On the Safe Use of Microwave and Shortwave Diathermy Units
11
On the Safe use of Microwave and Shortwave Diathermy Units Dipthermy is a common treatment modality used> to relieve pain through localized heating. This paper briefly discusses the mechanisms through which heat is generated in tissue and the absorption characteristics of the applied electromagnetic radiation. The adverse effects of this radiation are reviewed with particular emphasis on the current exposure limits for operators and non-patients in the vicinity of diathermy devices. The newly introduced codes of practice for the 'Safe Use of Shodwave (Radiofrequency) andlAicrowave Diathermy'are also discussed. 'i VINCENT DELPIZZO Vincent Delpizzo, Ph.D., is a physicist in the non- ionizing radiation group of the Australian Radiation Laboratory and is involved in research on the health hazards of electromagnetic radiation. KENNETH HENRY JOYNER Ken Joyner,Ph"D., is Principal Scientist at the Telecom Research Laboratories where he is con- ducting research in the interaction of electromag- netic radiation with matter. Diathermy is a form of therapy which utilizes electromagnetic radia- tion to induce heat inside the patient's body. This leads to increased blood circulation which is believed to induce faster healing. Diathermy is used ina variety of conditions including sprains and strains, muscle and tendon tears, chronic rheumatoid arthritis, tenosy- c novitis, bursitis and synovitis. The medical efficacy of this treat- ment ,has 'been the subject of some controversy, while the potential haz- ards posed by the high power,(> 200W) electromagnetic radiation emitted by a diathermy machine are certainly not to be neglected. In a Canadian survey of shortwave and microwave medical devices (DHW 1980) only 54.3 per cent of the short- wave diathermy operators were de- scribed as trained (38.5 per cent of the respondents provided no reply while 7.3 per cent admitted being untrained). The. same survey indicated that 8 per cent of the treatments involved irra- diation of the pelvis (including treat- ment of the reproductive and urinary" systems) and a similar percentage in- volved irradiation of the head. Although similar data is not avail- able for Australia, reports of unwise and potentially hazardous practices in the use of diathermy have caused dis- quiet among health regulatory author- ities and have prompted the National Health and Medical Research Council to issue a uniform code of practice for the safe use of diathermy machines. The code was produced in two slightly different versions, one for microwave and one for shortwave (radiofre- quency)'units. Both codes are included in Appendices AandB of this article. A similar code,has been established in Canada (DHW 1983). Shortwaves and Microwaves Technically, the term rediofrequency radiation refers to that portion of the frequency spe .. ctrum useful for radio- communications ie 10kHz to 300 GHz. However, it is not uncommon to fur- ther divide this frequency range into radiofrequency (10 kHz to 300 MHz) and microwave (300 MHz to 300 GHz) regions. This latter convention has been adopted for this paper and the codes. Because of the competing demands of various microwave and radiofrequency users, specific bands have been allo- cated by the International Telecom- municationUnion for industrial, scien- tific and medical (ISM) applications. In Australia diathermy' units are al- lowed to operate in only two of the ISM bands, namely the microwave band of 2450 MHz (wavelength = 122 mm) and the shortwave band of 27.12 MHz (wavelength = 11.1 m). The absorption properties and the methods of application associated with these two frequencies are considerably different and therefore the heating mechanisms and, more importantly, the resulting heating patterns vary. The interactions of electromagnetic fields with tissue can be considered on a macroscopic or microscopic level. On the microscopic level, three basicma- chanisms underlie the interactions. These include: (1) the orientation of electric dipoles that already exist in the atoms and molecules in the tissue; (2) polarization of atoms and mole- cules to produce electric dipoles; and 152 The Australian Journal of Physiotherapy. Vol. 33, No.3, 1987
-
Upload
kenneth-henry -
Category
Documents
-
view
215 -
download
1
Transcript of On the Safe Use of Microwave and Shortwave Diathermy Units

On the Safe use of Microwave and Shortwave DiathermyUnits
Dipthermy is a common treatment modalityused> to relieve pain through localized heating.This paper briefly discusses the mechanismsthrough which heat is generated in tissue andthe absorption characteristics of the appliedelectromagnetic radiation. The adverse effectsof this radiation are reviewed with particularemphasis on the current exposure limits foroperators and non-patients in the vicinity ofdiathermy devices.
The newly introduced codes of practice forthe 'Safe Use of Shodwave (Radiofrequency)andlAicrowave Diathermy'are also discussed.
'i
VINCENT DELPIZZO
Vincent Delpizzo, Ph.D., is a physicist in the nonionizing radiation group of the Australian RadiationLaboratory and is involved in research on the healthhazards of electromagnetic radiation.
KENNETH HENRY JOYNER
Ken Joyner,Ph"D., is Principal Scientist at theTelecom Research Laboratories where he is conducting research in the interaction of electromagnetic radiation with matter.
Diathermy is a form of therapywhich utilizes electromagnetic radiation to induce heat inside the patient'sbody. This leads to increased bloodcirculation which is believed to inducefaster healing. Diathermy is used inavariety of conditions including sprainsand strains, muscle and tendon tears,chronic rheumatoid arthritis, tenosy- c
novitis, bursitis and synovitis.The medical efficacy of this treat
ment ,has 'been the subject of somecontroversy, while the potential hazards posed by the high power,(> 200W)electromagnetic radiation emitted by adiathermy machine are certainly not tobe neglected.
In a Canadian survey of shortwaveand microwave medical devices (DHW1980) only 54.3 per cent of the shortwave diathermy operators were described as trained (38.5 per cent of therespondents provided no reply while7.3 per cent admitted being untrained).The. same survey indicated that 8 percent of the treatments involved irradiation of the pelvis (including treatment of the reproductive and urinary"systems) and a similar percentage involved irradiation of the head.
Although similar data is not available for Australia, reports of unwiseand potentially hazardous practices inthe use of diathermy have caused disquiet among health regulatory authorities and have prompted the NationalHealth and Medical Research Councilto issue a uniform code ofpractice forthe safe use of diathermy machines.The code was produced in two slightlydifferent versions, one for microwaveand one for shortwave (radiofrequency)'units. Both codes are includedin Appendices AandB of this article.A similar code, has been established inCanada (DHW 1983).
Shortwaves and Microwaves
Technically, the term rediofrequencyradiation refers to that portion of thefrequency spe..ctrum useful for radiocommunications ie 10kHz to 300 GHz.However, it is not uncommon to further divide this frequency range intoradiofrequency (10 kHz to 300 MHz)and microwave (300 MHz to 300 GHz)regions. This latter convention has beenadopted for this paper and the codes.
