shock. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 287-335.
Nursing Interventions
Neutropenic patients with fever Must be assessed immediately
Started on broad spectrum antibiotics
Monitor for sequelae of septic shock Frequent vital signs
Assess tissue perfusion (skin color, temperature, capillary refill)
Lung assessments
I & O – report urine output < 30cc/hr
Monitor for symptoms of DIC
Monitor response to medical treatment Assess for fluid overload
Monitor lab values, especially renal function & culture reports
Infection control measures
Holmes Gobel, et al (2013). Sepsis & septic shock. In Kaplan, M (Ed). Understanding and managing oncologic emergencies:
A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 287-335.

11
Possible Complications of Sepsis/Septic Shock
DIC
Multiple organ dysfunction syndrome
Death
Disseminated Intravascular Coagulation (DIC)
Syndrome of:
Thrombus formation (clotting)
Simultaneous Hemorrhage
Caused by over stimulation of normal coagulation processes
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.
Pathophysiology DIC
Paradox of DIC: bleeding & clotting
Triggered by: Intrinsic coagulation system activation (damage to blood vessels)
Transfusion reactions
Endotoxins/Septicemia
Sickle Cell Disease
Malignant hypothermia
Extrinsic coagulation system activation (tissue injury) Obstetrical Conditions
Extensive surgery
Crush injuries
Malignancies
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.
DIC in the Oncology Population:
Malignancy Induced
Acute Promyelocytic Leukemia (APL)
Procoagulant material release by granules of the immature promyelocyte initiates clotting cascade
Occurs in 85% patients with APL
Solid Tumors (adenocarcinomas)
Lung, pancreas, prostate, stomach, colon, ovary, gall bladder, breast, kidney
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.

12
Other Causes DIC (Oncology Population)
Chemotherapy May induce DIC by damaging tumor, normal cells, or endothelium causes release procoagulant material
Large tumor burden/large cell kill release granule procoagulant from dead cells into systemic circulation
Infection/sepsis Especially gram negative bacteria sepsis (release of endotoxin)
Hemolytic transfusion reactions Rupture of RBC’s platelet aggregation, release platelet factors that initiate clotting cascade
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.
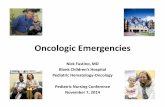
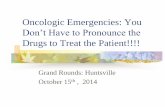
UNDERLYING
DISEASE OR
CONDITION
STIMULATION OF
COAGULATION
CASCADE
WIDESPREAD FIBRIN
CLOT FORMATION
ACTIVATION OF
FIBRINOLYSIS
MICROTHROMBI
DEPOSITS
THROUGHOUT
MICROCIRCULATION
CONSUMPTION OF:
PLATELETS
FIBRINOGEN
PROTHROMBIN
PRODUCTION OF:
FIBRIN SPLIT
PRODUCTS
tPA
ISCHEMIC TISSUE
DAMAGE
SYMPTOMS OF ORGAN
DYSFUNCTION
BLEEDING
Pathophysiology of DIC
Types of DIC
Acute DIC
Medical emergency
Chronic DIC
Produces coagulation abnormalities, with or without clinical manifestations, that can be medically managed
Most cases of chronic DIC due to underlying malignancy
Laboratory Values in DIC Laboratory Test Result Comments or Cause
Prothrombin Time (PT) Prolonged Nonspecific in DIC
Activated Partial Thromboplastin time (APPT)
Prolonged Nonspecific in DIC
International normalized ratio (INR)
Prolonged Nonspecific in DIC
Fibrin Degradation Products Elevated Indicates breakdown of fibrin & fibrinogen
D-Dimer Elevated Indicates hyperfibrinolysis
Platelet Count Decreased Platelets consumed
Fibrinogen Decreased Fibrinolysis; decreases very slowly only in severe DIC
Antithrombin Decreased Anticoagulant activity inhibited Accelerated coagulation
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.

13
DIC Clinical Presentation
Decreased tissue/organ perfusion Brain, CV, Lungs, Kidney, GI Tract, Skin
Decreased platelet count Petechiae, ecchymosis
Hemorrhage Tachycardia, hypotension
Tachypnea
Overt bleeding
Occult bleeding
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.
Mr. J: Nursing Assessment 9:45 pm
Disoriented, lethargic
Skin pale, cool
↓ breath sounds lower lobes bilaterally with diffuse bilateral rales, hemoptysis
Abdomen distended, rebound tenderness
No urine output
Oozing blood from venipuncture sites
HR 136 irregular, weak
RR 28 labored, oxygen saturation 88% room air
BP 88/50
Mr. J’s Labs at 10:00 pm
Lab 7:30 pm 10:00 pm Normal
Hemoglobin 10 g/dl 8.9 g/dl 14-18 g/dl male
Platelets 30,000/mm3 12,000/mm3 150,000 – 400,000/mm3
Fibrinogen 96 mg/dl 170 – 410 mg/dl
PT 15.8 sec 11.3 – 13.1 sec
Fibrin Degradation Products
60 mcg/ml <10 mcg/mL
Treatment of DIC
Early recognition & treatment of underlying disorder
Chemotherapy for malignancy
Antibiotics for infection
Correct hypoxia
Oxygen to maintain saturation >95%
Correct hypovolemia, hypotension, & acidosis
NS until type & cross match completed & blood available
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.

14
Treatment of DIC Stop the micro clotting to maintain perfusion & protect vital function
IV Heparin
Antithrombin III (inhibits action of thrombin)
Stop the bleeding
Pressure to active sites of bleeding
Blood products (FFP, cryoprecipitate, platelets, red blood cells)
Antifibrinolytic agents (EACA)
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.
Nursing Interventions
Prevent severity of symptoms
Direct pressure sites of bleeding, pressure dressings, sand bags
Monitor for progression DIC
Worsening vital signs, hypotension, anuria, ’s LOC
Monitor response to therapy
Sites & amounts of bleeding
Changes in lab values
Assess tissue perfusion parameters – color, temperature, peripheral pulses
Patient Teaching
Avoid ASA or NSAID’s (effects on platelet aggregation)
Signs and symptoms of DIC (bleeding and/or clotting)
Kaplan, M. (2013). Disseminated Intravascular Coagulation. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 69 – 102.
Hypercalcemia of Malignancy (HCM)
Metabolic disorder, in cancer patients, results from increased bone resorption
Serum calcium level >12-14 mg/dl (normal serum calcium 9-11 mg/dl)
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.
Normal Physiology
Normal levels Ca++ regulated by: Parathyroid gland (production of parathyroid hormone)
GI tract (absorption of Vitamin D)
Kidneys (excretion)
Ca++ levels below normal: Parathyroid stimulated to produce parathyroid hormone
Acts on bone release of calcium (bone resorption) into circulation
Ca++ levels above normal: Kidneys excretion of calcium
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.

15
HCM: Etiology Tumor-induced bone breakdown releasing Ca++ into bloodstream
Solid tumors of squamous cell origin – potential to produce parathyroid hormone-related protein that stimulates Ca++
release from bone Lung, breast, prostate, head & neck, esophagus, kidney
Decreased ability of kidneys to clear calcium from the blood
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.
Incidence of Hypercalcemia of Malignancy
Occurs in approximately 30% of cancer patients
Most often in advanced stages of disease
50% of patients die within 30 days of
diagnosis
Survival beyond 6 months is rare
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.
Incidence of Hypercalcemia of Malignancy
Malignancy Incidence of Hypercalcemia
Incidence of Bone Metastasis
Breast cancer with metastasis 30% - 40% 65% - 75%
Multiple myeloma 20% - 40% 70% - 90%
Squamous cell carcinoma of lung 12.5% - 35% 30% - 40%
Squamous cell carcinoma of head & neck
2.9% - 25% Uncommon
Renal cell carcinoma 3% - 17% 20% - 25%
Non-Hodgkin’s Lymphoma 14% - 33% Rare
T-Cell Lymphoma 50% Rare
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.
Hypercalcemia: Clinical Presentation
Clinical signs & symptoms related to rapidity of onset & serum calcium level
Corrected total serum calcium (TSC) needs to be calculated if albumin is low
Corrected Serum Calcium (mg/dl)=
Measured serum Ca++ + (4.0 – serum albumin g/dl) X 0.8
**Normal Serum Ca++ = 8.5 – 10.5 ml/dl