Because of the competing demands ofvarious microwave and radiofrequencyusers, specific bands have been allocated by the International TelecommunicationUnion for industrial, scientific and medical (ISM) applications.In Australia diathermy' units are allowed to operate in only two of theISM bands, namely the microwaveband of 2450 MHz (wavelength = 122mm) and the shortwave band of 27.12MHz (wavelength = 11.1 m).
The absorption properties and themethods of application associated withthese two frequencies are considerablydifferent and therefore the heatingmechanisms and, more importantly, theresulting heating patterns vary.
The interactions of electromagneticfields with tissue can be considered ona macroscopic or microscopic level. Onthe microscopic level, three basicmachanisms underlie the interactions.These include:(1) the orientation of electric dipoles
that already exist in the atoms andmolecules in the tissue;
(2) polarization of atoms and molecules to produce electric dipoles;and
152 The Australian Journal of Physiotherapy. Vol. 33, No.3, 1987

The Safe use of Microwave and Shortwave
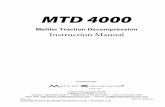
Figure 1: Inductive (a) and capacitive (b) applicators
(3) displacement or drift of conduction('free') electrons and ions in tissue.
Heat can be generated in tissue ineach of these three interactions. In thefirst .two cases the heat is generatedthrough .friction associated with themovement of atoms and molecules followin.g~the time variation of the electricfield. I'Q the case of displacement ofconduction charges, the collision ofelectrons and ions with atoms and molecules of the tissue produce heat. Notethat it is only the internal electric fieldthat transfers energy to the tissue.However,magnetic fields will induceelectric fields in tissues thereby generatingheat. Thus both electric and magnetic fields produced by the diathermyapplicator are important with respectto the generation of heat.
All three of the above interactionsare described by the macroscopic pr,operty of tissue, called. the 'complexpermittivity', which represents thedielectric constant and loss factor ofthe tissue. The complex permittivity oftissue is a function of frequency and,as a result, the propagation and attenuation of electromagnetic waves arealso dependent on th~ frequency(Schwan .1954, Schwan 1970).
In shortwave diathermy the patientis made part of the electrical circuit ofthe generator by using either an inductive coil (Figure la) or a capacitortype applicator (Figure Ib). A variablecapacitor in the unit is tuned· to matchthe generator with the patient-applicator circuit, thus.achieving maximumpower transfer.
If a capacitive applicator is used, thepatient is subjected to an oscillatingelectric field which causes molecules inthe tissue to vibrate and produce heat.In the case of the inductive applicator,primary heating is due ·to eddy currentsinduced by the oscillating magneticfield. The heating pattern is determinedby th.e type of applicator, by its sizeand by its position relative to thepatient.
For a microwave unit, the wavelength of the radiation (122mm) ismuch smaller than the overall dimen-
a
sians of the patient and therefore thedirectionaI.properties .of the radiationare important to its operation. Themicrowave radiation is emitted by asmall antenna and directed towards thearea of treatment by a suitably shapedreflector. The antenna and the reflectorconstitute the applicator. Differenttypes of applicators can be used withthe same unit to obtain different heatingpatterns.
The heating effect of microwaves isdue to energy dissipated by the watermolecules in the tissues as they vibrateto follow the oscillations of the electricfield. The heating pattern is determinedby the penetration characteristics of theradiation and by the type ofapplicator.Like light, microwaves can be transmitted t reflected, refractedandabsorbed by different media. Reflectionoccurs at the interface between twomedia through which the radiationpropagates at differing velocities (eg airand skin, muscle and fat) (Schwan1954).
Absorption is the transfer of energyfrom the electromagnetic wave to the
medium which it is penetrating. Tissueshaving a high water content absorbmore than tissues such as fat or bone.Within a given medium absorption depends on the electrical properties ofthe medium, on the frequency of theradiation and the distance travelled bythe wave. In general, in the radiofrequency range, absorption increases withincreasing frequency. At the frequencyof 2450 MHz, the amplitude of theelectric field falls by approximatelytwo-thirds after propagating for 20 mminto tissues of high water content. Asthe power of the radiation is .proportional to the square of the electric field,only about 10 per cent of the power istransmitted past that distance.
The rate· at which energy is impartedto a given mass of tissue is expressedby the specific absorption rate (SAR)which is measured in WIkg. The SARis calculated by the relationship (Wittersetol 1979):
4.19 x lcrC TSAR
t
The Australian Journal of· Physiotherapy. Vol. 33, No.3, 1987 153

The Safe use of Microwave and Shortwave
Occupationallyexposed *
whereC specific heat of tissueT temperature rise in tissuet time of energy deposition in the
tissue.
The SAR can also be expressed interms of the electrical properties of theabsorbiqg tissue (Osepchuk 1979):
--L . . 2SAR = .2p W€o € tan oEin
Wherep is the mass density of the body,
in kg/m3
fa is the permittivity of free space,in farads/m
€ is the relative dielectric constanttan 0 is the loss tangentw is the radian frequency given by
w= 211'"fEm is the electric field in volts/m at
the point in ·the body.
Experimental and clinical researchindicates that therapeutic responses willoccur as a result of elevating tissuetemperatures in the range 41° to 45°CrequiringSARs from 50 to 235 W/kg(U.S.A. Federal Register 1980) in thetreatment area (Guy etal 1974).
Because of the presence of differentlayers of tissue with different physicalproperties and because of the resultingcombined effects of absorption and re..flection, it is exceedingly difficult toaccurately estimate the dose ofradiation delivered to a specific organ. Inpractice the only indicator available tothe therapist is the thermal sensationexperienced by the patient and eventhis may not reflectacturately the pos...sible presence, for example, .of 'hotspots' in an area which does not pos..sess an adequate number of thermalreceptors. The power meter incorporated in the unit's console indicatesonly the" power emitted by the generator, not that delivered to the patient.
potentially hazardous, not only to thedirect user, but also to other personswho may be unintentionally exposed(WHO 1981).
At the Warsaw International Symposium on biological effects and healthhazards of microwave radiation in 1973it was ag!eed that, from the point ofview of the biological effects, microwave· power densities could be dividedinto the followiIfgranges:-High power densities, greater than
10 roW/cm2 at which distinct thermal effects predominate.
- Medium power densities,between1 mW/cm2 and 10 mW/cm2,whereweak but noticeable thermal effectsexist.Low power densities, belowlroW/ cm2
, where thermal effectsdo not appear to exist but othereffects have been reported. The exact nature of these non-thermal effects continues to be the subject ofmuch controversy as they are subjective in nature and difficult toquantify (see, .for example: Symposium on Health Aspects of Nonionising Radiation 1979, Steneck1984).
Although no formal agreement hasbeen reached, a similar classificationmay be applied to the shortwave fre"quency of 27.12 MHz.