16
Signs and Symptoms of Hypercalcemia of Malignancy
System Early Late
Neurologic Drowsiness, lethargy, weakness, restlessness, irritability, confusion, cognitive dysfunction, disorientation
Seizures Stupor Coma
Renal Polyuria, polydipsia, nocturia, dehydration, kidney stones, renal insufficiency
Renal failure
GI Anorexia, nausea, vomiting, constipation, vague abdominal pain, weight loss, peptic ulcers
Atonic ileus Obstipation
Cardiovascular EKG changes (slowed conduction, Prolonged PR, wide QRS, short QT, short ST), sinus bradycardia
Heart block Cardiac arrest
Musculoskeletal Muscle weakness, fatigue, hypotonia, bone pain
Ataxia Pathologic fractures
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.
Hypercalcemia: Treatment
Depends on serum calcium level & patient symptoms:
Ca++ <12 ml/dl & asymptomatic
observe carefully & treat as outpatient
Ca++ 12-15 ml/dl & asymptomatic
requires specific but non-urgent treatment
Ca++ >15 ml/dl & symptomatic
requires emergent treatment
Hypercalcemia: Treatment
Treat the cancer – tumor control or reduction is the only long-term measure for reversing hypercalcemia
Hydration & forced diuresis Oral fluids (3-4 L/day)
IV Saline Initial: NS 100-300 ml/hr
Maintenance: 2.5 – 5L/day
Loop diuretics (furosemide)
Mobilization
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.
Agents to Inhibit Bone Resorption
Agent Mechanism of Action Dosing
Bisphosphonates
• Pamidronate (Aredia) • Inhibits osteoclast activity
IV: 60-90 mg over 2 hrs May repeat after 7 days
• Zoledronate (Zometa) • Inhibits osteoclast activity
IV: 4 mg over 15 minutes May repeat after 7 days
Calcitonin • Direct inhibition of osteoclast receptors
• Increases renal calcium excretion
SC or IM: 4-8 IU/kg every 6-12 hours for 2 days
Gallium nitrate (Ganite) • Used when HCM resistant to bisphosphonates
• Inhibits osteoclast activity
IV: 200 mg/m2/day continuous for 5 days
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.

17
Hypercalcemia Treatment Dietary recommendations
Maintain salt intake
Dietary calcium restrictions not necessary
Medications to avoid
Thiazide diuretics
NSAIDS, H2 receptor antagonists
Vitamins A & D
Parenteral/enteral solutions with calcium
Corticosteroids
Therapy of choice multiple myeloma or lymphomas
Inhibits vitamin D conversion to calcitriol
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.
Nursing Interventions
Recognize early signs & symptoms
Careful monitoring of patients taking: Thiazide diuretics (inhibits calcium excretion)
Digitalis preparations (action potentiated in hypercalcemic states)
Measures to decrease calcium removal from bone: Ambulation, weight bearing, ROM, isometric exercises
Careful assessment & monitoring Fluid balance & renal function
GI motility
Cardiac Status
Mental status
Kaplan, M. (2013) Hypercalcemia of malignancy. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 103 – 155.
Mr. C: Hypercalcemia
62-year-old male diagnosed with stage IV squamous cell cancer of lung CT of spine showed metastatic disease in thoracic & lumbar spine at T1 & L3 vertebrae Based on extent of disease & poor pulmonary function, Mr. C. was not a surgical candidate. Scheduled for second course of palliative chemotherapy Also receiving concurrent radiation for the spinal metastasis
2nd Cycle Chemotherapy
Wife consults with nursing staff & reports:
Concern re: husband’s ↑ forgetfulness,
wonders if confusion is because of recent change in pain medication (oxycodone)
Husband experiencing more fatigue than usual (4-5 naps per day)

18
Mr. C’s Labs: 2nd Cycle Chemotherapy
WBC 4,500/mm3
Hgb 11.2 g/dl
Hct 35%
Platelets 119,000/mm3
Serum Ca++ 10.4
Creatinine 1.1 mg/dl
BUN 19 mg/dl
Albumin 2.3 g/dl
Corrected Serum Ca++
Mr. C’s : Ca++ 10.4 Albumin 2.3
Corrected Serum Calcium =
Measured serum Ca++ + (4.0 – serum albumin) X 0.8
= 10.4 + (4.0 – 2.3) X 0.8
= 10.4 + 1.7 X 0.8
= 10.4 + 1.36
= 11.78 (rounded up to 11.8)
Mr. C’s 3rd Cycle Chemotherapy
Wife reports confusion improved for 1st two weeks following last chemotherapy
Past week, he has been increasingly forgetful, depressed, and fatigued (stayed in bed last 2 days)
Mr. C’s Lab Trends
Lab Test 2nd Chemo Visit 3rd Chemo Visit
WBC 4,500/mm3 2,200/mm3
Hgb 11.2 d/dl 10.4 g/dl
Hct 35% 29%
Platelet count 119,000/mm3 102,000 mm/3
BUN 19 mg/dl 28 mg/dl
Creatinine 1.1 mg/dl 1.5 mg/dl
Serum calcium 10.4 mg/dl 12.8 mg/dl
Albumin 2.3 g/dl 2.1 g/dl