The thermal effect of electromagnetic. radiation which has already beendiscussed may lead toa number ofdetrimental effects from lesions .inspecific organs to gross thermal stressfrom hyperthermia. The severity of the
"Table 1:Maximum permissible exposure .Iimits
Frequency(MHz)
effect depends on many factors including ·the nature of the organ exposed,the intensity and duration of the exposure, on the size and the health condition of the subject exposed (SAA1985).
For the operators and members ofthe public, including other patients, receptionistsetc., any effect induced inthem is unwanted and therefore theexposure must be limited to the levelsprescribed by the Australian ·StandardAS2772(SAA 1985) and reported inTable 1. Occupationally exposed individuals are persons exposed to radiationas a direct consequence of theiremployment, which in this case meansthe operators of diathermy units.
Surveys of shortwave diathermy de...vices in the USA (Ruggera 1980) .andCanada (Stuchlyet a/1982) and resultsof measurements performed by the au...thorshave shown that, in general, ifthe operator remains approximately 1mfrom the applicator and, in particular,O.5m from the cables his or her exposure will be within the recommendedlimits.
However, exceptions to this rule havebeen reported. It was shown in theUSA survey (Ruggera 1980) that oneshortwave diathermy device producedunwanted power densities well in excessof the recommended limit at a distanceof 1 m from the applicator. Althoughthe authors of that survey did not commenton that result, other diathermydevices surveyed, of the same modeland used for the same· treatment mo...dality, produced much lower power
General
* ie persons exposed as a consequence of their occupation,in this casethe operator.
Personnel Exposure
Exposure LimitsLike many sources of electromag-;
netic radiations, diathermy devices are
27.12
2450
1.22 mW/cm2 0.24 ·mW/cm2
0.2 mW/cm2
154 The Australian Journatof Physiotherapy. Vol. 33, No.3, 1987

The Safe use of Microwave and Shortwave
Figure 2: Simultaneous use of more than one unit increases the chance ofoverexposure of the operator. The radiation levels reported in the figures wereobtained during normal therapeutic use of the machines.
The occupational exposure limit mayalso be exceeded if more than onediathermy unit is operating within 2 mof each other (Figure 2). We havemeasured the field existing in the spacebetween a number of diathermy units(both microwave and shortwave), during the administration of commontreatment modalities. The recornmended limit was exceeded between theshortwave devices, but not between twomicrowave devices, presumably due tothe greater directionality of the microwave applicators.
2m
.1.6 mW/cm2
Shortwavekneetreatment
1m
.0.53 mW/cm2
Microwave Shortwavehand treatment, hand treatment
.O.8mW/cm2
DDShortwave Microwaveknee treatment shoulder
treatment
excess of those recommended for occupationalexposure.
It is not impossible that persons notdirectly involved in the use of the machine will be subjected to doses in excess of the recommended limit (Figure4). It must be remembered that forthese persons the recommended limitis five times lower than that applicableto the operator. Normally however thissituation is unlikely to occur becausethe power density varies inversely asthe square of the distance.
Careful planning of the patient treatmentarea can minimize these risks.Advice on the matter can be obtainedfrom the relevant state authorities listedin Appendix C.
Hazards to the PatientObviously these 'safe' limits do not
apply to the patient as the inductionof thermal effects in the patient's bodyis the purpose of diathermy; however,the line between therapeutic and harmful dose can be uncomfortably thin.
In the specific case of diathermy thedetrimental effects of electromagneticradiation may appear in a number ofinstances as a consequence of inappropriate practice or because ofa particu-
Shortwave thightreatment
o1m
1.6 rnW/cm2
Shortwaveknee treatment
Shortwave hand treatment
Planning of Patient Treatment AreaOver-exposure to persons other than
the patient may result from inadequateplanning. To illustrate ,this we haverecreated in our laboratory two examples of badly planned treatmentareas and surveyed the radiation' levelsin positions which could conceivablybe occupied by the operator and/ormembers of the public.
Figure 3 illustrates how reflectionsfrom a filing cabinet and a wallmounted,metallic instrument panelmay produce, within one, metre froma microwave applicator, local fields in
densities at a distance of 1m from theapplicator. It would appear that theshortwave diathermy device in questionmay have had either faulty cables, connectors, or applicator. There were otherdevices in this survey that exceeded thelimits ata distance of 1 rn.
We'htlve tried to replicate this resultusing a$iemens Model 808 device witha wing 'applicator. An ,experiencedphysiotherapist was asked to administershortwave treatment to the thigh ofa patient using a normal therapeuticirradiation level. The environmentalradiation level was measured at severalpoints at a distance of 1 m from theapplicator, using a HoladayHI3002monitor fitted with a E-field probe. Wewere 'able to obtain a level in excess ofthe standard limit only if the cableswere positioned so that they were within0.5 m of the detector.
Also in the Canadian survey (Stu~hlyet af 1982) high power densities weremeasured at, we ,assume, the consoleof a shortwave diathermy device. Thisresult was attributed, in part, to thetreatment regime which consisted oftreating both knees using large diameter air spaced electrodes~ ,Again, theonly way 'we could replicate this result,was to be within 0.5 m of the cable.
In order to help ensure that operators are not exposed in excess of therecommended limit, the codes prescribe the minimum distances that theoperator should maintain from the applicators and leads:
- for shortwaves: 1m from the applicators and O.5m from the 'leads;short excursions closer to the electrodes are permitted but only whennecessary (DHW 1983).
- for microwaves: 2 m from the applicators, but remaining outside thedirect beam.
The distance of 2 m should ensurethat i~ reflections occur (it can be shownthat, due to the possible formation ofstanding waves, power densities mayincrease bya factor offour in this case)the operator exposure will be withinthe J;ecommended limits.
The Australian JQumal of Physiotherapy. Vol. 33, No.3, 1987 155

The Safe u.seofMicrowB.ve and Shortwave
~:0 ~O :0 Eo +fE, =lEo
I-=-
At the frequency ofoperation ofshortwave diathermy, the ratio between thetwo coefficients is such"that the electricfield in the fat layer is considerablylarger than in the muscle. Consequently as the power absorbed is proportional to the square of the electricfield, the power absorbed in~he fat isalmost eight times that absorbed inmuscle.
When the fat layer is not too thick,capacitive applicators may still be used,with care, but .they should be' avoidedwith obese patients (ie persons 20 percent or more over the normal weightrange).
However, if the electric field .is parallel to the interface between muscleand fat, as is the case for microwavetreatment (Figure 6), the boundarycondition requires that Er=Em• Inthis case muscle absorbs more powerthan fat, although the efficacy of the
Figure 6: The electric field of the mi·crowave radiation emitted by diathermyapplicator is parallel to the fat-muscle I
interface.
FigureS: Alignment of polar molecul~sin the dielectric reduces the electriCfield between the capacitor's plates.
~+-
(J \)~+- +
~
• 1.9mW/cm2
Ee
...::- 1 metre ~.. 1.1 mW/cm2
(boundary condition for the electricfield perpendicular to the fat and muscle layers)
of radiation there are some situationswhere they can be caused even by normal therapeutic doses.
The·subcutaneous fat layer is moreeasily heated than the muscle tissueduring shortwave treatment using capacitor type applicators. This effect,beside being a consequence of thepaucity of blood flow in the fat, is alsodue to the different intensities of theelectric field in the two layers (Guyetaf 1974). This can be explained usingan idealized plane wave (Christensenet af 1981).Whenan electric field Eois applied to a dielectric, such as fator muscle, it causes a realignment ofthe electric charges associated with itsmolecules (Figure 5). The charges thusrealigned create an induced field (E)which opposes the applied field. As aresult, the field (EJ within the dielectric is less than Eo.
We can write Eo/Ed = k, where kis the relative dielectric constant of themedium.
At the boundary between fat andmuscle we must have
CavityWalt·
(2 x10 mmplastersheets)
Bums and ScaldsBeside the obvious case ofa burn or ie
scald resulting from an excessive dose
larsusceptibility of the patient to injury.
In a recent Canadian survey (DHW1980) a small number (- 4070) of respondents have reported the incidenceofadverse effects, including increasedpain, burns and pacemaker interference, in some of their patients.
• 0.5 mW/cm2
Figure 4: Persons other than the oper- ~ator can also be exposed to radiation.In this example, the microwave powerdensity at the receptionist's waist .levelwas measured to be =0.5 mW/cm2
,
which is 2.5 times the recommendedlimit. The distances between therecep..tionist and the applicator was 2.1 m.The microwave output was 180 w.
Figure 3: The presence of reflecting objects may cause hazardous radiation levelseven behind a microwave applicator.
156 The Australian Journal of Physiotherapy. Vol. 33, No.3, 1987

The Safe use of Microwave and Shortwave
treatment is reduced, as there is no shown that elevations of core temper-therapeutic value in heating the fat ature in excess of 2.5°C during thelayer. For instance, it can be shown organogenesis stage of pregnancy re-that less than half of the incident power suIt in increased resorption of fetusesreaches the muscle if the fat layer is 2 and in congenital birth defects of thecm thick. central nervous system. The latter, and
An accurate estimate of the rate of the associated clinical disorders in an-temperature increase in fat and muscle imals, have been reviewed extensivelytissuei~very difficult to obtain because by Edwards (1978, 1981).of the 'many variables involved. The While experimental data is lackingultimate decision on the use of diath- for primates, retrospective and pro-ermy units with overweight patients spective studies of mothers with febrilemust be left to the professional judge- illnesses in the first trimester indicatement of the therapist. Shortwave ap- that hyperthermia has similar terato-plicators that have predominantly a genic effects on the developing humanmagnetic field output (egcoil, monode, fetus (Smith 1978, Clarren 1979)..diplode) are the most suitable to pro- A recent epidemiological study ofduce deep tissue heating without much birth outcomes among physiotherapistsrisk of burns to the fat layer (Kloth in Sweden has found a higher than1984). normal incidence of dead or mal-
Perspiration must be allowed to formed infants bornto those operatingevaporate freely not only to help dis- shortwave diathermy units (Kallenetsipate body heat but alsobecause~ater al 1982). Rubin and Erdman (1983)is heated by the electromagnetic radia- reported four cases of patients beingtion. In the case of microwaves this is treated with microwave diathermy forthe major heating mechanism. Drop-chronic pelvic inflamation who becamelets of perspiration on the skin can pregnant during the course of the treat-rapidly reach a very high temperature ment and therefore received-microwave(Kloth 1984). Only dry towelling should exposure to the pelvis just prior to andbe used when this is necessary to sup- during early pregnancy. In one case theport the induction coil used with some pregnancy resulted ina miscarriage.shortwave therapy regimes, otherwise Three similar cases, this time involvingall clothing, bandages and coverings shortwave diathermy, were reported byshould be removed. Nylon and other C Imrie (1971). One of the pregnanciessynthetic fibres are particularly unsuit- terminated in a miscarriage. Ghiettiable because they retain the moisture (1955) reported the birth of a mal-against the skin. If, in the course of a formed, -immature, convulsive infantmicrowave or shortwave treatment, whose mother had been treated withperspiration appears on the patient's shortwaves during the frrsttwomonthsskin, the treatment should be inter- of pregnan.cy. Although no direct linkrupted and the skin dried. For this can be established between these ad-reason and to make sure that the pa- verse pregnancy outcomes and thetient remains in the proper position and diathermy treatments, these cases, to-most importantly, does not look to- getherwith the results obtained fromwards the applicator, .it is necessary animal experimentation, suggest that itthat the patient not be left alone during is wise to avoid microwave and/orthe microwave treatment. shortwave exposure during pregnancy.
Teratogenic EffectsTeratogenic effects following mater
nalhyperthermia have beenexperimentally demonstrated in a number ofanimal sp.ecies,notably the guinea pig(Edwards 1967, 1978). It has been
Specific PrecautionsApart from the normal contraindi
cations such as open wounds, haemorrhage or acute infections, the followingare more specific risks.
If the irradiated region contains acancerous growth, temperature tendsto develop in the tumor higher thanthat in surrounding normal tissue(Babbs 1981). This increase in the temperature leads to the destruction ofcancerous cells and therefore, diathermy is sometimes used as <a therapyfor cancer patients. However, if thetemperature is between 40 and 41.5°C,the growth rate of tumors is accelerated(Burr 1974). The use of diathermy ·istherefore contraindicated in patientswith evidence of cancer, unless it ispart ofa specific cancer therapy regime.
Metal intensifies the electromagneticfields, potentially leading to hazardoustemperature increases. Therefore thetreatment of patients having metallicimplants in the treatment area is contraindicated. For the same reason allmetal such as rings and watches shouldbe removed from the area oftreatment.
The presence of a·cardiac pacemakerin a patient also constitutes acontraindicatlon. The risk, obviously, dependson·the treatment regime, being minimalfor treatment of the extremities.
Diathermy is also contraindicatedwith patients who do not possess normal pain and thermal sensation in thearea to be treated.
Adverse Effects on the EyeAcute exposure may cause injury to
the eye, particularly using frequenciesranging from 1 GHz to 10 GHz (andtherefore including the freqliency ofoperation of microwave diathermyunits). Cataract formation may be induced in animals by exposure for 1hour to power densities in the 150 to200 mW/cm~range (Ruggera 1980).These levels are similar to those produced by microwave diathermy units.Retinal lesions may also occur (Cleary1980).