19
Corrected Serum Ca++
Mr. C’s : Ca++ 12.8 Albumin 2.1
Corrected Serum Calcium =
Measured serum Ca++ + (4.0 – serum albumin) X 0.8
= 12.8 + (4.0 – 2.1) X 0.8
= 12.8 + 1.9 X 0.8
= 12.8 + 1.52
= 14.32 (rounded to 14.3)
The best immediate treatment to correct Mr. C’s calcium & symptoms is:
a. Hydration & Bisphosphonate (anti-Resorptive therapy) infusion
b. Chemotherapy administration & corticosteroids
c. Growth factor to improve fatigue and minimize myelosuppression
d. Hydration & observation
The best immediate treatment to correct Mr. C’s calcium & symptoms is:
a. Hydration & Bisphosphonate (anti-Resorptive therapy) infusion
b. Chemotherapy administration & corticosteroids
c. Growth factor to improve fatigue and minimize myelosuppression
d. Hydration & observation
Structural Oncologic Emergencies
Spinal Cord Compression
Superior Vena Cava Syndrome (SVCS)
Increased Intracranial Pressure (ICP)
Cardiac Tamponade
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.

20
Spinal Cord Compression
Compression of spinal cord Direct tumor pressure on cord
Tumor invasion of the vertebral column causing collapse & pressure on cord
Compression causes: Edema
Inflammation
Mechanical compression
Leads to: Direct neural injury to cord
Vascular Damage
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.
Incidence Occurs in approximately 5-14% of general cancer population
Highest incidence in solid tumors that metastasize via hematogenous routes to bone in the spine
Most common: Breast
Lung
Prostate
Lymphoma
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.
Cancers Associated with Risk of Spinal Cord Compression Frequency Cancer Type
Most Common • Breast (15% - 20%) • Lung (15% - 20%) • Prostate (15% - 20%) • Multiple Myeloma (10% - 15%) • Unknown primary (10%) • Renal cell carcinoma (5% - 10%) • Non-Hodgkin lymphoma 5% - 10%) • Hodgkin disease (5%)
Less Common • GI malignancies • Soft Tissue sarcoma • Thyroid cancer • Neuroblastoma
Uncommon • Melanoma • Uterine, cervical, bladder cancers • Leukemia
Rare • Head and neck cancer, brain, pancreatic, liver, ovarian, testicular, esophageal cancer
Clinical Presentation: Back Pain
Most common presenting symptom
Occurs in 90% of patients
Precedes other signs and symptoms (e.g. neurological) by weeks to months
Median time from onset to pain to diagnosis of spinal cord compression: 2 months
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.

21
Back Pain Associated with Spinal Cord Compression
Can occur at any level of the spine
Can take several forms: Local (near the site of compression)
Radicular (distributed along dermatones)
Referred (in a non-radicular distribution)
May be a combination of all 3 types
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.
Progression of Symptoms
Time Frame
Early
Late
Signs & Symptoms
• Pain
• Motor weakness or gait changes
• Sensory Loss
• Numbness, tingling, sensory changes
• Autonomic Dysfunction
• Constipation and/or bladder retention
• Bowel and/or bladder incontinence
• Paralysis
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.
Diagnostic Tests
MRI Gold standard for diagnosis
Accurate, sensitive, and specific diagnostic tool for spinal cord compression
Other Diagnostic Tests Spinal x-rays
CT scan
Myelography – reserved for patient’s who can’t undergo MRI
Bone Scan and/or PET Scan
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.
Treatment of Spinal Cord Compression
IMMEDIATE & aggressive
Corticosteroids – initial supportive treatment
High-dose steroids to spinal cord edema & inflammation
High-dose loading with Dexamethasone (up to 100 mg IV loading dose) followed by tapering doses over several days
Radiation therapy (radiosensitive tumors)
In general, a course of radiation with a total of 30 Gy in 10 fractions
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.