Unintentional irradiation of the eyesis a real .possibility due to the limiteddirectionality of the applicators.Bassen etal (1978) have reported that mostnon..contact applicators exhibit a highlevel of radiation 'leakage', that is ra"
The AustralIan Journal of PhysIotherapy. Vot 33, No.3, 1987 157

The Safe use of Microwave and Shortwave
diation delivered to the environmentrather than to the target tissue. Levelsup to 44mWIcm2 were measured at 5em from the applicator.
The danger that microwaves pose tothe eyes, cannot be overcome easily.Goggles do not offer adequate protec...tioll-\because, as the dimensions of theeyepie~esare comparable to the wavelength':bf the radiation, the diffractionaround the edges is significant. It hasalso been shown (Griffin 1983) thatmetal rimmed ,spectacles enhance thefield near the eye. Therefore it isrecommended that the head never beirradiated with microwaves except inthe course of cancer therapy.
Effects on the GonadsThe testes are also particularly sen...
sitive to hyperthemia. Exposure of thescrotal area to microwaves at 2450 MHzand at power densities greater thah 50mW/cm2 resulted in varying degrees oftesticular damage (such as oedema,atrophy, fibrosis and coagulation necrosis of seminiferous tubules) in lab...oratory animals (Leach 1980, WHO1982, Manikowska-Czerska 1985). Theoveries are also susceptible to hyperth...ermia; ,however,being located deep inthe pelvic cavity they are not normallyaffected by microwave diathermy(Elder 1984). Shortwaves, on the otherhand, can penetrate many centimetresof tissue and may put the ovaries atrisk.
Conclusion
We have reviewed the hazards presented by the high radiation level as...sociatedwith shortwave and microwave diathermy.
We have pointed out the possibilityfor the operator to be exposed to levelsexceeding those prescribed by the ap...propriatestandard.
Patients ,may also be at ,risk if theoperator is untrained and/or carelessor if the patient is unco...operative egunable to understand and follow theinstructions and appreciate thepotential risks.
It is therefore concluded that theseunits can only be operated by registeredhealth professionals as defined in theCodes (Appendices A and B).
AcknowledgementWe wish to thank Mrs JoanMc
Meeken and Mr Alex Ward for usefuldiscussions and for allowing us to carryout measurements on the diathermyunits at the Lincoln Institute of HealthSciences, Victoria.
ReferencesBabbs CF, DewittDP, (l981),Physicai principles
of local heat therapy for cancer, Medical Instrumentation (USA)~ 15, 367 ~ 73.
Bassen 'HI, Kantor G, Ruggera PS and WittersOM (1978), Leakage in the Proximity of Microwave Diathermy Applicators Used on Humans or Phantom Models~ HEW Publication(FDA),79-8073.
Burr B (1974), Heat as a Therapeutic ModalityAgainst Cancer, Report No. 16, US NationalCancer Institute, ,Bethesda, MD.
ChristensenDA and Durney CH (l985) Hyperthermia production for cancer therapy: Review offundamentals and methods, Journal of Microwave Power, ,16, 89-105.
ClarrenSK,Smith OW, Harvey MAS, Ward RHand Myrianthopoulas NC (1979),Hypertherrnia- a prospective evaluation of a possible teratogenic agent inman, Journal of Pediatrics~ 95,81-83.
Cleary SF (1980), Microwavecataractogenesis,Proceedings of the lEEE~68, 49~55.
DHW (1980), - Canada- Wide Survey of Nonionising Radiation Emitting Medical Devices,Canadian Department of Health and Welfare,80-EHD-52.
DHW (1983)" Safety code 25-ShortwaveDiathermy Guidelines for Limited RadiofrequencyExposure, Canadian Department of Health andWelfare, 83~EHD-98.
Edwards MJ(1967), Congenital ,defects in guineapigs following induced bypermia during gestation, Archives of Pathology and LaboratoryMedicine~84, ,42-48.
Edwards ,MJ (1978), Congenital defects due tohyperthermia, Advances in Veterinary Scienceand Comparative Medicine 22, 29-52.
Edwards MJ (1981) Clinical disorders offetal braindevelopment, in Fetal Brain Disorders-RecentApproaches to ,the Problem of Mental Deficiency, BS Hetzel and RM Smith (Eds.), ElsevierlNortb Holland Biomedical Press, Chapter14, pp. 335~364.
Elder JA and Cahill DF (Eds)(l984), BiologicalEffects ofRadiofrequency Radiation~ EPA-600188-83-026F,Research Triangle Park, North Carolina.
Ghietli A (1955), Embriopatia da onde corte Contributo cUnica sperimentale, Minerva Nipiologica (Torino)~5, 7-12.
GriffinDW (1983), Techniquesfor Measuring Microwave Fields Near the Eyes in Models ojHumans~ 19th International electronicsconvention and exhibition, The Institution of Radioand' Electronics Engineers, ,Sydney.
Guy AW,Lehmann JF and Stonebridge JB (1974),Therapeutic applications of electromagneticpower, Proceedings of the IEEE~(j2, 55-75.
Imrie AH(197l), Pelvic shortwave diathermy giveninadvertently in early pregnancy, Journal ofObstetrics and Gynaecology of the British Commonwealth, 7891-92.
KallenB, Malmquist G and Moritz U (1982),Delivery outcome among physiotherapists inSweden: Is non-ionizing radiation a fetalhazard?, Archives of Environmental Health~37,81-84.
Kloth L,Morrison MA and Ferguson BH (1984),Therapeutic Microwave and Shortwave Diathermy~ US Dept. of Health and Human Services"- HRS Publication FDA 85-8237.
LeachWM (1980), Genetic, growth and reproductioneffects of microwave radiation. Bulletinofthe New York Academy ofMedicine~ SecondSeries, '56, 249-257.
Manikowska-CzerskaE,CzerskiP and Leach WM(l985), Effects of microwaves on meiotic chromosomes of male CBA/CAYmice, The Journalof Heredity, 76, 71-73.
Osepchuk JM (1979), Sources and basic characteristics ofmicrowave/RF radiation, Bulletin ofthe New York Academy of Medicine~ 55,976998.
Rubin A and Erdman WJ (1959), Case reports,American Journal oj PhysicalMedicine~ 38,219-220.
Ruggera PS (1980), Measurements of EmissionLevels During Microwave and Shortwave Diathermy Treatments~ Bureau of Radiological Healthreport, HHSPublication (FDA) 80-8119.
SAA (1985), Australian Standard 2772, MaximumExposure Levels~ Radio-Frequency Radiation 300kHz ,to 3000Hz, 'Standards Association ofAustralia Publication, Sydney.
Schwan HP and Piersol GM (1954), The absorption of electromagnetic energy in body tissues,American Journal of Physical Medicine, 33,371-404.
Schwan HP (1970), Interaction of Microwave andRadiofrequencyRadiation with BiologicalSysterns, ,in "Biological Effects and Health Implications ojMicrowave Radiation, SF Cleary (Ed),US Department of Health, Education and Welfare,Washington, pg 13-20.
Smith OW, Clarren SKand Harvey MAS (1978),Hyperthermia as a 'possible teratogenic ,agent,Journal of Pediatrics, 92, 878-883.
SteneckNH (1984),The Microwave Debate~ MITPress, Cambridge, Mass., USA.
Stuchly MA, Repacholi MH, Lecyer DWandMann RD (1982), Exposure to the operator andpatient during shortwave diathermy treatments,Health Physics~ 42,341-366.
Symposium on Health Aspects of non-ionizingradiation (1979), Bulletin of the New YorkAcademy of Medicine, 55, 973-1296.
USA Federal Register, (1980), Microwave Diathermy products; Performance standard~ 45, (147).
Witters OM and Kantor G (1979), Free~Space
Electric Field Mapping of Microwave Diathermy Applicators~ HEW Publication (FDA)79.8074.
WHO (1981), Environmental Health Criteria 16- Radiofrequencyand Microwaves~ WorldHealth Organization - Geneva.
WHO (1982), WHO Regional Publication European Series 'No. 10, Non-ionizing RadiationProtection~ Copenhagen, p. 111.
158 The Australian Joumalof Physiotherapy. Vol. 33, No.3, 1987

The Safe use of Microwave and Shortwave
Appendix ACode of Practice for the SafeUse of Microwave Diathermy
Units (1985)*
IntroductionThe therapeutic use of heat produced by
microwtlye radiation absorbed in the bodyis called*, microwave diathermy. The heatincreases the .flow of blood in the tissuesthrough dilation of the blood vessels. Thisin tum increases capillary pressure, cellularmembrane permeabilitY,and metabolic rate,causing a more rapid transfer of nutrientsfrom the·blood across cell membranes. Theseactions may reduce pain and promotequicker healing.
A microwave diathermy unit is a devicedesigned to generate microwave radiationand transfer it, via a coaxial cable and aradiating antenna, to the area to be treated.The antennais incorporatedin an applicatorwhich· has the function of directing the radiation towards the area to be treated.
These devices are capable of generatinga sufficiently high levelaf radiation thatthere may because for concern for thesafety of the eyes, the gonads and, in thecase of pregnant patients, the foetus. It isclaimed that radiation from microwavediathermy applicators has caused cataractsin patients being treated for sinus conditions. The eyes of patients being treated fora neck or shoulder injury could also beinadvertently subjected .to ·stray radiation.Improper use of the machine may result inburnsand/or scalds and tissue or organdamage. Care must also be taken to avoidsubjecting the operatorand/or the publicto radiation levels exceeding those prescribed in the Australian standard AS 2772(Maximum Exposure Levels - Radio..frequency Radiation - 300kHz to 300GHz). It must be noted that the level ofradiation present in the vicinity ofadiathermy unit may .be increased by reflections.
Care must be taken to ensure that themicrowave radiation does not cause interference with other equipment.
This Code sets down appropriate rulesand procedures to avoid excessive and/orunnecessary exposure to microwaveradiationbut should be read in conjunction withany State/Territory regulations coveringtheir use.
DefinitionsMicrowave diathermy unit means a device
using electromagnetic energy in the microwave frequency range (300 MHz to 300 GHz)
• Reproduced by courtesy of The National Health andMedical Research Council.
for therapeutic purposes. The unit includesapplicators, the microwave generator, andall associated electronics, controls and enclosures. In Australia the only approvedfrequency for microwave diathermy treatments is 2450 MHz.Treatment means the use of a microwavediathermy unit ana human being to treata symptom, disease or disability.Applicator- means any device designed toconduct, transmit or transferelectromagnetic energy from a microwave diathermyunit to a patient undergoing treatment.Contro/means any control used during opertion of a microwave diathermy unit whichaffects the microwave radiation· emitted bythe applicator.Health professional means a registered person who has satisfactorily completed an appropriate course of training approved bythe relevant registration board and the State/Territory health authority.User means the person having administrative responsibility for ·use of·a particularmicrowave diathermy unit. This.person.shallbe the owner or hirer of the unit or hisagent or, if. the unit is owned or hired byan .institution .or organization, the agent ofthat body.Operator means the health professionalgiven the responsibility, by the user, to treatthe patient using .a microwave diathermyunit.Shall indicates that the particular requirement is considered necessary to ensure protection from radiation.Should indicates a procedure or precautionwhich is to be applied, whenever practicable, in the interests·of minimizing radiationhazards.
Hazards of ffigh Level Exposure to Microwave RadiationBurns
These may result as a consequence ofexcessive irradiances or may he due to pref..erential absorption of microwave radiation(as in the case of a wet dressing over awound) or to red.ucedheat dissipation mechanisms (as in the case· of the subcutaneousfat layer). .In some cases deep tissue andorgan damage may ensue.
Ocular effectsLens opacities maybe induced by micro
wave radiation..Single exposure to intense(> 100 mW /cm~ electromagnetic radiationat 2450 MHz for an hour or longer hasresulted in cataract formation inexperimental animals. The power density in thetherapeutic beam is of a similar level, butthe treatment time is generally somewhatshorter. However, repeated direct irradiation of the eye at such levels and for suchtreatment times does approach the power-
time threshold required for cataract production. Goggles do not offer reliable protection.
Effects on the GonadsExposure to microwave .radiation may in·
crease the temperature of the testes to thepoint where temporary sterility is induced.Very .high specific absorption rates maycause permanent damage. The ovaries mayalso be at risk.
Teratogenic EffectsAbnormalities in offspring have beenre
ported in several animal species after exposure to intense microwave radiation. Intense fields resulting in significanttemperature increase of the foetus couldresult in teratogenic effects in humans.
Examination and ·InterviewMicrowave treatment shall not be admin
istered unless prescribed by a health professional .(as previously defined). At the examination .and interview, when treatment isbeing prescribed, the health professionalshall determine the suitability of the patientfor treatment. This.should not be prescribedif:- The patient does not understand the
potential risks,- the patient is not able to co-operate with
the operator in maintaining the properposition and in reporting the presenceofa heating sensation which is the onlyindication of an adequate or excessivedose.
- the patient does not have normal sensation ·in the treatment area,
- the patient has metallic implants withinthe treatment area,
- the patient is pregnant,- the patient wears apacem,aker,- the patient has undergone ionizingra-
diation therapy to the treatment area inthe three months prior to the diathermybeing administered, as skin sensation andblood circulation may be diminished,
;,- there is evidence .or known history ofvascular insufficiency,
- the patient has any evidence of cancer,unless the microwave treatment is carriedout as partofa hyperthermia treatment regime. (The metastasis of a cancerous growth may be accelerated byamoderate increase in temperature,suchas .can be caused by a microwave treatment not specifically intended to treat amalignancy.),
- there are open wounds,haemorrhage,ischaemic tissue, tuberculous joints, oracute infections within· the treatmentarea.