22
Treatment of Spinal Cord Compression
Surgery Laminectomy (no longer typically used)
Anterior vertebral body resection with stabilization
Vertebroplasty
Kyphoplasty
Chemotherapy Rarely used in acute management
Response to treatment slow & unpredictable
Bisphosphonates Can effectively reduce pain and other skeletal complications of vertebral metastasis
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.
Nursing Interventions
Early recognition Thorough assessment of neck & back pain in high risk patients
Neurological assessments Mental status Cranial nerves Motor & sensory system Reflexes
Pain Management Mobility and safety issues Skin care Bowel and Bladder function Rehabilitation & palliative care
Kaplan, M. (2013). Spinal Cord Compression. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 337 – 383.
Superior Vena Cava Syndrome
Obstruction of superior vena cava that impairs venous drainage (above the obstruction)
Obstruction venous return from head, neck, upper arms, upper thorax impaired
Venous pressure increases
Cardiac output decreases
Shelton, B. K. (2013). Superior Vena Cava Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 385 – 410.
Incidence Occurs in 3 – 4% of Oncology Population
Malignant conditions: Majority of cases (70% - 95%) related to underlying malignancy
Most common: Small cell & non-small cell lung cancers
Non-Hodgkin lymphoma (high-grade)
Less common: Esophageal cancer
Thyroid cancer
Breast cancer, thymoma, mesothelioma, leukemia
Non-Malignant conditions: Intraluminal thrombus formation
Mediastinal fibrosis or benign mass
Shelton, B. K. (2013). Superior Vena Cava Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 385 – 410.

23
Clinical Presentation
Gradual onset (rarely occurs rapidly)
Symptoms vary depending on extent of obstruction, location, collateral circulation
Shelton, B. K. (2013). Superior Vena Cava Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 385 – 410.
Early/Common Physical Signs & Symptoms
Dyspnea
Facial and neck swelling (occurs when supine, subside after arising)
Sensation of fullness in head
Cough
Arm Swelling
Chest pain
Venous distention of neck & chest wall
Cyanosis
Shelton, B. K. (2013). Superior Vena Cava Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 385 – 410.
Late Physical Signs & Symptoms
Cyanosis of face & upper torso
Decreased or absent peripheral pulses
CHF
Decreased BP
Chest pain
Mental status changes
Tachypnea
Tachycardia
Engorged conjunctivae
Visual disturbances
Syncope
Hoarseness
Stridor
Shelton, B. K. (2013). Superior Vena Cava Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 385 – 410.
Diagnostic Evaluation Chest X-ray
MRI
Contrast-enhanced CT
Tissue diagnosis

24
Treatment SVCS
Based on etiology, severity of symptoms
Relieve obstruction & control underlying disease
Radiation therapy Gold standard for non-small cell lung cancer
Chemotherapy Primary treatment for chemo-sensitive malignancies
Small cell lung cancer
Non-Hodgkin Lymphoma
Surgical Intervention Stent placement or SVC bypass
Chronic or recurrent SVCS
Thrombolytic therapy SVCS caused by intraluminal thrombus)
Shelton, B. K. (2013). Superior Vena Cava Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 385 – 410.
Nursing Interventions Assess for signs & symptoms in patients at risk
Non-small cell lung cancer, small cell lung cancer, non-Hodkin lymphoma
Central venous catheter access devices
Interventions to relieve symptoms
Elevate HOB, avoid supine position & elevation of lower extremities
Avoid venipuncture, BP, IV therapy upper extremities
Monitoring response to treatment Assess for progressive respiratory distress or edema
Monitor tolerance of activities
Monitor fluid status(over hydration exacerbates symptoms)
Assess CNS (LOC, mental status change, visual changes, headache)
Shelton, B. K. (2013). Superior Vena Cava Syndrome. In Kaplan, M (Ed). Understanding and managing oncologic
emergencies: A resource for nurses, 2nd ED. ONS, Pittsburgh, PA. pp: 385 – 410.
Sepsis is a common cause of disseminated intravascular coagulation (DIC). Which of the following conditions most accurately describes how sepsis causes DIC?
a. Sepsis causes viruses to thrive, and viruses cause DIC
b. Endotoxins released from bacteria activate the coagulation cascade
c. Sepsis and bleeding occur simultaneously in patients who are immunosuppressed
d. Antiangiogenesis factors are released during periods of sepsis, which leads to DIC
Which of the these statements is not true in regards to hypercalcemia in malignancy?
a. It is a rare complication
b. Early manifestations of the syndrome are insidious including fatigue, muscle weakness, and depression and easily overlooked as manifestations of the disease.
c. Bisphosphonates are frequently used in the treatment of malignancy induced hypercalcemia because of their ability to interfere with osteoclastic activity
d. A complication of malignancy induced hypercalcemia include decreased GFR and acute kidney failure, neuropsychiatric disturbances, and cardiovascular complications.