In the cases where the health professional,after due risk/benefit consideration,sees itnecessary to prescribe >microwave diathermy
The Australian Journal of Physiotherapy. Vol. 33, No. 3)1987 159

The Safe use of Microwave and Shortwave
treatment outside the guidelines given above,adequate advice shall be given to the patient,to the user and to the operator ofthe micro,,wave diathermy unit.
The head shall not be directly irradiatedas there isa significant· risk of irradiatingthe eyes. Most applicators are notsuffi,.ciently directional to restrict irradiation tothe targeted area. Microwave irradiation ofthe head may only be carried <out as partof acaAcer therapy.
User ResponsibilitiesThe user shall ensure, by.administrative
controls or otherwise, that:- the microwave apparatus complies with
all relevant Australian Standards and ismaintained .inaccordance with the reI,.evant State requirements,
- the unit is operated only by healthprofessionals,
- the unit operator is not exposed to aradiation level exceeding the standardfor ·occupational exposure specified bythe appropriate .authority,
- the general public (including waiting patients, receptionist etc.) is not exp,osedtoa radiation level exceeding \hatrecommended by the appropriate authority,
- a range of applicators suitable for treating different areas of the body is avail,,able (the use of modern applicatorswhich reduce scattered radiation andconcentrate the energy to the treatmentarea is encouraged),
-"- a visibleandloraudibl~ signal is installed, to indicate that the unit is operating,
- the unit is not. the cause of electric interference with other equipment (Thismay require the use of a screened.cubicleand a.mains ruter.),
- non metallic chairs andlor beds areavailable to patients undergoing microwave diathermy treatments.
TreatmentBefore administering the treatment the
operator shall:-"-ensure that the thermal sensitivity of the
patients is not impaired by analgesics,- ensure that the patient has removed all
metallic objects (rings, watches metalrimmed glasses, etc.) from the treatmentarea,
-ensure that the treatment area is notcovered bya wet dressing or adhesivetape,
-"- remove bandages or clothing from thetreatment area,
-"- ensure that the skin is dry,- ensure that if the patient is wearing a
hearing aid, .it is. removed,-"-ask the patient to immediately report any
symptoms experienced during the treat-
ment except' 'a mild, comfortablewarmth",
-"-ensure that the testes are not .directlyirradiated and that care is taken to minimize indirect ·irradiation,
-ensure that the coaxial cable is correctlyconnected to both the machine .and theapplicator,
- .not rest the applicator or cable over metalsurfaces,
-align the·applicator. accurately to ensurean appropriate pattern of heating,
- direct the applicator awayfromthe unit'scontrols,
- use.care in.handling the applicator (damage may result in an alteration of itsdirectional properties),
- ensure that the chair or other patientsupport is not metallic.
After activating the unit the operatorshall:- remain outside the field of emission of
microwaves and at least 2 metres fromthe patient,
- not leave the patient alone in the roomduring .the treatment,
- ensure that the patient maintains the correct position and remains co-operative,
- interrupt the treatment if perspirationappears on· the patient'sskin,
- not allow the patient to touch the unit,- ensure that no other person is in the
vicinity of the unit or of the applicatorduring the treatment, in accordance withthe administrative controls establishedby the user.
AppendixB
Code of Practice for the SafeUse of Shortwave*
(Radiofrequency) DiathermyUnits (1985)
IntroductionThe therapeutic use of heat produced in
deep tissue ·by<electromagnetic radiation ab"sorbed ·in .the body is called diathermy. Theheat increases the flow of blood in the tissues through dilation of the blood vessels.This in tum increases capillary pressure,cellular membrane permeability, and metabolic rate, .causing a more rapid transferof nutrients from the blood across cellmembranes. These actions may reduce pain andpromote quicker healing~
• Reproduced by courtesy of the National Health andMedical· Research Council.
A shortwave diathermy unit is a devicedesigned to generate radiofrequency radiationand transfer it, via cables andelectrodes, to theare~ to be treated. The unitscan be operated in either a continuous waveor pulsed mode, but both produce heat indeep tissue. Two basic types of electrodes(applicators) are in use, the capacitor typeand the inductor type. Inthe first case tissueheating is basically due to the radiofrequency electric field, while for the inductiveelectrodes .(coils), .heating occurs by a combination of electric field effects and currentsinduced in the tissue by a magnetic field,the heating profile of the two mechanismsis somewhat different.
These devices are capable of generatinga sufficiently .high level of radiation thatthere maybe cause for concern for thesafety of the gonads and, in the case ofpregnant patients, the foetus. Improper useof the machine may result in burns andlorscalds and deep ·tissue or organ damage.Care must also be taken to avoid subjectingthe operatorand/or the public to radiationlevels exceeding those prescribed in the Australian standard AS 2772 (maximum exposure levels· - radio-frequency radiation 300kHz to 300 GHz). Itmust be noted thatthe level of radiation present in the vicinityof a diathermy unit may be increased bythe presence of nearby metallic objects orother units or by reflection from the wall.
Care must be taken to ensure that theshortwave radiation .does not cause interferencewith other equipment.
This Code sets down appropriate rulesand procedures to avoidexcessiveand/orunnecessary exposure to shortwave radia·tion but should be read in conjunction withanyState/Territory regulations coveringtheir use.
DefinitionsShortwave diathermy unit means a·device
using electromagnetic energy in the shortwave frequency range (3-30 MHz) fortherapeutic purposes. The unit includes electrodes, the shortwavegenerator,and allassociated electronics, controls andenclosures. In Australia the only approved frequency for shortwave diathermy is 27.12MHz.Treatment means the use ofa.shortwavediathermy unit ana human being to treata symptom, disease or disability.Applicator means any device designed toconduct, transmit or transfer electromag"netic energy from a shortwave diathermyunit to a patient undergoing treatment.Control means any control used during apemon of a shortwave diathermy unit whichaffects the radiation emitted by theapplicator.Health professional means a registered person who has satisfactorily completed an .ap-
1'60 The Australian. Journal of Physiotherapy. Vol. 33, No. 3,1987

The Safe use of Microwave and Shortwave
propriate course of training approved bythe relevant registration board and the State/Territory health authority.User means the person having administra..tive responsibility for use of a particularshortwave diathermy unit. This person shallbe the owner or hirer of the unit or hisagent or, if the unit is.owned or hired byan instttution or .organization, the agent ofthat bod¥.Operator means the health professionalgiven the responsibility, by the user,· to treatthe patient using a shortwave diathermy unit.Shall indicates that the particular requirement .is considered necessary to ensure pro..tection from radiation.Should indicates a procedure or precautionwhich is to be applied, whenever practicable, in the interests of minimizing radiationhazards.
Hazards of Higb Level Exposure to Microwave RadiationBurns
These may result as a consequence ofexcessive exposures or may be due to nonuniform heating of different tissue layer& orto reduced heat dissipation mechanisms (asin the case of the subcutaneous fat layer).In some cases deep tissue and organ damagemay ensue because heating is induced at adepth where thermal sensation is reduced.
Teratogenic EffectsAbnormalities in offspring have been re
ported in several animal species after exposure to intense shortwave radiation.Intense fields resulting in significant temperature increase of the foetus could resultin teratogenic effects in humans.
Effects on the GonadsExposure to shortwave radiation may in
crease the temperature of the testes to thepoint where temporary·sterility is induced.Very high specific absorption rates maycause permanent damage. The ovaries mayalso be at risk.
Examination and InterviewShortwave treatment shall not be admin
istered unless prescribed by a health professional (as previously defined). At the examination and interview, when treatment is _being prescribed, the health professionalshall determine the suitability of the patientfor treatment. This should not be prescribedif:-Thepatient does not understand the po
tential risks,- the 'patient is not able to co-operate with
the operator in maintaining the properposition and in reporting the presenceof a heating sensation which is the onlyindication of an adequate or excessivedose.
- the patient does not have normal sensation in the treatment area,
~ the patient has metallic implants withinthe treatment area,
- the· patient is pregnant,- the patient wears a pacemaker,- the patient has undergone ionizing ra"
diation therapy to the treatment area inthe three months prior to the diathermybeing administered, as skin sensation andblood circulation maybe diminished,
- there is evidence or known history ofvascular insuffiCiency in the treatmentarea,
- the patient has any evidence of cancer,unless the shortwave treatment is carriedollt.as part of a hyperthermia treatmentregime. (The metastasis of a cancerousgrowth may be accelerated by a moderate increase in temperature, such ascan be caused by a shortwave treatmentnot specifically intended to treat a malignancy.),
- there are open wounds, haemorrhage,ischaemic tissue, tuberculous joints, oracute infections within the treatmentarea.
In the cases where the clinician, ·after duerisk/benefit consideration, deems it necessary to prescribe shortwave diathermy treatment outside the guidelines given above,adequate advice shall be given to the patient,to the user and to the operator of the shortwave diathermy unit.
User ResponsibilitiesThe user shall ensure, by administrative
control or otherwise, that:- the shortwave diathermy unit complies
with all relevant Australian Standardsand is maintained in accordance withthe relevant State requirements,
- the unit is operated only by healthprofessionals,
- the unit operator is not exposed toaradiation level exceeding the standardfor occupational exposure specified bythe appropriate authority,
- the general public (including waitingpatients, receptionist etc.) is not exposedtoa radiation level exceeding thatrecommended by the appropriate authority,
- a range of applicators suitable for treating different areas of the body is available,
-a visibleand/or audible signal is installed, to indicate that the unit isoperating,
- the unit is not the cause of electric interferencewith other equipment ·(Thismay require the use of a screened cubicleand a mains filter.),
-non metallic chairs and/or beds areavailable to patients undergoing shortwave diathermy treatments.
TreatmentBefore administering the treatment the
operator shall:---ensure that the thermal sensitivity of the
patient is not impaired. by analgesics,--- ensure that the .patient has removed all
metallic objects (rings, watches, metalrimmed glasses, etc.) from the treatmentarea.
- remove bandages or clothing from thetreatment area,
- ensure that the skin is dry,- ensure that if the patient is wearing a
hearing aid, it is removed,- ask the patientto report immediately any
symptoms experienced during' treatmentexcept "a mild, comfortable warmth",
-ensure that the cables are correctly connected to both the machine and the applicator,
- not rest the applicator or cables overmetal .surfaces,
- align the applicator accurately to ensurean appropriate pattern of heating,
- ensure that the testes are not directlyirradiated and that care is taken to minimize indirect irradiation,
-ensure that the cables leading to the applicatorare not placed in the vicinity ofthe patient's non targeted tissue,
-ensure that the chair or other patientsupport is not metallic and that otherlarge metallic objects are kept at leastthree metres from the electrodesandcables.
After activating the unit the operatorshall:- remain at least .1 m from the electrodes
and 0.5 m from the cables during treatment,
- ensurethat the patientmainta,ins the cor-"rectposition and remains co~operative,
- not leave the patient during the .treatment,unless the patient has been supplied with an emergency cut-off switchand the patient is reliable,
- not· allow the patient to touch the unit,- ensure .that no other person is in .the
vicinity of the unit or of the applicatorduring the treatment, in accordance withthe administrative controls establishedby the user.
Appendix C
Advisory AuthoritiesAustralia:Australian Capital TerritoryConsultant, Radiation ·SafetyACT Health AuthorityPO Box 825CANBERRA CITY ACT 2601Telephone: (062) 47 2899
The Australian Joumalof Physiotherapy. Vol. 33, No.3, 1987 181

The Safe use of Microwave and Shortwave
New South WalesOfficer-in-ChargeRadiation Health ServicesDepartment of HealthPOBox 163LIDCOMBE NSW2141Telephone: (02) 646 0327
Norlhern TerritoryDirectorOccup~tional and Environmental HealthNT Department of HealthPO Box 1701DARWIN NT 5794Telephone: (089)802601
QueenslandDirectorDivision of Health and Medical Physics
.Department of Health535 Wickham TerraceBRISBANE QLD 4000Telephone: (07) 224 5611
South AustraliaSenior Health PhysicistOccupational Health and Radiation ControlBranchSouth Australian Health CommissionGPO Box 1313ADELAIDE SA 5001Telephone: (08) 2183473
TasmaniaHealth PhysicistDivision of Public HealthDepartment of Health ServicesPO Box 191BHOBART TAS 7001Telephone: (002) 306421
VictoriaChief Radiation OfficerRadiation Safety SectionHealth Department of Victoria555 Collins StreetMELBOURNE VIC 3000Telephone: (03) 616 7084
Western AustraliaThe. DirectorRadiation Health BranchHealth Department of Western AustraliaVerdun Street·NEDLANDS WA 6009Telephone: (09) 389 2713
CommonwealthDirectorAustralian Radiation LaboratoryLower Plenty RoadYALLAMBIE VIC 3085Telephone: (03) 433 2211
New Zealand:The DirectorNational Radiation LaboratoryPOBox 25-009CHRISTCHURCHTelephone: Christchurch 65 059
162 The Australian Journal of PhysiQtherapy. Vol. 33, No.3, 1987